
Exploration of Therapeutic Strategies of Herbal Prescriptions for Carbuncle Treatment to Suggest Modern Approaches to Inflammatory Bowel Disease: Cluster and Network Analyses of the Book «Liu Juan Zi Gui Yi Fang»


Abstract
:1. Introduction
2. Material and Methods
2.1. Selection of Prescriptions for Treating Carbuncles
2.2. Data Extraction, Standardization, and Tokenization
2.3. Prescription Clustering Based on EATM Expert Knowledge
2.4. Hierarchical and Non-Hierarchical Cluster Analysis
2.4.1. Jaccard Index Calculation as a Similarity Measure
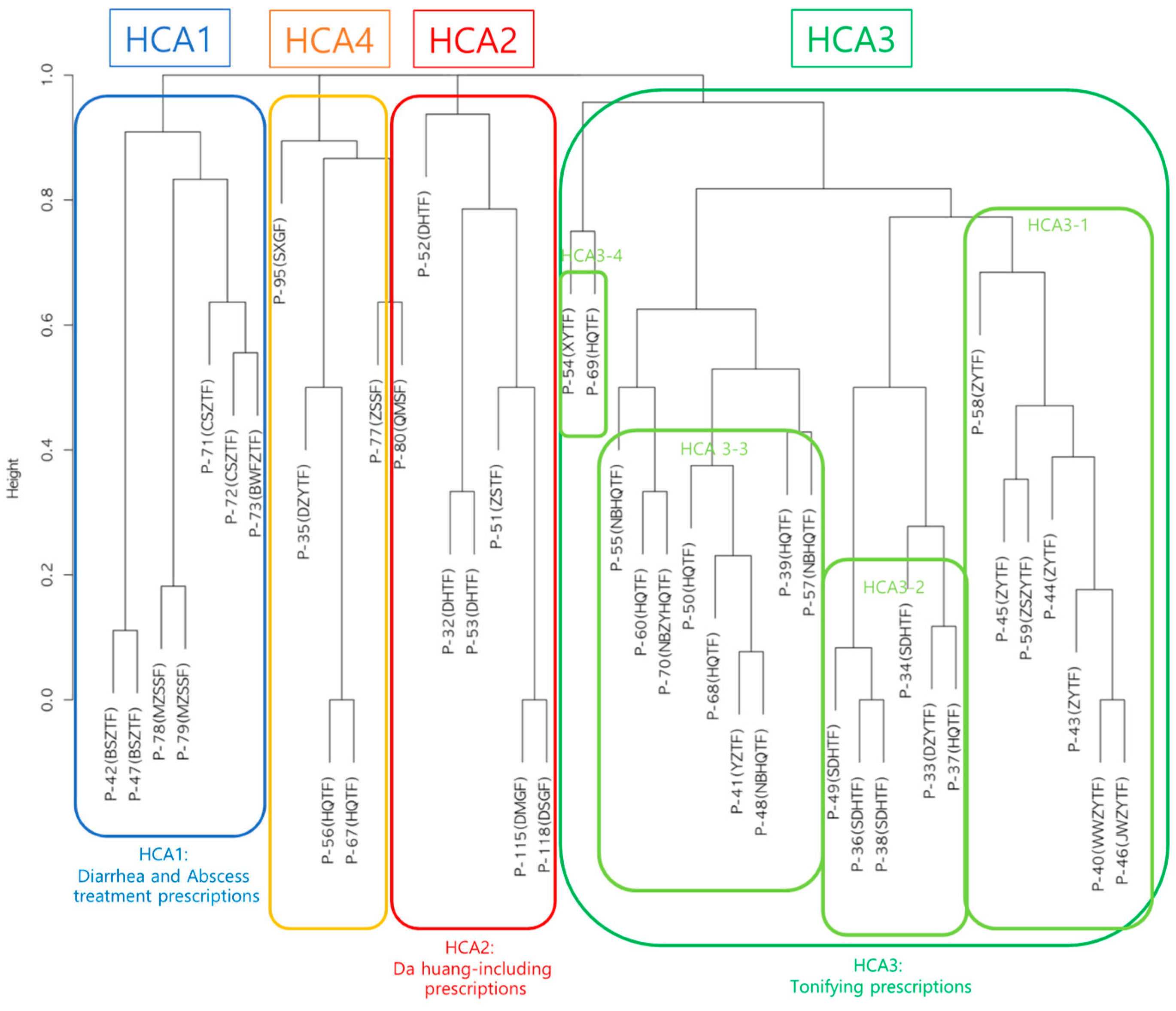
2.4.2. Hierarchical Cluster Analysis
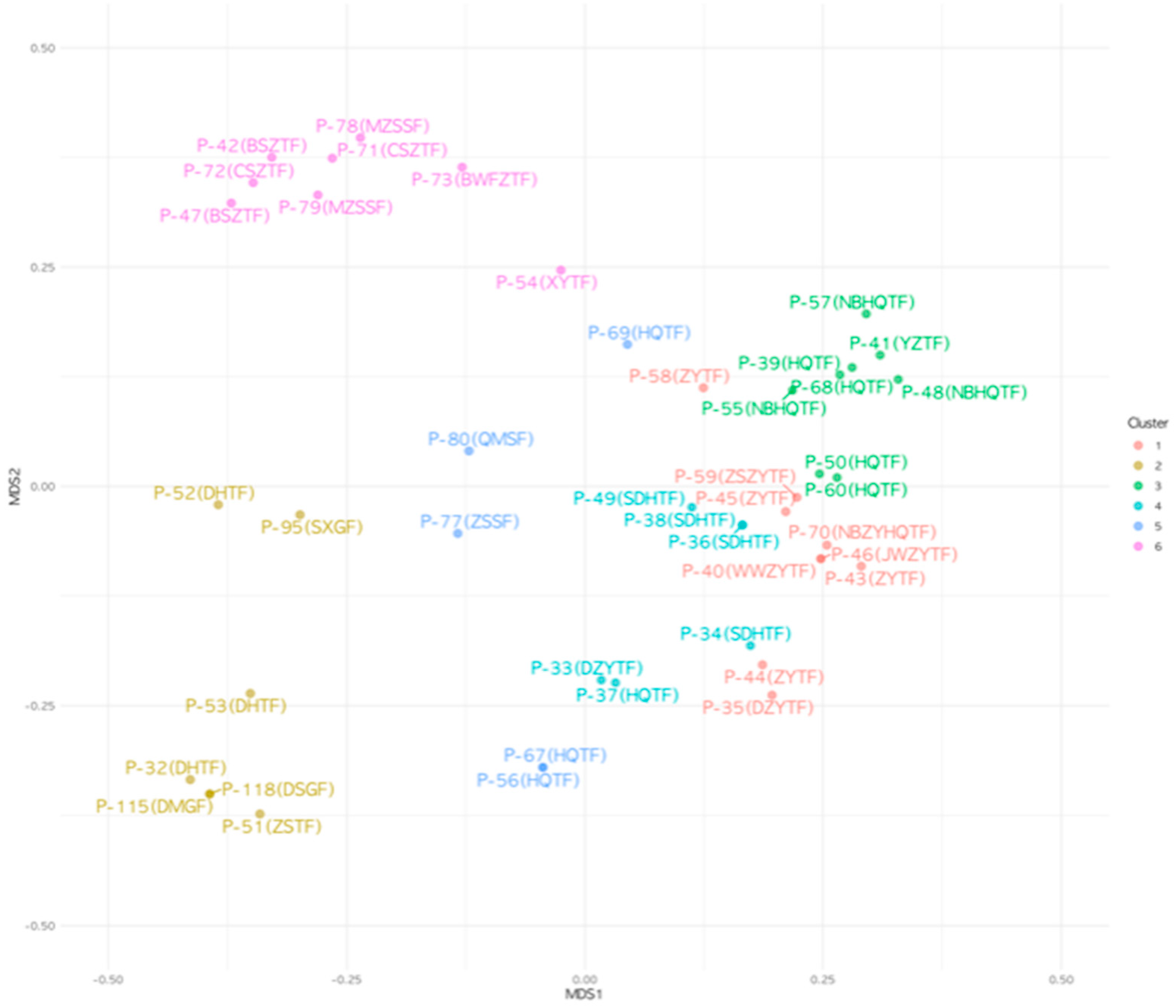
2.4.3. k-Means Cluster Analysis
2.5. Construction and Analysis of Heterogeneous Information Network of Herb–Indication (H-I) Relationship
3. Results
3.1. Prescription Clustering by EATM Expert Group
3.2. Results of Hierarchical Cluster Analysis
3.3. Prescription Group Partitioning by k-Means Cluster Analysis
3.4. Sensitivity Analysis of the Impact of the Pre-Specified Number of Clusters on Prescription Clustering by k-Means Cluster Analysis
3.5. Sensitivity Analysis of the Impact of Initial Centroid Position Changes on Prescription Clustering by k-Means Cluster Analysis
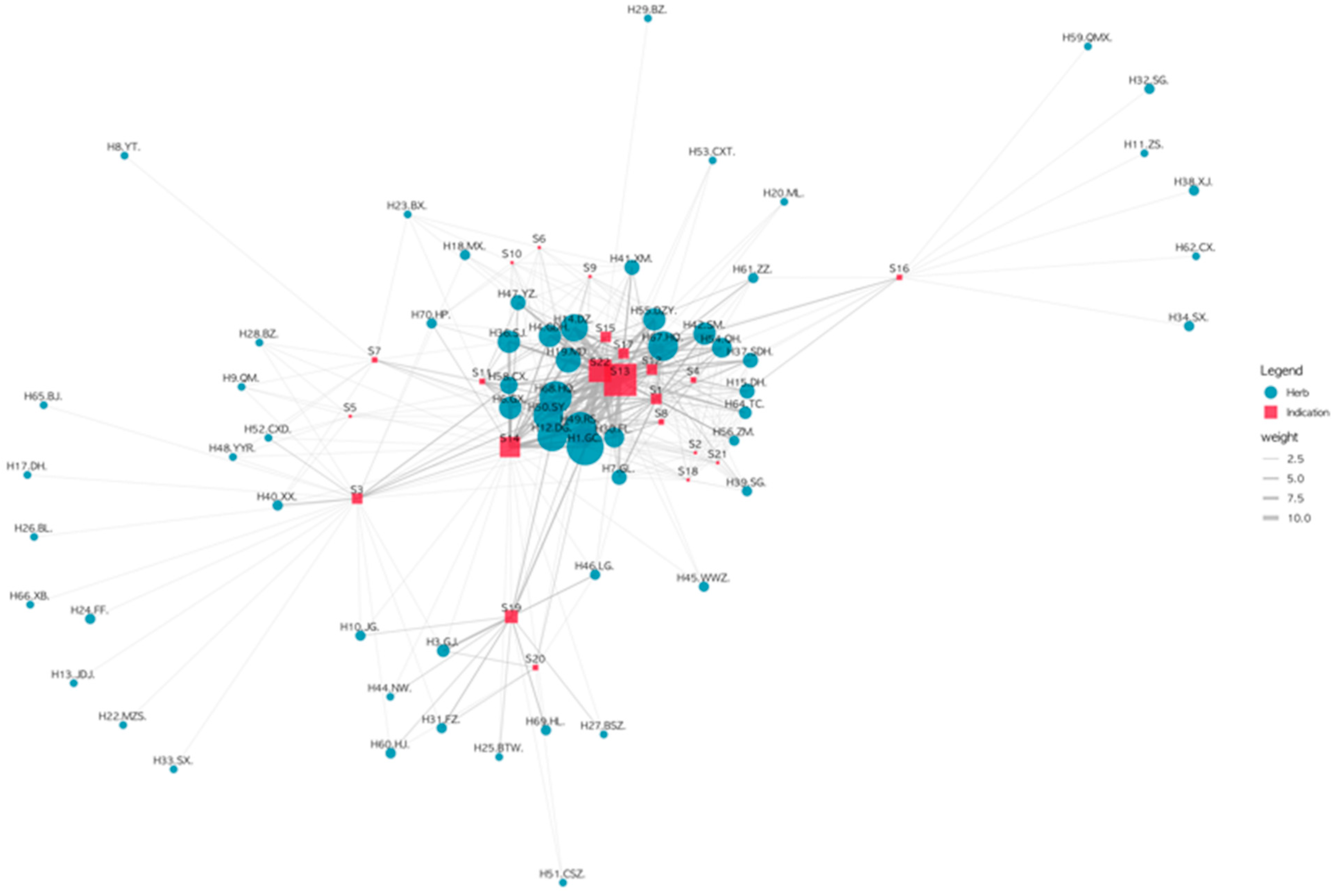
3.6. Constructing the Herb–Indication Relationship Network for Carbuncle Treatment Prescriptions
3.7. Cluster-Specific H-I Subnetworks
4. Discussion
4.1. Summary of Findings
4.2. Modern Applications of Herbal Prescriptions for IBD Management in Clinical Practice and Suggestions for Further Research
4.3. Importance of Integrating Expert Insights with Data Mining Methodology in EATM Knowledge Enrichment
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gordon, H.; Biancone, L.; Fiorino, G.; Katsanos, K.H.; Kopylov, U.; Al Sulais, E.; Axelrad, J.E.; Balendran, K.; Burisch, J.; de Ridder, L.; et al. ECCO Guidelines on Inflammatory Bowel Disease and Malignancies. J. Crohn’s Colitis 2023, 17, 827–854. [Google Scholar] [CrossRef]
- Agrawal, M.; Spencer, E.A.; Colombel, J.-F.; Ungaro, R.C. Approach to the Management of Recently Diagnosed Inflammatory Bowel Disease Patients: A User’s Guide for Adult and Pediatric Gastroenterologists. Gastroenterology 2021, 161, 47–65. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J.J.; Green, Z.; Kolimarala, V.; Beattie, R.M. Inflammatory Bowel Disease: Long-Term Therapeutic Challenges. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 1049–1063. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Luo, H.; Tan, D.; Peng, B.; Zhong, Z.; Wang, Y. Holism of Chinese Herbal Medicine Prescriptions for Inflammatory Bowel Disease: A Review Based on Clinical Evidence and Experimental Research. Phytomedicine 2022, 102, 154202. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhou, Q.; Ni, Y.; He, W.; Shen, H.; Zhu, L. Traditional Chinese Medicine for Mild-to-Moderate Ulcerative Colitis: Protocol for a Network Meta-Analysis of Randomized Controlled Trials. Medicine 2019, 98, e16881. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yin, F.; Kong, L.; Yang, L.; Sun, H.; Sun, Y.; Yan, G.; Han, Y.; Wang, X. Chinmedomics: A Potent Tool for the Evaluation of Traditional Chinese Medicine Efficacy and Identification of Its Active Components. Chin. Med. 2024, 19, 47. [Google Scholar] [CrossRef]
- Tang, H.; Huang, W.; Ma, J.; Liu, L. SWOT Analysis and Revelation in Traditional Chinese Medicine Internationalization. Chin. Med. 2018, 13, 5. [Google Scholar] [CrossRef]
- Lu, A.-P.; Jia, H.-W.; Xiao, C.; Lu, Q.-P. Theory of Traditional Chinese Medicine and Therapeutic Method of Diseases. World J. Gastroenterol. 2004, 10, 1854–1856. [Google Scholar] [CrossRef]
- Muluye, R.A.; Bian, Y.; Alemu, P.N. Anti-Inflammatory and Antimicrobial Effects of Heat-Clearing Chinese Herbs: A Current Review. J. Tradit. Complement. Med. 2014, 4, 93–98. [Google Scholar] [CrossRef]
- Lu, L. Study on Prescriptions and Traditional Herbs for Surgical Diseases of Liu Juan Zi Gui Yi Fang. Master’s Thesis, Nanjing University of Chinese Medicine, Nanjing, China, 2018. [Google Scholar]
- Hua, Y.; Jia, Y.; Zhang, X.; Yuan, Z.; Ji, P.; Hu, J.; Wei, Y. Baitouweng Tang Ameliorates DSS-Induced Ulcerative Colitis through the Regulation of the Gut Microbiota and Bile Acids via Pathways Involving FXR and TGR5. Biomed. Pharmacother. 2021, 137, 111320. [Google Scholar] [CrossRef]
- Seo, C.; Lee, H.; Choi, K.; Lim, D.; Ryu, H.; Lee, Y.; Choi, C.; Kim, H. Two Cases of Ulcerative Colitis Diagnosed as Damp-Heat Dysentery Treated with Jakyaktang-gamibang. J. Korean Orient. Intern. Med. 2006, 27, 984–990. [Google Scholar]
- Liu, C. Liu Juanzi Guiyifang; Beijing Science Technology Publishing Co., Ltd.: Beijing, China, 2014; ISBN 978-7-5304-6877-7. [Google Scholar]
- Korea Institute of Oriental Medicine Defining Dictionary for Medicinal Herbs [Korean, “Hanyak Giwon Sajeon”. Published on the Internet. Available online: https://oasis.kiom.re.kr/herblib/hminfo/hbmcod/hbmcodList.do (accessed on 27 May 2024).
- Jang, D.; Ha, Y.; Lee, C.-Y.; Kim, C.-E. Analysis of Symptoms-Herbs Relationships in Shanghanlun Using Text Mining Approach. J. Physiol. Pathol. Korean Med. 2020, 34, 159–169. [Google Scholar] [CrossRef]
- Tal, G. Dendextend: An R Package for Visualizing, Adjusting, and Comparing Trees of Hierarchical Clustering. Bioinformatics 2015, 31, 3718–3720. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, T.H.; Kang, H.-W.; Lee, S.G.; Yang, H.S.; Guk, Y.J.; Lo, I.S.; Jang, H.H.; Lyu, Y.S. Study for correlation between MMPI results and Sasang constitutions, in out-patients of Oriental Neuropsychiatry. Korean Soc. Orient. Neuropsychiatry 2004, 15, 175–185. [Google Scholar]
- Batool, F.; Hennig, C. Clustering with the Average Silhouette Width. Comput. Stat. Data Anal. 2021, 158, 107190. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-24275-0. [Google Scholar]
- Rodríguez-Lago, I.; Ramírez, C.; Merino, O.; Azagra, I.; Maiz, A.; Zapata, E.; Higuera, R.; Montalvo, I.; Fernández-Calderón, M.; Arreba, P.; et al. Early Microscopic Findings in Preclinical Inflammatory Bowel Disease. Dig. Liver Dis. 2020, 52, 1467–1472. [Google Scholar] [CrossRef]
- Song, H.; Zeng, M.; Chen, X.; Chen, X.; Peng, J.; Lin, Y.; Yu, R.; Cai, X.; Peng, Q. Antiulcerogenic Activity of Li-Zhong Decoction on Duodenal Ulcers Induced by Indomethacin in Rats: Involvement of TLR-2/MyD88 Signaling Pathway. Evid. Based Complement. Alternat. Med. 2020, 2020, 6538156. [Google Scholar] [CrossRef]
- Song, H.; Qiu, J.; Yu, C.; Xiong, M.; Ou, C.; Ren, B.; Zhong, M.; Zeng, M.; Peng, Q. Traditional Chinese Medicine Prescription Huang-Qi-Jian-Zhong-Tang Ameliorates Indomethacin-Induced Duodenal Ulcers in Rats by Affecting NF-κB and STAT Signaling Pathways. Biomed. Pharmacother. 2022, 156, 113866. [Google Scholar] [CrossRef]
- Granito, A.; Zauli, D.; Muratori, P.; Muratori, L.; Grassi, A.; Bortolotti, R.; Petrolini, N.; Veronesi, L.; Gionchetti, P.; Bianchi, F.B.; et al. Anti-Saccharomyces Cerevisiae and Perinuclear Anti-Neutrophil Cytoplasmic Antibodies in Coeliac Disease before and after Gluten-Free Diet. Aliment. Pharmacol. Ther. 2005, 21, 881–887. [Google Scholar] [CrossRef]
- Karim, M.R.; Iqbal, S.; Mohammad, S.; Lee, J.H.; Jung, D.; Mathiyalagan, R.; Yang, D.-C.; Yang, D.U.; Kang, S.C. A Review on Impact of Dietary Interventions, Drugs, and Traditional Herbal Supplements on the Gut Microbiome. Microbiol. Res. 2023, 271, 127346. [Google Scholar] [CrossRef]
- Mok, H.L.; Cheng, K.W.; Xu, Y.; Huang, C.; Lyu, C.; Xu, J.; Hu, D.; Zhu, L.; Lin, C.; Tan, H.-Y.; et al. Modified Zhenwu Decoction Suppresses Chronic Colitis via Targeting Macrophage CCR2/Fyn/P38 MAPK Signaling Axis. Phytomedicine 2024, 129, 155694. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.J.; Mustafa, N.; Mashor, M.; Rahman, K.; Wan Muhamad, W.Z.A.; Wai Zhe, L.; Cheor, W.L.; Oung, Q. Understanding Domain Knowledge in Initialization Method for K-Mean Clustering Algorithm in Medical Images. In Proceedings of the 6th International Conference on Electrical, Control and Computer Engineering. Lecture Notes in Electrical Engineering, Kuantan, Malaysia, 23 August 2021; Springer: Singapore, 2022; pp. 805–817, ISBN 9789811686894. [Google Scholar]
- Jia, Y.; Wang, Z.-Z.; Li, X.-M.; Miao, M.-S. Data mining of drug use rules based on traditional Chinese medicine treatment of ulcerative colitis. Zhongguo Zhong Yao Za Zhi 2021, 46, 2594–2600. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Common Major Indications * | Common Major Herbs ** | |
|---|---|---|
| Subset 1 | Diarrhea Coldness Abscess Abscess ruptured | H1 Gan cao, H10 Jie geng, H12 Dan gui, H25 Bai tou weng, H27 Bai shi zhi, H31 Fu zi, H46 Long gu, H49 ren shen, H69 Huang lian |
| Subset 2 | The early phase of the disease Difficulty in defecation Difficulty in urination Fever | H1 Gan cao, H12 Dan gui, H15 Da huang, H42 Sheng ma, H67 Huang qin |
| Subset 3 | Abscess ruptured Deficiency Fever | H1 Gan cao, H4 Gan di huang, H14 Da zao, H19 Mai dong, H30 Fu ling, H36 Sheng jiang, H49 Ren shen, H68 Huang qi |
| Subset 4 | Fever Deficiency Thirst | H1 Gan cao, H12 Dang gui, H30 Fu ling, H37 Sheng di huang, H49 Ren shen, H50 Shao yao, H55 Dan zhu ye, H64 Tong cao, H67 Huang qin, H68 Huang qi |
| Subset 5 | After laxation Difficulty in urination Fever | H1 Gan cao, H6 Gui xin, H12 Dang gui, H19 Mai dong, H41 Xiao mai, H49 Ren shen, H50 Shao yao, H55 Dan zhu ye, H67 Huang qin |
| Subset 6 | Abscess unruptured Abscess Abscess ruptured | H7 Gua lou, H50 Shao yao, H52 Chi xiao dou, H58 Chuan xiong, H68 Huang qi |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.; Jeong, H.; Leem, J. Exploration of Therapeutic Strategies of Herbal Prescriptions for Carbuncle Treatment to Suggest Modern Approaches to Inflammatory Bowel Disease: Cluster and Network Analyses of the Book «Liu Juan Zi Gui Yi Fang». Healthcare 2024, 12, 1499. https://doi.org/10.3390/healthcare12151499
Park D, Jeong H, Leem J. Exploration of Therapeutic Strategies of Herbal Prescriptions for Carbuncle Treatment to Suggest Modern Approaches to Inflammatory Bowel Disease: Cluster and Network Analyses of the Book «Liu Juan Zi Gui Yi Fang». Healthcare. 2024; 12(15):1499. https://doi.org/10.3390/healthcare12151499
Chicago/Turabian StylePark, Dasol, Heonyoung Jeong, and Jungtae Leem. 2024. "Exploration of Therapeutic Strategies of Herbal Prescriptions for Carbuncle Treatment to Suggest Modern Approaches to Inflammatory Bowel Disease: Cluster and Network Analyses of the Book «Liu Juan Zi Gui Yi Fang»" Healthcare 12, no. 15: 1499. https://doi.org/10.3390/healthcare12151499