
A Comparative Analysis of Emotional Regulation and Maladaptive Symptoms in Adolescents: Insights from Iran and Belgium
 , , , , and
, , , , and
Abstract
:1. Introduction
The Present Study
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Preliminary Analysis
3.2. Multivariate Analysis of Variance
3.3. Hierarchical Regression Analyses
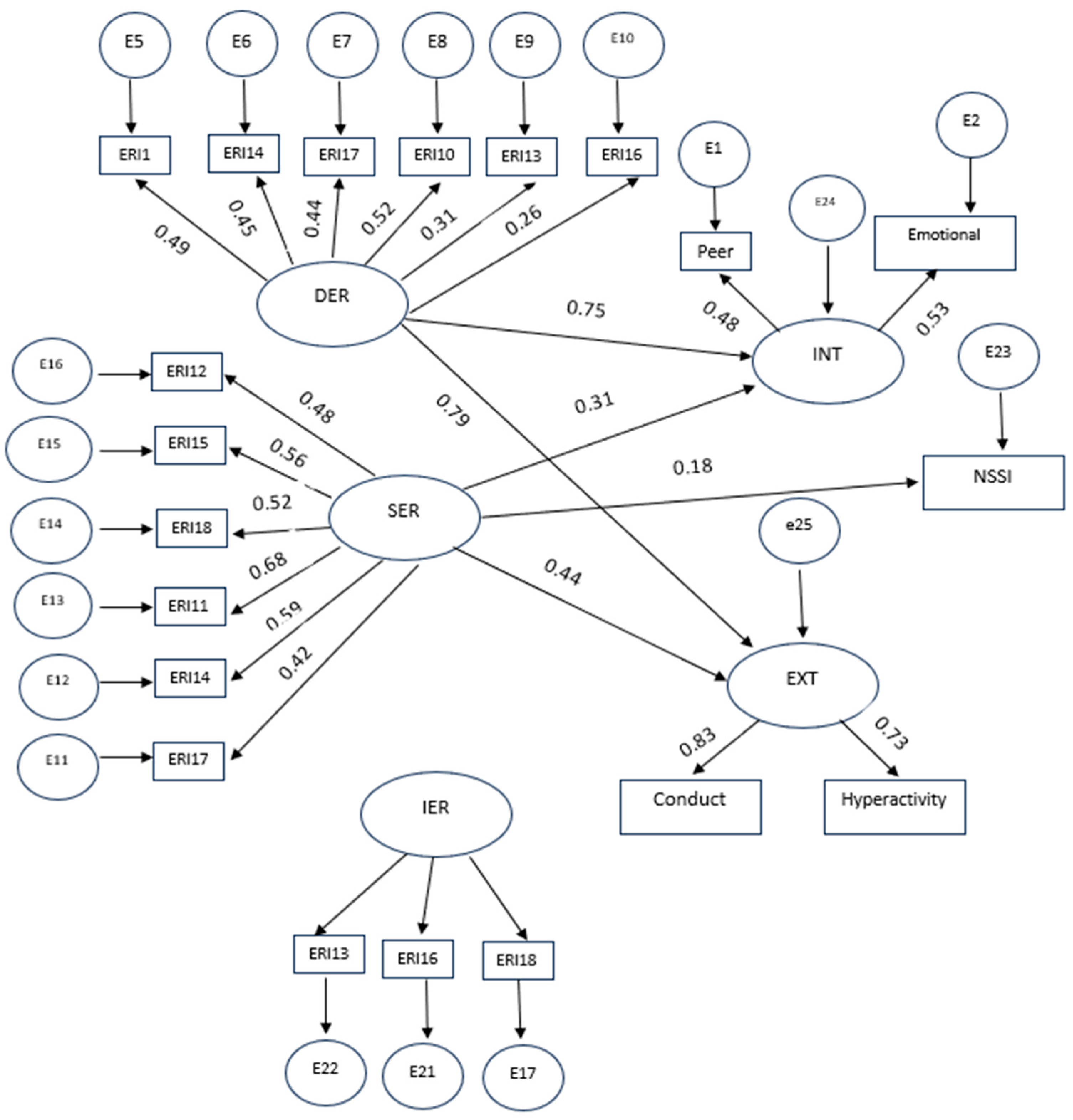
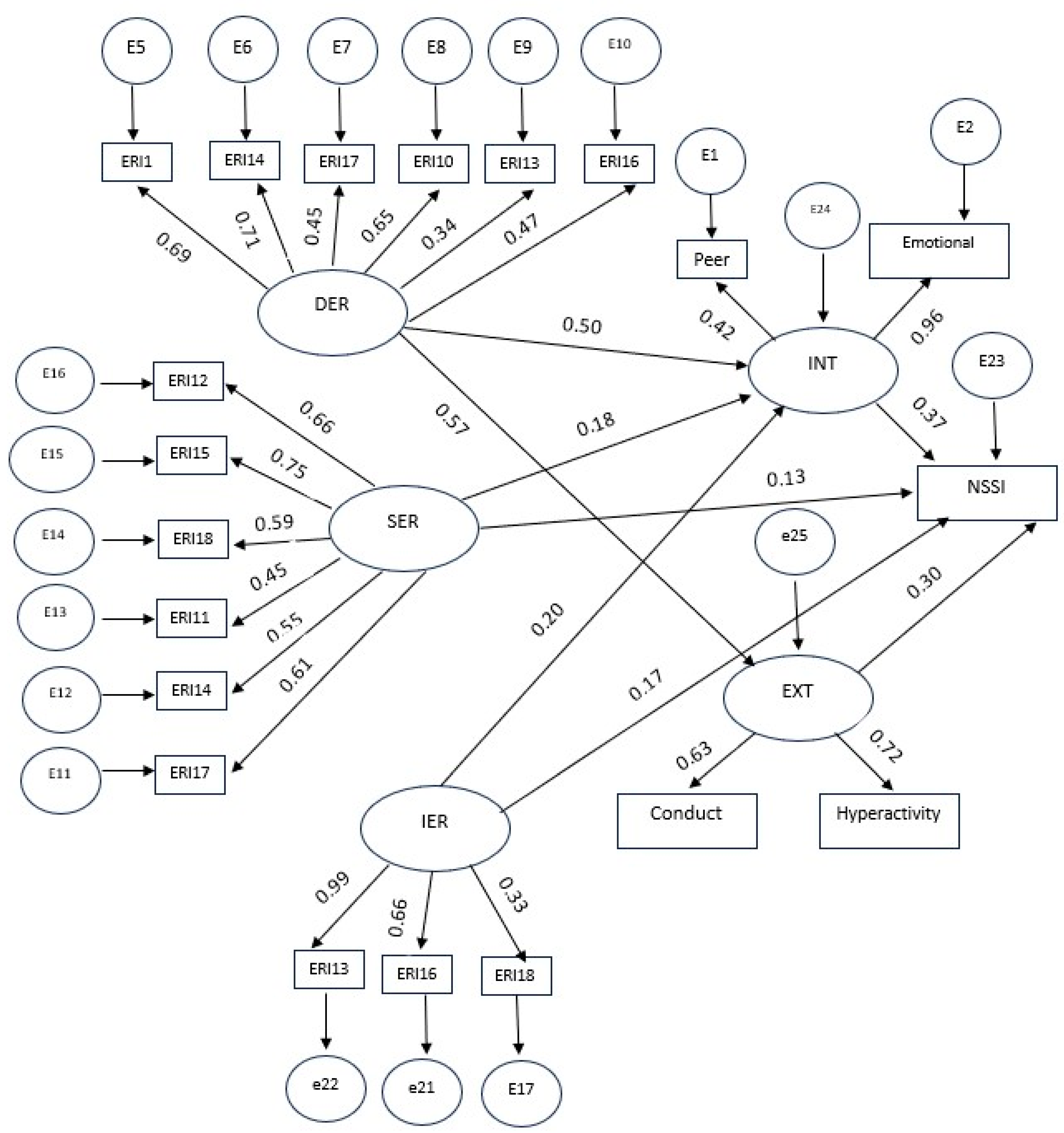
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gross, J.J. Emotion Regulation: Current Status and Future Prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- McRae, K.; Gross, J.J. Emotion Regulation. Emotion 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, T.; Schulze, L.; Renneberg, B. The Role of Emotion Regulation in the Characterization, Development and Treatment of Psychopathology. Nat. Rev. Psychol. 2022, 1, 272–286. [Google Scholar] [CrossRef]
- Compas, B.E.; Jaser, S.S.; Bettis, A.H.; Watson, K.H.; Gruhn, M.A.; Dunbar, J.P.; Williams, E.; Thigpen, J.C. Coping, Emotion Regulation, and Psychopathology in Childhood and Adolescence: A Meta-Analysis and Narrative Review. Psychol. Bull. 2017, 143, 939–991. [Google Scholar] [CrossRef]
- Werner, K.; Gross, J.J. Emotion Regulation and Psychopathology: A Conceptual Framework. In Emotion Regulation and Psychopathology: A Transdiagnostic Approach to Etiology and Treatment; The Guilford Press: New York, NY, USA, 2010; pp. 13–37. [Google Scholar]
- DeSteno, D.; Gross, J.J.; Kubzansky, L. Affective Science and Health: The Importance of Emotion and Emotion Regulation. Health Psychol. 2013, 32, 474. [Google Scholar] [CrossRef]
- Gardner, S.E.; Betts, L.R.; Stiller, J.; Coates, J. The Role of Emotion Regulation for Coping with School-Based Peer-Victimisation in Late Childhood. Personal. Individ. Differ. 2017, 107, 108–113. [Google Scholar] [CrossRef]
- Klein, R.; Nguyen, N.; Gyorda, J.; Jacobson, N. Adolescent Emotion Regulation and Future Psychopathology: A Prospective Transdiagnostic Analysis. J. Youth Adolesc. 2022, 32, 1592–1611. [Google Scholar] [CrossRef]
- Thomas, C.; Zolkoski, S. Preventing Stress among Undergraduate Learners: The Importance of Emotional Intelligence, Resilience, and Emotion Regulation. Front. Educ. 2020, 5, 94. [Google Scholar] [CrossRef]
- Bonanno, G.; Burton, C. Regulatory Flexibility: An Individual Differences Perspective on Coping and Emotion Regulation. Perspect. Psychol. Sci. 2013, 8, 591–612. [Google Scholar] [CrossRef]
- Roth, G.; Benita, M.; Amrani, C.; Shahar, B.; Asoulin, H.; Moed, A.; Bibi, U.; Kanat-Maymon, Y. Integration of Negative Emotional Experience Versus Suppression: Addressing the Question of Adaptive Functioning. Emotion 2014, 14, 908. [Google Scholar] [CrossRef]
- Ryan, R.; Deci, E. Self-Regulation and the Problem of Human Autonomy: Does Psychology Need Choice, Self-Determination, and Will? J. Personal. 2006, 74, 1557–1585. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.; Vansteenkiste, M.; Ryan, R. Integrative Emotion Regulation: Process and Development from a Self-Determination Theory Perspective. Dev. Psychopathol. 2019, 31, 945–956. [Google Scholar] [CrossRef] [PubMed]
- Silvers, J. Adolescence as a Pivotal Period for Emotion Regulation Development For Consideration at Current Opinion in Psychology. Curr. Opin. Psychol. 2021, 44, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Bailen, N.H.; Green, L.M.; Thompson, R.J. Understanding Emotion in Adolescents: A Review of Emotional Frequency, Intensity, Instability, and Clarity. Emot. Rev. 2019, 11, 63–73. [Google Scholar] [CrossRef]
- Maciejewski, D.; Lier, P.; Branje, S.; Meeus, W. A 5-Year Longitudinal Study on Mood Variability Across Adolescence Using Daily Diaries. Child Dev. 2015, 86, 1908–1921. [Google Scholar] [CrossRef] [PubMed]
- Brenning, K.; Soenens, B.; Vansteenkiste, M.; De Clercq, B.; Antrop, I. Emotion regulation as a transdiagnostic risk factor for (non)clinical adolescents’ internalizing and externalizing psychopathology: Investigating the intervening role of psychological need experiences. Child Psychiatry Hum. Dev. 2022, 53, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Brenning, K.; Waterschoot, J.; Dieleman, L.; Morbée, S.; Vermote, B.; Soenens, B.; Van der Kaap-Deeder, J.; van den Bogaard, D.; Vansteenkiste, M. The role of emotion regulation in mental health during the COVID-19 outbreak: A 10-wave longitudinal study. Stress Health 2023, 39, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Scharf, N.; Benita, M.; Benish-Weisman, M. Emotion Regulation Styles and Adolescent Adjustment Following a COVID-19 Lockdown. Stress Health 2023. early view. [Google Scholar]
- Benita, M.; Benish-Weisman, M.; Matos, L.; Torres, C. Integrative and Suppressive Emotion Regulation Differentially Predict Well-Being through Basic Need Satisfaction and Frustration: A Test of Three Countries. Motiv. Emot. 2020, 44, 67–81. [Google Scholar] [CrossRef]
- Brenning, K.; Soenens, B.; Van Petegem, S.; Vansteenkiste, M. Perceived Maternal Autonomy Support and Early Adolescent Emotion Regulation: A Longitudinal Study. Soc. Dev. 2015, 24, 561–578. [Google Scholar] [CrossRef]
- Vatandoost, S.; Baetens, I.; Van Den Meersschaut, J.; Van Heel, M.; Van Hove, L. The impact of the COVID-19 pandemic on the incidence of non-suicidal self-injury; a comparison between Iran and Belgium. Clin. Med. Insights Psychiatry 2023, 14, 1–12. [Google Scholar] [CrossRef]
- Brausch, A.; Clapham, R.; Littlefield, A. Identifying Specific Emotion Regulation Deficits That Associate with Nonsuicidal Self-Injury and Suicide Ideation in Adolescents. J. Youth Adolesc. 2022, 51, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Lan, Z.; Pau, K.; Md Yusof, H.; Huang, X. The Effect of Emotion Regulation on Non-Suicidal Self-Injury among Adolescents: The Mediating Roles of Sleep, Exercise, and Social Support. Psychol. Res. Behav. Manag. 2022, 15, 1451–1463. [Google Scholar] [CrossRef]
- Robinson, K.; Garisch, J.A.; Kingi, T.; Brocklesby, M.; O’Connell, A.; Langlands, R.L.; Russell, L.; Wilson, M.S. Reciprocal Risk: The Longitudinal Relationship between Emotion Regulation and Non-Suicidal Self-Injury in Adolescents. J. Abnorm. Child Psychol. 2019, 47, 325–332. [Google Scholar] [CrossRef] [PubMed]
- International Society for the Study of Self-Injury. What Is Self-Injury? International Society for the Study of Self-Injury: Cambridge, MA, USA, 2018. [Google Scholar]
- Baetens, I.; Greene, D.; Van Hove, L.; Van Leeuwen, K.; Wiersema, R.; Desoete, A.; Roelants, M. Predictors and consequences of non-suicidal self-injury in relation to life, peer, and school factors. J. Adolesc. 2021, 90, 100–108. [Google Scholar] [CrossRef]
- Cassels, M.; Wilkinson, P. Non-suicidal self-injury in adolescence. Paediatrics and Child Health. 2016, 26, 554–558. [Google Scholar] [CrossRef]
- Robinson, K.; Garisch, J.A.; Wilson, M.S. Nonsuicidal self-injury thoughts and behavioural characteristics: Associations with suicidal thoughts and behaviours among community adolescents. J. Affect. Disord. 2021, 282, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Gee, D.G.; De Los Reyes, A.; Seager, I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Dev. Psychopathol. 2016, 28, 927–946. [Google Scholar] [CrossRef]
- Cludius, B.; Mennin, D.; Ehring, T. Emotion Regulation as a Transdiagnostic Process. Emotion 2020, 20, 37–42. [Google Scholar] [CrossRef]
- Cole, P.M.; Hall, S.E.; Hajal, N.J.; Beauchaine, T.P.; Hinshaw, S.P. Emotion dysregulation as a vulnerability to psychopathology. In Child and Adolescent Psychopathology; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 346–386. [Google Scholar] [CrossRef]
- Cai, R.Y.; Hardan, A.Y.; Phillips, J.M.; Frazier, T.W.; Uljarević, M. Brief Report: Emotion Regulation Influences on Internalizing and Externalizing Symptoms across the Normative-Clinical Continuum. Front. Psychiatry 2021, 12, 693570. [Google Scholar] [CrossRef]
- Cavicchioli, M.; Stefanazzi, C.; Tobia, V.; Ogliari, A. The Role of Attachment Styles in Attention-Deficit Hyperactivity Disorder: A Meta-Analytic Review from the Perspective of a Transactional Development Model. Eur. J. Dev. Psychol. 2022, 20, 436–464. [Google Scholar] [CrossRef]
- Schneider, R.; Arch, J.; Landy, L.; Hankin, B. The Longitudinal Effect of Emotion Regulation Strategies on Anxiety Levels in Children and Adolescents. J. Clin. Child Adolesc. Psychol. 2016, 47, 978–991. [Google Scholar] [CrossRef]
- Baetens, I.; Claes, L.; Muehlenkamp, J.; Grietens, H.; Onghena, P. Differences in Psychological Symptoms and Self-Competencies in Non-Suicidal Self-Injurious Flemish Adolescents. J. Adolesc. 2012, 35, 753–759. [Google Scholar] [CrossRef]
- Cipriano, A.; Cella, S.; Cotrufo, P. Nonsuicidal Self-Injury: A Systematic Review. Front. Psychol. 2017, 8, 1946. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.; Prinstein, M. A Functional Approach to the Assessment of Self-Mutilative Behavior. J. Consult. Clin. Psychol. 2004, 72, 885–890. [Google Scholar] [CrossRef]
- Kranzler, A.; Fehling, K.B.; Anestis, M.D.; Selby, E.A. Emotional dysregulation, internalizing symptoms, and self-injurious and suicidal behavior: Structural equation modeling analysis. Death Stud. 2016, 40, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Arens, E.A.; Balkir, N.; Barnow, S. Ethnic Variation in Emotion Regulation: Do Cultural Differences End Where Psychopathology Begins? J. Cross-Cult. Psychol. 2013, 44, 335–351. [Google Scholar] [CrossRef]
- Matsumoto, D.; Yoo, S.H.; Nakagawa, S. Culture, Emotion Regulation, and Adjustment. J. Personal. Soc. Psychol. 2008, 94, 925–937. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J.-L.; Mistry, R.; Ran, G.; Wang, X. Relation between Emotion Regulation and Mental Health: A Meta-Analysis Review. Psychol. Rep. 2014, 114, 341–362. [Google Scholar] [CrossRef]
- Diener, M.L.; Lucas, R.E. Adults’ Desires for Children’s Emotions Across 48 Countries: Associations with Individual and National Characteristics. J. Cross-Cult. Psychol. 2004, 35, 525–547. [Google Scholar] [CrossRef]
- Hofstede, G. Empirical Models of Cultural Differences. In Contemporary Issues in Cross-Cultural Psychology; Swets & Zeitlinger Publishers: Lisse, The Netherlands, 1991; pp. 4–20. [Google Scholar]
- Ghorbani, N.; Bing, M.N.; Watson, P.J.; Davison, H.K.; LeBreton, D.L. Individualist and Collectivist Values: Evidence of Compatibility in Iran and the United States. Personal. Individ. Differ. 2003, 35, 431–447. [Google Scholar] [CrossRef]
- Sharifzadeh, V. Middle Eastern-rooted families. In Developing Cross-Cultural Competence, 3rd ed.; Lynch, E., Hanson, M., Eds.; Brookes: Baltimore, MD, USA, 2004; pp. 373–410. [Google Scholar]
- Boiger, M.; Ceulemans, E.; De Leersnyder, J.; Uchida, Y.; Norasakkunkit, V.; Mesquita, B. Beyond Essentialism: Cultural Differences in Emotions Revisited. Emotion 2018, 18, 1142–1162. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.R.; Kitayama, S. Culture and the Self: Implications for Cognition, Emotion, and Motivation. Psychol. Rev. 1991, 98, 224–253. [Google Scholar] [CrossRef]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef]
- Goodman, A.; Goodman, R. Strengths and Difficulties Questionnaire as a Dimensional Measure of Child Mental Health. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Muris, P.; Meesters, C.; van den Berg, F. The Strengths and Difficulties Questionnaire (SDQ)—Further evidence for its reliability and validity in a community sample of Dutch children and adolescents. Eur. Child Adolesc. Psychiatry 2003, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Mohammadi, M.R.; Md, J.; Tehranidoost, M.; Shahrivar, Z.; Saadat, S. The Farsi Version of the Strength and Difficulties Questionnaire Selfreport Form: The Normative Data and Scale Properties. Iran. J. Child Neurol. 2009, 3, 27–34. [Google Scholar]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.; Assor, A.; Niemiec, C.P.; Ryan, R.M.; Deci, E.L. The Emotional and Academic Consequences of Parental Conditional Regard: Comparing Conditional Positive Regard, Conditional Negative Regard, and Autonomy Support as Parenting Practices. Dev. Psychol. 2009, 45, 1119–1142. [Google Scholar] [CrossRef]
- Brenning, K.; Soenens, B.; Braet, C.; Bosmans, G. Attachment and depressive symptoms in middle childhood and early adolescence: Testing the validity of the emotion regulation model of attachment. Pers. Relatsh. 2012, 19, 445–464. [Google Scholar] [CrossRef]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pr. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Sansone, R.A.; Wiederman, M.W.; Sansone, L.A. The Self-Harm Inventory (SHI): Development of a Scale for Identifying Self-Destructive Behaviors and Borderline Personality Disorder. J. Clin. Psychol. 1998, 54, 973–983. [Google Scholar] [CrossRef]
- Baetens, I.; Claes, L.; Willem, L.; Muehlenkamp, J.; Bijttebier, P. The Relationship between Non-Suicidal Self-Injury and Temperament in Male and Female Adolescents Based on Child- and Parent-Report. Personal. Individ. Differ. 2011, 50, 527–530. [Google Scholar] [CrossRef]
- Tahbaz Hoseinzadeh, S.; Ghorbani, N.; Nabavi, S. Comparison of selfdestructive tendencies and integrative self-knowledge among multiple sclerosis and healthy people. Contemp. Psychol. 2011, 6, 35–44. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1998. [Google Scholar] [CrossRef]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; Volume 1. [Google Scholar]
- McLaughlin, K.A.; Sheridan, M.A.; Tibu, F.; Fox, N.A.; Zeanah, C.H.; Nelson, C.A. Causal Effects of the Early Caregiving Environment on Development of Stress Response Systems in Children. Proc. Natl. Acad. Sci. USA 2015, 112, 5637–5642. [Google Scholar] [CrossRef]
- Dvir, Y.; Ford, J.D.; Hill, M.; Frazier, J.A. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harv. Rev. Psychiatry 2014, 22, 149–161. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; Möhler, E.; Plener, P.; Popow, C. Emotional Dysregulation in Children and Adolescents with Psychiatric Disorders. A Narrative Review. Front. Psychiatry 2021, 12, 628252. [Google Scholar] [CrossRef]
- Clapham, R.; Brausch, A. Internalizing and Externalizing Symptoms Moderate the Relationship between Emotion Dysregulation and Suicide Ideation in Adolescents. Child Psychiatry Hum. Dev. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; John, O.P. Individual Differences in Two Emotion Regulation Processes: Implications for Affect, Relationships, and Well-Being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Tamir, M.; McGonigal, K.M.; John, O.P.; Gross, J.J. The Social Costs of Emotional Suppression: A Prospective Study of the Transition to College. J. Personal. Soc. Psychol. 2009, 96, 883–897. [Google Scholar] [CrossRef]
- Mesquita, B.; Boiger, M. Emotions in Context: A Sociodynamic Model of Emotions. Emot. Rev. 2014, 6, 298–302. [Google Scholar] [CrossRef]
- Dadkhah, A.; Shirinbayan, P. Emotion Regulation Characteristics Development in Iranian Primary School Pupils. Iran. Rehabil. J. 2014, 12, 17–21. [Google Scholar]
- Soto, J.A.; Perez, C.R.; Kim, Y.-H.; Lee, E.A.; Minnick, M.R. Is Expressive Suppression Always Associated with Poorer Psychological Functioning? A Cross-Cultural Comparison between European Americans and Hong Kong Chinese. Emotion 2011, 11, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Hird, K.; Hasking, P.; Boyes, M. Relationships between Outcome Expectancies and Non-Suicidal Self-Injury: Moderating Roles of Emotion Regulation Difficulties and Self-Efficacy to Resist Self-Injury. Arch. Suicide Res. 2022, 26, 1688–1701. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | M (SD) | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|
| 1. INT | 7.52 (3.26) | 1 | |||||
| 2. EXT | 5.65 (3.83) | 0.06 | 1 | ||||
| 3. NSSI | 2.10 (2.09) | 0.16 ** | 0.54 ** | 1 | |||
| 4. DER | 2.77 (0.75) | 0.29 ** | 0.43 ** | 0.38 ** | 1 | ||
| 5. SER | 3.21 (0.84) | 0.32 ** | −0.37 ** | 0.18 ** | −0.07 | 1 | |
| 6. IER | 2.98 (0.79) | −0.09 | 0.11 | 0.001 | 0.14 * | −0.19 ** | 1 |
| Variables | M (SD) Belgium | M (SD) Iran | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. INT | 6.39 (3.55) | 8.55 (2.60) | 1 | 0.32 ** | 0.27 ** | 0.31 ** | 0.21 * | −0.03 |
| 2. EXT | 7.57 (3.53) | 3.81 (3.31) | 0.22 * | 1 | 0.57 ** | 0.48 ** | −0.26 ** | 0.11 |
| 3. NSSI | 0.39 ** | 0.33 ** | 1 | 0.42 ** | −0.13 | −0.03 | ||
| 4. DER | 2.86 (0.76) | 2.68 (0.73) | 0.39 ** | 0.38 ** | 0.32 ** | 1 | 0.04 | 0.13 |
| 5. SER | 2.72 (0.71) | 3.65 (0.70) | 0.15 | −0.03 | 0.19 * | −0.04 | 1 | 0.05 |
| 6. IER | 3.19 (0.69) | 2.79 (0.82) | 0.02 | −0.14 | −0.2 * | 0.09 | −0.19 * | 1 |
| Variables | Iran (n = 117) | Belgium (n = 107) | F |
|---|---|---|---|
| M (SD) | M (SD) | ||
| DER | 2.68 (0.74) | 2.86 (0.76) | 3.215 |
| SER | 3.65 (0.71) | 2.72 (0.71) | 95.9 ** |
| IER | 2.79 (0.82) | 3.19 (0.69) | 15.04 ** |
| Internalizing | 8.55 (2.6) | 6.39 (3.55) | 27.03 ** |
| Externalizing | 3.81 (3.3) | 7.57 (3.53) | 67.5 ** |
| NSSI | |||||
| β | SE | B | t | ||
| Model 1 | Age | −0.07 | 0.13 | −0.13 | −0.99 |
| Gender | −0.02 | 0.26 | −0.09 | −0.36 | |
| Country | −0.44 | 0.32 | −1.85 | −5.76 ** | |
| Model 2 | Age | −0.04 | 0.12 | −0.08 | −0.62 |
| Gender | −0.02 | 0.24 | −1.13 | 0.46 | |
| Country | −0.46 | 0.33 | −1.92 | −5.69 ** | |
| DER | 0.35 | 0.16 | 0.97 | 5.96 ** | |
| SER | 0.05 | 0.16 | 0.13 | 0.81 | |
| IER | −0.15 | 0.16 | −0.41 | −2.59 | |
| Internalizing problems | |||||
| β | SE | B | t | ||
| Model 1 | Age | 0.13 | 0.21 | 0.05 | 0.62 |
| Gender | −1.89 | 0.4 | −0.29 | −4.76 ** | |
| Country | 2.53 | 0.49 | 0.4 | 5.19 ** | |
| Model 2 | Age | 0.14 | 0.2 | 0.05 | 0.74 |
| Gender | −1.56 | 0.37 | −0.24 | −4.19 ** | |
| Country | 2.01 | 0.52 | 0.32 | 3.91 ** | |
| DER | 1.37 | 0.25 | 0.32 | 5.47 ** | |
| SER | 0.68 | 0.26 | 0.18 | 2.65 ** | |
| IER | −0.23 | 0.24 | −0.06 | −0.94 | |
| Externalizing problems | |||||
| β | SE | B | t | ||
| Model 1 | Age | −0.47 | 0.24 | −0.14 | −1.93 |
| Gender | 0.42 | 0.46 | 0.05 | 0.9 | |
| Country | −4.45 | 0.57 | −0.57 | −7.82 ** | |
| Model 2 | Age | −0.44 | 0.22 | −0.13 | −1.97 * |
| Gender | 0.88 | 0.42 | 0.11 | 2.08 * | |
| Country | −3.58 | 0.58 | −0.46 | −6.14 ** | |
| DER | 2.04 | 0.28 | 0.39 | 7.22 ** | |
| SER | −0.66 | 0.29 | −0.14 | −2.26 * | |
| IER | −0.13 | 0.27 | −0.03 | −0.47 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vatandoost, S.; Baetens, I.; Erjaee, Z.; Azadfar, Z.; Van Heel, M.; Van Hove, L. A Comparative Analysis of Emotional Regulation and Maladaptive Symptoms in Adolescents: Insights from Iran and Belgium. Healthcare 2024, 12, 341. https://doi.org/10.3390/healthcare12030341
Vatandoost S, Baetens I, Erjaee Z, Azadfar Z, Van Heel M, Van Hove L. A Comparative Analysis of Emotional Regulation and Maladaptive Symptoms in Adolescents: Insights from Iran and Belgium. Healthcare. 2024; 12(3):341. https://doi.org/10.3390/healthcare12030341
Chicago/Turabian StyleVatandoost, Shokoufeh, Imke Baetens, Zeinab Erjaee, Zahra Azadfar, Martijn Van Heel, and Lisa Van Hove. 2024. "A Comparative Analysis of Emotional Regulation and Maladaptive Symptoms in Adolescents: Insights from Iran and Belgium" Healthcare 12, no. 3: 341. https://doi.org/10.3390/healthcare12030341