
A Community-Based Intervention to Enhance Subjective Well-Being in Older Adults: Study Design and Baseline Participant Profiles
 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Method
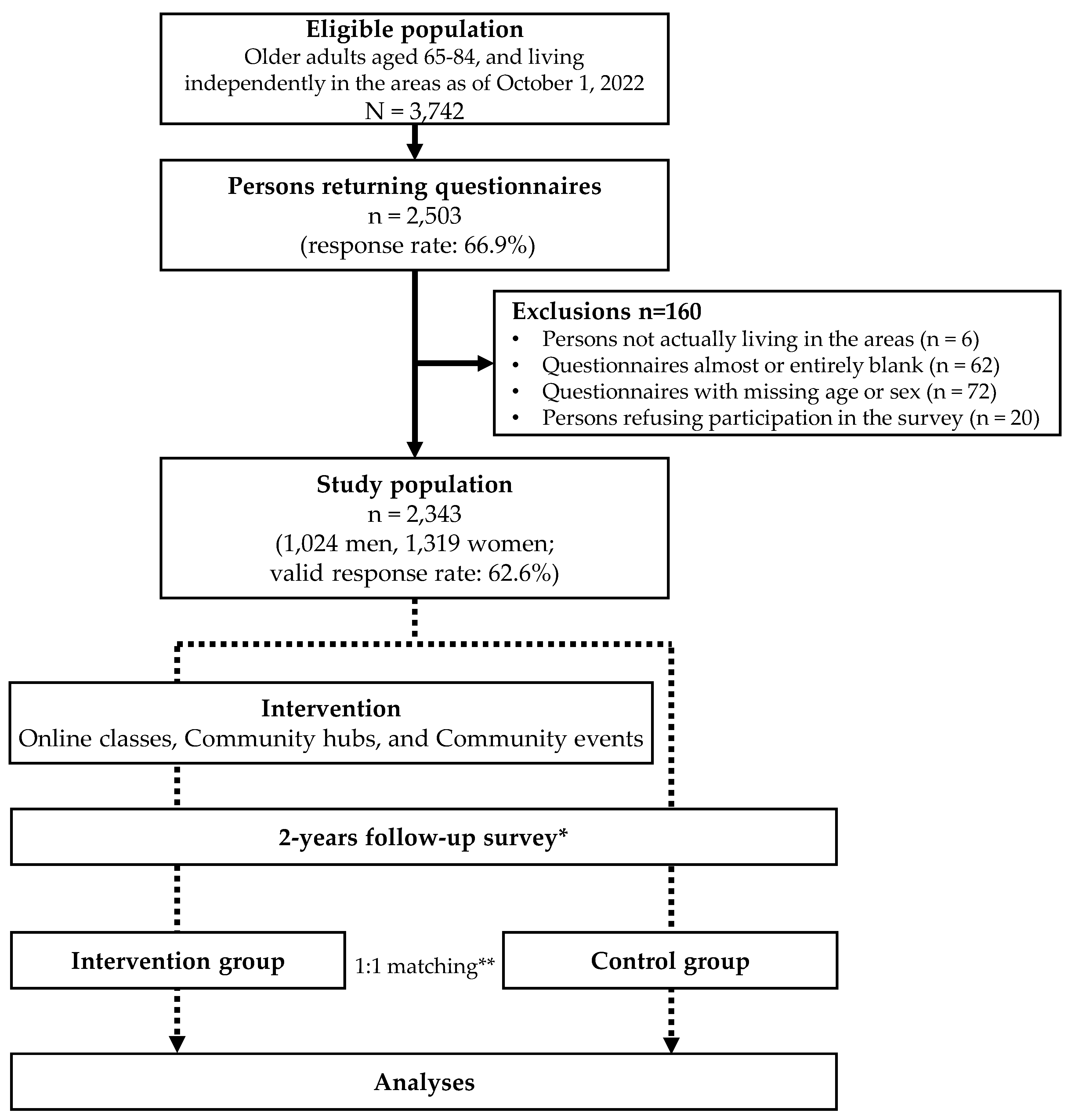
2.1. Study Design, Study Setting, and Participants
2.2. Baseline and Follow-Up Surveys
2.3. Primary Outcome Measures
2.4. Secondary Outcome Measures
2.4.1. Psychosocial Function
2.4.2. Physical Activity and Physical Function
2.4.3. Dietary Habits
2.4.4. Use of ICT
2.5. Intervention Overview
2.6. Ethical Considerations
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office. Japan Annual Report on the Ageing Society FY2022 (Entire Edition). Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2022/html/zenbun/index.html (accessed on 12 June 2023). (In Japanese)
- Andersen, F.K.; Christensen, K.; Frederiksen, H. Self-rated health and age: A cross-sectional and longitudinal study of 11,000 Danes aged 45–102. Scand. J. Public. Health 2007, 35, 164–171. [Google Scholar] [CrossRef]
- Matsui, Y.; Tanizaki, Y.; Arima, H.; Yonemoto, K.; Doi, Y.; Ninomiya, T.; Sasaki, K.; Iida, M.; Iwaki, T.; Kanba, S.; et al. Incidence and survival of dementia in a general population of Japanese elderly: The Hisayama study. J. Neurol. Neurosurg. Psychiatry 2009, 80, 366–370. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J. Marital biography and health at mid-life. J. Health Soc. Behav. 2009, 50, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Laditka, J.N.; Laditka, S.B. Increased hospitalization risk for recently widowed older women and protective effects of social contacts. J. Women Aging 2003, 15, 7–28; discussion 185. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Mental Health Action Plan 2013–2020. Available online: https://www.who.int/publications-detail-redirect/9789241506021 (accessed on 12 June 2023).
- Gale, C.R.; Cooper, C.; Deary, I.J.; Aihie Sayer, A. Psychological well-being and incident frailty in men and women: The English longitudinal study of ageing. Psychol. Med. 2014, 44, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, Y.; Saito, Y. Subjective well-being and active life expectancy in Japan: Evidence from a longitudinal Study. Innov. Aging 2023, 7, igac075. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. Available online: https://psycnet.apa.org/doi/10.1037/0882-7974.15.2.187 (accessed on 1 June 2023). [CrossRef] [PubMed]
- Iwano, S.; Kambara, K.; Aoki, S. Psychological interventions for well-being in healthy older adults: Systematic review and meta-analysis. J. Happiness Stud. 2022, 23, 2389–2403. [Google Scholar] [CrossRef]
- Suragarn, U.; Hain, D.; Pfaff, G. Approaches to enhance social connection in older adults: An integrative review of literature. Aging Health Res. 2021, 1, 100029. [Google Scholar] [CrossRef]
- Kokubun, K.; Ogawa, T.; Browne, R.; Shinada, T.; Granrath, L.; Moeller, J.; Tram, N.; Wieching, R.; Taki, Y. Social capital mediates the association between the ICT usage and well-being of older People in Japan: Implication for a new design paradigm. Sustainability 2022, 14, 4148. [Google Scholar] [CrossRef]
- Putnam, R.D.; Alone, B. America’s declining social capital. In Culture and Politics; Reader, A., Crothers, L., Lockhart, C., Eds.; Palgrave MacMillan: New York, NY, USA, 2000; pp. 223–234. ISBN 978-1-349-62397-6. [Google Scholar]
- Gasteiger, C.; Collens, P.; du Preez, E. Community-based support to improve mental health and wellbeing in older sexually and gender diverse people: A scoping review. Aging Ment. Health 2023, 1–9. [Google Scholar] [CrossRef]
- Foettinger, L.; Albrecht, B.M.; Altgeld, T.; Gansefort, D.; Recke, C.; Stalling, I.; Bammann, K. The Role of community-based men’s sheds in health promotion for older men: A mixed-methods systematic review. Am. J. Mens. Health 2022, 16, 15579883221084490. [Google Scholar] [CrossRef]
- Giebel, C.; Shrestha, N.; Reilly, S.; White, R.G.; Zuluaga, M.I.; Saldarriaga, G.; Liu, G.; Allen, D.; Gabbay, M. Community-based mental health and well-being interventions for older adults in low- and middle-income countries: A systematic review and meta-analysis. BMC Geriatr. 2022, 22, 773. [Google Scholar] [CrossRef]
- Handley, M.A.; Lyles, C.R.; McCulloch, C.; Cattamanchi, A. Selecting and improving quasi-experimental designs in effectiveness and implementation research. Annu. Rev. Public. Health 2018, 39, 5–25. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Seino, S.; Nofuji, Y.; Sugawara, Y.; Osuka, Y.; Kitamura, A.; Shinkai, S. The Kesennuma Study in Miyagi, Japan: Study design and baseline profiles of participants. J. Epidemiol. 2022, 32, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Chofu City Households and Population in Chofu City. 2021. Available online: https://www.city.chofu.tokyo.jp/www/contents/1610018912361/index.html (accessed on 1 June 2023). (In Japanese).
- Statistics of Japan Population Census 2020. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001136464&cycle=0&tclass1=000001136472&tclass2=000001159886&cycle_facet=tclass1%3Acycle&tclass3val=0 (accessed on 1 June 2023). (In Japanese)
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public. Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Tomine, Y.; Nishi, M.; Hata, T.; Fujiwara, Y.; Shinkai, S.; Kitamura, A. Effectiveness of a community-wide intervention for population-level frailty and functional health in older adults: A 2-year cluster nonrandomized controlled trial. Prev. Med. 2021, 149, 106620. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Kitamura, A.; Tomine, Y.; Tanaka, I.; Nishi, M.; Nonaka, K.; Nofuji, Y.; Narita, M.; Taniguchi, Y.; Yokoyama, Y.; et al. A community-wide intervention trial for preventing and reducing frailty among older adults living in metropolitan areas: Design and baseline survey for a study integrating participatory action research with a cluster trial. J. Epidemiol. 2019, 29, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Glatzer, W.; Gulyas, J. Cantril self-anchoring striving scale. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 509–511. ISBN 978-94-007-0753-5. [Google Scholar]
- Saito, M.; Kondo, K.; Ojima, T.; Hirai, H.; JAGES group. Criteria for social isolation based on associations with health indicators among older people a 10-year follow-up of the Aichi gerontological evaluation study. Nihon Koshu Eisei Zasshi 2015, 62, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Kitamura, A.; Nishi, M.; Tomine, Y.; Tanaka, I.; Taniguchi, Y.; Yokoyama, Y.; Amano, H.; Narita, M.; Ikeuchi, T.; et al. Individual- and community-level neighbor relationships and physical activity among Older Japanese adults living in a metropolitan area: A cross-sectional multilevel analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 46. [Google Scholar] [CrossRef]
- Nakamura, H.; Nakamura, M.; Okada, E.; Ojima, T.; Kondo, K. Association of food access and neighbor relationships with diet and underweight among community-dwelling Older Japanese. J. Epidemiol. 2017, 27, 546–551. [Google Scholar] [CrossRef]
- Ishikawa, H.; Nomura, K.; Sato, M.; Yano, E. Developing a measure of communicative and critical health literacy: A pilot study of Japanese office workers. Health Promot. Int. 2008, 23, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Awata, S.; Bech, P.; Yoshida, S.; Hirai, M.; Suzuki, S.; Yamashita, M.; Ohara, A.; Hinokio, Y.; Matsuoka, H.; Oka, Y. Reliability and validity of the Japanese version of the World Health Organization-five well-being index in the context of detecting depression in diabetic patients. Psychiatry Clin. Neurosci. 2007, 61, 112–119. [Google Scholar] [CrossRef]
- Awata, S.; Bech, P.; Koizumi, Y.; Seki, T.; Kuriyama, S.; Hozawa, A.; Ohmori, K.; Nakaya, N.; Matsuoka, H.; Tsuji, I. Validity and utility of the Japanese version of the WHO-five well-being index in the context of detecting suicidal ideation in elderly community residents. Int. Psychogeriatr. 2007, 19, 77–88. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item Geriatric Depression Scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Kitayuguchi, J.; Inoue, S.; Ishikawa, Y.; Nishiuchi, H.; Okada, S.; Harada, K.; Kamioka, H.; Shiwaku, K. A community-wide campaign to promote physical activity in middle-aged and elderly People: A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 44. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Shinkai, S.; Watanabe, N.; Yoshida, H.; Fujiwara, Y.; Amano, H.; Lee, S.; Nishi, M.; Tsuchiya, Y. Research on Screening for Frailty: Development of “the Kaigo-Yobo Checklist”. Nihon Koshu Eisei Zasshi 2010, 57, 345–354. [Google Scholar] [CrossRef]
- Shinkai, S.; Watanabe, N.; Yoshida, H.; Fujiwara, Y.; Nishi, M.; Fukaya, T.; Lee, S.; Kim, M.J.; Ogawa, K.; Murayama, H.; et al. Validity of the “Kaigo-Yobo Check-List” as a frailty index. Nihon Koshu Eisei Zasshi 2013, 60, 262–274. [Google Scholar] [PubMed]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG index of competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Kinugasa, T.; Nagasaki, H. Reliability and validity of the motor fitness scale for older adults in the community. Aging 1998, 10, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Nihon Koshu Eisei Zasshi 2003, 50, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Moriyasu, A.; Kumagai, S.; Furuna, T.; Akita, S.; Kimura, S.; Suzuki, T. Community-based intervention to improve dietary habits and promote physical activity among older adults: A cluster randomized trial. BMC Geriatr. 2013, 13, 8. [Google Scholar] [CrossRef]
- Tani, Y.; Sasaki, Y.; Haseda, M.; Kondo, K.; Kondo, N. Eating Alone and depression in older men and women by cohabitation status: The JAGES longitudinal survey. Age Ageing 2015, 44, 1019–1026. [Google Scholar] [CrossRef]
- LaMonica, H.M.; Davenport, T.A.; Roberts, A.E.; Hickie, I.B. Understanding technology preferences and requirements for health information technologies designed to improve and maintain the mental health and well-being of older adults: Participatory design Study. JMIR Aging 2021, 4, e21461. [Google Scholar] [CrossRef] [PubMed]
- Duplaga, M. The association between Internet use and health-related outcomes in older adults and the elderly: A cross-sectional study. BMC Med. Inform. Decis. Mak. 2021, 21, 150. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: A randomized controlled trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Otake, M.; Kato, M.; Takagi, T.; Asama, H. The Coimagination method and its evaluation via the conversation interactivity measuring method. In Early Detection and Rehabilitation Technologies for Dementia: Neuroscience and Biomedical Applications; IGI Global: Hershey, PA, USA, 2011; pp. 356–364. [Google Scholar]
- Mihoko, O.-M. Conversation assistive technology for maintaining cognitive health. J. Korean Gerontol. Nurs. 2018, 20 (Suppl. 1), 154–159. [Google Scholar] [CrossRef]
- Asakawa, Y.; Endo, F.; Yamaguchi, H.; Takahashi, R. The characteristics of participants and the effects of self-paced resistance training for community-dwelling elders in early period of a residents-led preventive care program, the Onishi Model. Rigaku Ryōhōgaku 2008, 35, 229–236. [Google Scholar] [CrossRef]
- Matsubayashi, Y.; Asakawa, Y.; Yamaguchi, H. Low-frequency group exercise improved the motor functions of community-dwelling elderly People in a rural area when combined with home exercise with self-monitoring. J. Phys. Ther. Sci. 2016, 28, 366–371. [Google Scholar] [CrossRef]
- Fiatarone, M.A.; Marks, E.C.; Ryan, N.D.; Meredith, C.N.; Lipsitz, L.A.; Evans, W.J. High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA 1990, 263, 3029–3034. [Google Scholar] [CrossRef]
- Marzuki, A.A.; Nor, N.N.F.M.; Rashid, S.M.R.A.; Ghazali, S. Social support by communities for older adults in Malaysia. Nurture 2023, 17, 272–280. [Google Scholar] [CrossRef]
- Choi, E.; Han, K.M.; Chang, J.; Lee, Y.J.; Choi, K.W.; Han, C.; Ham, B.J. Social participation and depressive symptoms in community-dwelling older adults: Emotional social support as a mediator. J. Psychiatr. Res. 2021, 137, 589–596. [Google Scholar] [CrossRef]
- Colistra, C.; Bixler, R.; Schmalz, D. Exploring factors that contribute to relationship building in a community center. J. Leis. Res. 2019, 50, 1–17. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Tiefenbach, T.; Kohlbacher, F. Subjective well-being across gender and age in Japan: An econometric analysis. In Gender, Lifespan and Quality of Life: An International Perspective; Eckermann, E., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 183–201. ISBN 978-94-007-7829-0. [Google Scholar] [CrossRef]
- Blanchflower, D.G.; Oswald, A.J. Is well-being U-shaped over the life cycle? Soc. Sci. Med. 2008, 66, 1733–1749. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, J.F.; Layard, R.; Sachs, J.D.; Neve, J.E.D.; Aknin, L.B.; Wang, S. World Happiness Report; Gallup: Washington, DC, USA, 2023; Volume 2023. [Google Scholar]
- Saito, T.; Sugisawa, H.; Harada, K.; Kai, I. Population aging in local areas and subjective well-being of older adults: Findings from two studies in Japan. BioSci Trends 2016, 10, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Statistics Bureau of Japan Current Population Estimates as of 2021. Available online: https://www.stat.go.jp/english/data/jinsui/2021np/index.html (accessed on 13 June 2023).
- Döring, N.; Conde, M.; Brandenburg, K.; Broll, W.; Gross, H.M.; Werner, S.; Raake, A. Can communication technologies reduce loneliness and social isolation in older People? A scoping review of reviews. Int. J. Environ. Res. Public. Health 2022, 19, 11310. [Google Scholar] [CrossRef] [PubMed]
- Hunsaker, A.; Hargittai, E. A review of Internet use among older adults. New Media Soc. 2018, 20, 3937–3954. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications the Communications Usage Trend Survey. 2022. Available online: https://www.soumu.go.jp/johotsusintokei/statistics/statistics05.html (accessed on 5 July 2023).
- Murayama, H.; Nofuji, Y.; Matsuo, E.; Nishi, M.; Taniguchi, Y.; Fujiwara, Y.; Shinkai, S. The Yabu cohort Study: Design and profile of participants at baseline. J. Epidemiol. 2014, 24, 519–525. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Primary outcome measures |
| Subjective well-being |
| Secondary outcome measures |
| Psychosocial function |
| Social isolation |
| Neighborhood relationships |
| Social participation |
| Health literacy (CCHL) |
| Psychological health (WHO-5) |
| Depressive mood (GDS-5) |
| Physical activity and physical function |
| Exercise habits |
| Frailty status (CL15) |
| Activities of daily living (TMIG-IC) |
| Motor Fitness Scale |
| Dietary habits |
| Dietary Variety Score |
| Food Frequency Score |
| Eating alone |
| Use of ICT |
| Type of own ICT |
| Frequency of Internet usage |
| Additional measures |
| Age |
| Sex |
| Cohabiters |
| Years of residence in the neighborhood area |
| Financial status |
| Employment status |
| Chronic musculoskeletal pain (shoulder, low back, knee) |
| Body mass index (self-rated height and weight) |
| Drinking and smoking |
| Variables | All | Men | Women | p-Value | |||
|---|---|---|---|---|---|---|---|
| Number of residents aged 65–84 years old | 3742 | 1681 | 2061 | ||||
| Number of analyzed participants (eligible response rate; %) | 2343 | (62.6) | 1024 | (60.9) | 1319 | (64.0) | |
| Age, years, mean (SD) | 74.4 | (5.4) | 74.2 | (5.5) | 74.5 | (5.3) | 0.094 |
| 65–74, n (%) | 1232 | (52.6) | 564 | (55.1) | 668 | (50.6) | |
| 75–84, n (%) | 1111 | (47.4) | 460 | (44.9) | 651 | (49.4) | 0.033 |
| Living alone, n (%) | 454 | (19.5) | 157 | (15.4) | 297 | (22.7) | <0.001 |
| Year of residence in the neighborhood, n (%) | |||||||
| <29 | 718 | (30.8) | 337 | (33.0) | 381 | (29.0) | |
| 30–59 | 1407 | (60.3) | 561 | (54.9) | 846 | (64.4) | |
| >59 | 209 | (9.0) | 123 | (12.0) | 86 | (6.5) | <0.001 |
| Financial status (self-rated), n (%) | |||||||
| Low | 76 | (3.3) | 42 | (4.1) | 34 | (2.6) | |
| Middle-low | 303 | (13.0) | 143 | (14.1) | 160 | (12.2) | |
| Middle | 888 | (38.2) | 361 | (35.5) | 527 | (40.3) | |
| Middle-high | 941 | (40.5) | 419 | (41.2) | 522 | (39.9) | |
| High | 118 | (5.1) | 52 | (5.1) | 66 | (5.0) | 0.055 |
| Employment status, n (%) | |||||||
| No | 1537 | (66.5) | 581 | (57.0) | 956 | (73.9) | |
| Yes | 776 | (33.5) | 439 | (43.0) | 337 | (26.1) | <0.001 |
| Musculoskeletal pain (either shoulder, low back, or knee), n (%) | |||||||
| No | 792 | (34.8) | 391 | (39.1) | 401 | (31.5) | |
| Yes | 1482 | (65.2) | 610 | (60.9) | 872 | (68.5) | <0.001 |
| Body mass index, kg/m2, mean (SD) | 22.7 | (3.2) | 23.3 | (2.9) | 22.2 | (3.3) | <0.001 |
| <18.5, n (%) | 178 | (7.8) | 38 | (3.8) | 140 | (10.9) | |
| 18.5–24.9, n (%) | 1632 | (71.1) | 719 | (71.4) | 913 | (70.9) | |
| ≥25, n (%) | 485 | (21.1) | 250 | (24.8) | 235 | (18.2) | <0.001 |
| Alcohol drinking status, n (%) | |||||||
| Never or former | 1026 | (44.0) | 274 | (26.8) | 752 | (57.4) | |
| Current | 1307 | (56.0) | 749 | (73.2) | 558 | (42.6) | <0.001 |
| Smoking status, n (%) | |||||||
| Never or former | 2116 | (90.8) | 865 | (84.7) | 1251 | (95.5) | |
| Current | 215 | (9.2) | 156 | (15.3) | 59 | (4.5) | <0.001 |
| Primary outcome measures | |||||||
| Subjective well-being, mean (SD) | 7.2 | (1.9) | 6.9 | (1.9) | 7.4 | (1.8) | <0.001 |
| Secondary outcome measures | |||||||
| Social relationships | |||||||
| Social isolation, n (%) | 1572 | (68.6) | 782 | (78.1) | 790 | (61.2) | <0.001 |
| Neighborhood relationships, n (%) | |||||||
| Visiting each other | 489 | (21.8) | 132 | (13.3) | 357 | (28.4) | |
| Standing and chatting | 921 | (41.0) | 344 | (34.6) | 577 | (46.0) | |
| Exchanging of greetings | 694 | (30.9) | 421 | (42.4) | 273 | (21.8) | |
| None | 144 | (6.4) | 96 | (9.7) | 48 | (3.8) | <0.001 |
| Social participation more than once a month, n (%) | 1032 | (44.6) | 346 | (34.1) | 686 | (52.9) | <0.001 |
| Health literacy (CCHL), mean (SD) | 3.6 | (0.8) | 3.6 | (0.8) | 3.5 | (0.8) | 0.028 |
| Psychological health (WHO-5: 0–25), mean (SD) | 15.0 | (5.4) | 14.6 | (5.6) | 15.3 | (5.3) | 0.004 |
| Depressive mood (GDS-5 2), n (%) | 814 | (36.0) | 365 | (36.8) | 449 | (35.5) | 0.526 |
| Physical activity and physical function | |||||||
| Engaging in any exercise more than once a week, n (%) | 1735 | (76.8) | 756 | (76.1) | 979 | (77.4) | 0.456 |
| Engaging in walking 150 or more minutes per week, n (%) | 1473 | (65.0) | 615 | (62.1) | 858 | (67.2) | 0.012 |
| Going out more than once a day, n (%) | 1504 | (65.1) | 672 | (66.7) | 832 | (63.8) | 0.136 |
| Frailty (CL15 score 4), n (%) | 497 | (22.8) | 252 | (26.4) | 245 | (20.0) | <0.001 |
| TMIG-IC (score: 0–13), mean (SD) | 11.3 | (1.8) | 10.9 | (2.1) | 11.6 | (1.6) | <0.001 |
| Motor Fitness Scale, mean (SD) | 10.5 | (3.5) | 10.9 | (3.2) | 10.1 | (3.7) | <0.001 |
| Dietary variety | |||||||
| Dietary Variety Score (0–10), mean (SD) | 3.4 | (2.3) | 2.8 | (2.2) | 3.9 | (2.3) | <0.001 |
| Food Frequency Score (0–30), mean (SD) | 18.4 | (5.2) | 16.9 | (5.1) | 19.6 | (4.9) | <0.001 |
| Eat alone at least a whole day per week, n (%) | 1041 | (46.6) | 442 | (44.7) | 599 | (48.1) | 0.112 |
| Use of ICT | |||||||
| Owing smartphone | 1529 | (66.2) | 677 | (67.0) | 852 | (65.6) | 0.488 |
| Using the Internet more than once a day, n (%) | 1059 | (46.7) | 545 | (54.6) | 514 | (40.5) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakada, T.; Kozawa, T.; Seino, S.; Murota, S.; Eto, M.; Shimasawa, J.; Shimizu, Y.; Tsurugano, S.; Katsukawa, F.; Sakamoto, K.; et al. A Community-Based Intervention to Enhance Subjective Well-Being in Older Adults: Study Design and Baseline Participant Profiles. Healthcare 2024, 12, 322. https://doi.org/10.3390/healthcare12030322
Nakada T, Kozawa T, Seino S, Murota S, Eto M, Shimasawa J, Shimizu Y, Tsurugano S, Katsukawa F, Sakamoto K, et al. A Community-Based Intervention to Enhance Subjective Well-Being in Older Adults: Study Design and Baseline Participant Profiles. Healthcare. 2024; 12(3):322. https://doi.org/10.3390/healthcare12030322
Chicago/Turabian StyleNakada, Tsubasa, Takako Kozawa, Satoshi Seino, Shinichi Murota, Miki Eto, Junko Shimasawa, Yumiko Shimizu, Shinobu Tsurugano, Fuminori Katsukawa, Kazunori Sakamoto, and et al. 2024. "A Community-Based Intervention to Enhance Subjective Well-Being in Older Adults: Study Design and Baseline Participant Profiles" Healthcare 12, no. 3: 322. https://doi.org/10.3390/healthcare12030322
APA StyleNakada, T., Kozawa, T., Seino, S., Murota, S., Eto, M., Shimasawa, J., Shimizu, Y., Tsurugano, S., Katsukawa, F., Sakamoto, K., Washizaki, H., Ishigaki, Y., Sakamoto, M., Takadama, K., Yanai, K., Matsuo, O., Kameue, C., Suzuki, H., Kurotani, K., & Ohkawara, K. (2024). A Community-Based Intervention to Enhance Subjective Well-Being in Older Adults: Study Design and Baseline Participant Profiles. Healthcare, 12(3), 322. https://doi.org/10.3390/healthcare12030322