
Epidemiology of Dementia in China in 2010–2020: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
1. Research Manuscript Sections
Background
2. Methods
2.1. Objective
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias in Individual Studies
2.7. Data Analysis
3. Results
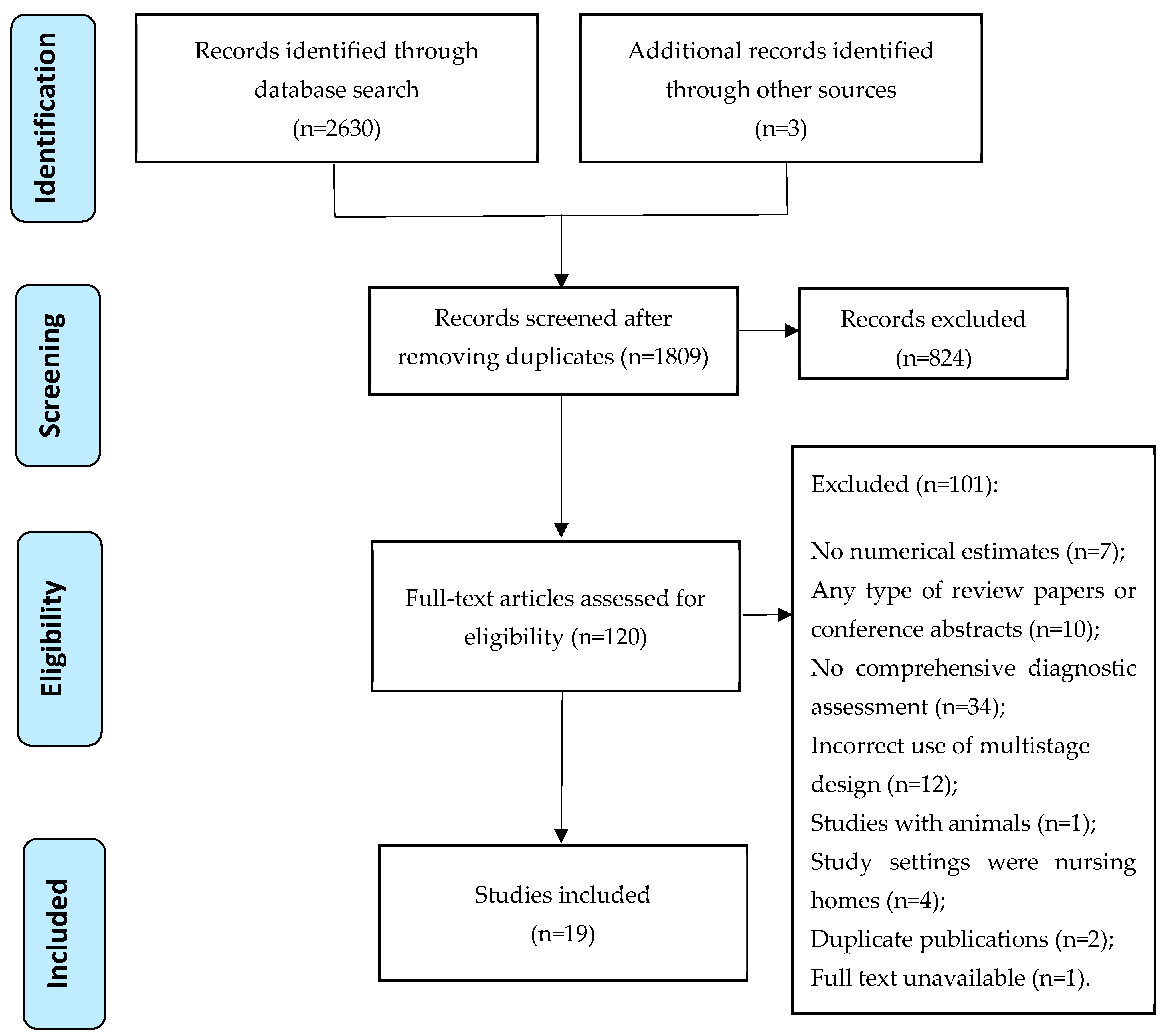
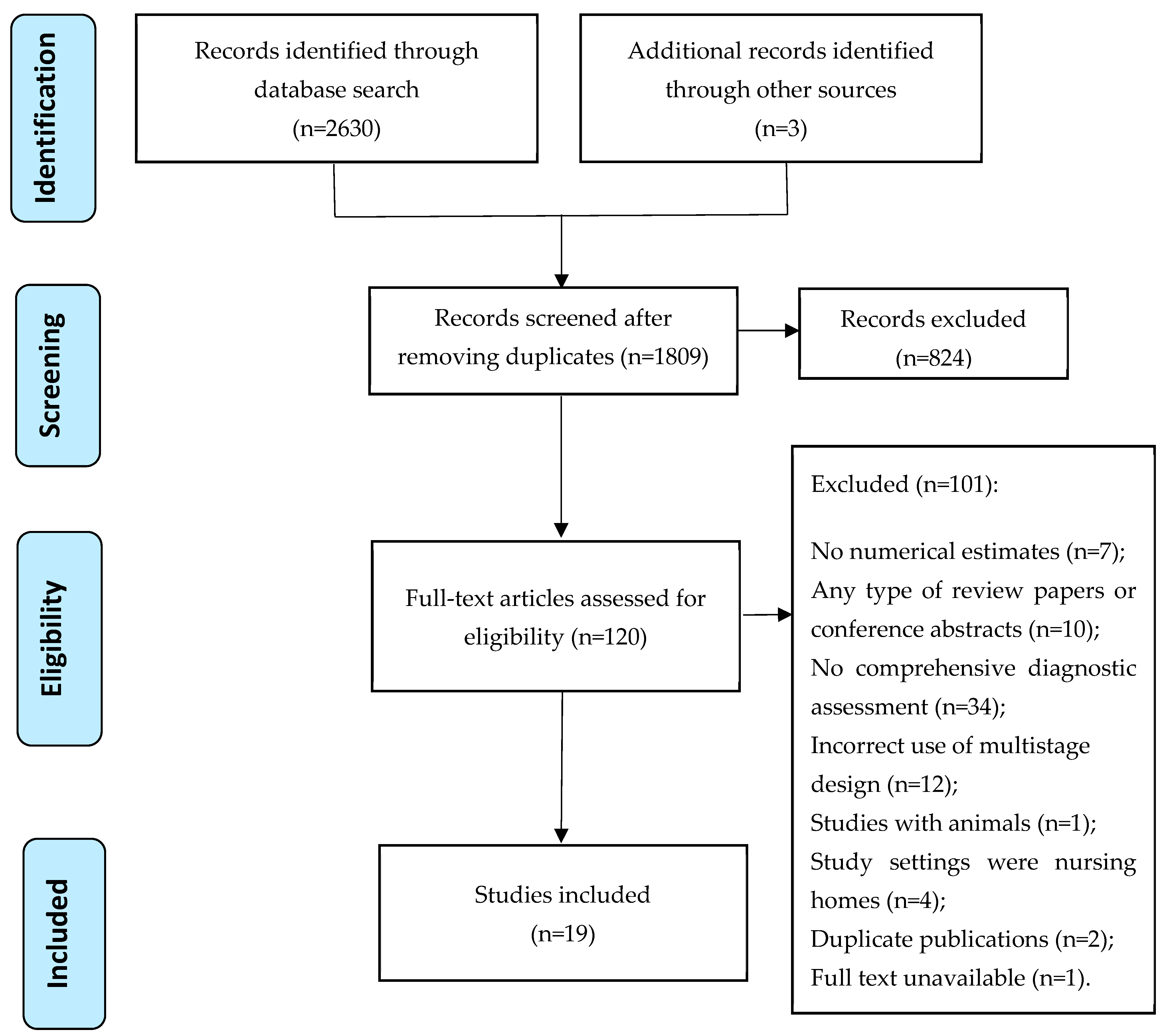
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality of Included Studies
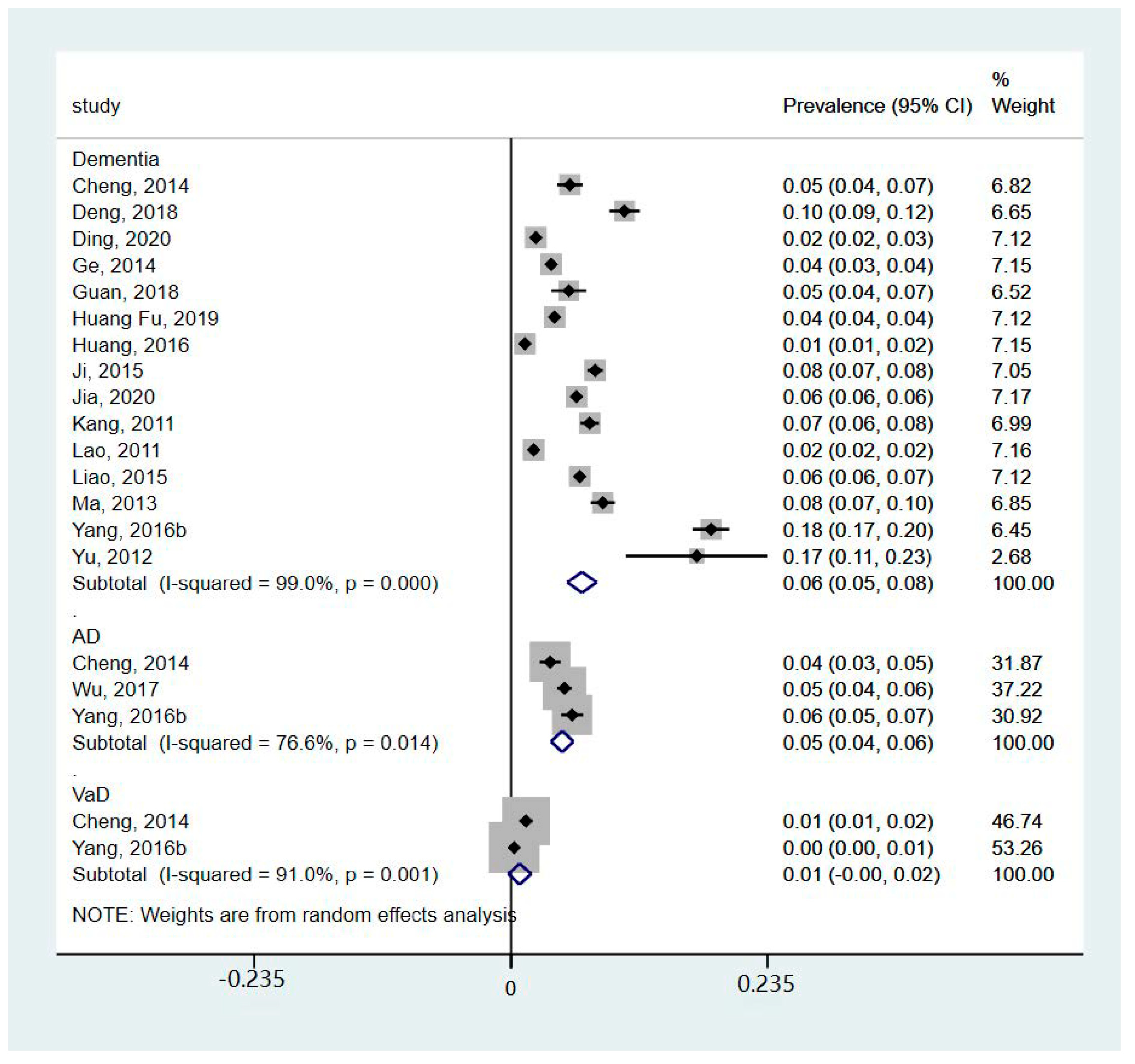
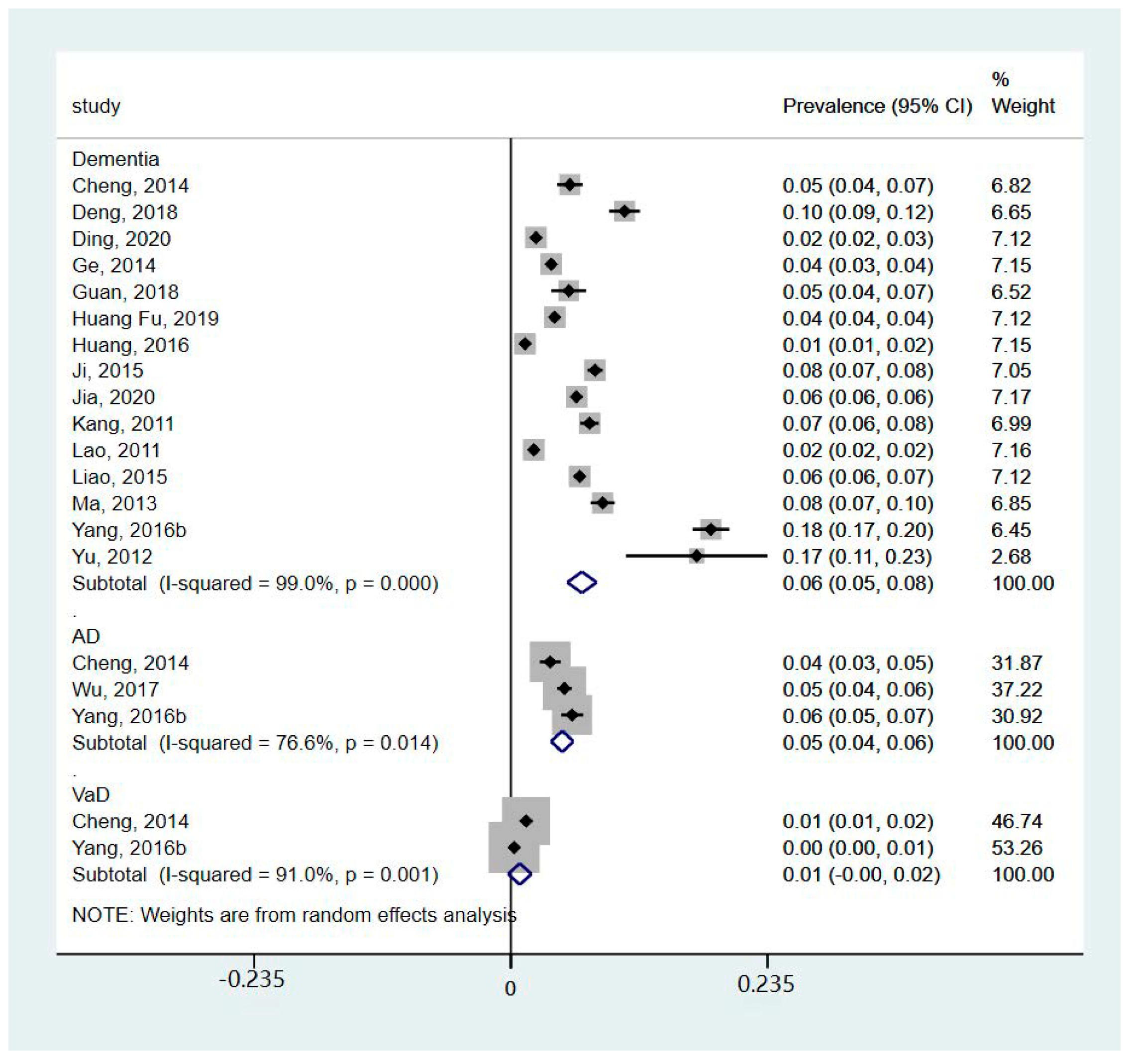
3.4. Incidence, Prevalence, and Mortality of Dementia in China between 2010 and 2020
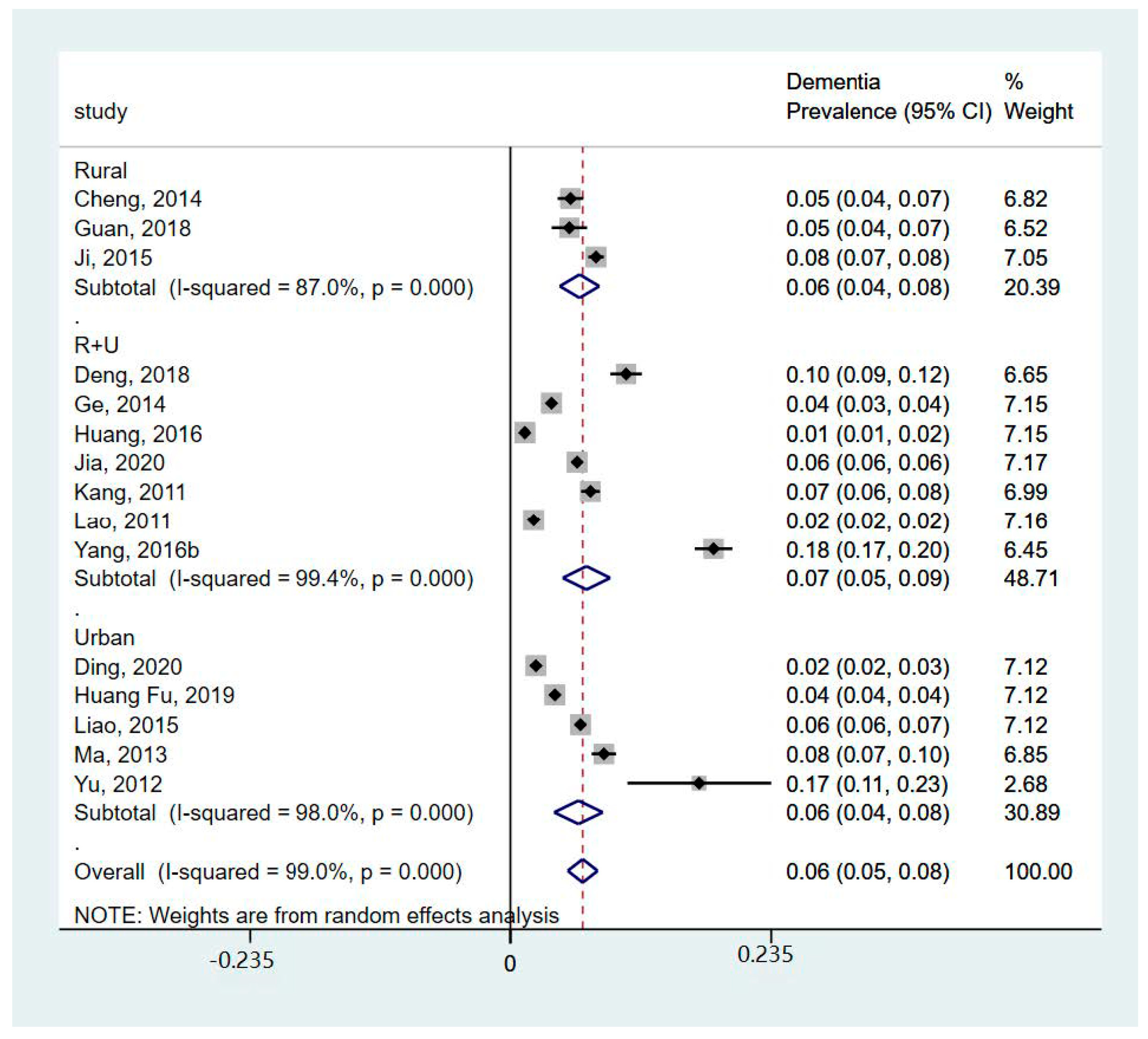
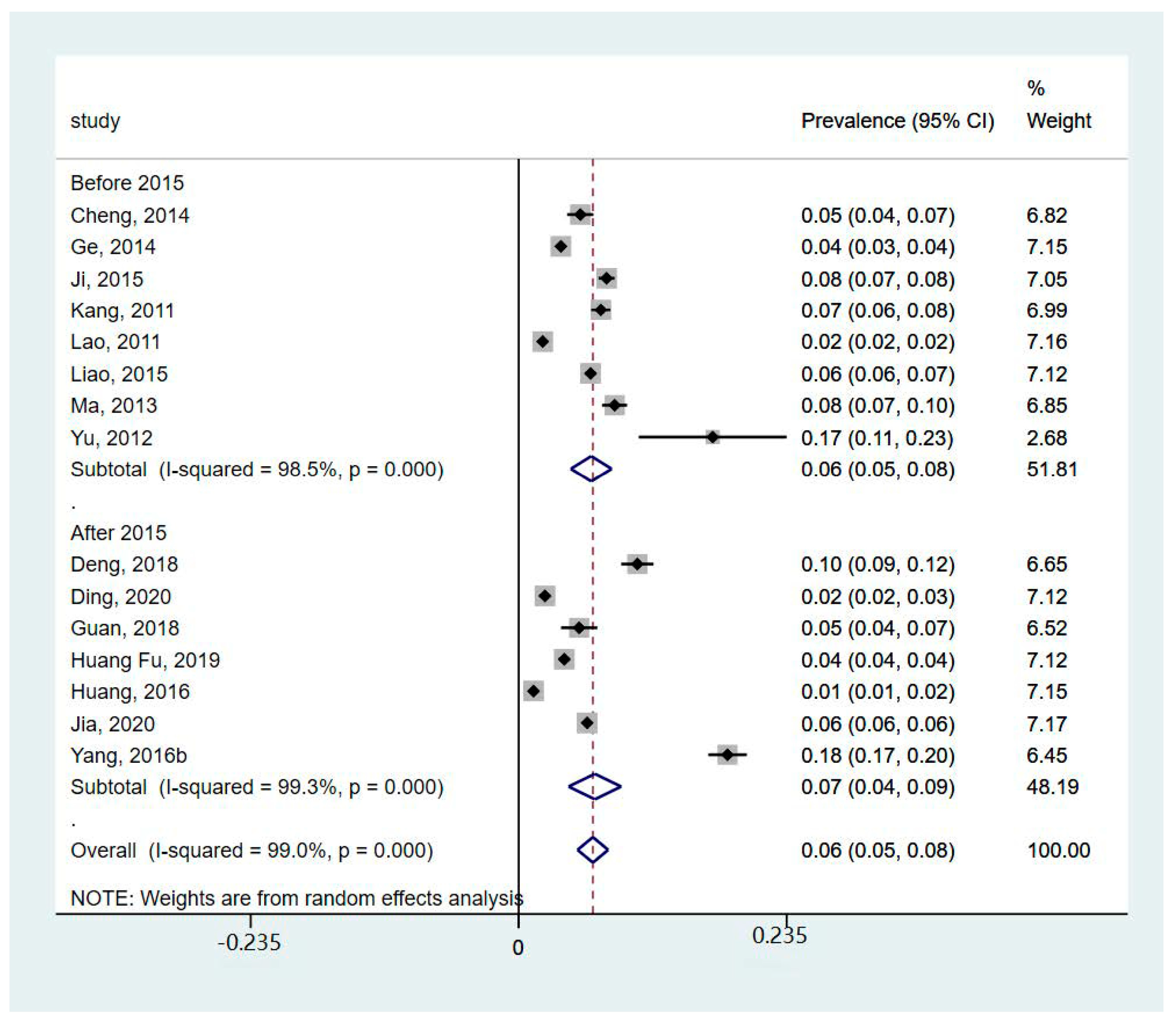
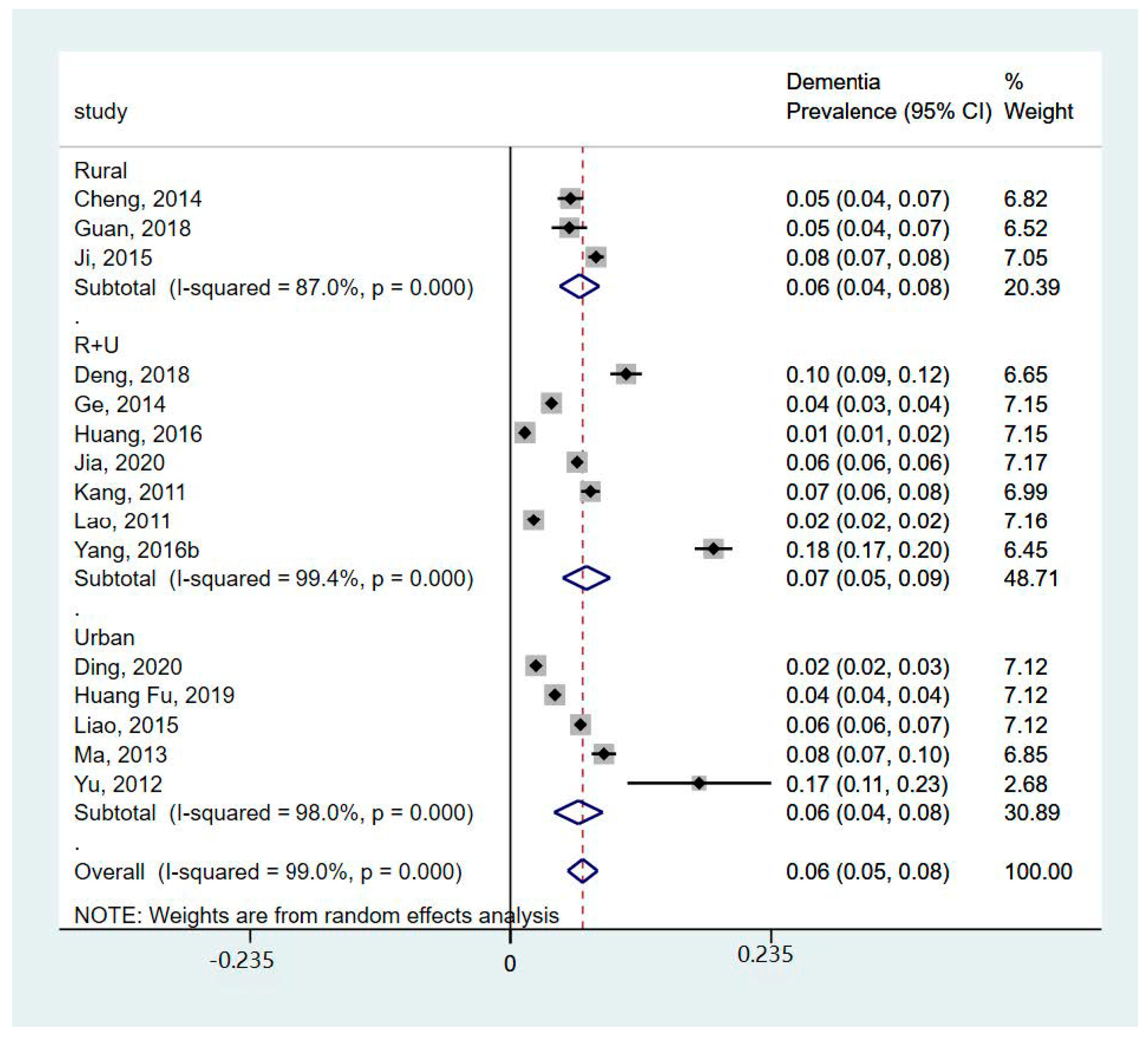
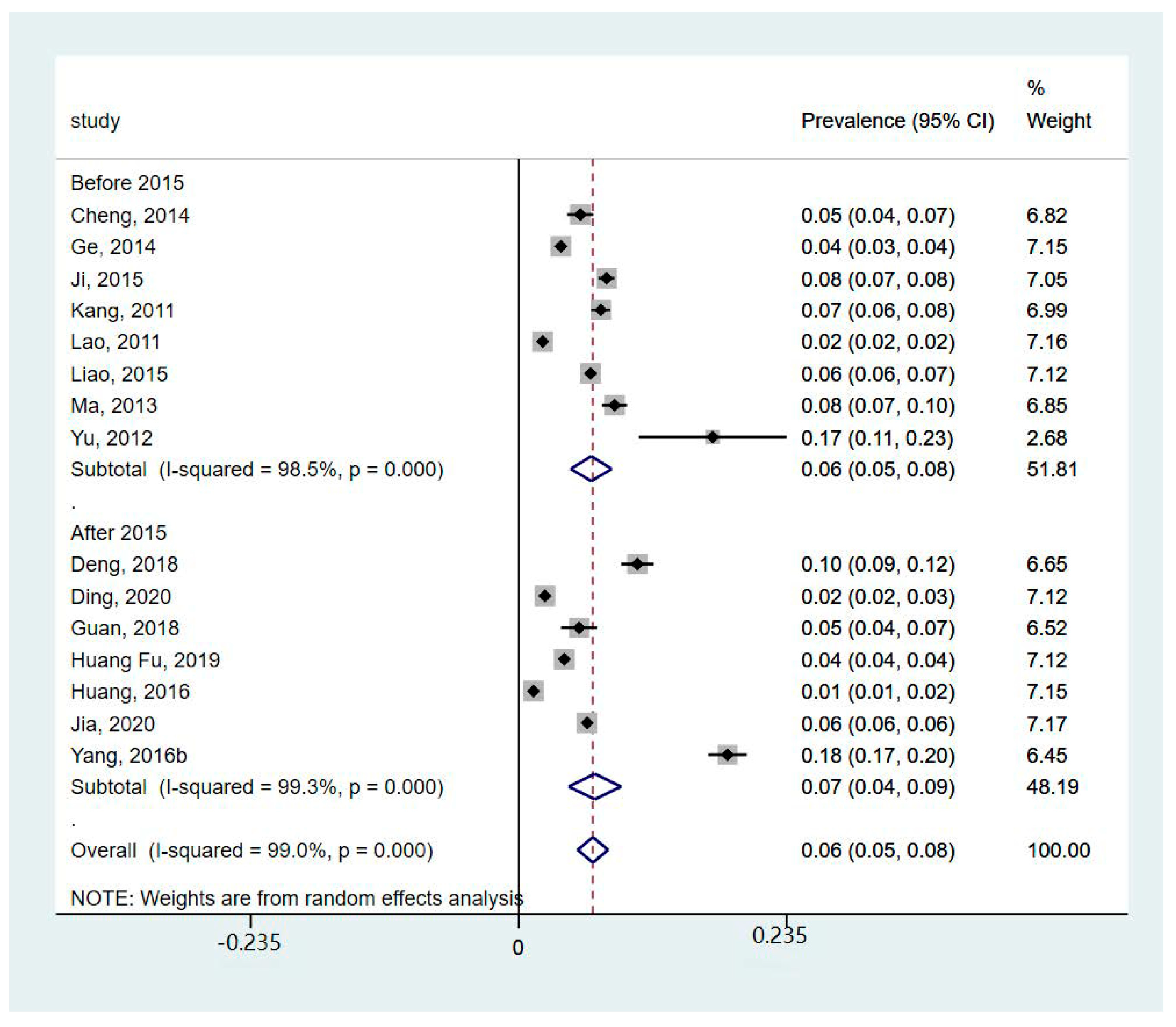
3.5. Geographical, Age, and Sex Differences in the Prevalence and Incidence of Dementia in China between 2010 and 2020
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quinn, T.J.; Fearon, P.; Noel-Storr, A.H.; Young, C.; McShane, R.; Stott, D.J.; Quinn, T.J. Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) for the diagnosis of dementia within community dwelling populations. Cochrane Database Syst. Rev. 2014, 2014, CD010079. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on the Public Health Response to Dementia; WHO: Geneva, Switzerland, 2021.
- Milne, A. Dementia screening and early diagnosis: The case for and against. Health Risk Soc. 2010, 12, 65–76. [Google Scholar] [CrossRef]
- Banerjee, S.; Wittenberg, R. Clinical and cost effectiveness of services for early diagnosis and intervention in dementia. Int. J. Geriatr. Psychiatry J. Psychiatry Late Life Allied Sci. 2009, 24, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.; Langerman, H. Alzheimer’s disease–why we need early diagnosis. Degener. Neurol. Neuromuscul. Dis. 2019, 9, 123. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, B.A.; Senan, E.M.; Rassem, T.H.; Makbol, N.M.; Alanazi, A.A.; Al-Mekhlafi, Z.G.; Almurayziq, T.S.; Ghaleb, F.A. Multi-method analysis of medical records and MRI images for early diagnosis of dementia and Alzheimer’s disease based on deep learning and hybrid methods. Electronics 2021, 10, 2860. [Google Scholar] [CrossRef]
- Wang, Y.; Xiao, L.D.; Ullah, S.; He, G.-P.; De Bellis, A. Evaluation of a nurse-led dementia education and knowledge translation programme in primary care: A cluster randomized controlled trial. Nurse Educ. Today 2017, 49, 1–7. [Google Scholar] [CrossRef]
- Paddick, S.-M.; Yoseph, M.; Gray, W.K.; Andrea, D.; Barber, R.; Colgan, A.; Dotchin, C.; Urasa, S.; Kissima, J.; Haule, I. Effectiveness of app-based cognitive screening for dementia by lay health workers in low resource settings. A validation and feasibility study in rural Tanzania. J. Geriatr. Psychiatry Neurol. 2021, 34, 613–621. [Google Scholar] [CrossRef]
- Chan, K.Y.; Wang, W.; Wu, J.J.; Liu, L.; Theodoratou, E.; Car, J.; Middleton, L.; Russ, T.C.; Deary, I.J.; Campbell, H.; et al. Epidemiology of Alzheimer’s disease and other forms of dementia in China, 1990–2010: A systematic review and analysis. Lancet 2013, 381, 2016–2023. [Google Scholar] [CrossRef]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement. 2013, 9, 63–75.e2. [Google Scholar] [CrossRef]
- Ji, Y.; Shi, Z.; Zhang, Y.; Liu, S.; Liu, S.; Yue, W.; Liu, M.; Huo, Y.R.; Wang, J.; Wisniewski, T. Prevalence of dementia and main subtypes in rural northern China. Dement. Geriatr. Cogn. Disord. 2015, 39, 294–302. [Google Scholar] [CrossRef]
- Yang, L.; Jin, X.; Yan, J.; Jin, Y.; Yu, W.; Wu, H.; Xu, S. Prevalence of dementia, cognitive status and associated risk factors among elderly of Zhejiang province, China in 2014. Age Ageing 2016, 45, 708–712. [Google Scholar] [CrossRef]
- Alladi, S.; Hachinski, V. World dementia: One approach does not fit all. Neurology 2018, 91, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Crescioli, G.; Cavedo, E.; Lucenteforte, E.; Casazza, G.; Bellatorre, A.G.; Lista, C.; Costantino, G.; Frisoni, G.; Virgili, G. Structural magnetic resonance imaging for the early diagnosis of dementia due to Alzheimer’s disease in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Miraglia, F.; Vecchio, F. Early dementia diagnosis, MCI-to-dementia risk prediction, and the role of machine learning methods for feature extraction from integrated biomarkers, in particular for EEG signal analysis. Alzheimer’s Dement. 2022, 18, 2699–2706. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Xie, X.; Wu, Q.; Zhang, X.; Cheng, H.; Tao, S.; Quan, H. Inequality in the health services utilization in rural and urban China: A horizontal inequality analysis. Medicine 2020, 99, e18625. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Checklist for Systematic Reviews and Research Syntheses; Joanna Briggs Institute: Adelaide, SA, Australia, 2017. [Google Scholar]
- Bo, Z.; Wan, Y.; Meng, S.S.; Lin, T.; Kuang, W.; Jiang, L.; Qiu, P. The temporal trend and distribution characteristics in mortality of Alzheimer’s disease and other forms of dementia in China: Based on the National Mortality Surveillance System (NMS) from 2009 to 2015. PLoS ONE 2019, 14, e0210621. [Google Scholar] [CrossRef]
- Cheng, Q.; Sun, H.-X.; Ye, F.-L.; Wang, G.; Ling, H.-W.; Chen, S.-D.; Jiang, G.-X. Dementia among elderly in Shanghai suburb: A rural community survey. J. Alzheimer’s Dis. 2014, 39, 883–889. [Google Scholar] [CrossRef]
- Deng, J.; Cao, C.; Jiang, Y.; Peng, B.; Wang, T.; Yan, K.; Lian, J.; Wang, Z. Prevalence and effect factors of dementia among the community elderly in Chongqing, China. Psychogeriatrics 2018, 18, 412–420. [Google Scholar] [CrossRef]
- Ding, D.; Zhao, Q.; Wu, W.; Xiao, Z.; Liang, X.; Luo, J.; Hong, Z. Prevalence and incidence of dementia in an older Chinese population over two decades: The role of education. Alzheimer’s Dement. 2020, 16, 1650–1662. [Google Scholar] [CrossRef]
- Ge, X.; Wang, M.; Tang, J.; Zhou, W.; Xie, Z. Investigation on the prevalence and risk factors of senile dementia in Changsha area. Chin. J. Nerv. Ment. Dis. 2014, 40, 493–496. [Google Scholar]
- Guan, J. Incidence of Alzheimer in Persons over 60 Years Old in Taizhou City and Influencing Factors. Med. Soc. 2018, 31, 52–54. [Google Scholar]
- Hu, W.; Zhou, X.; Gong, Z.; Zhang, T.; Qin, W.; Luo, X. Mortality analysis of senile dementia in Kunshan from 2005 to 2015. Chin. J. Health Stat. 2018, 35, 542–545. [Google Scholar]
- Huang, F.; Chang, F.; Zhang, F.; Hao, X.; Guo, J.; Han, L. Study on the prevalence of senile dementia and its influencing factors in Zhengzhou. Mod. Prev. Med. 2019, 46, 3347–3350. [Google Scholar]
- Huang, F.; Shang, Y.; Luo, Y.; Wu, P.; Huang, X.; Tan, X.; Lu, X.; Zhen, L.; Hu, X. Lower prevalence of Alzheimer’s disease among Tibetans: Association with religious and genetic factors. J. Alzheimer’s Dis. 2016, 50, 659–667. [Google Scholar] [CrossRef]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Zhu, M.; Jiao, H.; Song, Y. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: A cross-sectional study. Lancet Public Health 2020, 5, e661–e671. [Google Scholar] [CrossRef]
- Kang, M.; Gao, Y.; Huo, H.; Chen, Y.; Wang, J.; Li, M.; Du, T. Epidemiological leatures of chronic and Aizheimer’s diseases in the community-based elderly living in cities and couties in Hebei province. Chin. J. Epidemiol. 2011, 32, 672–675. [Google Scholar]
- Lao, M.; Zhang, H.; Yi, X.; Huang, Y.; Wu, Z.; Luo, G. Epidemiological investigation of Alzheimer’s disease in Hainan Island. Chin. J. Gerontol. 2011, 31, 4016–4018. [Google Scholar]
- Liao, J.; Hunag, H.; Yan, J.; Ma, J.; Tao, X.; Liao, X.; Wu, L. The prevalence of Alzheimer’s disease in Nanchang community and its influencing factors. Chin. J. Gerontol. 2015, 35, 7176–7177. [Google Scholar]
- Ma, Y.; Jiang, Z.; Wang, J.; Xue, J.; He, M.; Zhang, Y. Prevalence of major subtypes of dementia in people over 65 years old in Xujiahui Street, Shanghai. Chin. J. Gerontol. 2013, 33, 1365–1366. [Google Scholar]
- Wu, Y.; Cheng, Z.; Bao, Z.; Fan, J.; Tang, L.; Guo, T. Survey on the status of Alzheimer’s disease and psychological health of family caregivers in Wuxi. Chin. Prev. Med. 2017, 18, 7. [Google Scholar]
- Yang, C.; Chen, J.; Wu, M.; Pan, Y.; Wang, N.; Wu, L.; Huang, G. Investigation and analysis of the incidence of Alzheimer’s disease in Nanchang community. Chin. J. Gerontol. 2016, 36, 5709–5711. [Google Scholar]
- Yu, Y.; Zhang, N.; Dong, J.; Lou, Y.; Xiao, W. Prevalence of Dementia among the Elderly and Its Influential Factors. Chin. Gen. Pract. 2012, 15, 2685–2687. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, H.; Lu, X.-L.; Zhang, B.; Weng, W.; Yang, J.; Zhang, J.; Dong, M.-J. Prevalence of dementia in the People’s Republic of China from 1985 to 2015: A systematic review and meta-regression analysis. BMC Public Health 2019, 19, 578. [Google Scholar] [CrossRef]
- Chenze, J.; Shouchao, W.; Tingting, L.; Xiao, B.; Wenrong, C.; Zhimin, L.; Wanjuan, P.; Wei, W.; Zhou, L. The prevalence of vascular dementia in China: A systematic review and meta-analysis from 2009–2019. Iran. J. Public Health 2021, 50, 11. [Google Scholar]
- Ding, H.; Chen, Y.; Yu, M.; Zhong, J.; Hu, R.; Chen, X.; Wang, C.; Xie, K.; Eggleston, K. The effects of chronic disease management in primary health care: Evidence from rural China. J. Health Econ. 2021, 80, 102539. [Google Scholar] [CrossRef]
- Wittenberg, R.; Hu, B.; Barraza-Araiza, L.; Rehill, A. Projections of Older People with Dementia and Costs of Dementia Care in the United Kingdom, 2019–2040; London School of Economics: London, UK, 2019. [Google Scholar]
- Farina, N.; Ibnidris, A.; Alladi, S.; Comas-Herrera, A.; Albanese, E.; Docrat, S.; Ferri, C.P.; Freeman, E.; Govia, I.; Jacobs, R. A systematic review and meta-analysis of dementia prevalence in seven developing countries: A STRiDE project. Glob. Public Health 2020, 15, 1878–1893. [Google Scholar] [CrossRef]
- Bacigalupo, I.; Mayer, F.; Lacorte, E.; Di Pucchio, A.; Marzolini, F.; Canevelli, M.; Di Fiandra, T.; Vanacore, N. A systematic review and meta-analysis on the prevalence of dementia in Europe: Estimates from the highest-quality studies adopting the DSM IV diagnostic criteria. J. Alzheimer’s Dis. 2018, 66, 1471–1481. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Auta, A.; Ezejimofor, M.; Oyedokun, A.; Harhay, M.O.; Rudan, I.; Chan, K.Y. Prevalence of dementia in Nigeria: A systematic review of the evidence. J. Glob. Health Rep. 2019, 3, e2019014. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, A.; Ranjan, J.K.; Asthana, H.S. Prevalence of dementia in India: A systematic review and meta-analysis. Indian J. Public Health 2021, 65, 152–158. [Google Scholar] [PubMed]
- Jang, J.-W.; Park, J.H.; Kim, S.; Lee, S.-H.; Lee, S.-H.; Kim, Y.-J. Prevalence and incidence of dementia in South Korea: A nationwide analysis of the national health insurance service senior cohort. J. Clin. Neurol. 2021, 17, 249. [Google Scholar] [CrossRef]
- Lan, D.; Ji, W.; Lin, B.; Chen, Y.; Huang, C.; Xiong, X.; Fu, M.; Mipam, T.D.; Ai, Y.; Zeng, B. Correlations between gut microbiota community structures of Tibetans and geography. Sci. Rep. 2017, 7, 16982. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015-The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Jia, J.; Wang, F.; Wei, C.; Zhou, A.; Jia, X.; Li, F.; Tang, M.; Chu, L.; Zhou, Y.; Zhou, C. The prevalence of dementia in urban and rural areas of China. Alzheimer’s Dement. 2014, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Tu, S.; Ge, D.; Li, T.; Liu, Y. The allocation and management of critical resources in rural China under restructuring: Problems and prospects. J. Rural. Stud. 2016, 47, 392–412. [Google Scholar] [CrossRef]
- Ngandu, T.; von Strauss, E.; Helkala, E.-L.; Winblad, B.; Nissinen, A.; Tuomilehto, J.; Soininen, H.; Kivipelto, M. Education and dementia: What lies behind the association? Neurology 2007, 69, 1442–1450. [Google Scholar] [CrossRef]
- Deckers, K.; Cadar, D.; van Boxtel, M.P.; Verhey, F.R.; Steptoe, A.; Köhler, S. Modifiable risk factors explain socioeconomic inequalities in dementia risk: Evidence from a population-based prospective cohort study. J. Alzheimer’s Dis. 2019, 71, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Sharp, E.S.; Gatz, M. The relationship between education and dementia an updated systematic review. Alzheimer Dis. Assoc. Disord. 2011, 25, 289. [Google Scholar] [CrossRef]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef]
- Fuhlbrigge, A.; Marvel, J.; Electricwala, B.; Siddall, J.; Scott, M.; Middleton-Dalby, C.; Small, M. Physician–Patient Concordance in the Assessment of Asthma Control. J. Allergy Clin. Immunol. Pract. 2021, 9, 3080–3088.e1. [Google Scholar] [CrossRef]
- Cao, Q.; Tan, C.-C.; Xu, W.; Hu, H.; Cao, X.-P.; Dong, Q.; Tan, L.; Yu, J.-T. The prevalence of dementia: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2020, 73, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Cheng, G.; An, L.; Gan, X.; Wu, Y.; Zhang, B.; Hu, S.; Zeng, Y.; Wu, L. Public Knowledge about Dementia in China: A National WeChat-Based Survey. Int. J. Environ. Res. Public Health 2019, 16, 4231. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Cheung, D.S.K.; Leung, A.Y.M.; Davidson, P.M. Bibliotherapy for improving caregiving appraisal of informal caregivers of people with dementia: A pilot randomized controlled trial. Res. Nurs. Health 2021, 44, 692–703. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| Bo, 2019 [19] | Y | Y | Y | Y | Y | Y | U | Y | U |
| Cheng, 2014 [20] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Deng, 2018 [21] | Y | Y | Y | Y | U | Y | Y | U | Y |
| Ding, 2020 [22] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Ge, 2014 [23] | Y | Y | Y | Y | U | Y | Y | U | Y |
| Guan, 2018 [24] | Y | Y | Y | Y | Y | U | U | Y | Y |
| Hu, 2018 [25] | Y | N/A | Y | Y | Y | U | U | Y | N/A |
| Huang, 2019 [26] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Huang, 2016 [27] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Ji, 2015 [11] | Y | U | Y | Y | Y | Y | Y | Y | Y |
| Jia, 2020 [28] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Kang, 2011 [29] | Y | Y | Y | Y | U | Y | Y | U | Y |
| Lao, 2011 [30] | Y | Y | Y | Y | U | Y | Y | U | Y |
| Liao, 2015 [31] | Y | U | Y | Y | U | U | U | U | Y |
| Ma, 2013 [32] | Y | Y | Y | Y | U | Y | Y | U | Y |
| Wu, 2017 [33] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Yang, 2016a [12] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Yang, 2016b [34] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Yu, 2012 [35] | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Studies | Design | Setting | Sample Size (Female) | Age | Case Identification | Prevalence | Incidence | Mortality |
|---|---|---|---|---|---|---|---|---|
| Bo, 2019 [19] | Longitudinal study | Both | 77 million (49%) | All ages | ICD-10 | N/A | N/A | 2010 y: 2845; 2011 y: 2890; 2012 y: 3155; 2013 y: 10,654; 2014 y: 11,466; 2015 y: 12,187 |
| Cheng, 2014 [20] | Cross-sectional study | Rural | 1472 (54.8%) | 69.7 ± 7.1 | C-MMSE, DSM-IV, NIA-AA, NINDS-AIREN | Dementia: 5.37%; AD: 3.60%; VaD: 1.43% | N/A | N/A |
| Deng, 2018 [21] | Cross-sectional study | Both | 1781 (60.5%) | 60–69 y: 46% 70–79 y: 41.5% >80 y: 12.5% | C-MMSE, IADL | 10.44% | N/A | N/A |
| Ding, 2020 [22] | Longitudinal study | Urban | 3670 (55.4%) | 55–64 y: 36% 65–74 y: 31% 75–84 y: 27.1% ≥85 y: 5.9% | C-MMSE, ADL, Clinical Dementia Rating Scale, DSM-IV | 2.30% | 1.33% | N/A |
| Ge, 2014 [23] | Cross-sectional study | Both | 10,026 (51.7%) | 75.4 ± 10.2 | MMSE, DSM-IV | 3.66% | N/A | N/A |
| Guan, 2018 [24] | Cross-sectional study | Rural | 760 (47%) | 60–69 y: 38.7% 70–79 y: 35% ≥80 y: 26.3% | GMS, self-developed dementia cognition scale | 5.26% | N/A | N/A |
| Hu, 2018 [25] | Longitudinal study | Urban | 778,389 (50.4%) | ≥60 | ICD-10 | N/A | N/A | 2010 y: 15.73 (1/105) 2011 y: 13.94 (1/105) 2012 y: 16.70 (1/105) 2013 y: 22.81 (1/105) 2014 y: 26.80 (1/105) 2015 y: 21.58 (1/105) |
| Huang Fu, 2019 [26] | Cross-sectional study | Urban | 6419 (56.8%) | 67.1 ± 5.4 | DSM-IV, MMSE, ADL, MoCA, CCMD-3 | 4.02% | N/A | N/A |
| Huang, 2016 [27] | Cross-sectional study | Both | 3974 (61.6%) | 60–64 y: 24.5% 65–69 y: 24.8% 70–74 y: 20.9% 75–79 y: 16.4% 80–84 y: 9.2% ≥85 y: 4.2% | MMSE, ADL, Hachinski Ischemic Scale | 1.33% | N/A | N/A |
| Ji, 2015 [11] | Cross-sectional study | Rural | 5578 (55.5%) | ≥60 | MMSE | 7.7% | N/A | N/A |
| Jia, 2020 [28] | Cross-sectional study | Both | 46,011 (50.3%) | ≥60 | MMSE, MoCA, WHO California-Los Angeles Auditory Verbal test | 6.0% | N/A | N/A |
| Kang, 2011 [29] | Cross-sectional study | Both | 3632 (46.7%) | 70.90 ± 7.2 | MMSE | 7.24% | N/A | N/A |
| Lao, 2011 [30] | Cross-sectional study | Both | 7665 (54.2%) | 66.4 ± 10.0 | HDS | 2.07% | N/A | N/A |
| Liao, 2015 [31] | Cross-sectional study | Urban | 9733 (50.9%) | 72.3 ± 6.5 | MMSE | 6.29% | N/A | N/A |
| Ma, 2013 [32] | Cross-sectional study | Urban | 2442 (53.7%) | 75.8 ± 7.6 | MMSE | 8.44% | N/A | N/A |
| Wu, 2017 [33] | Cross-sectional study | Both | 4195 (51.1%) | 71.0 ± 7.6 | MMSE | AD: 4.89% | N/A | N/A |
| Yang, 2016a [12] | Longitudinal study | Urban | 9733 (50.9%) | 72.8± 7.8 | MMSE | N/A | 13.13/1000 person-years (AD) | N/A |
| Yang, 2016b [34] | Cross-sectional study | Both | 2015 (58.8%) | 79.5 ± 7.6 | NIA-AA, MMSE, CDR | Dementia: 18.3%; AD: 5.6%; VaD: 0.3% | N/A | N/A |
| Yu, 2012 [35] | Longitudinal study | Urban | 129 (34.1%) | 83.5 ± 3.5 | MMSE | 17.02% | 9.30% | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, Y.; Tam, H.L.; Quint, J.; Chen, M.; Ding, R.; Zhang, X. Epidemiology of Dementia in China in 2010–2020: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 334. https://doi.org/10.3390/healthcare12030334
Yin Y, Tam HL, Quint J, Chen M, Ding R, Zhang X. Epidemiology of Dementia in China in 2010–2020: A Systematic Review and Meta-Analysis. Healthcare. 2024; 12(3):334. https://doi.org/10.3390/healthcare12030334
Chicago/Turabian StyleYin, Yueheng, Hon Lon Tam, Jennifer Quint, Mengyun Chen, Rong Ding, and Xiubin Zhang. 2024. "Epidemiology of Dementia in China in 2010–2020: A Systematic Review and Meta-Analysis" Healthcare 12, no. 3: 334. https://doi.org/10.3390/healthcare12030334
APA StyleYin, Y., Tam, H. L., Quint, J., Chen, M., Ding, R., & Zhang, X. (2024). Epidemiology of Dementia in China in 2010–2020: A Systematic Review and Meta-Analysis. Healthcare, 12(3), 334. https://doi.org/10.3390/healthcare12030334