

Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Appraisal
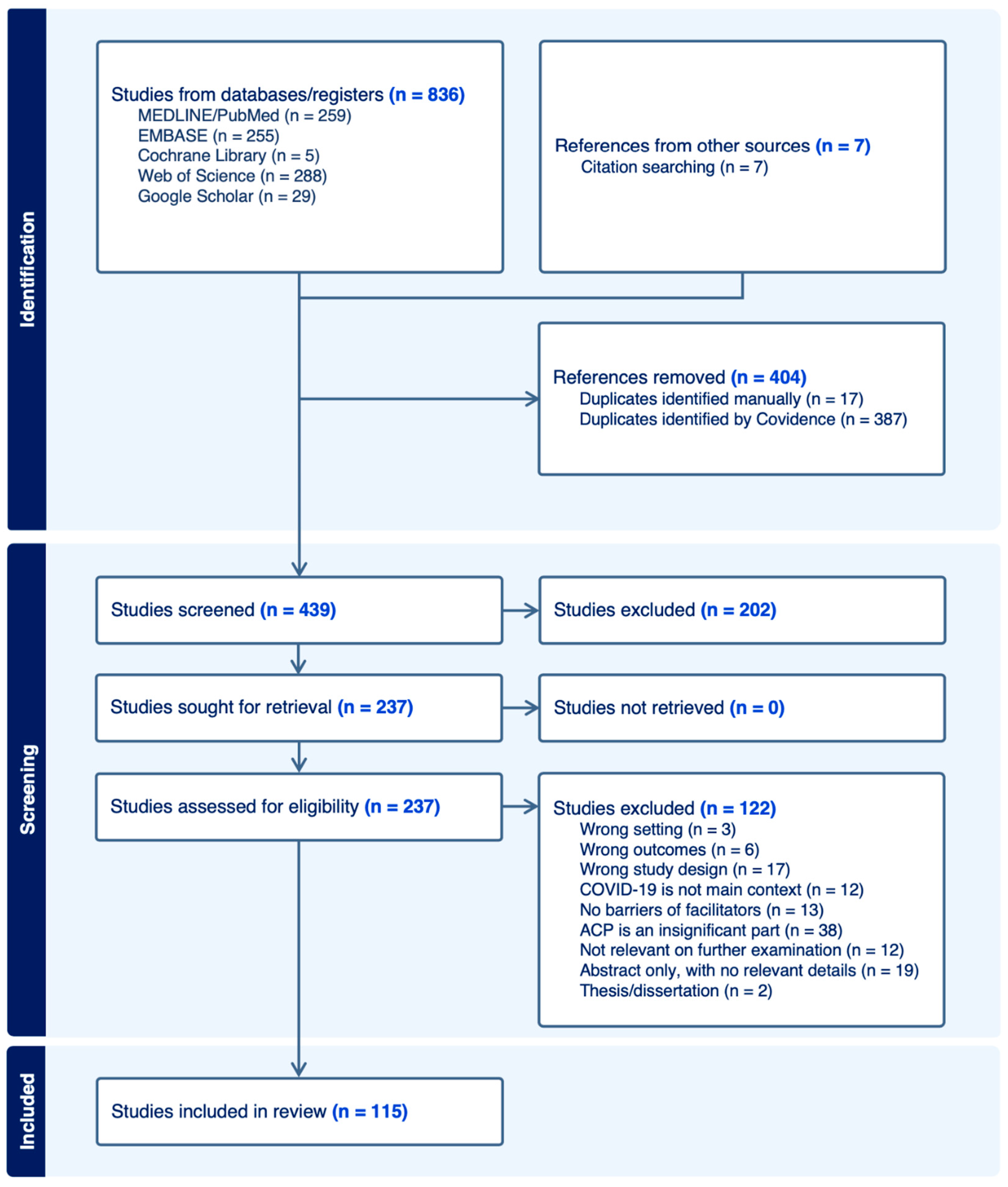
3. Results
3.1. Overview of the Results
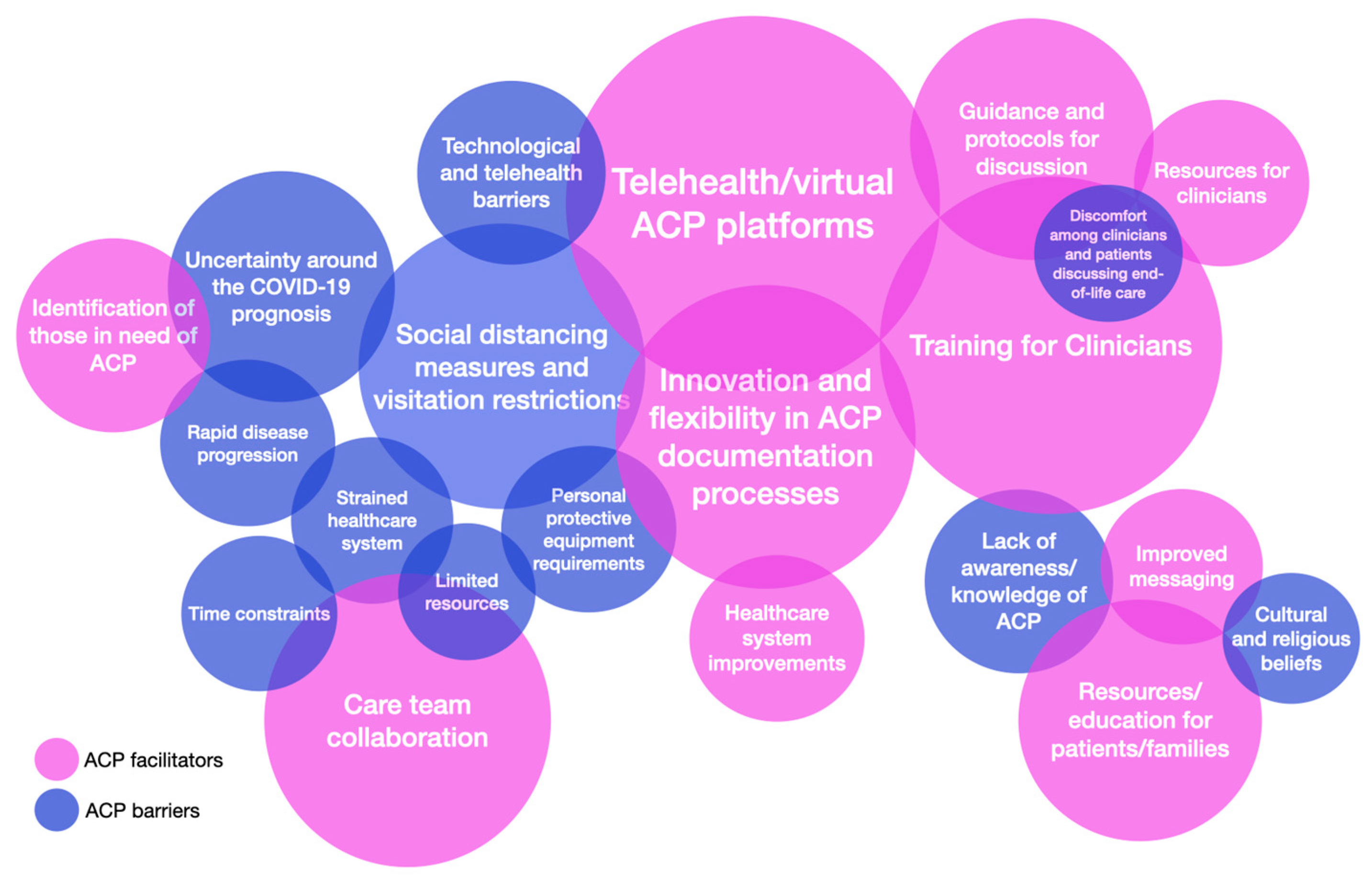
3.2. ACP Barriers and Facilitators during the COVID-19 Pandemic
3.2.1. Situation Category

{kind=link}
{kind=link}
| Study ID | Country | Setting | Population | Number of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| Mota Romero 2022 [35] | SP | NH | HP | 20 | ■ | Barriers: Lack of awareness/knowledge of ACP |
| Statler 2022 [36] | US | HO | PT | 356 | ■ | Barriers: Legal concerns; Uncertainty surrounding the COVID-19 prognosis; Limited resources; Healthcare system barriers; Discomfort among clinicians and patients discussing end-of-life care Facilitators: Resources/education for patients/families; Proactive ACP conversations; Telehealth/virtual ACP platforms; Identification of those in need of ACP |
| Porteny 2022 [37] | US | HO | PT | 76 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms |
| Epler 2022 [38] | US | HO | PT | 720 | ■ | Barriers: Discomfort among clinicians and patients discussing end-of-life care; Familial disagreement; Time constraints; Rapid disease progression |
| Kaehr 2022 * [39] | US | NH | HP | 17 | ■ | Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Uncertainty surrounding the COVID-19 prognosis |
| Sun 2022 [40] | US | HO | PT | 276 | ■ | Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Strained healthcare system; Uncertainty surrounding the COVID-19 prognosis Facilitators: Identification of those in need of ACP |
| Barnato 2022 [41] | US | ED | PT | 5394 | ■ | Facilitators: Diagnosis of dementia |
| Ter Brugge 2022 [42] | NL | NH | HP | 127 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Understanding/fear of COVID-19; Telehealth/virtual ACP platforms; Public awareness of ACP |
| Perumalswami 2022 [43] | US | HO | HP | 22 | ■ | Barriers: Technological/telehealth barriers |
| Jayes 2022 [44] | UK | HO, NH | HP | 107 | ■ | Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Time constraints |
| Janssen 2021 [45] | NL | HO | PT | ■ | Barriers: Uncertainty surrounding the COVID-19 prognosis; Time constraints; Negative perceptions about advance care planning Facilitators: Public awareness of ACP; Telehealth/virtual ACP platforms; Training for clinicians; Guidance and protocols for ACP discussions; Care team collaboration | |
| Brophy 2021 [46] | US | SV | PB | 522 | ■ | Barriers: Emotional barriers Facilitators: Understanding/fear of COVID-19 |
| Piers 2021 [47] | BL | HO | PT | 711 | ■ | Facilitators: ACP/palliative care experts: co-management by geriatricians |
| Bradshaw 2021 [48] | UK | NH | HP | 277 | ■ | Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Strained healthcare system; Rapid disease progression; Emotional barriers; Uncertainty surrounding the COVID-19 prognosis Facilitators: Innovation and flexibility in ACP documentation processes; Public awareness of ACP; Telehealth/virtual ACP platforms; Care team collaboration; ACP/palliative care experts; Training for clinicians |
| Dujardin 2021 [49] | NL | HO | HP | 15 | ■ | Barriers: Uncertainty surrounding the COVID-19 prognosis; Discomfort among clinicians and patients discussing end-of-life care; Technological/telehealth barriers; Social distancing measures and visitation restrictions; Time constraints; Healthcare system barriers Facilitators: Trusting clinical relationship; Telehealth/virtual ACP platforms; Healthcare system improvements |
| Connellan 2021 [50] | IR | ED | PT | 430 | ■ | Facilitators: Understanding/fear of COVID-19 |
| Vellani 2021 [51] | CN | NH | HP | 14 | ■ | Facilitators: ACP/palliative care experts; Telehealth/virtual ACP platforms; Care team collaboration; Proactive ACP Conversations |
| Toccafondi 2021 * [52] | IT | HO | PT | 110 | ■ | Facilitators: Guidance and protocols for ACP discussions |
| DeGette 2021 * [53] | US | HO | PT | 258 | ■ | Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Uncertainty surrounding the COVID-19 prognosis; Racial and ethnic barriers Facilitators: Identification of those in need of ACP |
| Copley 2021 [54] | UK | HO | PT | 164 | ■ | Facilitators: Resources for clinicians; Understanding/fear of COVID-19; Public awareness of ACP; Resources/education for patients/families |
| Lin 2021 [55] | TW | HO | PT | 2493 | ■ | Barriers: Social distancing measures and visitation restrictions; Lack of awareness/knowledge of ACP; Healthcare system barriers; Limited resources; Legal concerns; Discomfort among clinician and patients discussing end-of-life care; Time constraints; Strained healthcare system Facilitators: Telehealth/virtual ACP platforms |
| Ye 2021 [56] | US | NH | PT | 963 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Proactive ACP conversations |
| Huayanay 2021 [57] | US | HO | PT | 1 | ■ | Barriers: Communication difficulties; Cultural and religious beliefs; Financial concerns |
| Nguyen 2021 [58] | US | SV | PT | 100 | ■ | Facilitators: Public awareness of ACP; Improved messaging |
| Coles 2020 * [59] | UK | NH | HP | ■ | Facilitators: Care team collaboration; ACP/palliative care experts; Healthcare system improvements | |
| Wei 2020 [60] | US | HO | HP | ■ | Barriers: Rapid disease progression; Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms; Tablet computers; ACP/palliative care experts | |
| Maia 2020 * [61] | PO | HO | PT | 51 | ■ | Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Strained healthcare system; Technological/telehealth barriers |
| Hendriks 2022 [62] | NL | HO | PT | 275 | ■ | Facilitators: Training for clinicians; Resources for clinicians |
| Holdsworth L.M. 2022 [63] | US | HO | HP | 15 | ■ | Barriers: Technological/telehealth barriers; Social distancing measures and visitation restrictions Facilitators: Innovation and flexibility in ACP documentation processes |
| Dassel 2021 [64] | US | HC | FC | 82 | ■ | Barriers: Emotional barriers; Social distancing measures and visitation restrictions; Lack of awareness/knowledge of ACP Facilitators: Guidance and protocols for ACP discussions; Resources/education for patients/families |
| de Vries 2021 [65] | CN | SV | PB | 3923 | ■ | Barriers: Distrust in the healthcare system Facilitators: Resources/education for patients/families |
| Payne 2022 [66] | US | ED | PB | 50 | ■ | Barriers: Lack of awareness/knowledge of ACP Facilitators: Innovation and flexibility in ACP documentation processes; Resources/education for patients/families; Improved messaging |
| Ninteau 2022 [67] | US | NH | HP | 7 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: ACP/palliative care experts; Training for clinicians; Telehealth/virtual ACP platforms |
| Elizondo 2022 * [68] | AR | HO | PT | ■ | Facilitators: Care team collaboration; Innovation and flexibility in ACP documentation processes; Healthcare system improvements | |
| Hafid 2022 * [69] | CN | HO | HP | 48 | ■ | Facilitators: Public awareness of ACP; Resources/education for patients/families; Telehealth/virtual ACP platforms |
3.2.2. Education Category
| Study ID | Country | Setting | Population | No. of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| van de Wiel 2022 [70] | BL | AC | MS | 172 | ■ | Facilitators: Training for clinicians |
| Casey 2022 [71] | US | HO | PT | 143 | ■ | Facilitators: Training for clinicians; Guidance and protocols for ACP discussions; Innovation and flexibility in ACP documentation processes |
| Cousins 2022 [72] | UK | NH | HP, FM | 54 | ■ | Facilitators: Resources/education for patients/families; Resources for clinicians; Training for clinicians |
| Rosedale 2022 * [73] | US | HO | PT | ■ | Facilitators: Training for clinicians; ACP/palliative care experts | |
| Rabow 2021 [74] | US | OT | HP | ■ | Facilitators: Training for clinicians; Resources for clinicians | |
| Oulton 2021 [75] | US | HO | HP | 9 | ■ | Facilitators: Training for clinicians |
| Budidi 2021 * [76] | US | AC | HP | 30 | ■ | Barriers: Time constraints; Low education level; Communication difficulties; Technological/telehealth barriers; Lack of adequate ACP training for clinicians Facilitators: Training for clinicians |
| Price 2021 * [77] | US | HO | PT | 143 | ■ | Facilitators: Training for clinicians |
| Roberts 2020 [78] | US | AC | HP | ■ | Facilitators: Training for clinicians | |
| Markwalter 2022 * [79] | US | HO | PT | 143 | ■ | Facilitators: Training for clinicians; Resources for clinicians |
| Preston 2022 * [80] | UK | NH | HP, NH, FM | ■ | Barriers: Technological/telehealth barriers Facilitators: Training for clinicians; Resources/education for patients/families | |
| Cooney 2022 [81] | US | AC | MS | 83 | ■ | Facilitators: Training for clinicians |
| Holdsworth 2022 * [82] | UK | HO | PT | 69 | ■ | Facilitators: Training for clinicians; Identification of those in need of ACP; Guidance and protocols for ACP discussions |
| Volandes 2022 [83] | US | HO | PT | 14107 | ■ | Facilitators: Resources/education for patients/families; Training for clinicians |
| Mills 2021 [84] | US | HO | HP | 48 | ■ | Facilitators: Telehealth/virtual ACP platforms |
| Varey 2021 * [85] | UK | OT | HP, PT, FM | ■ | Facilitators: Resources/education for patients/families | |
| Phenwan 2021 [86] | TL | OT | MS, HP, PB | 103 | ■ | Barriers: Cultural and religious beliefs; Lack of awareness/knowledge of ACP Facilitators: Training for clinicians |
| Berning 2021 [87] | US | NH | PT | 581 | ■ | Facilitators: Care team collaboration; Identification of those in need of ACP; Guidance and protocols for ACP discussions |
| Dobert 2021 * [88] | US | NH | HP | ■ | Facilitators: Care team collaboration; Training for clinicians; Improved messaging; Resources for clinicians; Telehealth/virtual ACP platforms | |
| Smith 2020 [89] | US | OT | PT | 413 | ■ | Facilitators: Training for clinicians |
| McAfee 2022 [90] | US | AC | PB, HP | ■ | Barriers: Cultural and religious beliefs; Racial and ethnic barriers; Healthcare system barriers; Lack of awareness/knowledge of ACP; Low health literacy; Limited resources: accessibility to health directives | |
| Huang 2021 [91] | US | HO | HP | ■ | Barriers: Discomfort among clinicians and patients discussing end-of-life care; Lack of adequate ACP training for clinicians Facilitators: Improved messaging |
3.2.3. Innovation Category
| Study ID | Country | Setting | Population | No. of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| Finger 2022 [92] | US | NH | PT | 24 | ■ | Barriers: Social distancing measures and visitation restrictions; Strained healthcare system Facilitators: Care team collaboration; Guidance and protocols for ACP discussions |
| Hannon 2022 * [93] | CN | NH, HO | PT | 26 | ■ | Facilitators: Telehealth/virtual ACP platforms |
| Hui 2022 * [94] | US | HO | PT | 12,941 | ■ | Facilitators: Guidance and protocols for ACP discussions; Identification of those in need of ACP; Care team collaboration; Training for clinicians; Healthcare system improvements |
| Zhukovsky 2022 * [95] | US | HO | PT | 76 | ■ | Facilitators: Care team collaboration |
| Gessling 2022 * [96] | US | OT | PT | 294 | ■ | Facilitators: Telehealth/virtual ACP platforms; Care team collaboration |
| Vellani 2022 [97] | CN | HO | PT | 21 dyads | ■ | Barriers: Emotional barriers Facilitators: ACP/palliative care experts; Training for clinicians; Public awareness of ACP; Resources/education for patients/families |
| Yen 2022 [98] | TW | HO | PT | 897 | ■ | Barriers: Uncertainty surrounding the COVID-19 prognosis; Limited resources Facilitators: Identification of those in need of ACP |
| Liberman 2022 [99] | US | HO | PT | 64 | ■ | Facilitators: Telehealth/virtual ACP platforms; ACP/palliative care experts |
| Meyers 2022 * [100] | US | OT | VT | 106 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Identification of those in need of ACP; Telehealth/virtual ACP platforms |
| Yourman 2022 * [101] | US | HO | PT | 53 | ■ | Facilitators: Training for clinicians; Telehealth/virtual ACP platforms |
| MacInnes 2022 * [102] | UK | OT | HP | ■ | Facilitators: Telehealth/virtual ACP platforms | |
| Allen 2021 * [103] | UK | OT | PT, HP, PB | ■ | Facilitators: Resources for clinicians | |
| Acevedo Rodriguez 2021 * [104] | US | OT | VT | 500 | ■ | Facilitators: Telehealth/virtual ACP platforms |
| Singh 2021 [105] | US | HO | PT | ■ | Facilitators: Care team collaboration; Healthcare system improvements | |
| Nandhra 2021 * [106] | UK | NH | PT | 585 | ■ | Facilitators: Identification of those in need of ACP; ACP/palliative care experts |
| Paladino 2021 [107] | US | HO | HP | ■ | Facilitators: Guidance and protocols for ACP discussions | |
| Lin 2020 [108] | US | ED | HP | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms; Healthcare system improvements; Tablet computers; Language support services; Training for clinicians | |
| Handalage 2020 * [109] | UK | OT | PT | 160 | ■ | Facilitators: Resources for clinicians; ACP/palliative care experts |
| Schoenherr 2020 [110] | US | HO | PT | 29 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Identification of those in need of ACP |
| Langmaid 2020 [111] | US | OT | PT | ■ | Facilitators: Care team collaboration; Telehealth/virtual ACP platforms | |
| Gaur 2020 [112] | US | NH | HP | 10 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Guidance and protocols for ACP discussions |
| Bhatia 2021 [113] | US | HO | PT | 356 | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms; Proactive ACP conversations |
| Cavalier 2020 [114] | US | HO | PT | ■ | Facilitators: Innovation and flexibility and in ACP documentation processes | |
| Janssen 2020 [115] | NL | SV | HP | 68 | ■ | Facilitators: Proactive ACP conversations |
| Baharlou 2020 [116] | US | OT | PT | 183 | ■ | Facilitators: Innovation and flexibility in ACP documentation processes; Understanding/fear of COVID-19; Healthcare system improvements; Care team collaboration; Training for clinicians; ACP/palliative care experts; Telehealth/virtual ACP platforms |
| McFarlane 2022 * [117] | UK | ED | PB | 56,343 | ■ | Facilitators: Innovation and flexibility in ACP documentation processes |
| Mulyak 2021 * [118] | UK | ED | PT | 107,614 | ■ | Facilitators: Innovation and flexibility in ACP documentation processes |
| Hurlow 2021 [119] | UK | ED | PT | ■ | Facilitators: Innovation and flexibility in ACP documentation processes | |
| Funk 2020 [120] | US | ED | PB | ■ | Facilitators: Telehealth/virtual ACP platforms; Innovation and flexibility in ACP documentation processes | |
| Portz 2020 [121] | US | OT | PB | 3292 | ■ | Facilitators: Innovation and flexibility in ACP documentation processes; Resources/education for patients/families |
| Schifeling 2020 [122] | US | OT | PT | 190 | ■ | Facilitators: Telehealth/virtual ACP platforms |
| Auriemma 2020 [123] | US | OT | PT, FM | ■ | Facilitators: Resources/education for patients/families |
3.2.4. Recommendation Category
| Study ID | Country | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|
| Auriemma 2022 [124] | US | ■ | Barriers: Social distancing measures and visitation restrictions; Technological/telehealth barriers; Uncertainty surrounding the COVID-19 prognosis; Negative perceptions about advance care planning; Distrust in the healthcare system; Racial and ethnic barriers Facilitators: Identification of those in need of ACP; Guidance and protocols for ACP discussions; ACP/palliative care experts |
| Back 2021 [125] | US | ■ | Barriers: Lack of awareness/knowledge of ACP; Uncertainty surrounding the COVID-19 prognosis; Distrust in the healthcare system Facilitators: Improved messaging |
| Bender 2021 [126] | US | ■ | Barriers: Time constraints; Limited resources; Healthcare system barriers; Discomfort among clinicians and patients discussing end-of-life care; Strained healthcare system; Personal protective equipment requirements Facilitators: Telehealth/virtual ACP platforms; Care team collaboration; Innovation and flexibility in ACP documentation processes |
| Block 2020 [127] | US | ■ | Barriers: Legal concerns; Social distancing measures and visitation restrictions Facilitators: Care team collaboration; Innovation and flexibility in ACP documentation processes; Resources/education for patients/families; Telehealth/virtual ACP platforms |
| Chan 2020 [128] | UK | ■ | Barriers: Limited resources; Familial disagreement; Uncertainty surrounding the COVID-19 prognosis; Lack of awareness/knowledge of ACP; Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms; Innovation and flexibility in ACP documentation processes |
| Chase 2020 [129] | CN | ■ | Facilitators: Telehealth/virtual ACP platforms; Healthcare system improvements; Guidance and protocols for ACP discussions |
| Curtis 2020 [130] | US | ■ | Barriers: Strained healthcare system Facilitators: Telehealth/virtual ACP platforms; Care team collaboration |
| Dattolo 2021 [131] | IT | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms |
| Dewhurst 2021 [132] | UK | ■ | Facilitators: Proactive ACP Conversations |
| Farrell 2020 [133] | US | ■ | Facilitators: Healthcare system improvements; Care team collaboration: teamwork/multi-disciplinary involvement; Telehealth/virtual ACP platforms; Identification of those in need of ACP |
| Gordon 2020 [134] | UK | ■ | Barriers: Social distancing measures and visitation restrictions; Blanket approaches to ACP; Negative perceptions about advance care planning Facilitators: ACP/palliative care experts; Individualized ACP discussion |
| Hill 2021 [135] | UK | ■ | Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements Facilitators: Telehealth/virtual ACP platforms; Early ACP; Trusting clinical relationship; Innovation and flexibility in ACP documentation processes |
| Hopkins 2020 [136] | UK | ■ | Barriers: Social distancing measures and visitation restrictions; Technological/telehealth barriers Facilitators: Triggers to initiate conversations |
| Hughes 2021 [137] | US | ■ | Barriers: Distrust in the healthcare system; Lack of awareness/knowledge of ACP Facilitators: Resources for clinicians; Language support services; Improved messaging |
| Janwadkar 2020 [138] | US | ■ | Barriers: Limited resources; Time constraints; Rapid disease progression; Social distancing measures and visitation restrictions; Technological/telehealth barriers Facilitators: Telehealth/virtual ACP platforms; Innovation and flexibility in ACP documentation processes |
| Kuzuya 2020 [139] | JP | ■ | Barriers: Social distancing measures and visitation restrictions; Rapid disease progression; Communication difficulties Facilitators: Telehealth/virtual ACP platforms; Guidance and protocols for ACP discussions; Information sharing; Care team collaboration |
| Moorman 2021 [140] | US | ■ | Barriers: Emotional barriers; Social distancing measures and visitation restrictions; Familial disagreement; Rapid disease progression; Financial concerns; Low education level; Racial and ethnic barriers; Strained healthcare system Facilitators: Trusting clinical relationship |
| Palipane 2021 [141] | UK | ■ | Barriers: Rapid disease progression Facilitators: Public awareness of ACP; Guidance and protocols for ACP discussions |
| Parekh de Campos 2021 [142] | US | ■ | Barriers: Limited resources; Time constraints; Lack of adequate ACP training for clinicians; Cultural and religious beliefs |
| Parks 2021 [143] | US | ■ | Barriers: Social distancing measures and visitation restrictions; Communication difficulties |
| Powell 2021 [144] | US | ■ | Barriers: Social distancing measures and visitation restrictions Facilitators: Guidance and protocols for ACP discussions; ACP/palliative care experts |
| Sinclair 2020 [145] | AU | ■ | Barriers: Personal protective equipment requirements Facilitators: Resources/education for patients/families; Telehealth/virtual ACP platforms; Resources for clinicians; Innovation and flexibility in ACP documentation processes |
| Swinford 2020 [146] | US | ■ | Facilitators: Telehealth/virtual ACP platforms; Care team collaboration; Guidance and protocols for ACP discussions |
| Van Buren 2021 [147] | US | ■ | Barriers: Family clustering of COVID-19; Social distancing measures and visitation restrictions Facilitators: Telehealth/virtual ACP platforms; Innovation and flexibility in ACP documentation processes; Care team collaboration; ACP/palliative care experts; Healthcare system improvements; Guidance and protocols for ACP discussions |
| Wallace 2020 [148] | US | ■ | Barriers: Rapid disease progression Facilitators: Guidance and protocols for ACP discussions; Resources for clinicians; Innovation and flexibility in ACP documentation processes; ACP/palliative care experts; Telehealth/virtual ACP platforms |
| Zaurova 2020 [149] | US | ■ | Barriers: Strained healthcare system; Rapid disease progression; Uncertainty surrounding the COVID-19 prognosis Facilitators: Early ACP; Guidance and protocols for ACP discussions; Triggers to initiate conversations |
3.3. ACP Barriers and Facilitators Coding
3.4. Sub-Analysis of ACP Documentation/Engagement Increase and Decrease
4. Discussion
4.1. Barriers to ACP during the COVID-19 Pandemic
4.2. Facilitators of ACP during the COVID-19 Pandemic
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.; Lapierre, N.; Faieta, J.; Vincent, C.; Duchesne, L.; Ouellet, M.; et al. Impact of the COVID-19 Pandemic on Older Adults: Rapid Review. JMIR Aging 2021, 4, e26474. [Google Scholar] [CrossRef] [PubMed]
- Nanda, A.; Vura, N.V.R.K.; Gravenstein, S. COVID-19 in older adults. Aging Clin. Exp. Res. 2020, 32, 1199–1202. [Google Scholar] [CrossRef] [PubMed]
- Kasar, K.S.; Karaman, E. Life in lockdown: Social isolation, loneliness and quality of life in the elderly during the COVID-19 pandemic: A scoping review. Geriatr. Nurs. 2021, 42, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. COVID-19 and the consequences of isolating the elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, B.R.; Torossian, E. Older Adults’ Experience of the COVID-19 Pandemic: A Mixed-Methods Analysis of Stresses and Joys. Gerontologist 2021, 61, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Vahia, I.V.; Jeste, D.V.; Reynolds, C.F. Older Adults and the Mental Health Effects of COVID-19. JAMA 2020, 324, 2253–2254. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K. Older adults and COVID-19 pandemic: Resilience matters. Arch. Gerontol. Geriatr. 2020, 89, 104124. [Google Scholar] [CrossRef] [PubMed]
- Brinkman-Stoppelenburg, A.; Rietjens, J.A.; van der Heide, A. The effects of advance care planning on end-of-life care: A systematic review. Palliat. Med. 2014, 28, 1000–1025. [Google Scholar] [CrossRef]
- Houben, C.H.; Spruit, M.A.; Groenen, M.T.; Wouters, E.F.; Janssen, D.J. Efficacy of advance care planning: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2014, 15, 477–489. [Google Scholar] [CrossRef]
- Detering, K.M.; Hancock, A.D.; Reade, M.C.; Silvester, W. The impact of advance care planning on end of life care in elderly patients: Randomised controlled trial. BMJ 2010, 340, c1345. [Google Scholar] [CrossRef]
- Weathers, E.; O’Caoimh, R.; Cornally, N.; Fitzgerald, C.; Kearns, T.; Coffey, A.; Daly, E.; O’sullivan, R.; McGlade, C.; Molloy, D. Advance care planning: A systematic review of randomised controlled trials conducted with older adults. Maturitas 2016, 91, 101–109. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.J.; Choong, M.C.; Cheong, E.H.; Kalimuddin, S.; Wen, S.D.; Phua, G.C.; Chan, K.S.; Mohideen, S.H. Rapid progression to acute respiratory distress syndrome: Review of current understanding of critical illness from coronavirus disease 2019 (COVID-19) infection. Ann. Acad. Med. Singap. 2020, 49, 108–118. [Google Scholar] [CrossRef]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. Covid-19—Implications for the health care system. N. Engl. J. Med. 2020, 383, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.K.; Merriam, L.T.; Pearson, J.C.; Lipnick, M.S.; McKleroy, W.; Kim, E.Y. Treating COVID-19: Evolving approaches to evidence in a pandemic. Cell Rep. Med. 2022, 3, 3. [Google Scholar] [CrossRef] [PubMed]
- Panesar, K.; Dodson, T.; Lynch, J.; Bryson-Cahn, C.; Chew, L.; Dillon, J. Evolution of COVID-19 guidelines for University of Washington oral and maxillofacial surgery patient care. J. Oral Maxillofac. Surg. 2020, 78, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, W.B.; Bennett, D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: A national survey. Am. J. Prev. Med. 2020, 59, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Lanciano, T.; Graziano, G.; Curci, A.; Costadura, S.; Monaco, A. Risk perceptions and psychological effects during the Italian COVID-19 emergency. Front. Psychol. 2020, 11, 580053. [Google Scholar] [CrossRef]
- Motta Zanin, G.; Gentile, E.; Parisi, A.; Spasiano, D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3024. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.Y.; Lin, C.P.; Chan, H.Y.L.; Martina, D.; Mori, M.; Kim, S.H.; Ng, R. Advance care planning in Asian culture. Jpn. J. Clin. Oncol. 2020, 50, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.; Luth, E.A. Advance Care Planning: Contemporary Issues and Future Directions. Innov. Aging 2017, 1, igx012. [Google Scholar] [CrossRef] [PubMed]
- Dall, T.M.; Gallo, P.D.; Chakrabarti, R.; West, T.; Semilla, A.P.; Storm, M.V. An aging population and growing disease burden will require alarge and specialized health care workforce by 2025. Health Aff. 2013, 32, 2013–2020. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Klingler, C.; in der Schmitten, J.; Marckmann, G. Does facilitated Advance Care Planning reduce the costs of care near the end of life? Systematic review and ethical considerations. Palliat. Med. 2016, 30, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Pfaff, K.; Markaki, A. Compassionate collaborative care: An integrative review of quality indicators in end-of-life care. BMC Palliat. Care 2017, 16, 65. [Google Scholar] [CrossRef]
- Bomba, P.A.; Orem, K. Lessons learned from New York’s community approach to advance care planning and MOLST. Ann. Palliat. Med. 2015, 4, 10–21. [Google Scholar] [CrossRef]
- Martina, D.; Geerse, O.P.; Lin, C.P.; Kristanti, M.S.; Bramer, W.M.; Mori, M.; Korfage, I.J.; van der Heide, A.; Rietjens, J.A.; van der Rijt, C.C. Asian patients’ perspectives on advance care planning: A mixed-method systematic review and conceptual framework. Palliat. Med. 2021, 35, 1776–1792. [Google Scholar] [CrossRef]
- Inokuchi, R.; Hanari, K.; Shimada, K.; Iwagami, M.; Sakamoto, A.; Sun, Y.; Mayers, T.; Sugiyama, T.; Tamiya, N. Barriers to and facilitators of advance care planning implementation for medical staff after the COVID-19 pandemic: An overview of reviews. BMJ Open 2023, 13, e075969. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org; https://support.covidence.org/help/general-information-for-cochrane-authors (accessed on 7 March 2024).
- Pluye, P.; Hong, Q.N. Combining the power of stories and the power of numbers: Mixed Methods Research and Mixed Studies Reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef]
- Tyndall, J.; AACODS Checklist. Flinders University. 2010. Available online: http://dspace.flinders.edu.au/dspace/ (accessed on 27 June 2022).
- Mota Romero, E.; Puente Fernández, D.; Rodríguez Pertíñez, C.; Árbol Fernández, G.; Moreno Guerrero, S.; Montoya Juárez, R. Inadequate Human Resources, Equipment and Training: A Qualitative Assessment of the Objectives of the NUHELP End-of-Life Care Programme in the Context of the COVID-19 Pandemic. Palliat. Med. 2022, 36, 1252–1262. [Google Scholar] [CrossRef] [PubMed]
- Statler, T.M.; Hsu, F.-C.; Silla, L.; Sheehan, K.N.; Cowles, A.; Brooten, J.K.; Omlor, R.L.; Gabbard, J. Occurrence of Advance Care Planning and Hospital Course in Patients Admitted for Coronavirus Disease 2019 (COVID-19) During the Pandemic. Am. J. Hosp. Palliat. Care 2022, 40, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Porteny, T.; Gonzales, K.M.; Aufort, K.E.; Levine, S.; Wong, J.B.; Isakova, T.; Rifkin, D.E.; Gordon, E.J.; Rossi, A.; Di Perna, G.; et al. Treatment Decision Making for Older Kidney Patients during COVID-19. Clin. J. Am. Soc. Nephrol. 2022, 17, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Epler, K.; Lenhan, B.; O’Callaghan, T.; Painter, N.; Troost, J.; Barrett, J.; Jacobson, E. If Your Heart Were to Stop: Characterization and Comparison of Code Status Orders in Adult Patients Admitted with COVID-19. J. Palliat. Med. 2022, 25, 888–896. [Google Scholar] [CrossRef]
- Kaehr, E.; Gowan, T.; Unroe, K.; Rattray, N.; Hathaway, E. Front-Line Nursing Home Staff Provide Insight on Advance Care Planning in a Crisis. J. Am. Med. Dir. Assoc. 2022, 23, B17–B18. [Google Scholar] [CrossRef]
- Sun, F.; Lipinsky DeGette, R.; Cummings, E.C.; Deng, L.X.; Hauser, K.A.; Kopp, Z.; Penner, J.C.; Scott, B.S.; Raffel, K.E.; Kantor, M.A. Capturing What Matters: A Retrospective Observational Study of Advance Care Planning Documentation at an Academic Medical Center during the COVID-19 Pandemic. Palliat. Med. 2022, 36, 342–347. [Google Scholar] [CrossRef]
- Barnato, A.E.; Birkmeyer, J.D.; Skinner, J.S.; O’Malley, A.J.; Birkmeyer, N.J.O. Treatment Intensity and Mortality among COVID-19 Patients with Dementia: A Retrospective Observational Study. J. Am. Geriatr. Soc. 2022, 70, 40–48. [Google Scholar] [CrossRef]
- Ter Brugge, B.P.H.; van Atteveld, V.A.; Fleuren, N.; Douma, M.H.; van der Ploeg, M.B.; Hoeksma, J.E.; Smalbrugge, M.; Sizoo, E.M. Advance Care Planning in Dutch Nursing Homes During the First Wave of the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2022, 23, 1–6.e1. [Google Scholar] [CrossRef]
- Perumalswami, C.R.; Chen, E.; Martin, C.; Goold, S.D.; De Vries, R.; Griggs, J.J.; Jagsi, R. “I’m Being Forced to Make Decisions I Have Never Had to Make Before”: Oncologists’ Experiences of Caring for Seriously Ill Persons With Poor Prognoses and the Dilemmas Created by COVID-19. JCO Oncol. Pract. 2022, 18, e89–e97. [Google Scholar] [CrossRef]
- Jayes, M.; Borrett, S.; Bose, A. Mental Capacity Legislation and Communication Disability: A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Provision of Specialist Decision-Making Support by UK SLTs. Int. J. Lang. Commun. Disord. 2022, 57, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Janssen, D.J.A. Palliative Care in COVID-19. Curr. Opin. Support. Palliat. Care 2021, 15, 199–204. [Google Scholar] [CrossRef]
- Brophy, N.S.; Seiter, C.R.; Zhao, X. COVID-19 Risk Perceptions and Intentions to Engage in Familial Advance Care Planning: The Mediating Role of Death Anxiety. J. Health Commun. 2021, 26, 684–695. [Google Scholar] [CrossRef]
- Piers, R.; Van Braeckel, E.; Benoit, D.; Van Den Noortgate, N. Early Resuscitation Orders in Hospitalized Oldest-Old with COVID-19: A Multicenter Cohort Study. Palliat. Med. 2021, 35, 1288–1294. [Google Scholar] [CrossRef]
- Bradshaw, A.; Dunleavy, L.; Walshe, C.; Preston, N.; Cripps, R.L.; Hocaoglu, M.; Bajwah, S.; Maddocks, M.; Oluyase, A.O.; Sleeman, K.; et al. Understanding and Addressing Challenges for Advance Care Planning in the COVID-19 Pandemic: An Analysis of the UK CovPall Survey Data from Specialist Palliative Care Services. Palliat. Med. 2021, 35, 1225–1237. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, J.; Schuurmans, J.; Westerduin, D.; Wichmann, A.B.; Engels, Y. The COVID-19 Pandemic: A Tipping Point for Advance Care Planning? Experiences of General Practitioners. Palliat. Med. 2021, 35, 1238–1248. [Google Scholar] [CrossRef]
- Connellan, D.; Diffley, K.; McCabe, J.; Cotter, A.; McGinty, T.; Sheehan, G.; Ryan, K.; Cullen, W.; Lambert, J.S.; Callaly, E.L.; et al. Documentation of Do-Not-Attempt-Cardiopulmonary-Resuscitation Orders amid the COVID-19 Pandemic. Age Aging 2021, 50, 1048–1051. [Google Scholar] [CrossRef] [PubMed]
- Vellani, S.; Boscart, V.; Escrig-Pinol, A.; Cumal, A.; Krassikova, A.; Sidani, S.; Zheng, N.; Yeung, L.; McGilton, K.S. Complexity of Nurse Practitioners’ Role in Facilitating a Dignified Death for Long-Term Care Home Residents during the COVID-19 Pandemic. J. Pers. Med. 2021, 11, 433. [Google Scholar] [CrossRef]
- Toccafondi, A.; Simone, G.; Lombardi, M.; Dattolo, P.C. Covid-19 Pandemic Increased Advance Care Planning Demand. Nephrol. Dial. Transpl. 2021, 36, 182. [Google Scholar] [CrossRef]
- DeGette, R.L.; Sun, F.D.; Cummings, E.; Deng, L.X.; Hauser, K.; Kopp, Z.; Penner, J.; Scott, B.; Raffel, K.; Kantor, M.A. A Missed Opportunity: Advance Care Planning Documentation in Patients with COVID-19. J. Pain Symptom Manag. 2021, 61, 640. [Google Scholar] [CrossRef]
- Copley, A.; West, M.; Morris, J.; Hargreaves, F.; Tayebjee, M.H. ReSPECT (Recommended Summary Plan for Emergency Care and Treatment) in a Pandemic: The Impact of COVID-19 on Advance Care Planning in a UK University Hospital Cardiology Department. BMJ Support Palliat. Care 2021, 11, A17. [Google Scholar] [CrossRef]
- Lin, C.T.; Bookman, K.; Sieja, A.; Markley, K.; Altman, R.L.; Sippel, J.; Perica, K.; Reece, L.; Davis, C.; Horowitz, E.; et al. Clinical Informatics Accelerates Health System Adaptation to the COVID-19 Pandemic: Examples from Colorado. J. Am. Med. Inform. Assoc. 2020, 27, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- Ye, P.; Fry, L.; Champion, J.D. Changes in Advance Care Planning for Nursing Home Residents During the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2021, 22, 209–214. [Google Scholar] [CrossRef]
- Huayanay, I.; Pantoja, C.; Chang, C. End of Life Decision-Making Challenges in a Latino Patient with COVID-19: Facing Barriers. Gerontol. Geriatr. Med. 2021, 7, 23337214211021730. [Google Scholar] [CrossRef]
- Nguyen, A.L.; Davtyan, M.; Taylor, J.; Christensen, C.; Brown, B. Perceptions of the Importance of Advance Care Planning During the COVID-19 Pandemic Among Older Adults Living With HIV. Front. Public Health 2021, 9, 636786. [Google Scholar] [CrossRef]
- Coles, T.; Crawley, S.; Martin, F.; Diem, P.; Patel, J.; Masterton, J.; Noble, J.; Wilson, D.; Perks, C.; Kalsi, T. Reflections of a Care Home Provider on the COVID-19 Pandemic: A Catalyst for Integrated Care. Eur. Geriatr. Med. 2020, 11, S63–S64. [Google Scholar]
- Wei, E.; Segall, J.; Villanueva, Y.; Dang, L.B.; Gasca, V.I.; Gonzalez, M.P.; Roman, M.; Mendez-Justiniano, I.; Cohen, A.G.; Cho, H.J. Coping with Trauma, Celebrating Life: Reinventing Patient and Staff Support During The COVID-19 Pandemic. Health Aff. 2020, 39, 1597–1600. [Google Scholar] [CrossRef]
- Maia, P.; Mano, D.; Campos, P.; Vidal, C.; Madeira, I.; Freire, E.; Ramalho, J. Communication and Humanization in End-of-Life COVID-19 ICU Patients. Intensive Care Med. Exp. 2020, 8, 73. [Google Scholar] [CrossRef]
- Hendriks, V.J.J.; Faes, M.C.; van der Meer, J.B.L.; Janse, E.S.; van der Meer, N.J.M.; van der Linden, C.M.J. Shared Decision-Making in Advance Care Planning among Hospitalized Older COVID-19 Patients: A Multicenter, Retrospective Cohort Study. Aging Clin. Exp. Res. 2022, 34, 3165–3169. [Google Scholar] [CrossRef]
- Holdsworth, L.M.; Mui, H.Z.; Winget, M.; Lorenz, K.A. “Never Waste a Good Crisis”: A Qualitative Study of the Impact of COVID-19 on Palliative Care in Seven Hospitals Using the Dynamic Sustainability Framework. Palliat. Med. 2022, 36, 1544–1551. [Google Scholar] [CrossRef]
- Dassel, K.B.; Towsley, G.L.; Utz, R.L.; Ellington, L.; Terrill, A.; Scammon, D.; Bristol, A.A.; Thompson, A.; Mickens, M. A Limited Opportunity: COVID-19 and Promotion of Advance Care Planning. Palliat. Med. Rep. 2021, 2, 194–198. [Google Scholar] [CrossRef]
- de Vries, B.; Gutman, G.; Beringer, R.; Gill, P.; Daudt, H. Advance Care Planning among Older Canadians amid the COVID-19 Pandemic: A Focus on Sexual Orientation. Palliat. Care Soc. Pract. 2021, 15, 26323524211019056. [Google Scholar] [CrossRef]
- Payne, J.; Sadeghi, M.A.; Liu, J.; Siess, S.; Moyer, A. The Comprehensiveness and Comprehensibility of Publicly-Available, State-Approved Advance Directive Documents. Psychol. Health Med. 2022, 28, 3131–3148. [Google Scholar] [CrossRef]
- Ninteau, K.; Bishop, C.E. Nursing Home Palliative Care During the Pandemic: Directions for the Future. Innov. Aging 2022, 6, igac030. [Google Scholar] [CrossRef]
- Elizondo, C.; Ferre, M.F.; Gallo, C.M.; Marco, A.; Bendelman, G.; Bonella, B.; Perman, G.; Schapira, M.; Giber, F.; Gilszlak, E.; et al. Advance Care Planning and Use of Hospital Resources among COVID-19 Nursing Home Patients in an Integrated Care Programme for the Elderly. Int. J. Integr. Care 2022, 22, 183. [Google Scholar] [CrossRef]
- Hafid, A.; Arora, N.; Elston, D.; Carverhill, J.; Guenter, D.; Gallagher, E.; Howard, M.; Dong, J. Primary Care Physicians’ Perceptions on Advance Care Planning before and during the COVID-19 Pandemic 2022. Ann. Fam. Med. 2022, 20, 2750. [Google Scholar] [CrossRef]
- van de Wiel, M.; Bombeke, K.; Janssens, A. Communication Skills Training in Advance Care Planning: A Survey among Medical Students at the University of Antwerp. BMC Palliat. Care 2022, 21, 154. [Google Scholar] [CrossRef]
- Casey, M.F.; Price, L.; Markwalter, D.; Bohrmann, T.; Tsujimoto, T.M.; Lavin, K.; Hanson, L.C.; Lin, F.-C.; Platts-Mills, T.F. Advance Care Planning for Emergency Department Patients with COVID-19 Infection: An Assessment of a Physician Training Program. Am. J. Hosp. Palliat. Care 2022, 39, 1358–1363. [Google Scholar] [CrossRef]
- Cousins, E.; Preston, N.; Doherty, J.; Varey, S.; Harding, A.; McCann, A.; Harrison Dening, K.; Finucane, A.; Carter, G.; Mitchell, G.; et al. Implementing and Evaluating Online Advance Care Planning Training in UK Nursing Homes during COVID-19: Findings from the Necessary Discussions Multi-Site Case Study Project. BMC Geriatr. 2022, 22, 419. [Google Scholar] [CrossRef]
- Rosedale, R.L.; Parsley, H.; Rubenstein, C.B. Advance Care Planning and Health Equity: Pursuing Quality Improvement in a Family Medicine Residency Clinic. Epidemiology 2022, 70, S184. [Google Scholar]
- Rabow, M.W.; Keyssar, J.R.; Long, J.; Aoki, M.; Kojimoto, G. Palliative Care Education During COVID-19: The MERI Center for Education in Palliative Care at UCSF/Mt. Zion. Am. J. Hosp. Palliat. Care 2021, 38, 845–849. [Google Scholar] [CrossRef]
- Oulton, J.R.; Fu, E.; Babineau, S.; Rubenstein, C. Improving Advance Care Planning and Completion of Advance Directives: A Role for Virtual Peer Training. J. Am. Geriatr. Soc. 2021, 69, S65. [Google Scholar]
- Budidi, S.; Chippendale, R.; Soliz, M. Advanced Care Planning in the COVID-19 Era. J. Am. Geriatr. Soc. 2021, 69, S119. [Google Scholar]
- Price, L.E.; Casey, M.F.; Markwalter, D.; Bohrmann, T.; Tsujimoto, T.M.; Lavin, K.; Hanson, L.; Lin, F.; Platts-Mills, T.F. An Educational Intervention to Increase Advance Care Planning Activities among Emergency Medicine Providers during the COVID-19 Pandemic. J. Am. Geriatr. Soc. 2021, 69, S208. [Google Scholar]
- Roberts, B.; Wright, S.M.; Christmas, C.; Robertson, M.; Wu, D.S. COVID-19 Pandemic Response: Development of Outpatient Palliative Care Toolkit Based on Narrative Communication. Am. J. Hosp. Palliat. Care 2020, 37, 985–987. [Google Scholar] [CrossRef]
- Markwalter, D.; Casey, M.; Price, L.; Bohrmann, T.; Tsujimoto, T.; Lavin, K.; Hanson, L.; Lin, F.-C.; Platts-Mills, T. Advance Care Planning for Emergency Department Patients with COVID-19 Infection: An Assessment of a Physician Training Program (QI411). J. Pain Symptom Manag. 2022, 63, 891. [Google Scholar] [CrossRef]
- Preston, N. Research on Advance Care Planning in Nursing Homes During the COVID-19 Pandemic. Palliat. Med. 2022, 36, 12. [Google Scholar]
- Cooney, A.; Walker, M.; Sanchez-Reilly, S.; Ross, J. Enhancing Virtual Communication Skills Among Medical Learners: A COVID-19 Telemedicine Goals of Care Standardized Encounter (QI430). J. Pain Symptom Manag. 2022, 63, 901–902. [Google Scholar] [CrossRef]
- Holdsworth, E.; Ryall, R.; Greenwood, E. 783 Advance Care Planning in a Large Teaching Hospital Emerging From the COVID-19 Pandemic: A Quality Improvement Project. Age Aging 2022, 51, afac034-783. [Google Scholar] [CrossRef]
- Volandes, A.E.; Zupanc, S.N.; Paasche-Orlow, M.K.; Lakin, J.R.; Chang, Y.; Burns, E.A.; LaVine, N.A.; Carney, M.T.; Martins-Welch, D.; Emmert, K.; et al. Association of an Advance Care Planning Video and Communication Intervention With Documentation of Advance Care Planning Among Older Adults: A Nonrandomized Controlled Trial. JAMA Netw. Open 2022, 5, e220354. [Google Scholar] [CrossRef]
- Mills, S.; Cioletti, A.; Gingell, G.; Ramani, S. Training Residents in Virtual Advance Care Planning: A New Twist in Telehealth. J. Pain Symptom Manag. 2021, 62, 691–698. [Google Scholar] [CrossRef]
- Varey, S.; Doherty, J.; Cousins, E.; Carter, G.; Finucane, A.; Harding, A.; Harrison-Dening, K.; McCann, A.; Mitchell, G.; Preston, N.; et al. Necessary Discussions: The Development of Online Resources to Support Advance Care Planning in Nursing Homes in a COVID-19 Context. Palliat. Med. 2021, 35, 225. [Google Scholar]
- Phenwan, T.; Peerawong, T.; Jarusomboon, W.; Sittiwantana, E.; Satian, C.; Supanichwatana, S. Using Zoom and Card Game to Conduct Advance Care Planning Classes: An Innovative Practice. Omega 2021, 87, 1028–1047. [Google Scholar] [CrossRef]
- Berning, M.J.; Palmer, E.; Tsai, T.; Mitchell, S.L.; Berry, S.D. An Advance Care Planning Long-Term Care Initiative in Response to COVID-19. J. Am. Geriatr. Soc. 2021, 69, 861–867. [Google Scholar] [CrossRef]
- Dobert, R.; Sibley, A.; Mustain, C.; Peretti, J.; Speight, I. What Matters for Frail Older Adults during a Global Pandemic. J. Am. Geriatr. Soc. 2021, 69, S127. [Google Scholar]
- Smith, G.M.; Hui, F.A.; Bleymaier, C.R.; Bragg, A.R.; Harman, S.M. What If I Get Seriously Ill? A Virtual Workshop for Advance Care Planning During COVID-19. J. Pain Symptom Manag. 2020, 60, e21–e24. [Google Scholar] [CrossRef]
- McAfee, C.A.; Jordan, T.R.; Cegelka, D.; Polavarapu, M.; Wotring, A.; Wagner-Greene, V.R.; Hamdan, Z. COVID-19 Brings a New Urgency for Advance Care Planning: Implications of Death Education. Death Stud. 2022, 46, 91–96. [Google Scholar] [CrossRef]
- Huang, D.C.; Buss, M.K.; Hayes, M.M. COVID-19 as a Catalyst for Teaching Advance Care Planning. ATS Sch. 2021, 2, 503–507. [Google Scholar] [CrossRef]
- Finger, H.J.; Dury, C.A.; Sansone, G.R.; Rao, R.N.; Dubler, N.N. An Interdisciplinary Ethics Panel Approach to End-of-Life Decision Making for Unbefriended Nursing Home Residents. J. Clin. Ethics 2022, 33, 101–111. [Google Scholar] [CrossRef]
- Hannon, B.; Castro, M.J.A.; Nissim, R.; Mak, E.; Lau, J.; O’Connor, B.; Zimmermann, C. Patients’ Experiences With Virtual Outpatient Palliative Care Visits During The COVID-19 Pandemic: A Qualitative Study. Support Care Cancer 2022, 30, S120. [Google Scholar] [CrossRef]
- Hui, D.; Nortje, N.; George, M.C.; Wilson, K.; Urbauer, D.L.; Lenz, C.; Wallace, S.K.; Andersen, C.; Mendoza, T.R.; Haque, S.; et al. Impact of an Interdisciplinary Goals of Care Program on Hospital Outcomes at a Comprehensive Cancer Center during the COVID-19 Pandemic: A Propensity Score Analysis. J. Clin. Oncol. 2022, 40, 6502. [Google Scholar] [CrossRef]
- Zhukovsky, D.; Enriquez, P.; Nortje, N.; Heung, Y.; Itzep, N.; Wong, A.; Lu, Z.; Stanton, P.; Bruera, E. Goals of Care Rapid Response Team at a Comprehensive Cancer Center: Feasibility and Preliminary Outcomes (S537). J. Pain Symptom Manag. 2022, 63, 926. [Google Scholar] [CrossRef]
- Gessling, A.; Tran, Q.; Langston, J.; Soloway, A.; Larson, D. COVID-19 and Advance Care Planning: A Unique Opportunity. J. Pain Symptom Manag. 2022, 63, 901. [Google Scholar] [CrossRef]
- Vellani, S.; Puts, M.; Iaboni, A.; McGilton, K.S. Acceptability of the Voice Your Values, an Advance Care Planning Intervention in Persons Living with Mild Dementia Using Videoconferencing Technology. PLoS ONE 2022, 17, e0266826. [Google Scholar] [CrossRef]
- Yen, Y.-F.; Hu, H.-Y.; Chou, Y.-C.; Chen, C.-C.; Ho, C.-Y. Utilization of Palliative Care Screening Tool to Early Identify Patients with COVID-19 Needing Palliative Care: A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 1054. [Google Scholar] [CrossRef]
- Liberman, T.; Roofeh, R.; Chin, J.; Chin, K.; Razack, B.; Aquilino, J.; Herod, S.H.; Amato, T. Remote Advance Care Planning in the Emergency Department During COVID-19 Disaster: Program Development and Initial Evaluation. J. Emerg. Nurs. 2022, 48, 22–31. [Google Scholar] [CrossRef]
- Meyers, G.; Mandujano, C.; Sholtis, L.; Tauber, L.; Jallad, R.; Goodlin, S. Advance Care Planning in a Geriatric Veterans Primary Care Clinic During COVID-19. Epidemiology 2022, 70, S176. [Google Scholar]
- Yourman, L.; Malhotra, R.; Civello, B.; Ramirez, Y.; Bompat, M.; Nguyen, K.; Bauer, S.; Lum, H. Acceptability and Effectiveness of Virtual Group Visits for Advance Care Planning. Epidemiology 2022, 70, S120. [Google Scholar]
- MacInnes, L.; Canning, D.; Hutchinson, W.; Akinbami, A.; Ashaye, E.; Ratcliffe, C.; Smith, B.; Bonnar, K.; Ripley, D. Advance Care Planning Virtually During a Pandemic. BMJ Support Palliat. Care 2022, 12, A12. [Google Scholar] [CrossRef]
- Allen, G.; Towns, C. Community Response During the COVID-19 Pandemic. BMJ Support Palliat. Care 2021, 11, A29. [Google Scholar] [CrossRef]
- Acevedo Rodriguez, M.; Harris, B. Improving the Quality of Care in Patients with COVID-19. J. Am. Geriatr. Soc. 2021, 69, S82. [Google Scholar]
- Singh, S.; Herrmann, K.; Cyriacks, W.; Youngwerth, J.; Bickel, K.E.; Lum, H.D. Increasing Medical Power of Attorney Completion for Hospitalized Patients During the COVID Pandemic: A Social Work Led Quality Improvement Intervention. J. Pain Symptom Manag. 2021, 61, 579–584.e1. [Google Scholar] [CrossRef]
- Nandhra, G.; Head, J.; Massey, A.; Hassell, J.; Lynch, F.; Stringer, K.; Lacy-Colson, A. The Promotion of Successful Advance Care Planning (ACP) for Care Home Residents During the COVID-19 Pandemic. BMJ Support Palliat. Care 2021, 11, A2. [Google Scholar] [CrossRef]
- Paladino, J.; Mitchell, S.; Mohta, N.; Lakin, J.R.; Downey, N.; Fromme, E.K.; Gullo, S.; Benjamin, E.; Sanders, J.J. Communication Tools to Support Advance Care Planning and Hospital Care During the COVID-19 Pandemic: A Design Process. Jt. Comm. J. Qual. Patient Saf. 2021, 47, 127–136. [Google Scholar] [CrossRef]
- Lin, M.-H.; Hsu, J.-L.; Chen, T.-J.; Hwang, S.-J. Impact of the COVID-19 Pandemic on the Use of Advance Care Planning Services within the Veterans Administration System in Taiwan. J. Chin. Med. Assoc. 2021, 84, 197–202. [Google Scholar] [CrossRef]
- Handalage, C.; Jundi, A.; Anthony, R.; Chhokar, G.; Burns, E. Does a Geriatrician-Led Telephone Advice Line Optimise Care for Frail Older People during the COVID-19 Pandemic? Eur. Geriatr. Med. 2020, 11, S49–S50. [Google Scholar]
- Schoenherr, L.A.; Cook, A.; Peck, S.; Humphreys, J.; Goto, Y.; Saks, N.T.; Huddleston, L.; Elia, G.; Pantilat, S.Z. Proactive Identification of Palliative Care Needs Among Patients With COVID-19 in the ICU. J. Pain Symptom Manag. 2020, 60, e17–e21. [Google Scholar] [CrossRef]
- Langmaid, L.; Ratner, L.; Huysman, C.; Curran, S.; Uluer, A. Supporting the Medically Fragile: Individualized Approach to Empowering Young Adults With Chronic Disease During the COVID-19 Pandemic. J. Adolesc. Health 2020, 67, 453–455. [Google Scholar] [CrossRef]
- Gaur, S.; Pandya, N.; Dumyati, G.; Nace, D.A.; Pandya, K.; Jump, R.L.P. A Structured Tool for Communication and Care Planning in the Era of the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 943–947. [Google Scholar] [CrossRef]
- Bhatia, V.; Geidner, R.; Mirchandani, K.; Huang, Y.; Warraich, H.J. Systemwide Advance Care Planning during the Covid-19 Pandemic: The Impact on Patient Outcomes and Cost. NEJM Catal. Innov. Care Deliv. 2021, 2. [Google Scholar] [CrossRef]
- Cavalier, J.S.; Maguire, J.M.; Kamal, A.H. Beyond Traditional Advance Care Planning: Tailored Preparedness for COVID-19. J. Pain Symptom Manag. 2020, 60, E4–E6. [Google Scholar] [CrossRef]
- Janssen, D.J.A.; Ekström, M.; Currow, D.C.; Johnson, M.J.; Maddocks, M.; Simonds, A.K.; Tonia, T.; Marsaa, K. COVID-19: Guidance on Palliative Care from a European Respiratory Society International Task Force. Eur. Respir. J. 2020, 56, 2002583. [Google Scholar] [CrossRef]
- Baharlou, S.; Orem, K.; Kelley, A.S.; Aldridge, M.D.; Popp, B. Rapid Implementation of EMOLST Order Completion and Electronic Registry to Facilitate Advance Care Planning: MOLST Documentation Using Telehealth in the Covid-19 Pandemic. NEJM Catal. Innov. Care Deliv. 2020, 1. [Google Scholar] [CrossRef]
- McFarlane, P.; Bunce, C.; Sleeman, K.E.; Orlovic, M.; Rosling, J.; Bearne, A.; Powell, M.; Riley, J.; Koffman, J.; Droney, J. Advance Care Plans: Creation, Content and Use During Wave 1 of the COVID-19 Pandemic. A Retrospective Cohort Study of Coordinate My Care, a Large Electronic Palliative Care Coordination System. Palliat. Med. 2022, 36, 33–34. [Google Scholar]
- Mulyak, M.; Riley, J.; Fischer, S. Review of DNACPR Orders within the Coordinate My Care (CMC) System during the First Wave of the COVID-19 Pandemic. Palliat. Med. 2021, 35, 222–223. [Google Scholar]
- Hurlow, A.; Wyld, L.; Breen, A. An Evaluation of Advance Care Planning during the COVID-19 Pandemic: A Retrospective Review of Patient Involvement in Decision Making Using Routinely Collected Data from Digital ReSPECT Records. Clin. Med. 2021, 21, e395–e398. [Google Scholar] [CrossRef]
- Funk, D.C.; Moss, A.H.; Speis, A. How COVID-19 Changed Advance Care Planning: Insights From the West Virginia Center for End-of-Life Care. J. Pain Symptom Manag. 2020, 60, e5–e9. [Google Scholar] [CrossRef]
- Portz, J.D.; Brungardt, A.; Shanbhag, P.; Staton, E.W.; Bose-Brill, S.; Lin, C.-T.; Kutner, J.S.; Lum, H.D. Advance Care Planning among Users of a Patient Portal during the COVID-19 Pandemic: Retrospective Observational Study. J. Med. Internet Res. 2020, 22, e21385. [Google Scholar] [CrossRef]
- Schifeling, C.H.; Shanbhag, P.; Johnson, A.; Atwater, R.C.; Koljack, C.; Parnes, B.L.; Vejar, M.M.; Farro, S.A.; Phimphasone-Brady, P.; Lum, H.D. Disparities in Video and Telephone Visits Among Older Adults During the COVID-19 Pandemic: Cross-Sectional Analysis. JMIR Aging 2020, 3, e23176. [Google Scholar] [CrossRef]
- Auriemma, C.L.; Halpern, S.D.; Asch, J.M.; Van Der Tuyn, M.; Asch, D.A. Completion of Advance Directives and Documented Care Preferences During the Coronavirus Disease 2019 (COVID-19) Pandemic. JAMA Netw. Open 2020, 3, e2015762. [Google Scholar] [CrossRef]
- Auriemma, C.L.; Eneanya, N.D.; Courtright, K.R. COVID-19: An Opportunity to Rethink Advance Care Planning Conversations in Acute Serious Illness. Palliat. Med. 2022, 36, 216–218. [Google Scholar] [CrossRef]
- Back, A.L.; Grant, M.S.; Mccabe, P.J. Public Messaging for Serious Illness Care in the Age of Coronavirus Disease: Cutting through Misconceptions, Mixed Feelings, and Distrust. J. Palliat. Med. 2021, 24, 816–819. [Google Scholar] [CrossRef]
- Bender, M.A.; Huang, K.-N.; Raetz, J. Advance Care Planning during the COVID-19 Pandemic. J. Am. Board Fam. Med. 2021, 34, S16–S20. [Google Scholar] [CrossRef] [PubMed]
- Block, B.L.; Smith, A.K.; Sudore, R.L. During COVID-19, Outpatient Advance Care Planning Is Imperative: We Need All Hands on Deck. J. Am. Geriatr. Soc. 2020, 68, 1395–1397. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.Y. The Underappreciated Role of Advance Directives: How the Pandemic Revitalises Advance Care Planning Actions. Eur. J. Health Law 2020, 27, 451–475. [Google Scholar] [CrossRef] [PubMed]
- Chase, J. Caring for Frail Older Adults during COVID-19: Integrating Public Health Ethics into Clinical Practice. J. Am. Geriatr. Soc. 2020, 68, 1666–1670. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Kross, E.K.; Stapleton, R.D. The Importance of Addressing Advance Care Planning and Decisions About Do-Not-Resuscitate Orders During Novel Coronavirus 2019 (COVID-19). JAMA J. Am. Med. Assoc. 2020, 323, 1771–1772. [Google Scholar] [CrossRef] [PubMed]
- Dattolo, P.C.; Toccafondi, A.; Somma, C. COVID-19 Pandemic: A Chance to Promote Cultural Sensitivity on Advance Care Planning. J. Palliat. Med. 2021, 24, 646. [Google Scholar] [CrossRef]
- Dewhurst, F.; Billett, H.; Simkiss, L.; Bryan, C.; Barnsley, J.; Charles, M.; Fleming, E.; Grieve, J.; Hacking, S.; Howorth, K.; et al. Multicenter Evaluation of 434 Hospital Deaths From COVID-19: How Can We Improve End-of-Life Care During a Pandemic? J. Pain Symptom Manag. 2021, 61, e7–e12. [Google Scholar] [CrossRef] [PubMed]
- Farrell, T.W.; Ferrante, L.E.; Brown, T.; Francis, L.; Widera, E.; Rhodes, R.; Rosen, T.; Hwang, U.; Witt, L.J.; Thothala, N.; et al. AGS Position Statement: Resource Allocation Strategies and Age-Related Considerations in the COVID-19 Era and Beyond. J. Am. Geriatr. Soc. 2020, 68, 1136–1142. [Google Scholar] [CrossRef]
- Gordon, A.L.; Goodman, C.; Achterberg, W.; Barker, R.O.; Burns, E.; Hanratty, B.; Martin, F.C.; Meyer, J.; O’Neill, D.; Schols, J.; et al. Commentary: COVID in Care Homes-Challenges and Dilemmas in Healthcare Delivery. Age Aging 2020, 49, 701–705. [Google Scholar] [CrossRef]
- Hill, L.; Lambrinou, E.; Moser, D.K.; Beattie, J.M. The COVID-19 Pandemic: Challenges in Providing Supportive Care to Those with Cardiovascular Disease in a Time of Plague. Curr. Opin. Support Palliat. Care 2021, 15, 147–153. [Google Scholar] [CrossRef]
- Hopkins, S.A.; Lovick, R.; Polak, L.; Bowers, B.; Morgan, T.; Kelly, M.P.; Barclay, S. Reassessing Advance Care Planning in the Light of Covid-19. BMJ 2020, 369, m1927. [Google Scholar] [CrossRef]
- Hughes, M.C.; Vernon, E. Hospice Response to COVID-19: Promoting Sustainable Inclusion Strategies for Racial and Ethnic Minorities. J. Gerontol. Soc. Work 2021, 64, 101–105. [Google Scholar] [CrossRef]
- Janwadkar, A.S.; Bibler, T.M. Ethical Challenges in Advance Care Planning During the COVID-19 Pandemic. Am. J. Bioeth. 2020, 20, 202–204. [Google Scholar] [CrossRef]
- Kuzuya, M.; Aita, K.; Katayama, Y.; Katsuya, T.; Nishikawa, M.; Hirahara, S.; Miura, H.; Yanagawa, M.; Arai, H.; Iijima, K.; et al. The Japan Geriatrics Society Consensus Statement “Recommendations for Older Persons to Receive the Best Medical and Long-Term Care during the COVID-19 Outbreak-Considering the Timing of Advance Care Planning Implementation”. Geriatr. Gerontol. Int. 2020, 20, 1112–1119. [Google Scholar] [CrossRef]
- Moorman, S.; Boerner, K.; Carr, D. Rethinking the Role of Advance Care Planning in the Context of Infectious Disease. J. Aging Soc. Policy 2021, 33, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Palipane, N.; Ponnampalampillai, A.; Gupta, S. Advance Care Planning for Patients with COVID-19: A Communication Guide. Br. J. Hosp. Med. 2021, 82, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Parekh de Campos, A.; Daniels, S. Ethical Implications of COVID-19: Palliative Care, Public Health, and Long-Term Care Facilities. J. Hosp. Palliat. Nurs. JHPN 2021, 23, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Parks, J.A.; Howard, M. Dying Well in Nursing Homes during COVID-19 and beyond: The Need for a Relational and Familial Ethic. Bioethics 2021, 35, 589–595. [Google Scholar] [CrossRef]
- Powell, V.D.; Silveira, M.J. Palliative Care for Older Adults with Multimorbidity in the Time of COVID 19. J. Aging Soc. Policy 2021, 33, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, C.; Nolte, L.; White, B.P.; Detering, K.M. Advance Care Planning in Australia during the COVID-19 Outbreak: Now More Important than Ever. Intern. Med. J. 2020, 50, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Swinford, E.; Galucia, N.; Morrow-Howell, N. Applying Gerontological Social Work Perspectives to the Coronavirus Pandemic. J. Gerontol. Soc. Work 2020, 63, 513–523. [Google Scholar] [CrossRef]
- Van Buren, N.R.; Weber, E.; Bliton, M.J.; Cunningham, T. V In This Together: Navigating Ethical Challenges Posed by Family Clustering during the Covid-19 Pandemic. Hastings Cent. Rep. 2021, 51, 16–21. [Google Scholar] [CrossRef]
- Wallace, C.L.; Wladkowski, S.P.; Gibson, A.; White, P. Grief During the COVID-19 Pandemic: Considerations for Palliative Care Providers. J. Pain Symptom Manag. 2020, 60, e70–e76. [Google Scholar] [CrossRef] [PubMed]
- Zaurova, M.; Krouss, M.; Israilov, S.; Hart, L.; Jalon, H.; Conley, G.; Luong, K.; Wei, E.K.; Smeltz, R.; Frankenthaler, M.; et al. Working Upstream in Advance Care Planning in Pandemic Palliative Care. Health Secur. 2020, 18, 367–371. [Google Scholar] [CrossRef] [PubMed]


| Study Characteristics | n (%) | |
|---|---|---|
| Type of study | Nonrandomized | 34 (29.6) |
| Letters/Opinions/Editorials | 28 (24.3) | |
| Quantitative Descriptive | 20 (14.4) | |
| Qualitative | 19 (16.5) | |
| Reports | 7 (6.1) | |
| Mixed methods | 7 (6.1) | |
| Country | United States | 70 (60.9) |
| United Kingdom | 21 (18.8) | |
| Canada | 6 (5.2) | |
| The Netherlands | 5 (4.3) | |
| Other | 13 (11.3) | |
| Setting | Hospital | 42 (36.5) |
| Nursing Home | 21 (18.3) | |
| Online/Telehealth | 15 (13.0) | |
| Electronic data | 9 (7.6) | |
| Academic | 5 (4.3) | |
| Other | 6 (5.2) | |
| Participants | Patients/Nursing home residents | 58 (50.4) |
| Healthcare professionals | 34 (29.6) | |
| General public | 9 (7.6) | |
| Family/Family caregivers | 6 (5.2) | |
| Medical students | 3 (2.6) | |
| Veterans | 2 (1.7) |
| ACP Barrier Codes | Citation | Category | Total | |||
|---|---|---|---|---|---|---|
| SI | ED | IN | RE | n (%) | ||
| Social distancing measures and visitation restrictions | [36,37,39,40,42,44,48,49,53,55,56,60,61,63,64,67,92,100,108,110,112,113,124,127,128,131,134,135,136,138,139,140,143,144,147] | 16 | 0 | 6 | 13 | 35 (20.7) |
| Uncertainty surrounding the COVID-19 prognosis | [36,39,40,45,48,49,53,98,124,125,128,149] | 7 | 0 | 1 | 4 | 12 (7.1) |
| Technological/Telehealth barriers | [43,49,61,63,76,80,124,136,138] | 4 | 3 | 0 | 3 | 10 (5.9) |
| Lack of awareness/knowledge of ACP | [35,55,64,66,86,90,125,128,137] | 4 | 2 | 0 | 3 | 9 (5.3) |
| Limited resources | [36,55,90,98,126,128,138,142] | 3 | 1 | 1 | 4 | 9 (5.3) |
| Personal protective equipment requirements | [39,40,44,48,53,61,126,135,145] | 6 | 0 | 0 | 3 | 9 (5.3) |
| Rapid disease progression | [38,48,60,138,139,140,141,148,149] | 3 | 0 | 0 | 6 | 9 (5.3) |
| Strained healthcare system | [40,48,55,61,92,126,130,140,149] | 4 | 0 | 1 | 4 | 9 (5.3) |
| Time constraints | [38,44,45,49,55,76,126,138,142] | 5 | 1 | 0 | 3 | 9 (5.3) |
| Cultural and religious beliefs | [57,86,90,142] | 2 | 4 | 0 | 1 | 7 (4.1) |
| Discomfort among clinicians and patients discussing end-of-life care | [36,38,49,91,126] | 4 | 2 | 0 | 1 | 7 (4.1) |
| Healthcare system barriers | [36,49,55,90,126] | 3 | 1 | 0 | 3 | 7 (4.1) |
| Emotional barriers | [46,48,82,97,140] | 3 | 0 | 1 | 1 | 5 (3.0) |
| Communication difficulties | [57,76,139,143] | 1 | 1 | 0 | 2 | 4 (2.4) |
| Distrust in the healthcare system | [65,124,125,137] | 1 | 0 | 0 | 3 | 4 (2.4) |
| Legal concerns | [36,55,127] | 2 | 0 | 0 | 2 | 4 (2.4) |
| Racial and ethnic barriers | [53,90,124,140] | 1 | 1 | 0 | 2 | 4 (2.4) |
| Familial disagreement | [38,128,140] | 1 | 0 | 0 | 2 | 3 (1.8) |
| Lack of adequate ACP training for clinicians | [76,91,142] | 0 | 2 | 0 | 1 | 3 (1.8) |
| Negative perceptions about advance care planning | [45,124,134] | 1 | 0 | 0 | 2 | 3 (1.8) |
| Financial concerns | [57,140] | 1 | 0 | 0 | 1 | 2 (1.2) |
| Low education level | [76,140] | 0 | 1 | 0 | 1 | 2 (1.2) |
| Blanket approaches to ACP | [134] | 0 | 0 | 0 | 1 | 1 (0.6) |
| Family clustering of COVID-19 | [147] | 0 | 0 | 0 | 1 | 1 (0.6) |
| Low health literacy | [90] | 0 | 1 | 0 | 0 | 1 (0.6) |
| Total | 72 | 20 | 10 | 67 | 169 (100) | |
| ACP Facilitator Codes | Citations | Category | Total | |||
|---|---|---|---|---|---|---|
| SI | ED | IN | RE | n (%) | ||
| Telehealth/virtual ACP platforms | [36,37,42,45,48,49,51,55,60,67,69,84,88,93,96,99,100,101,102,104,108,111,113,116,120,122,126,127,128,129,130,131,133,135,138,139,145,146,147,148] | 11 | 2 | 14 | 14 | 41 (16.4) |
| Training for clinicians | [45,47,62,67,70,71,72,73,74,75,76,77,78,79,80,81,82,83,86,88,89,94,97,101,108,116] | 6 | 18 | 5 | 0 | 29 (11.6) |
| Care team collaboration | [45,48,51,59,68,78,87,88,92,94,95,96,105,111,116,126,127,130,133,139,146] | 5 | 3 | 9 | 7 | 24 (9.6) |
| Innovation and flexibility in ACP documentation processes | [48,63,66,68,71,116,117,118,119,120,121,126,127,128,135,138,145,147,148] | 5 | 1 | 6 | 10 | 22 (8.8) |
| Guidance and protocols for ACP discussions | [45,52,64,71,82,87,92,94,107,112,124,129,139,141,144,146,147,148,149] | 3 | 3 | 4 | 11 | 21 (8.4) |
| ACP/palliative care experts | [47,48,51,59,60,67,73,97,99,106,109,116,124,134,144,147,148] | 7 | 1 | 5 | 5 | 18 (7.2) |
| Resources/education for patients/families | [36,54,64,65,66,69,72,80,83,85,97,121,123,127,145] | 7 | 4 | 3 | 2 | 16 (6.4) |
| Identification of those in need of ACP | [36,40,53,82,87,94,98,100,106,110,124,133] | 3 | 2 | 5 | 2 | 12 (4.8) |
| Healthcare system improvements | [49,59,68,94,105,108,116,129,133,147] | 3 | 0 | 5 | 3 | 11 (4.4) |
| Improved messaging | [58,66,88,91,125,137] | 2 | 2 | 0 | 7 | 11 (4.4) |
| Resources for clinicians | [54,62,72,74,78,88,103,109,137,145,148] | 2 | 4 | 2 | 3 | 11 (4.4) |
| Public awareness of ACP | [42,45,48,54,58,69,97,141] | 6 | 0 | 1 | 1 | 8 (3.2) |
| Proactive ACP conversations | [36,51,56,113,115,132] | 3 | 0 | 2 | 1 | 6 (2.4) |
| Understanding/fear of COVID-19 | [42,46,50,54,116] | 4 | 0 | 2 | 0 | 6 (2.4) |
| Trusting clinical relationship | [49,84,135,140] | 1 | 1 | 0 | 2 | 4 (1.6) |
| Early ACP | [135,149] | 0 | 0 | 0 | 2 | 2 (0.8) |
| Language support services | [108,137] | 0 | 0 | 1 | 1 | 2 (0.8) |
| Tablet computers | [60,108] | 1 | 0 | 1 | 0 | 2 (0.8) |
| Triggers to initiate conversations | [136,149] | 0 | 0 | 0 | 2 | 2 (0.8) |
| Individualized ACP discussion | [134] | 0 | 0 | 0 | 1 | 1 (0.4) |
| Information sharing | [139] | 0 | 0 | 0 | 1 | 1 (0.4) |
| Total | 69 | 41 | 65 | 77 | 252 (100) | |
| Study ID | Title | Country | Category | ACP Increase (%) |
|---|---|---|---|---|
| Auriemma 2020 [123] | Completion of Advance Directives and Documented Care Preferences During the Coronavirus Disease 2019 (COVID-19) Pandemic | US | IN | 396 |
| Copley 2021 [54] | ReSPECT (Recommended Summary Plan for Emergency Care and Treatment) in a Pandemic: The impact of COVID-19 on Advance Care Planning in a UK University Hospital Cardiology Department | UK | SI | 355 |
| McFarlane 2022 [117] | Advance Care Plans: Creation, Content and Use During Wave 1 of the COVID-19 Pandemic. A Retrospective Cohort Study of Coordinate My Care, a Large Electronic Palliative Care Coordination System | UK | IN | 296 |
| Connellan 2021 [50] | Documentation of Do-Not-Attempt-Cardiopulmonary-Resuscitation orders amid the COVID-19 pandemic | IR | SI | 291.5 |
| Hurlow 2021 [119] | An evaluation of advance care planning during the COVID-19 pandemic: a retrospective review of patient involvement in decision making using routinely collected data from digital ReSPECT records | UK | IN | 230.9 |
| Portz 2020 [121] | Advance Care Planning Among Users of a Patient Portal During the COVID-19 Pandemic: Retrospective Observational Study | US | IN | 148 |
| Yourman 2022 [101] | Acceptability and Effectiveness of Virtual Group Visits for Advance Care Planning | US | IN | Virtual ACP: 35 Clinic ACP: 136 |
| Gaur 2020 [112] | A Structured Tool for Communication and Care Planning in the Era of the COVID-19 Pandemic | US | IN | 114 |
| Casey 2022 [71] | Advance Care Planning for Emergency Department Patients With COVID-19 Infection: An Assessment of a Physician Training Program | US | ED | 101.6 |
| Price 2021 [77] | An Educational Intervention to Increase Advance Care Planning Activities among Emergency Medicine Providers during the COVID-19 Pandemic | US | ED | 98.4 |
| Meyers 2022 [100] | Advance Care Planning in a Geriatric Veterans Primary Care Clinic During COVID-19 | US | IN | 78 |
| Berning 2021 [87] | An advance care planning long-term care initiative in response to COVID-19 | US | ED | 46 |
| Acevedo Rodriguez 2021 [104] | Improving the quality of care in patients with COVID-19 | US | IN | AD: 37 LST notes: 3163 |
| Hui 2022 [94] | Impact of an interdisciplinary goals of care program on hospital outcomes at a comprehensive cancer center during the COVID-19 pandemic: A propensity score analysis. | US | IN | 33.3 |
| Volandes 2022 [83] | Association of an Advance Care Planning Video and Communication Intervention With Documentation of Advance Care Planning Among Older Adults: A Nonrandomized Controlled Trial | US | ED | 32 |
| Rosedale 2022 [73] | Advance Care Planning and Health Equity: Pursuing Quality Improvement in a Family Medicine Residency Clinic | US | ED | 27.9 |
| Markwalter 2022 [79] | Advance Care Planning for Emergency Department Patients with COVID-19 Infection: An Assessment of a Physician Training Program | US | ED | 25.4 |
| Singh 2021 [105] | Increasing Medical Power of Attorney Completion for Hospitalized Patients During the COVID Pandemic: A Social Work Led Quality Improvement Intervention | US | IN | 12.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayers, T.; Sakamoto, A.; Inokuchi, R.; Hanari, K.; Ring, H.Z.; Tamiya, N. Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19. Healthcare 2024, 12, 667. https://doi.org/10.3390/healthcare12060667
Mayers T, Sakamoto A, Inokuchi R, Hanari K, Ring HZ, Tamiya N. Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19. Healthcare. 2024; 12(6):667. https://doi.org/10.3390/healthcare12060667
Chicago/Turabian StyleMayers, Thomas, Ayaka Sakamoto, Ryota Inokuchi, Kyoko Hanari, Huijun Z. Ring, and Nanako Tamiya. 2024. "Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19" Healthcare 12, no. 6: 667. https://doi.org/10.3390/healthcare12060667
APA StyleMayers, T., Sakamoto, A., Inokuchi, R., Hanari, K., Ring, H. Z., & Tamiya, N. (2024). Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19. Healthcare, 12(6), 667. https://doi.org/10.3390/healthcare12060667