
How Are Diagnosis-Related Groups and Staffing Allocation Systems Associated with the Complexity of Nursing Care? An Observational Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. Variables and Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Y.; Wang, G.; Qin, T.-G.; Kobayashi, S.; Karako, T.; Song, P. Comparison of Diagnosis-Related Groups (DRG)-Based Hospital Payment System Design and Implementation Strategies in Different Countries: The Case of Ischemic Stroke. Biosci. Trends 2024, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pirson, M.; Delo, C.; Di Pierdomenico, L.; Laport, N.; Biloque, V.; Leclercq, P. Variability of Nursing Care by APR-DRG and by Severity of Illness in a Sample of Nine Belgian Hospitals. BMC Nurs. 2013, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.; Kocic, S.; Jakovljevic, M. Review of Diagnosis-Related Group-Based Financing of Hospital Care. Health Serv. Res. Manag. Epidemiol. 2016, 3, 2333392816647892. [Google Scholar] [CrossRef] [PubMed]
- Russo, S. Economia e Management Delle Aziende Sanitarie Pubbliche: Profili Evolutivi, Assetto Istituzionale e Performance; CEDAM: Milano, Italy, 2013; ISBN 8813328540. [Google Scholar]
- Nonis, M.; Bertinato, L.; Arcangeli, L.; Cadeddu, C.; Palinuro, A.; Frattura, L.; Merlino, G.; Verdini, E.; Lispi, L.; Ricciardi, W. The Evolution of Drg System in Italy: The It-Drg Project. Eur. J. Public Health 2018, 28, cky218-09. [Google Scholar] [CrossRef]
- Nonis, M.; Rosati, E. Guida Ai DRG. Manuale Pratico per Il Corretto Utilizzo Della Versione 24.0 Del Sistema DRG e Della Corrispondente ICD-9-CM 2007; Istituto Poligrafico e Zecca dello Stato: Roma, Italy, 2008. [Google Scholar]
- Welton, J.M.; Zone-Smith, L.; Fischer, M.H. Adjustment of Inpatient Care Reimbursement for Nursing Intensity. Policy Politics Nurs. Pract. 2006, 7, 270–280. [Google Scholar] [CrossRef]
- Welton, J.M.; Halloran, E.J. Nursing Diagnoses, Diagnosis-Related Group, and Hospital Outcomes. J. Nurs. Adm. 2005, 35, 541–549. [Google Scholar] [CrossRef]
- Knauf, R.A.; Ballard, K.; Mossman, P.N.; Lichtig, L.K. Nursing Cost by DRG: Nursing Intensity Weights. Policy Politics Nurs. Pract. 2006, 7, 281–289. [Google Scholar] [CrossRef]
- You, L.; Aiken, L.H.; Sloane, D.M.; Liu, K.; He, G.; Hu, Y.; Jiang, X.; Li, X.; Li, X.; Liu, H.; et al. Hospital Nursing, Care Quality, and Patient Satisfaction: Cross-Sectional Surveys of Nurses and Patients in Hospitals in China and Europe. Int. J. Nurs. Stud. 2013, 50, 154–161. [Google Scholar] [CrossRef]
- Ball, J.E.; Bruyneel, L.; Aiken, L.H.; Sermeus, W.; Sloane, D.M.; Rafferty, A.M.; Lindqvist, R.; Tishelman, C.; Griffiths, P. Post-Operative Mortality, Missed Care and Nurse Staffing in Nine Countries: A Cross-Sectional Study. Int. J. Nurs. Stud. 2018, 78, 10–15. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van Den Heede, K.; Griffiths, P.; Busse, R.; Diomidous, M.; Kinnunen, J.; Kózka, M.; Lesaffre, E.; et al. Nurse Staffing and Education and Hospital Mortality in Nine European Countries: A Retrospective Observational Study. Lancet 2014, 383, 1824–1830. [Google Scholar] [CrossRef]
- Hessels, A.J.; Paliwal, M.; Weaver, S.H.; Siddiqui, D.; Wurmser, T.A. Impact of Patient Safety Culture on Missed Nursing Care and Adverse Patient Events. J. Nurs. Care Qual. 2019, 34, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Cimiotti, J.P.; Sloane, D.M.; Smith, H.L.; Flynn, L.; Neff, D.F. Effects of Nurse Staffing and Nurse Education on Patient Deaths in Hospitals with Different Nurse Work Environments. Med. Care 2011, 49, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sermeus, W.; Van Den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient Safety, Satisfaction, and Quality of Hospital Care: Cross Sectional Surveys of Nurses and Patients in 12 Countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef]
- Ausili, D.; Bernasconi, D.P.; Rebora, P.; Prestini, L.; Beretta, G.; Ferraioli, L.; Cazzaniga, A.; Valsecchi, M.G.; Di Mauro, S. Complexity of Nursing Care at 24 h from Admission Predicts In-Hospital Mortality in Medical Units: A Cohort Study. BMC Health Serv. Res. 2020, 20, 181. [Google Scholar] [CrossRef]
- Griffiths, P.; Saville, C.; Ball, J.; Jones, J.; Pattison, N.; Monks, T. Nursing Workload, Nurse Staffing Methodologies and Tools: A Systematic Scoping Review and Discussion. Int. J. Nurs. Stud. 2020, 103, 103487. [Google Scholar] [CrossRef]
- The Shelford Group Safer Nursing Care Tool Implementation Resource Pack. Available online: https://shelfordgroup.org/safer-nursing-care-tool/ (accessed on 26 September 2024).
- Regione Lombardia Delibera Giunta Regionale Lombardia 6 Agosto 1998—n. 6/38133. “Definizione Di Requisiti e Indicatori per l’accreditamento Delle Strutture Sanitarie” 1998. Available online: https://cdn.onb.it/2013/11/dgr1998_38133.pdf (accessed on 26 September 2024).
- Galimberti, S.; Rebora, P.; Di Mauro, S.; D’Ilio, I.; Viganò, R.; Moiset, C.; Valsecchi Maria, G. The SIPI for Measuring Complexity in Nursing Care: Evaluation Study. Int. J. Nurs. Stud. 2012, 49, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Balan, T.A.; Putter, H. A Tutorial on Frailty Models. Stat. Methods Med. Res. 2020, 29, 3424–3454. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, F.; Vellone, E.; Cocchieri, A.; Welton, J.; Maurici, M.; Polistena, B.; Spandonaro, F.; Zega, M.; Alvaro, R.; Sanson, G. Nursing Diagnoses as Predictors of Hospital Length of Stay: A Prospective Observational Study. J. Nurs. Sch. 2019, 51, 96–105. [Google Scholar] [CrossRef]
- Thompson, J.D. The Measurement of Nursing Intensity. Health Care Financ. Rev. 1984, 1984, 47. [Google Scholar]
- Welton, J.M.; Harper, E.M. Measuring Nursing Care Value. Nurs. Econ. 2016, 34, 7–14. [Google Scholar] [PubMed]
- Needleman, J. The Economic Case for Fundamental Nursing Care. Nurs. Leadersh. 2016, 29, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Ausserhofer, D.; Zander, B.; Busse, R.; Schubert, M.; De Geest, S.; Rafferty, A.M.; Ball, J.; Scott, A.; Kinnunen, J.; Heinen, M.; et al. Prevalence, Patterns and Predictors of Nursing Care Left Undone in European Hospitals: Results from the Multicountry Cross-Sectional RN4CAST Study. BMJ Qual. Saf. 2014, 23, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Fagerström, L.; Kinnunen, M.; Saarela, J. Nursing Workload, Patient Safety Incidents and Mortality: An Observational Study from Finland. BMJ Open 2018, 8, e016367. [Google Scholar] [CrossRef] [PubMed]
- Bruyneel, L.; Li, B.; Ausserhofer, D.; Lesaffre, E.; Dumitrescu, I.; Smith, H.L.; Sloane, D.M.; Aiken, L.H.; Sermeus, W. Organization of Hospital Nursing, Provision of Nursing Care, and Patient Experiences with Care in Europe. Med. Care Res. Rev. 2015, 72, 643–664. [Google Scholar] [CrossRef]
- Twigg, D.; Duffield, C.; Thompson, P.L.; Rapley, P. The Impact of Nurses on Patient Morbidity and Mortality—The Need for a Policy Change in Response to the Nursing Shortage. Aust. Health Rev. 2010, 34, 312–316. [Google Scholar] [CrossRef]
- Sanson, G.; Vellone, E.; Kangasniemi, M.; Alvaro, R.; D’Agostino, F. Impact of Nursing Diagnoses on Patient and Organisational Outcomes: A Systematic Literature Review. J. Clin. Nurs. 2017, 26, 3764–3783. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Median [IQR] or N (%) | SIPI < 50 (N = 3950) Median [IQR] or N (%) | SIPI ≥ 50 (N = 2922) Median [IQR] or N (%) |
|---|---|---|---|
| Age, years | 76 [64, 84] | 70.5 [57, 79] | 81 [73, 87] |
| Biological Sex | |||
| M | 3647 (53.1) | 1717 (43.5) | 1508 (51.6) |
| F | 3225 (46.9) | 2233 (56.5) | 1414 (48.4) |
| Ward | |||
| Low intensity | 4530 (65.9) | 1373 (34.8) | 969 (33.2) |
| Medium intensity | 2342 (34.1) | 2577 (65.2) | 1953 (66.8) |
| Access | |||
| Ordinary | 573 (8.3) | 496 (12.6) | 77 (2.6) |
| Emergency | 6299 (91.7) | 3454 (87.4) | 2845 (97.4) |
| CCI | |||
| 0 | 1677 (24.4) | 1110 (28.1) | 568 (19.4) |
| 1 | 3408 (49.6) | 1770 (44.8) | 1232 (42.2) |
| 2 | 1355 (19.7) | 871 (22.1) | 803 (27.5) |
| 3 | 380 (5.5) | 175 (4.4) | 273 (9.3) |
| ≥4 | 52 (0.7) | 24 (0.6) | 46 (1.6) |
| SIPI | 42.70 [23.40, 68.80] | 26.10 [16.20, 37.58] | 71.40 [61.70, 81.10] |
| ≥50 | 3950 (57.5) | ||
| <50 | 2922 (42.5) | ||
| DRG rate, EUR | 3325 [2445, 4145] | 3285 [2298, 4052] | 3536 [2805, 4278] |
| Nurse staffing, minutes per patient per day (Clinical Unit) | |||
| 120 (Medicine) | 1649 (24.0) | 722 (18.3) | 927 (31.7) |
| 180 (Nefrology, Oncology, SOAP) | 4409 (64.2) | 2638 (66.8) | 1771 (60.6) |
| 240 (Infectious Diseases) | 814 (11.8) | 590 (14.9) | 224 (7.7) |
| Length of stay at discharge, days | 11 [7, 18] | 9 [6, 15] | 13 [8, 21] |
| Death during hospital stay | 469 (6.8) | 74 (1.9) | 395 (13.5) |
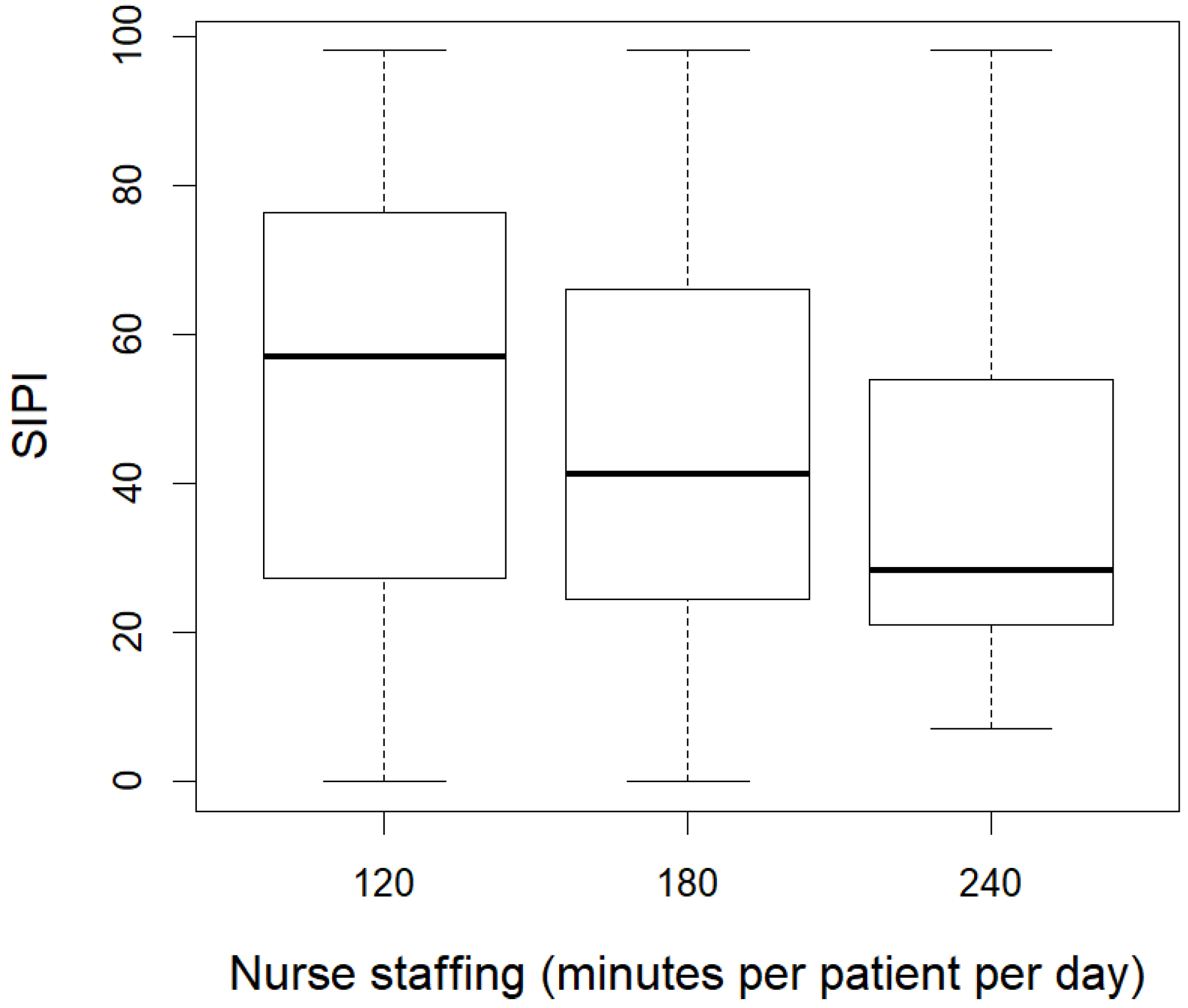
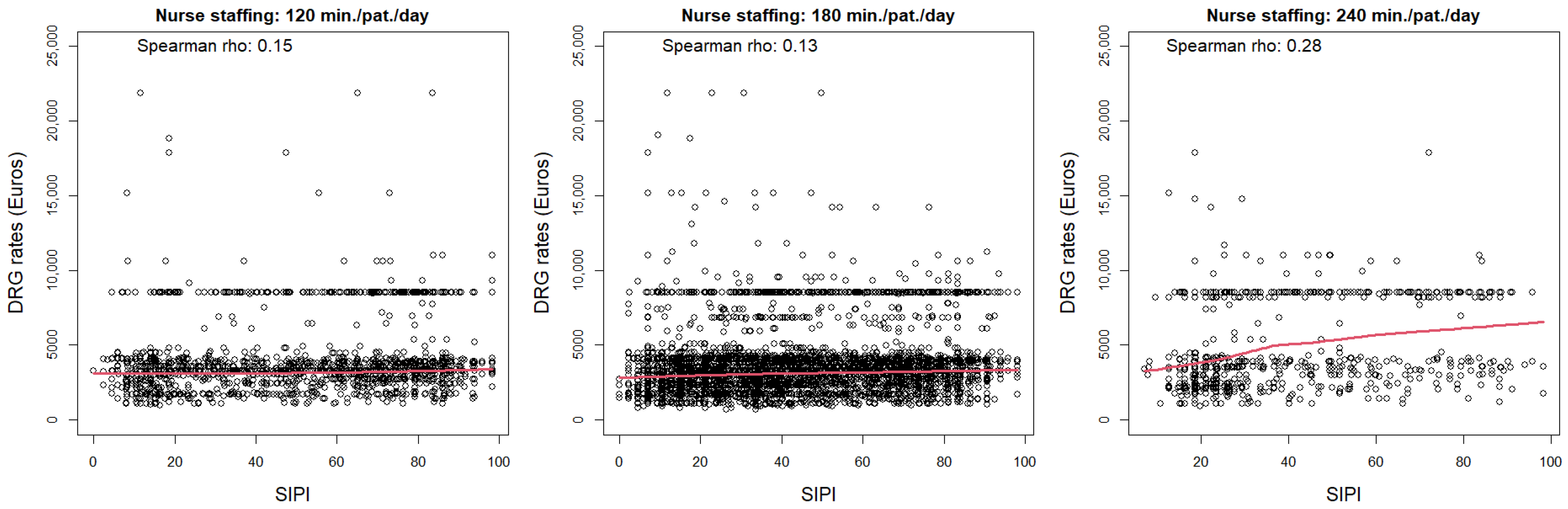
| Variables | Nurse Staffing in Minutes per Patient per Day (Clinical Unit) | ||
|---|---|---|---|
| 120 (Medicine) N = 1649 Median [IQR] or N (%) | 180 (Nefrology, Oncology, SOAP) N = 4409 Median [IQR] or N (%) | 240 (Infectious Diseases) N = 814 Median [IQR] or N (%) | |
| Age, years | 81 [73, 87] | 75 [65, 83] | 57 [42, 73] |
| Biological Sex | |||
| M | 841 (51.0) | 2077 (47.1) | 307 (37.7) |
| F | 808 (49.0) | 2332 (52.9) | 507 (62.3) |
| Ward | |||
| Medium intensity | 0 (0.0) | 2342 (53.1) | 0 (0.0) |
| Low intensity | 1649 (100.0) | 2067 (46.9) | 814 (100.0) |
| Access | |||
| Ordinary | 45 (2.7) | 511 (11.6) | 17 (2.1) |
| Emergency | 1604 (97.3) | 3898 (88.4) | 797 (97.9) |
| CCI | |||
| 0 | 377 (22.9) | 894 (20.3) | 407 (50.0) |
| 1 | 635 (38.5) | 2110 (47.9) | 257 (31.6) |
| 2 | 456 (27.7) | 1100 (24.9) | 118 (14.5) |
| 3 | 158 (9.6) | 260 (5.9) | 30 (3.7) |
| ≥4 | 23 (1.4) | 45 (1.0) | 2 (0.2) |
| SIPI | 57.00 [27.40, 76.50] | 41.30 [24.60, 66.10] | 28.30 [21.00, 53.88] |
| SIPI ≥50 | 722 (43.8) | 2638 (59.8) | 590 (72.5) |
| SIPI <50 | 927 (56.2) | 1771 (40.2) | 224 (27.5) |
| DRG rate, EUR | 3298 [2734, 4052] | 3285 [2437, 4145] | 3536 [2445, 8534] |
| Length of stay at discharge, days | 14 [10, 21] | 9 [6, 15] | 10 [6, 19] |
| Death during hospital stay | 126 (7.6) | 312 (7.1) | 31 (3.8) |
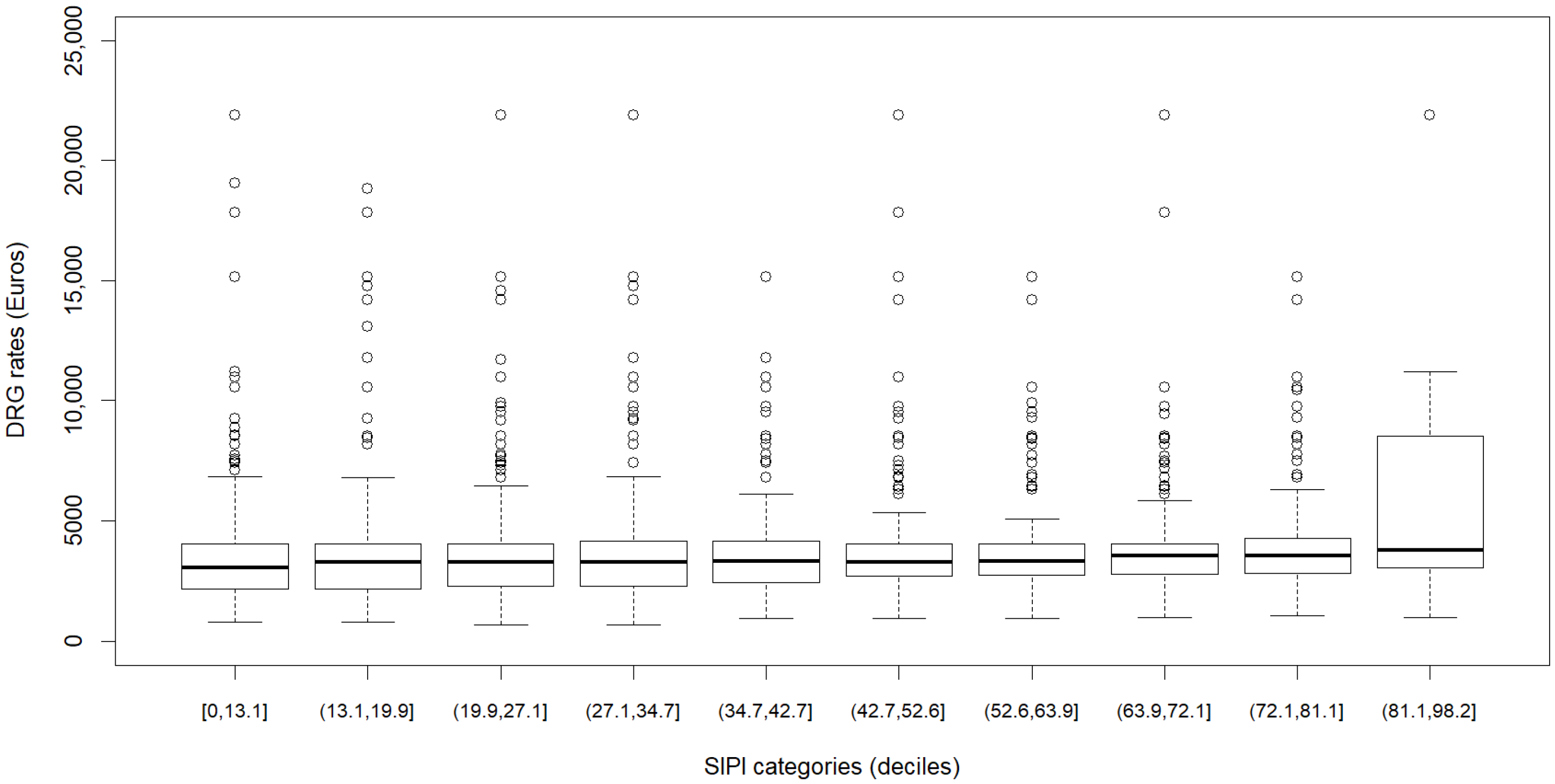
| SIPI Categories (Deciles) | DRG Rates, EUR (Median [IQR]) |
|---|---|
| [0, 13.1] | 3063 [2170, 4052] |
| (13.1, 19.9] | 3285 [2184, 4052] |
| (19.9, 27.1] | 3285 [2298, 4052] |
| (27.1, 34.7] | 3285 [2298, 4145] |
| (34.7, 42.7] | 3325 [2445, 4154] |
| (42.7, 52.6] | 3285 [2701, 4052] |
| (52.6, 63.9] | 3311 [2734, 4052] |
| (63.9, 72.1] | 3536 [2792, 4052] |
| (72.1, 81.1] | 3536 [2802, 4278] |
| (81.1, 98.2] | 3791 [3063, 8534] |
| Factors | Unadjusted (N = 6872) | Adjusted (N = 6872) | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age, per 10 years | 1.483 (1.363; 1.613) | <0.001 | 1.281 (1.164; 1.410) | <0.001 |
| Gender, Male vs. Female | 1.050 (0.875; 1.260) | 0.640 | 1.208 (1.001; 1.458) | 0.049 |
| Ward, Medium Intensity vs. Low | 1.612 (1.333; 1.949) | <0.001 | 1.262 (0.992; 1.605) | 0.058 |
| Access, Emergency vs. Ordinary | 5.037 (2.086; 12.160) | <0.001 | 3.553 (1.437; 8.786) | 0.006 |
| CCI, 1 vs. 0 | 1.609 (1.238; 2.091) | <0.001 | 1.411 (1.077; 1.848) | 0.012 |
| CCI, ≥2 vs. 0 | 1.654 (1.252; 2.186) | <0.001 | 1.396 (1.061; 1.836) | 0.017 |
| SIPI > 50, vs. ≤50 at ≤10 days since admission | 7.907 (5.450; 11.473) | <0.001 | 6.222 (4.254; 9.100) | <0.001 |
| SIPI > 50, vs. ≤50 at >10 days since admission | 2.868 (2.048; 4.016) | <0.001 | 2.456 (1.741; 3.464) | <0.001 |
| DRG rates, per EUR 1000 | 1.007 (0.995; 1.019) | 0.280 | 1.018 (1.004; 1.032) | 0.014 |
| Nurse staffing, minutes per patient per day 180 vs. 120 | 1.347 (1.094; 1.658) | 0.005 | 1.545 (1.197; 1.994) | 0.008 |
| Nurse staffing, minutes per patient per day 240 vs. 120 | 0.627 (0.423; 0.929) | 0.020 | 1.091 (0.727; 1.636) | 0.670 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabrizi, D.; Bernasconi, D.; Locatelli, G.; Luciani, M.; Beretta, G.; Di Mauro, S.; Rebora, P.; Ausili, D. How Are Diagnosis-Related Groups and Staffing Allocation Systems Associated with the Complexity of Nursing Care? An Observational Study. Healthcare 2024, 12, 1988. https://doi.org/10.3390/healthcare12191988
Fabrizi D, Bernasconi D, Locatelli G, Luciani M, Beretta G, Di Mauro S, Rebora P, Ausili D. How Are Diagnosis-Related Groups and Staffing Allocation Systems Associated with the Complexity of Nursing Care? An Observational Study. Healthcare. 2024; 12(19):1988. https://doi.org/10.3390/healthcare12191988
Chicago/Turabian StyleFabrizi, Diletta, Davide Bernasconi, Giulia Locatelli, Michela Luciani, Giorgio Beretta, Stefania Di Mauro, Paola Rebora, and Davide Ausili. 2024. "How Are Diagnosis-Related Groups and Staffing Allocation Systems Associated with the Complexity of Nursing Care? An Observational Study" Healthcare 12, no. 19: 1988. https://doi.org/10.3390/healthcare12191988