
Nurses’ Role in Obesity Management in Adults in Primary Healthcare Settings Worldwide: A Scoping Review



Abstract
1. Introduction
Significance
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
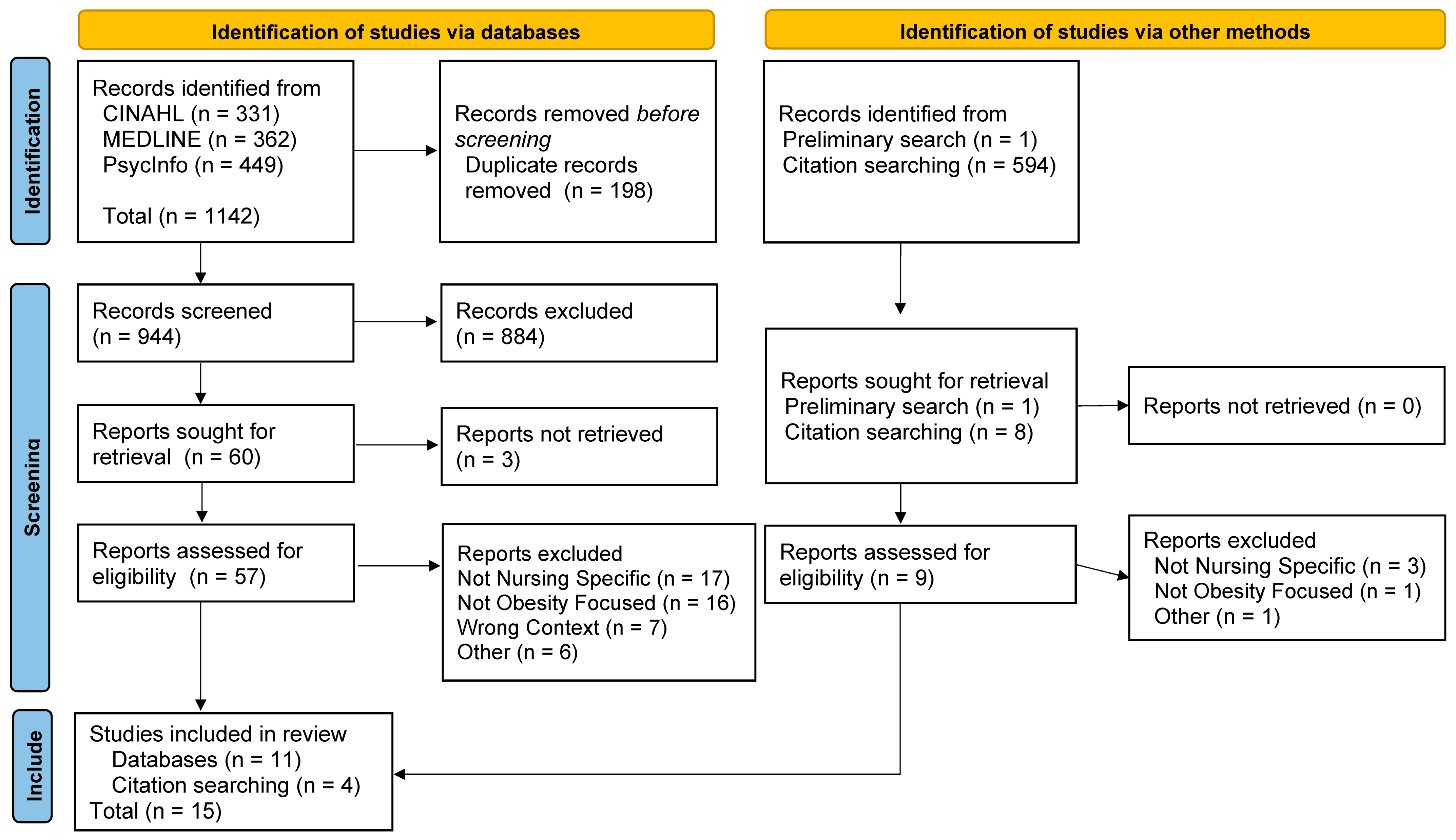
2.5. Selection of Sources of Evidence
2.6. Process of Data Extraction
2.7. Thematic Analysis
3. Results
3.1. Characteristics of the Studies
3.2. Synthesis of Results
3.2.1. Patient-Centred Care
3.2.2. Patient Assessments
3.2.3. Therapeutic Nursing Interventions
3.2.4. Patient Education
3.2.5. Care Management
3.2.6. Professional Development
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wharton, S.; Lau, D.C.W.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Can. Med. Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 April 2024).
- Pray, R.; Riskin, S. The history and faults of the body mass index and where to look next: A literature review. Cureus 2023, 15, e48230. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, C.W.; Fu, Y.Y.; Li, Y.Z.; Chen, L.; Zhang, Q.W.; Chen, Y.F. Global, regional, and national burden of chronic respiratory diseases and associated risk factors, 1990-2019: Results from the Global Burden of Disease Study 2019. Front. Med. 2023, 10, 1066804. [Google Scholar] [CrossRef] [PubMed]
- The British Heart Foundation. Global Heart & Circulatory Diseases Factsheet. Available online: https://www.bhf.org.uk/-/media/files/for-professionals/research/heart-statistics/bhf-cvd-statistics-global-factsheet.pdf (accessed on 10 March 2024).
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef]
- World Obesity Federation. World Obesity Atlas 2024. Available online: https://data.worldobesity.org/publications/?cat=22 (accessed on 10 April 2024).
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Obesity Canada. Health Impacts of Obesity. Available online: https://obesitycanada.ca/understanding-obesity/health-impacts-obesity/ (accessed on 20 November 2023).
- Recalde, M.; Pistillo, A.; Viallon, V.; Fontvieille, E.; Duarte-Salles, T.; Freisling, H. Body mass index and incident cardiometabolic conditions in relation to obesity-related cancer risk: A population-based cohort study in Catalonia, Spain. Cancer Med. 2023, 12, 20188–20200. [Google Scholar] [CrossRef]
- Rueda-Clausen, C.F.; Poddar, M.; Lear, S.A.; Poirier, P.; Sharma, A.M. Canadian Adult Obesity Clinical Practice Guidelines: Assessment of People Living with Obesity. Available online: https://obesitycanada.ca/guidelines/assessment (accessed on 20 November 2023).
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective; Continuous Update Project Expert Report; World Cancer Research Fund International: London, UK, 2018. [Google Scholar]
- Puhl, R.M.; Lessard, L.M.; Himmelstein, M.S.; Foster, G.D. The roles of experienced and internalized weight stigma in healthcare experiences: Perspectives of adults engaged in weight management across six countries. PLoS ONE 2021, 16, e0251566. [Google Scholar] [CrossRef]
- Wu, Y.K.; Berry, D.C. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: A systematic review. J. Adv. Nurs. 2018, 74, 1030–1042. [Google Scholar] [CrossRef]
- World Health Organization. WHO Acceleration Plan to Stop Obesity. Available online: https://www.who.int/publications/i/item/9789240075634 (accessed on 21 November 2023).
- World Health Organization. Declaration of Alma Ata. International Conference on Primary Health Care, Alma-Ata, USSR, 6–12 September 1978. Available online: https://www.who.int/docs/default-source/documents/almaata-declaration-en.pdf (accessed on 12 April 2024).
- World Health Organization. WHO Package of Essential Noncommunicable (WHO PEN) Disease Interventions for Primary Health Care. Available online: https://www.who.int/publications/i/item/9789240009226 (accessed on 21 September 2023).
- Tandan, M.; Dunlea, S.; Cullen, W.; Bury, G. Teamwork and its impact on chronic disease clinical outcomes in primary care: A systematic review and meta-analysis. Public Health 2024, 229, 88–115. [Google Scholar] [CrossRef]
- Semlitsch, T.; Stigler, F.L.; Jeitler, K.; Horvath, K.; Siebenhofer, A. Management of overweight and obesity in primary care-A systematic overview of international evidence-based guidelines. Obes. Rev. 2019, 20, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Griffin, C.D. A Primary Care Nursing Perspective on Chronic Disease Prevention and Management. Del. J. Public Health 2017, 3, 78–83. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Regional Office for Europe. Competencies for Nurses Working in Primary Health Care. Available online: https://iris.who.int/handle/10665/365607 (accessed on 20 March 2024).
- Wilkes, L.; Cioffi, J.; Cummings, J.; Warne, B.; Harrison, K. Clients with chronic conditions: Community nurse role in a multidisciplinary team. J. Clin. Nurs. 2014, 23, 844–855. [Google Scholar] [CrossRef]
- World Health Organization. Nursing and Midwifery. Available online: https://www.who.int/news-room/fact-sheets/detail/nursing-and-midwifery (accessed on 21 September 2023).
- Jackson, S.E.; Wardle, J.; Johnson, F.; Finer, N.; Beeken, R.J. The impact of a health professional recommendation on weight loss attempts in overweight and obese British adults: A cross-sectional analysis. BMJ Open 2013, 3, e003693. [Google Scholar] [CrossRef] [PubMed]
- Bright, D.; Gray, B.J.; Kyle, R.G.; Bolton, S.; Davies, A.R. Factors influencing initiation of health behaviour conversations with patients: Cross-sectional study of nurses, midwives, and healthcare support workers in Wales. J. Adv. Nurs. 2021, 77, 4427–4438. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.; Grech, C.; Hill, K. Health advice and education given to overweight patients by primary care doctors and nurses: A scoping literature review. Prev. Med. Rep. 2019, 14, 100812. [Google Scholar] [CrossRef]
- Warr, W.; Aveyard, P.; Albury, C.; Nicholson, B.; Tudor, K.; Hobbs, R.; Roberts, N.; Ziebland, S. A systematic review and thematic synthesis of qualitative studies exploring GPs’ and nurses’ perspectives on discussing weight with patients with overweight and obesity in primary care. Obes. Rev. 2021, 22, e13151. [Google Scholar] [CrossRef]
- Rust, C.; Prior, R.M.; Stec, M. Implementation of a clinical practice guideline in a primary care setting for the prevention and management of obesity in adults. Nurs. Forum 2020, 55, 485–490. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. JBI Man. Evid. Synth. 2020, 169, 467–473. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Framondi, L.; Di Matteo, R.; Verde, L.; Vetrani, C.; Graziadio, C.; Pugliese, G.; Laudisio, D.; Vitale, G.; Iannicelli, A.; et al. The role of the nurse in the Obesity Clinic: A practical guideline. Panminerva Medica 2021, 63, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Braga, V.A.S.; Jesus, M.C.P.; Conz, C.A.; Silva, M.H.D.; Tavares, R.E.; Merighi, M.A.B. Actions of nurses toward obesity in primary health care units. Rev. Bras. Enferm. 2020, 73, e20180404. [Google Scholar] [CrossRef] [PubMed]
- Brewah, H.; Todhunter, J.; Bades, A.; Colyer, S. Can community nurses take on obesity? J. Community Nurs. 2018, 32, 8–11. [Google Scholar]
- Campbell-Scherer, D.L.; Asselin, J.; Osunlana, A.M.; Ogunleye, A.A.; Fielding, S.; Anderson, R.; Cave, A.; Johnson, J.A.; Sharma, A.M. Changing provider behaviour to increase nurse visits for obesity in family practice: The 5As Team randomized controlled trial. CMAJ Open 2019, 7, E371–E378. [Google Scholar] [CrossRef]
- Fernández-Ruiz, V.E.; Armero-Barranco, D.; Paniagua-Urbano, J.A.; Sole-Agusti, M.; Ruiz-Sánchez, A.; Gómez-Marín, J. Short-medium-long-term efficacy of interdisciplinary intervention against overweight and obesity: Randomized controlled clinical trial. Int. J. Nurs. Pract. 2018, 24, e12690. [Google Scholar] [CrossRef]
- Fernández-Ruiz, V.E.; Paniagua-Urbano, J.A.; Solé-Agustí, M.; Ruiz-Sánchez, A.; Gómez-Marín, J.; Armero-Barranco, D. Impact of the I2AO2 interdisciplinary program led by nursing on psychological comorbidity and quality of life: Randomized controlled clinical trial. Arch. Psychiatr. Nurs. 2018, 32, 268–277. [Google Scholar] [CrossRef]
- Govindasamy, S.; Beek, K.; Yates, K.; Jayasuriya, R.; Reynolds, R.; de Wit, J.B.F.; Harris, M. Experiences of overweight and obese patients with diabetes and practice nurses during implementation of a brief weight management intervention in general practice settings serving Culturally and Linguistically Diverse disadvantaged populations. Aust. J. Prim. Health 2023, 29, 358–364. [Google Scholar] [CrossRef]
- Hinks, S.R. Exploring community nurses’ views on the implementation of a local Weight Management Pathway. Br. J. Community Nurs. 2022, 27, 612–618. [Google Scholar] [CrossRef]
- Kelley, S. The Role of the Faith Community Nurse in Weight Management. J. Christ. Nurs. 2018, 35, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, C.S.; Mussi, F.C.; Santos, C.A.S.d.T.; Lima, M.L.; Ladeia, A.M.T.; Silva, L.C.d.J. Effect of remote nursing monitoring on overweight in women: Clinical trial. Rev. Lat.-Am. De Enferm. 2019, 27, e3129. [Google Scholar] [CrossRef]
- Parker, S.; Tran, A.; Saito, S.; McNamara, C.; Denney-Wilson, E.; Nutbeam, D.; Harris, M.F. Exploring organisational readiness to implement a preventive intervention in Australian general practice for overweight and obese patients: Key learnings from the HeLP-GP trial. Aust. J. Prim. Health 2024, 30, PY23085. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.M.; Barr, M.; Stocks, N.; Denney-Wilson, E.; Zwar, N.; Karnon, J.; Kabir, A.; Nutbeam, D.; Roseleur, J.; Liaw, S.-T.; et al. Preventing chronic disease in overweight and obese patients with low health literacy using eHealth and teamwork in primary healthcare (HeLP-GP): A cluster randomised controlled trial. BMJ Open 2022, 12, e060393. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.M.; Stocks, N.; Nutbeam, D.; Thomas, L.; Denney-Wilson, E.; Zwar, N.; Karnon, J.; Lloyd, J.; Noakes, M.; Liaw, S.-T.; et al. Preventing chronic disease in patients with low health literacy using eHealth and teamwork in primary healthcare: Protocol for a cluster randomised controlled trial. BMJ Open 2018, 8, e023239. [Google Scholar] [CrossRef]
- Shaji, P.; Singh, M.; Sahu, B.; Arulappan, J. Effectiveness of Nurse-led Lifestyle Modification Intervention on Obesity Among Young Women in India. SAGE Open Nurs. 2023, 9, 23779608231186705. [Google Scholar] [CrossRef]
- Virtanen, J.; Penttinen, M.; Kautiainen, H.; Korhonen, P. The impact of lifestyle counselling on weight management and quality of life among working-age females. Scand. J. Prim. Health Care 2021, 39, 382–388. [Google Scholar] [CrossRef]
- Alexander, S.C.; Cox, M.E.; Boling Turer, C.L.; Lyna, P.; Østbye, T.; Tulsky, J.A.; Dolor, R.J.; Pollak, K.I. Do the five A’s work when physicians counsel about weight loss? Fam. Med. 2011, 43, 179–184. [Google Scholar]
- Braga, V.A.S.; Jesus, M.C.P.; Conz, C.A.; Tavares, R.E.; Silva, M.H.D.; Merighi, M.A.B. Nursing interventions with people with obesity in Primary Health Care: An integrative review. Rev. Esc. Enferm. USP 2017, 51, e03293. [Google Scholar] [CrossRef]
- Jay, M.; Gillespie, C.; Schlair, S.; Sherman, S.; Kalet, A. Physicians’ use of the 5As in counseling obese patients: Is the quality of counseling associated with patients’ motivation and intention to lose weight? BMC Health Serv. Res. 2010, 10, 159. [Google Scholar] [CrossRef]
- Ogunleye, A.; Osunlana, A.; Asselin, J.; Cave, A.; Sharma, A.M.; Campbell-Scherer, D.L. The 5As team intervention: Bridging the knowledge gap in obesity management among primary care practitioners. BMC Res. Notes 2015, 8, 810. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation on Obesity; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- European Association for the Study of Obesity. Environmental Scan of Obesity Care Policies and Strategies for Adults in Europe 2020; European Association for the Study of Obesity: London, UK, 2020. [Google Scholar]
- Luli, M.; Yeo, G.; Farrell, E.; Ogden, J.; Parretti, H.; Frew, E.; Bevan, S.; Brown, A.; Logue, J.; Menon, V.; et al. The implications of defining obesity as a disease: A report from the Association for the Study of Obesity 2021 annual conference. EClinicalMedicine 2023, 58, 101962. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. Executive Summary. NHLBI Obesity Education Initiative Expert Panel. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2008/ (accessed on 17 July 2024).
- Allison, D.B.; Downey, M.; Atkinson, R.L.; Billington, C.J.; Bray, G.A.; Eckel, R.H.; Finkelstein, E.A.; Jensen, M.D.; Tremblay, A. Obesity as a disease: A white paper on evidence and arguments commissioned by the Council of the Obesity Society. Obesity 2008, 16, 1161–1177. [Google Scholar] [CrossRef] [PubMed]
- American Medical Association. Proceedings of the 2013 Annual Meeting of the House of Delegates. 162nd Annual Meeting; AMA: Chicago, IL, USA, 2013. Available online: https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/hod/a13-resolutions_0.pdf (accessed on 12 July 2024).
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- Burki, T. European Commission classifies obesity as a chronic disease. Lancet Diabetes Endocrinol. 2021, 9, 418. [Google Scholar] [CrossRef] [PubMed]
- Tham, K.W.; Abdul Ghani, R.; Cua, S.C.; Deerochanawong, C.; Fojas, M.; Hocking, S.; Lee, J.; Nam, T.Q.; Pathan, F.; Saboo, B.; et al. Obesity in South and Southeast Asia-A new consensus on care and management. Obes. Rev. 2023, 24, e13520. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Gratteri, S.; Gualtieri, P.; Cammarano, A.; Bertucci, P.; Di Renzo, L. Why primary obesity is a disease? J. Transl. Med. 2019, 17, 169. [Google Scholar] [CrossRef]
- Heshka, S.; Allison, D.B. Is obesity a disease? Int. J. Obes. 2001, 25, 1401–1404. [Google Scholar] [CrossRef]
- Stunkard, A.J. Current views on obesity. Am. J. Med. 1996, 100, 230–236. [Google Scholar] [CrossRef]
- Vallgårda, S.; Nielsen, M.E.J.; Hansen, A.K.K.; Cathaoir, K.Ó.; Hartlev, M.; Holm, L.; Christensen, B.J.; Jensen, J.D.; Sørensen, T.I.A.; Sandøe, P. Should Europe follow the US and declare obesity a disease?: A discussion of the so-called utilitarian argument. Eur. J. Clin. Nutr. 2017, 71, 1263–1267. [Google Scholar] [CrossRef]
- Aboueid, S.; Ahmed, R.; Jasinska, M.; Pouliot, C.; Hermosura, B.J.; Bourgeault, I.; Giroux, I. Weight Communication: How Do Health Professionals Communicate about Weight with Their Patients in Primary Care Settings? Health Commun. 2022, 37, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Smolowitz, J.; Speakman, E.; Wojnar, D.; Whelan, E.M.; Ulrich, S.; Hayes, C.; Wood, L. Role of the registered nurse in primary health care: Meeting health care needs in the 21st century. Nurs. Outlook 2015, 63, 130–136. [Google Scholar] [CrossRef]
- Davis, K.M.; Eckert, M.C.; Hutchinson, A.; Harmon, J.; Sharplin, G.; Shakib, S.; Caughey, G.E. Effectiveness of nurse–led services for people with chronic disease in achieving an outcome of continuity of care at the primary-secondary healthcare interface: A quantitative systematic review. Int. J. Nurs. Stud. 2021, 121, 103986. [Google Scholar] [CrossRef] [PubMed]
- Holloway, D.; James, S.; Ekinci, E.; Craft, J. Systematic review of the effectiveness of nurse-led care in reducing glycated haemoglobin in adults with Type 1 or 2 diabetes. Int. J. Nurs. Pract. 2023, 29, e13135. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.-H.; Wang, H.-S.; Liu, N. The evaluation of a nurse-led hypertension management model in an urban community healthcare: A randomized controlled trial. Medicine 2020, 99, e20967. [Google Scholar] [CrossRef]
- Herrmann-Werner, A.; Loda, T.; Wiesner, L.M.; Erschens, R.S.; Junne, F.; Zipfel, S. Is an obesity simulation suit in an undergraduate medical communication class a valuable teaching tool? A cross-sectional proof of concept study. BMJ Open 2019, 9, e029738. [Google Scholar] [CrossRef]
- Mayer-Brown, S.; Basch, M.C.; Robinson, M.E.; Janicke, D.M. Impact of child and maternal weight on healthcare trainee clinical assessment decision making: A virtual human study. Child. Obes. 2019, 15, 63–70. [Google Scholar] [CrossRef]
- Tanneberger, A.; Ciupitu-Plath, C. Nurses’ Weight Bias in Caring for Obese Patients: Do Weight Controllability Beliefs Influence the Provision of Care to Obese Patients? Clin. Nurs. Res. 2018, 27, 414–432. [Google Scholar] [CrossRef]
- Ryan, L.; Coyne, R.; Heary, C.; Birney, S.; Crotty, M.; Dunne, R.; Conlan, O.; Walsh, J.C. Weight stigma experienced by patients with obesity in healthcare settings: A qualitative evidence synthesis. Obes. Rev. 2023, 24, e13606. [Google Scholar] [CrossRef]
- Telo, G.H.; Friedrich Fontoura, L.; Avila, G.O.; Gheno, V.; Bertuzzo Brum, M.A.; Teixeira, J.B.; Erthal, I.N.; Alessi, J.; Telo, G.H. Obesity bias: How can this underestimated problem affect medical decisions in healthcare? A systematic review. Obes. Rev. 2024, 25, e13696. [Google Scholar] [CrossRef]
- Garcia, J.T.; Amankwah, E.K.; Hernandez, R.G. Assessment of Weight Bias Among Pediatric Nurses and Clinical Support Staff Toward Obese Patients and Their Caregivers. J. Pediatr. Nurs. 2016, 31, e244–e251. [Google Scholar] [CrossRef] [PubMed]
- McHale, C.T.; Laidlaw, A.H.; Cecil, J.E. Primary care patient and practitioner views of weight and weight-related discussion: A mixed-methods study. BMJ Open 2020, 10, e034023. [Google Scholar] [CrossRef] [PubMed]
- Ringel, M.M.; Ditto, P.H. The moralization of obesity. Soc. Sci. Med. 2019, 237, 112399. [Google Scholar] [CrossRef]
- Torres-Carot, V.; Suárez-González, A.; Lobato-Foulques, C. The energy balance hypothesis of obesity: Do the laws of thermodynamics explain excessive adiposity? Eur. J. Clin. Nutr. 2022, 76, 1374–1379. [Google Scholar] [CrossRef]
- Masood, B.; Moorthy, M. Causes of obesity: A review. Clin. Med. 2023, 23, 284–291. [Google Scholar] [CrossRef]
- Sternson, S.M.; Eiselt, A.K. Three Pillars for the Neural Control of Appetite. Annu. Rev. Physiol. 2017, 79, 401–423. [Google Scholar] [CrossRef] [PubMed]
- Kanmiki, E.W.; Fatima, Y.; Mamun, A.A. Multigenerational transmission of obesity: A systematic review and meta-analysis. Obes. Rev. 2022, 23, e13405. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Kumar, P.; Fahmi, N.; Garg, B.; Dutta, S.; Sachar, S.; Matharu, A.S.; Vimaleswaran, K.S. Endocrine disruption and obesity: A current review on environmental obesogens. Curr. Res. Green Sustain. Chem. 2020, 3, 100009. [Google Scholar] [CrossRef]
- Safaei, M.; Sundararajan, E.A.; Driss, M.; Boulila, W.; Shapi’i, A. A systematic literature review on obesity: Understanding the causes & consequences of obesity and reviewing various machine learning approaches used to predict obesity. Comput. Biol. Med. 2021, 136, 104754. [Google Scholar] [CrossRef]
- Mojkowska, A.; Sobczak, K.; Leoniuk, K.; Henzler, M.; Jackowski, M. Medical or Common Knowledge? Knowledge of Medical Professionals on Obesity Diagnosis Criteria and Treatment. Obes. Facts 2023, 16, 216–223. [Google Scholar] [CrossRef]
- Vallis, M.; Piccinini-Vallis, H.; Sharma, A.M.; Freedhoff, Y. Clinical review: Modified 5 As: Minimal intervention for obesity counseling in primary care. Can. Fam. Physician 2013, 59, 27–31. [Google Scholar] [PubMed]
- Rueda-Clausen, C.F.; Benterud, E.; Bond, T.; Olszowka, R.; Vallis, M.T.; Sharma, A.M. Effect of implementing the 5As of obesity management framework on provider-patient interactions in primary care. Clin. Obes. 2014, 4, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.M. M, M, M & M: A mnemonic for assessing obesity. Obes. Rev. 2010, 11, 808–809. [Google Scholar] [CrossRef] [PubMed]
- Berring, L.L.; Holm, T.; Hansen, J.P.; Delcomyn, C.L.; Søndergaard, R.; Hvidhjelm, J. Implementing Trauma-Informed Care—Settings, Definitions, Interventions, Measures, and Implementation across Settings: A Scoping Review. Healthcare 2024, 12, 908. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Inclusion | Exclusion | |
|---|---|---|
| Population | Registered nurses Case management nurses General practice nurses | Student nurses Advanced practice nurses Nurse practitioner (NP) Clinical nurse specialist (CNS) Certified Registered Nurse Anesthetist (CRNA) Certified Nurse Midwife (CNM) |
| Concept | Individuals with obesity Adults (19–64 years old) Nurses’ role or intervention | RN’s role indecipherable from other disciplines Primary focus on other disease (e.g., cancer, serious mental illness, NAFLD, T2DM, etc.) Bariatric and pharmaceutical related interventions Population who requires expertise beyond scope of this paper (i.e., perinatal, postnatal, prenatal, and parenting and people with developmental, and intellectual disabilities) |
| Context | Worldwide Primary healthcare setting District nursing General practice Community settings (home care, occupational health, or faith-based) | Any setting outside inclusion criteria |
| Medical Subject Headings (MeSHs) and Descriptors | String/ Boolean | Keywords (Title or Abstract) | |
|---|---|---|---|
| Population | “nurses” OR “nursing” OR “Public Health Service Nurses” | Or | nurs* |
| And | |||
| Concept | “role” OR “Nursing Role” OR “Nursing Interventions” OR “Professional Role” OR “Delivery of Health Care” OR “Practice Patterns, Nurses” OR | Or | role* or “nurs* intervention*” OR “nurs* strateg*” OR “nurs* role” OR “nurs* guided” OR “nurse-directed” OR “nurse-led” OR “nurse-managed” OR “nurs* function*” |
| And | |||
| “obesity” OR “Obesity, Morbid” OR “weight control” OR “Weight Reduction Programs” OR “weight management” OR “obesity management” OR “Body Weight Maintenance” OR “Body Weight Changes” OR “weight loss+” OR “Weight Reduction Programs+” OR “Body Weight” OR “overweight” OR “body mass index” OR “Obesity (Attitudes Toward)” | Or | obes* OR “high BMI” OR “high body mass index” OR “weight control” OR “weight reduction” OR “weight management” OR “overweight” | |
| Context | Omitted (too restrictive) | Omitted (too restrictive) | |
| Frist Author/Year/Citation | Title | Study Design | Population | Setting | Country | |
|---|---|---|---|---|---|---|
| Barrea (2021) [34] | The role of the nurse in the obesity clinic: a practical guideline. | Review | RNs caring for people living with obesity (PwO) | Outpatient obesity clinics | Italy | |
| Braga (2020) [35] | Actions of nurses toward obesity in primary health care units. | Qualitative | Primary healthcare nurses (PHNs) | Primary healthcare Units | Brazil | |
| Brewah (2018) [36] | Can community nurses take on obesity? | Commentary | District/ community RNs caring for homebound PwO | Home care | U.K. | |
| Campbell- Scherer (2019) [37] | Changing provider behaviour to increase nurse visits for obesity in family practice: the 5As Team randomized controlled trial (RCT). | Mixed-methods, RCT, and qualitative | Chronic disease RNs in a primary care clinic providing care for PwO | Primary care network clinics | Canada | |
| Fernández- Ruiz (2018) [38] | Short-medium-long-term efficacy of interdisciplinary intervention against overweight and obesity: randomized controlled clinical trial. | RCT | Multidisciplinary program for PwO led and coordinated by RNs | Community care centre | Spain | |
| Fernández- Ruiz (2018) [39] | Impact of the I(2)AO(2) interdisciplinary program led by nursing on psychological comorbidity and quality of life: randomized controlled clinical trial. | RCT | Multidisciplinary program for PwO led and coordinated by RNs | Community care centre | Spain | |
| Govindasamy (2023) [40] | Experiences of overweight and obese patients with diabetes and practice nurses during implementation of a brief weight management intervention in general practice settings serving culturally and linguistically diverse disadvantaged populations. | Qualitative | RNs PwO who are culturally and linguistically diverse with socioeconomic disadvantage | General practice office | Australia | |
| Hinks (2022) [41] | Exploring community nurses’ views on the implementation of a local weight management pathway. | Qualitative | District and community RNs | Community care | Isle of Man | |
| Kelley (2018) [42] | The role of the faith community nurse in weight management. | Opinion | Faith community RNs providing care for PwO | Faith community setting (church) | USA | |
| Palmeira (2019) [43] | Effect of remote nursing monitoring on overweight in women: clinical trial. | RCT | RNs providing remote weight monitoring for PwO | Primary care Remote nursing | Brazil | |
| Parker | 2018 [46] | Preventing chronic disease in patients with low health literacy using eHealth and teamwork in primary healthcare: protocol for a cluster randomised controlled trial. | Protocol | RNs caring for PwO | General practice | Australia |
| 2022 [45] | Preventing chronic disease in overweight and obese patients with low health literacy using eHealth and teamwork in primary healthcare (HeLP-GP): a cluster randomised controlled trial. | RCT | RNs caring for PwO | General practice | Australia | |
| 2024 [44] | Exploring organisational readiness to implement a preventive intervention in Australian general practice for overweight and obese patients: key learnings from the HeLP-GP trial. | Qualitative | RNs caring for PwO | General practice | Australia | |
| Shaji et al. (2023) [47] | Effectiveness of nurse-led lifestyle modification intervention on obesity among young women in India. | Quantitative | RN caring for PwO | General practice office and telehealth | India | |
| Virtanen (2021) [48] | The impact of lifestyle counselling on weight management and quality of life among working-age females. | Quantitative cohort study | RNs caring for PwO | Primary healthcare | Finland | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piwowarczyk, E.; MacPhee, M.; Howe, J. Nurses’ Role in Obesity Management in Adults in Primary Healthcare Settings Worldwide: A Scoping Review. Healthcare 2024, 12, 1700. https://doi.org/10.3390/healthcare12171700
Piwowarczyk E, MacPhee M, Howe J. Nurses’ Role in Obesity Management in Adults in Primary Healthcare Settings Worldwide: A Scoping Review. Healthcare. 2024; 12(17):1700. https://doi.org/10.3390/healthcare12171700
Chicago/Turabian StylePiwowarczyk, Emilia, Maura MacPhee, and Jo Howe. 2024. "Nurses’ Role in Obesity Management in Adults in Primary Healthcare Settings Worldwide: A Scoping Review" Healthcare 12, no. 17: 1700. https://doi.org/10.3390/healthcare12171700
APA StylePiwowarczyk, E., MacPhee, M., & Howe, J. (2024). Nurses’ Role in Obesity Management in Adults in Primary Healthcare Settings Worldwide: A Scoping Review. Healthcare, 12(17), 1700. https://doi.org/10.3390/healthcare12171700