
Can Digital Technologies Be Useful for Weight Loss in Individuals with Overweight or Obesity? A Systematic Review

 ,
,  ,
,  , , , ,
, , , ,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
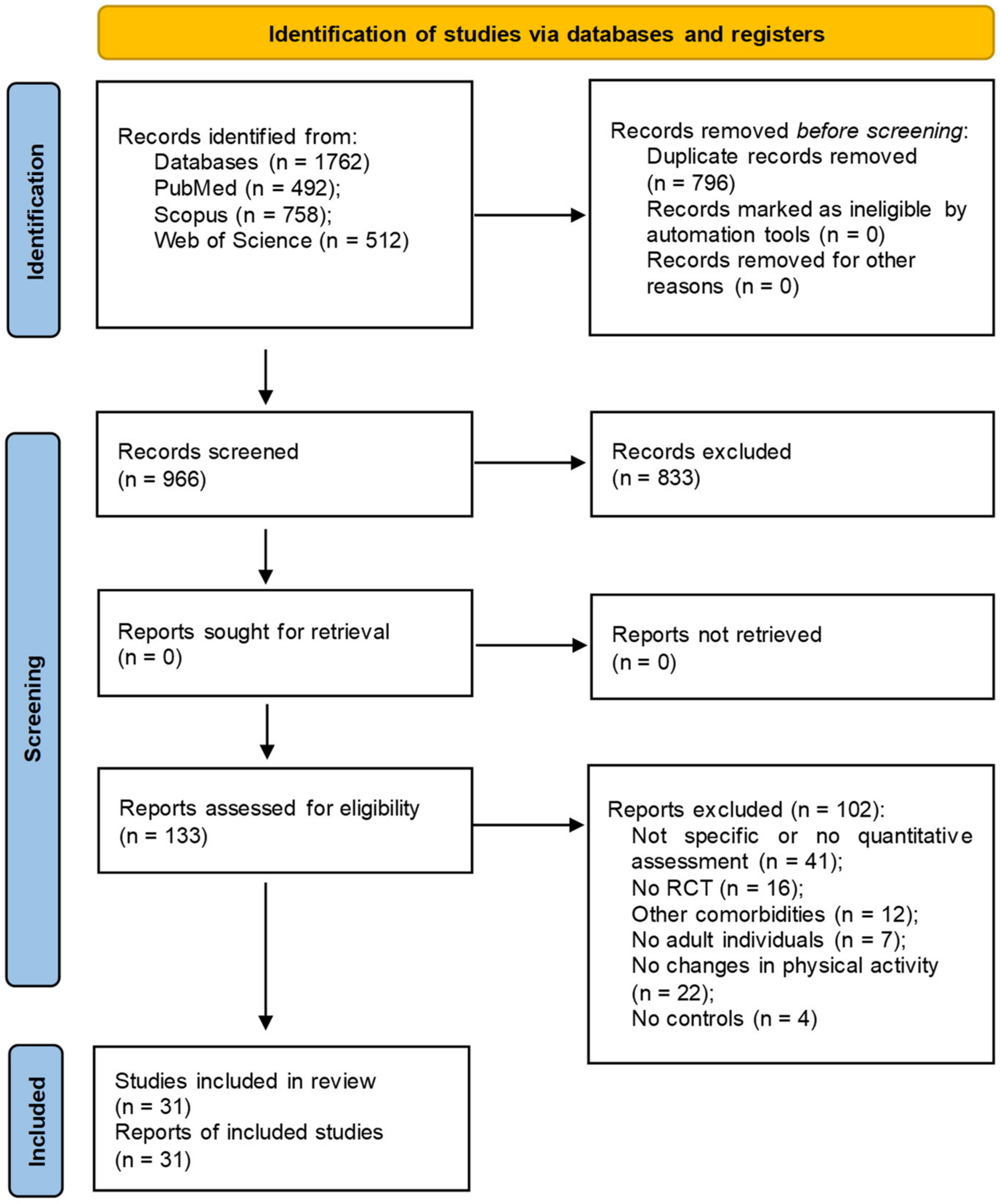
2.1. Selection Protocol and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, W. WHO recognition of the global obesity epidemic. Int. J. Obes. 2008, 32, 120–126. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. In Fact Sheets; no 311 January 2015; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 December 2023).
- Nguyen, N.T.; Nguyen, X.T.; Lane, J.; Wang, P. Relationship between obesity and diabetes in a US adult population: Findings from the National Health and Nutrition Examination Survey, 1999–2006. Obes. Surg. 2011, 21, 351–355. [Google Scholar] [CrossRef]
- World Obesity Atlas. World Obesity Federation. London. 2022. Available online: https://s3-eu-west-1.amazonaws.com/wof-files/World_Obesity_Atlas_2022.pdf (accessed on 1 December 2023).
- Chong, B.; Jayabaskaran, J.; Kong, G.; Chan, Y.H.; Chin, Y.H.; Goh, R.; Kannan, S.; Ng, C.H.; Loong, S.; Kueh, M.T.W.; et al. Trends and predictions of malnutrition and obesity in 204 countries and territories: An analysis of the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 57, 101850. [Google Scholar] [CrossRef]
- Huang, C.Y.; Yang, M.C.; Huang, C.Y.; Chiu, P.S.; Liu, Z.S.; Chang, R.I. Design and implementation of a dynamic healthcare system for weight management and health promotion. In Proceedings of the IEEE International Conference on Industrial Engineering and Engineering Management (IEEM 2017), Singapore, 10–13 December 2017; pp. 2386–2390. [Google Scholar] [CrossRef]
- Pi-Sunyer, X. The Medical Risks of Obesity. Postgrad. Med. 2009, 121, 21–23. [Google Scholar] [CrossRef]
- Argyrakopoulou, G.; Dalamaga, M.; Spyrou, N.; Kokkinos, A. Gender Differences in Obesity-Related Cancers. Curr. Obes. Rep. 2021, 10, 100–115. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Obesity and Cancer Factsheet. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/obesity-fact-sheet (accessed on 1 December 2023).
- World Obesity Federation. World Obesity (Formerly IASO) History. Available online: https://www.worldobesity.org/about/about-us/history (accessed on 1 December 2023).
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2023. Available online: https://nih.gov (accessed on 21 January 2024).
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Bussetto, L.; Misic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Eur. Guidel. Obes. Manag. Adults 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M. The health gap: The challenge of an unequal world. Lancet 2015, 386, 2442–2444. [Google Scholar] [CrossRef] [PubMed]
- Marceca, M.; Sabato, M.; Aloise, I.; Baiocchi, N.; Mancini, G. Public Health Approach to Outdoor Urban Health. In Equity in Health and Health Promotion in Urban Areas. Green Energy and Technology; Battisti, A., Marceca, M., Ricotta, G., Iorio, S., Eds.; Springer: Cham, Switzerland, 2023. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef]
- Twells, L.K.; Harris Walsh, K.; Blackmore, A.; Adey, T.; Donnan, J.; Peddle, J.; Ryan, D.; Farrell, A.; Nguyen, H.; Gao, Z.; et al. Nonsurgical weight loss interventions: A systematic review of systematic reviews and meta-analyses. Obes. Rev. 2021, 22, e13320. [Google Scholar] [CrossRef]
- Ellis, D.A. Are smartphones really that bad? Improving the psychological measurement of technology-related behaviors. Comput. Hum. Behav. 2019, 97, 60–66. [Google Scholar] [CrossRef]
- Ratan, Z.A.; Parrish, A.M.; Zaman, S.B.; Alotaibi, M.S.; Hosseinzadeh, H. Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12257. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Martínez-Pérez, B.; de la Torre-Díez, I.; López-Coronado, M. Mobile Health Applications for the Most Prevalent Conditions by the World Health Organization: Review and Analysis. J. Med. Internet Res. 2013, 15, e120. [Google Scholar] [CrossRef] [PubMed]
- Istepanian, R.; Laxminarayan, S.; Pattichis, C.S. (Eds.) M-Health: Emerging Mobile Health Systems; Springer Science & Business Media: Berlin, Germany, 2007. [Google Scholar] [CrossRef]
- World Health Organisation. Global Observatory for eHealth. Available online: https://www.who.int/observatories/global-observatory-for-ehealth (accessed on 3 December 2023).
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef] [PubMed]
- Ang, G.; Edney, S.M.; Tan, C.S.; Lim, N.; Tan, J.; Müller-Riemenschneider, F.; Chen, C. Physical Activity Trends Among Adults in a National Mobile Health Program: A Population-Based Cohort Study of 411,528 Adults. Am. J. Epidemiol. 2023, 192, 397–407. [Google Scholar] [CrossRef]
- Braakhuis, H.E.M.; Berger, M.A.M.; Bussmann, J.B.J. Effectiveness of healthcare interventions using objective feedback on physical activity: A systematic review and meta-analysis. J. Rehabil. Med. 2019, 51, 151–159. [Google Scholar] [CrossRef]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using pedometers to increase physical activity and improve health: A systematic review. JAMA 2007, 298, 2296–2304. [Google Scholar] [CrossRef]
- Brickwood, K.J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-Based Wearable Activity Trackers Increase Physical Activity Participation: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth 2019, 7, e11819. [Google Scholar] [CrossRef]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior change techniques implemented in electronic lifestyle activity monitors: A systematic content analysis. J. Med. Internet Res. 2014, 16, e192. [Google Scholar] [CrossRef]
- Duan, Y.; Shang, B.; Liang, W.; Du, G.; Yang, M.; Rhodes, R.E. Effects of eHealth-Based Multiple Health Behavior Change Interventions on Physical Activity, Healthy Diet, and Weight in People With Noncommunicable Diseases: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e23786. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.; Kassavou, A.; Sutton, S. Does self-monitoring diet and physical activity behaviors using digital technology support adults with obesity or overweight to lose weight? A systematic literature review with meta-analysis. Obes. Rev. 2021, 22, e13306. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and examples for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Tugwell, P.; Giraudeau, B.; Poiraudeau, B.; Nizard, R.; Ravaud, P. A checklist to evaluate a report of a nonpharmacological trial (CLEAR NPT) was developed using consensus. J. Clin. Epidemiol. 2005, 58, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Alkaduhimi, H.; Saarig, A.; van der Linde, J.A.; Willigenburg, N.W.; van Deurzen, D.F.P.; van den Bekerom, M.P.J. An assessment of quality of randomized controlled trials in shoulder instability surgery using a modification of the clear CLEAR-NPT score. Shoulder Elb. 2018, 10, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Kamioka, H.; Tsutani, K.; Mutoh, Y.; Okuizum, H.; Ohta, M.; Handa, S.; Okada, S.; Kitayuguchi, J.; Kamada, M.; Shiozawa, N.; et al. A systematic review of nonrandomized controlled trials on the curative effects of aquatic exercise. Int. J. Gen. Med. 2011, 4, 239–260. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Cui, J.; Liu, X.; Chen, K.W.; Chen, X.; Li, R. The effect of tai chi and Qigong exercise on depression and anxiety of individuals with substance use disorders: A systematic review and meta-analysis. BMC Complement. Med. Ther. 2020, 20, 161. [Google Scholar] [CrossRef]
- Protano, C.; Fontana, M.; De Giorgi, A.; Marotta, D.; Cocomello, N.; Crucianelli, S.; Del Cimmuto, A.; Vitali, M. Balneotherapy for osteoarthritis: A systematic review. Rheumatol. Int. 2023, 43, 1597–1610. [Google Scholar] [CrossRef]
- Apiñaniz, A.; Cobos-Campos, R.; Sáez de Lafuente-Moríñigo, A.; Parraza, N.; Aizpuru, F.; Pérez, I.; Goicoechea, E.; Trápaga, N.; García, L. Effectiveness of randomized controlled trial of a mobile app to promote healthy lifestyle in obese and overweight patients. Fam. Pract. 2019, 36, 699–705. [Google Scholar] [CrossRef]
- Balk-Møller, N.C.; Poulsen, S.K.; Larsen, T.M. Effect of a Nine-Month Web- and App-Based Workplace Intervention to Promote Healthy Lifestyle and Weight Loss for Employees in the Social Welfare and Health Care Sector: A Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e108. [Google Scholar] [CrossRef]
- Beatty, J.A.; Greene, G.W.; Blissmer, B.J.; Delmonico, M.J.; Melanson, K.J. Effects of a novel bites, steps and eating rate-focused weight loss randomised controlled trial intervention on body weight and eating behaviours. J. Hum. Nutr. Diet. 2020, 33, 330–341. [Google Scholar] [CrossRef]
- Block, G.; Azar, K.M.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H. Diabetes Prevention and Weight Loss with a Fully Automated Behavioral Intervention by Email, Web, and Mobile Phone: A Randomized Controlled Trial Among Persons with Prediabetes. J. Med. Internet Res. 2015, 17, e240. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.E.; Sereika, S.M.; Bizhanova, Z.; Parmanto, B.; Kariuki, J.; Cheng, J.; Beatrice, B.; Cedillo, M.; Pulantara, I.W.; Wang, Y.; et al. Effect of tailored, daily feedback with lifestyle self-monitoring on weight loss: The SMARTER randomized clinical trial. Obesity 2022, 30, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.J.; Lee, J.H.; Shim, J.S.; Yeom, H.; Lee, S.J.; Jeon, Y.W.; Kim, H.C. Effect of Smartphone-Based Lifestyle Coaching App on Community-Dwelling Population With Moderate Metabolic Abnormalities: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e17435. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Fenton, S.; Brown, W.J.; Collins, C.E.; Glozier, N.; Kolt, G.S.; Holliday, E.G.; Morgan, P.J.; Murawski, B.; Plotnikoff, R.C.; et al. Efficacy of a Multi-component m-Health Weight-loss Intervention in Overweight and Obese Adults: A Randomised Controlled Trial. International. Int. J. Environ. Res. Public Health 2020, 17, 6200. [Google Scholar] [CrossRef]
- Farage, G.; Simmons, C.; Kocak, M.; Klesges, R.C.; Talcott, G.W.; Richey, P.; Hare, M.; Johnson, K.C.; Sen, S.; Krukowski, R. Assessing the Contribution of Self-Monitoring through a Commercial Weight Loss App: Mediation and Predictive Modeling Study. JMIR Mhealth Uhealth 2021, 9, e18741. [Google Scholar] [CrossRef]
- Fukuoka, Y.; Gay, C.L.; Joiner, K.L.; Vittinghoff, E. A Novel Diabetes Prevention Intervention Using a Mobile App: A Randomized Controlled Trial With Overweight Adults at Risk. Am. J. Prev. Med. 2015, 49, 223–237. [Google Scholar] [CrossRef]
- Hernández-Reyes, A.; Cámara-Martos, F.; Molina Recio, G.; Molina-Luque, R.; Romero-Saldaña, M.; Moreno Rojas, R. Push Notifications From a Mobile App to Improve the Body Composition of Overweight or Obese Women: Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e13747. [Google Scholar] [CrossRef]
- Hong, J.; Kim, S.W.; Joo, H.; Kong, H.J. Effects of smartphone mirroring-based telepresence exercise on body composition and physical function in obese older women. Aging Clin. Exp. Res. 2021, 34, 1113–1121. [Google Scholar] [CrossRef]
- Hurkmans, E.; Matthys, C.; Bogaerts, A.; Scheys, L.; Devloo, K.; Seghers, J. Face-to-Face Versus Mobile Versus Blended Weight Loss Program: Randomized Clinical Trial. JMIR Mhealth Uhealth 2018, 6, e14. [Google Scholar] [CrossRef]
- Hutchesson, M.J.; Callister, R.; Morgan, P.J.; Pranata, I.; Clarke, E.D.; Skinner, G.; Ashton, L.M.; Whatnall, M.C.; Jones, M.; Oldmeadow, C.; et al. A Targeted and Tailored eHealth Weight Loss Program for Young Women: The Be Positive Be Healthe Randomized Controlled Trial. Healthcare 2018, 6, 39. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Davis, K.K.; Rogers, R.J.; King, W.C.; Marcus, M.D.; Helsel, D.; Rickman, A.D.; Wahed, A.S.; Belle, S.H. Effect of Wearable Technology Combined With a Lifestyle Intervention on Long-term Weight Loss: The IDEA Randomized Clinical Trial. JAMA 2016, 316, 1161–1171. [Google Scholar] [CrossRef]
- Jiang, W.; Huang, S.; Ma, S.; Gong, Y.; Fu, Z.; Zhou, L.; Hu, W.; Mao, G.; Ma, Z.; Yang, L.; et al. Effectiveness of companion-intensive multi-aspect weight management in Chinese adults with obesity: A 6-month multicenter randomized clinical trial. Nutr. Metab. 2021, 18, 17. [Google Scholar] [CrossRef]
- Johnson, K.E.; Alencar, M.K.; Coakley, K.E.; Swift, D.L.; Cole, N.H.; Mermier, C.M.; Kravitz, L.; Amorim, F.T.; Gibson, A.L. Telemedicine-Based Health Coaching Is Effective for Inducing Weight Loss and Improving Metabolic Markers. Telemed. J. E-Health 2019, 25, 85–92. [Google Scholar] [CrossRef]
- Johnston, C.A.; Rost, S.; Miller-Kovach, K.; Moreno, J.P.; Foreyt, J. A randomized controlled trial of a community-based behavioral counseling program. Am. J. Med. 2013, 126, 1143.e19–1143.e24. [Google Scholar] [CrossRef] [PubMed]
- Laing, B.Y.; Mangione, C.M.; Tseng, C.H.; Leng, M.; Vaisberg, E.; Mahida, M.; Bholat, M.; Glazier, E.; Morisky, D.E.; Bell, D.S. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: A randomized, controlled trial. Ann. Intern. Med. 2014, 61, S5–S12. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Sanchez-Calavera, M.A.; Repiso-Gento, I.; Adalia, E.G.; Ramirez-Manent, J.I.; Agudo-Conde, C.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Recio-Rodriguez, J.I.; Garcia-Ortiz, L. EVIDENT 3 Investigators. Investigators. Effectiveness of an mHealth Intervention Combining a Smartphone App and Smart Band on Body Composition in an Overweight and Obese Population: Randomized Controlled Trial (EVIDENT 3 Study). JMIR mHealth uHealth 2020, 8, e21771. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Repiso-Gento, I.; GAdalia, E.; Ramirez-Manent, J.I.; Sanchez-Calavera, M.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Garcia-Ortiz, L. EVIDENT 3 Investigators. EVIDENT 3 Investigators. Long-term Effectiveness of a Smartphone App Combined with a Smart Band on Weight Loss, Physical Activity, and Caloric Intake in a Population with Overweight and Obesity (Evident 3 Study): Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e30416. [Google Scholar] [CrossRef]
- Martin, C.K.; Miller, A.C.; Thomas, D.M.; Champagne, C.M.; Han, H.; Church, T. Efficacy of SmartLoss, a smartphone-based weight loss intervention: Results from a randomized controlled trial. Obesity 2015, 23, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rodríguez, A.; Martínez-Olcina, M.; Mora, J.; Navarro, P.; Caturla, N.; Jones, J. New App-Based Dietary and Lifestyle Intervention on Weight Loss and Cardiovascular Health. Sensors 2022, 22, 768. [Google Scholar] [CrossRef] [PubMed]
- Nakata, Y.; Sasai, H.; Gosho, M.; Kobayashi, H.; Shi, Y.; Ohigashi, T.; Mizuno, S.; Murayama, C.; Kobayashi, S.; Sasaki, Y. A Smartphone Healthcare Application. CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial. Nutrients 2022, 14, 4608. [Google Scholar] [CrossRef]
- Roth, L.; Ordnung, M.; Forkmann, K.; Mehl, N.; Horstmann, A. A randomized-controlled trial to evaluate the app-based multimodal weight loss program zanadio for patients with obesity. Obesity 2023, 31, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Saldivar, P.; Mira, V.; Duran, P.; Moldovan, C.; Ang, G.; Parikh, N.; Lee, M.L.; Friedman, T.C. Implementing texting programs in the P.O.W.E.R. (preventing obesity with eating right) medical group visit for weight loss. Obes. Sci. Pract. 2021, 7, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Spring, B.; Pellegrini, C.A.; Pfammatter, A.; Duncan, J.M.; Pictor, A.; McFadden, H.G.; Siddique, J.; Hedeker, D. Effects of an abbreviated obesity intervention supported by mobile technology: The ENGAGED randomized clinical trial. Obesity 2017, 25, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Stephens, J.D.; Yager, A.M.; Allen, J. Smartphone Technology and Text Messaging for Weight Loss in Young Adults: A Randomized Controlled Trial. J. Cardiovasc. Nurs. 2017, 32, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Goldstein, C.M.; Bond, D.S.; Hadley, W.; Tuerk, P.W. Web-based virtual reality to enhance behavioural skills training and weight loss in a commercial online weight management programme: The Experience Success randomized trial. Obes. Sci. Pract. 2020, 6, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Thorgeirsson, T.; Torfadottir, J.E.; Egilsson, E.; Oddsson, S.; Gunnarsdottir, T.; Aspelund, T.; Olafsdottir, A.S.; Valdimarsdottir, U.A.; Kawachi, I.; Adami, H.O.; et al. Randomized Trial for Weight Loss Using a Digital Therapeutic Application. J. Diabetes Sci. Technol. 2022, 16, 1150–1158. [Google Scholar] [CrossRef]
- Vaz, C.L.; Carnes, N.; Pousti, B.; Zhao, H.; Williams, K.J. A randomized controlled trial of an innovative, user-friendly, interactive smartphone app-based lifestyle intervention for weight loss. Obes. Sci. Pract. 2021, 7, 555–568. [Google Scholar] [CrossRef]
- Zhang, N.; Zhou, M.; Li, M.; Ma, G. Effects of Smartphone-Based Remote Interventions on Dietary Intake, Physical Activity, Weight Control, and Related Health Benefits Among the Older Population with Overweight and Obesity in China: Randomized Controlled Trial. J. Med. Internet Res. 2023, 25, e41926. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Torkamani, A.; Butte, A.J.; Glicksberg, B.S.; Schuller, B.; Rodriguez, B.; Ting, D.S.W.; Bates, D.; Schaden, E.; Peng, H.; et al. The promise of digital healthcare technologies. Front. Public Health 2023, 11, 1196596. [Google Scholar] [CrossRef]
- Irvin, L.; Madden, L.A.; Marshall, P.; Vince, R.V. Digital Health Solutions for Weight Loss and Obesity: A Narrative Review. Nutrients 2023, 15, 1858. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R.; Toth, L.P.; LaMunion, S.R.; Crouter, S.E. Step Counting: A Review of Measurement Considerations and Health-Related Applications. Sport. Med. 2017, 47, 1303–1315. [Google Scholar] [CrossRef]
- Mamede, A.; Noordzij, G.; Jongerling, J.; Snijders, M.; Schop-Etman, A.; Denktas, S. Combining Web-Based Gamification and Physical Nudges with an App (MoveMore) to Promote Walking Breaks and Reduce Sedentary Behavior of Office Workers: Field Study. J. Med. Internet Res. 2021, 23, e19875. [Google Scholar] [CrossRef]
- Valeriani, F.; Protano, C.; Marotta, D.; Liguori, G.; Romano Spica, V.; Valerio, G.; Vitali, M.; Gallè, F. Exergames in Childhood Obesity Treatment: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4938. [Google Scholar] [CrossRef] [PubMed]
- Memon, A.R.; Masood, T.; Awan, W.A.; Waqas, A. The effectiveness of an incentivized physical activity programme (Active Student) among female medical students in Pakistan: A Randomized Controlled Trial. J. Pak. Med. Assoc. 2018, 68, 1438–1445. [Google Scholar]
- Scarry, A.; Rice, J.; O’Connor, E.M.; Tierney, A.C. Usage of Mobile Applications or Mobile Health Technology to Improve Diet Quality in Adults. Nutrients 2022, 14, 2437. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; Wright, C.; Stone, C.; Ho, N.Y.; Adhyaru, P.; Kostjasyn, S.; Hickman, I.J.; Campbell, K.L.; Mayr, H.L.; Kelly, J.T. Effectiveness of dietary interventions delivered by digital health to adults with chronic conditions: Systematic review and meta-analysis. J. Hum. Nutr. Diet. 2023, 36, 632–656. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Marques, M.M. Health behavior change for obesity management. Obes. Facts 2018, 10, 666–673. [Google Scholar] [CrossRef]
- Chaudhry, U.A.R.; Wahlich, C.; Fortescue, R.; Cook, D.G.; Knightly, R.; Harris, T. The effects of step-count monitoring interventions on physical activity: Systematic review and meta-analysis of community-based randomised controlled trials in adults. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 129. [Google Scholar] [CrossRef]
- Brindal, E.; Hendrie, G.; Freyne, J.; Coombe, M.; Berkovsky, S.; Noakes, M. Design and Pilot Results of a Mobile Phone Weight-Loss Application for Women Starting a Meal Replacement Programme. J. Telemed. Telecare 2013, 19, 166–174. [Google Scholar] [CrossRef]
- Chen, Y.; Perez-Cueto, F.J.A.; Giboreau, A.; Mavridis, I.; Hartwell, H. The Promotion of Eating Behaviour Change through Digital Interventions. Int. J. Environ. Res. Public Health 2020, 17, 7488. [Google Scholar] [CrossRef]
- Tay, A.; Hoeksema, H.; Murphy, R. Uncovering Barriers and Facilitators of Weight Loss and Weight Loss Maintenance: Insights from Qualitative Research. Nutrients 2023, 15, 1297. [Google Scholar] [CrossRef]
- Jakob, R.; Harperink, S.; Rudolf, A.M.; Fleisch, E.; Haug, S.; Mair, J.L.; Salamanca-Sanabria, A.; Kowatsch, T. Factors Influencing Adherence to mHealth Apps for Prevention or Management of Noncommunicable Diseases: Systematic Review. J. Med. Internet Res. 2022, 24, e35371. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R.; Fantigrassi, M.; Motel, I. The efficacy of wearable activity tracking technology as part of a weight loss program: A systematic review. J. Sports Med. Phys. Fit. 2018, 58, 534–548. [Google Scholar] [CrossRef]
- Beleigoli, A.M.; Andrade, A.Q.; Cançado, A.G.; Paulo, M.N.; Diniz, M.F.H.; Ribeiro, A.L. Web-Based Digital Health Interventions for Weight Loss and Lifestyle Habit Changes in Overweight and Obese Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef]


{kind=link}
| Author Year Country | Sample Size Study Population | Type of Device | Type of Intervention, Duration, Frequency | Comparison | Main and Secondary Outcomes | Results | Quality |
|---|---|---|---|---|---|---|---|
| Apinaniz et al., 2019 Spain [38] | 110, 54 intervention and 56 controls; 38.5 ± 5 years; 72% F and 28% M; BMI 32.7 ± 4.9 kg/m2 | Smartphone app AKTIDIET | The AKTIDIET app on patients’ smartphones provided reinforced health advice, including exercise programs, food intake tracking and instructional videos. Patients followed up at 1, 3 and 6 months. The program required daily self-reporting of diet and exercise, with personalized feedback and weekly assignments. The examination was repeated at 16 and 38 weeks | Usual care and motivational advice including recommendations on diet and physical exercise | Body weight after 6 months and adherence to dietary and exercise recommendations | There were no significant differences in weight change, nor in the adherence to dietary or physical exercise recommendations | 6 Yes, 3 No, 1 Unclear; Medium Bias Risk |
| Balk-Møller et al., 2017 Denmark [39] | 566, 355 intervention and 211 controls; 47 ± 10 years; 92.2% F and 7.8% M; BMI 73.8 ± 15.4 kg/m2 | Web and smartphone app SoSu-life | Daily self-reporting of diet and exercise, personalized feedback about specific health issues related to the chosen pledge, with weekly assignments and challenges. The examination was repeated at 16 and 38 weeks | No activities | Change in body weight and anthropometric markers | The SoSu-life group had a larger decrease in body weight (−1.01 kg, p = 0.03), body fat percentage (−0.78%, p = 0.03), and WC (−1.79 cm, p = 0.007) after 38 weeks compared with the control group. The SoSu-life group had a larger decrease in body weight (−1.54 kg, p < 0.001) and a decrease in body fat percentage of −0.81% (p = 0.003) compared with the control group during the first 16 weeks | 9 Yes, 0 No, 1 Unclear: Low Bias Risk |
| Beatty et al., 2020 USA [40] | 72, 37 intervention and 35 controls; 37.7 ± 15.3 years, 65.3% F and 34.7% M; BMI 31.3 ± 3.2 kg/m2 | A wrist-worn ELMM device capable of tracking bites, displayed after each meal, as well as the number of steps taken by the user. | WD for 8 weeks. Workbook offered education regarding eating rate, energy intake and energy expenditure. | WO | Weight loss | No significant difference between WD and WO groups with respect to weight change [−0.46 (1.11) vs. 0.26 (0.82) kg, respectively, p = 0.40] | 4 Yes, 2 No, 4 Unclear; High Bias Risk |
| Block et al., 2015 USA [41] | 339, 163 intervention and 176 controls; 55 ± 8.9 years; 31.3% F and 68.7%; BMI 31.2 ± 4.4 kg/m2 | Alive-PD program via Web, smartphone and automated phone calls | The program offered personalized dietary and PA goals, tracking tools, health information, quizzes, social support, feedback and reminders via web, email, IVR phone calls and mobile. The program lasted for a year, with regular goal setting and contact. Users received goals weekly for the first six months and bi-weekly thereafter, plus midweek reminders. | No contact from Alive-PD system except reminders to complete a 3-month and 6-month online follow-up questionnaire | Changes in body weight, BMI, WC | Reductions in weight, BMI and WC were all significantly greater in the intervention group than the control group (p = 0.01) | 9 Yes, 0 No, 1 Unclear; Low Bias Risk |
| Burke et al., 2022 USA [42] | 502, 251 intervention and 251 controls; 45.0 ± 14.4 years; 79.5% F and 20.5% M; BMI 33.7 ± 4.0 kg/m2 | Fitbit Charge 2, smartphone app | SM+FB of diet, PA and weight in a behavioral weight-loss intervention at 6 and 12 months. The calorie goal was determined based on the person’s baseline body weight and real-time synced SM data to send messages that were responsive to the participants’ SM entries; wrist-worn Fitbit Charge 2 was used to self-monitor PA with an aim of 150 min/week by 12 weeks. Participants weighed themselves daily. In-app messages were sent 3 times daily over the 12-month intervention | SM | Weight loss and changes in BMI from baseline to 6 months, percentage of body fat, WC | At 6 months, there was a significant percentage of weight change in both groups (SM+FB: −3.16%, 95% CI: −3.85% to −2.47%, p < 0.0001; SM: −3.20%, 95% CI: −3.86% to −2.54%, p < 0.0001) but no significant between-group mean difference (−0.04%, 95% CI: −0.99% to 0.91%, p = 0.940). | 9 Yes, 0 No, 1 Unclear; Low Bias Risk |
| Cho et al., 2020 Republic of Korea [43] | 129, 88 intervention and 41 controls; 49.2 ± 7.7 years; 51.2% F and 48.8% M; BMI 26.3 ± 3 kg/m2 | Smartphone app | An app-based diet and exercise self-logging group (app only), or app-based self-logging and personalized coaching from professional dieticians and exercise coordinators group. The app delivered structured health-related curricula and personalized feedback based on reviews of the user’s logs. Assessments were performed at baseline, week 6, week 12 and week 24 | Baseline education; no apps | Weight changes, body fat mass, WC between baseline and follow-up assessments | Those using the app with the personalized coaching group had greater body weight reductions (control −0.12 ± 0.30 kg; app only −0.35 ± 0.36 kg, p = 0.67; app with personalized coaching −0.96 ± 0.37 kg, p = 0.08), specifically by body fat mass reduction (control −0.13 ± 0.34 kg; app only −0.64 ± 0.38 kg, p = 0.22; app with personalized coaching −0.79 ± 0.38 kg, p = 0.08) | 9 Yes, 0 No, 1 Unclear; Low Bias Risk |
| Duncan et al., 2020 Australia [44] | 116, 39 Enhanced, 41 Traditional and 36 Control; 44.5 ± 10.4 years; 70.7% F and 29.3% M; BMI 31.7 ± 3.9 kg/m2 | Smartphone app Balanced, Fitbit, Accelerometer (Geneactiv) | In a 6-month intervention, Enhanced and Traditional group participants received personalized dietary recommendations, access to the ‘Balanced’ smartphone app, a calorie-counting platform, a face-to-face dietary consultation, a Fitbit activity tracker, body weight scales and a handbook. | The waitlist control group was asked to maintain current weight, PA and dietary intake | Weight change | At 6 months, weight was not significantly different between the pooled intervention groups and control group (difference = −0.92, 95% CI (−3.33, 1.48)) or 12 months (difference = 0.00, 95% CI (−2.62, 2.62)). | 8 Yes, 2 No, 0 Unclear; Low Bias Risk |
| Farage et al., 2021 USA [45] | 191, 103 intervention and 88 controls; 34.8 ± 7.6 years; 51.8% F and 48.2% M; BMI 46% 25–30 and 54% over 30 kg/m2 | Smartphone app Lose it! | Electronic diet and exercise self-monitoring and weight loss interventions on 4- and 12-month weight loss; 28 phone calls over 12 months with counselors, regular feedback through email and weight monitoring using the BodyTrace e-scale. In addition, the participants received a personalized exercise plan based on their self-reported baseline PA. They were asked to gradually increase aerobic exercise from their baseline level until reaching 225–250 min weekly | Self-paced participants received assistance upon request | Weight change | At 4 months, the counselor-initiated treatment group lost an average of 3.7 kg (SD 3.6), and the self-paced treatment group lost 0.6 kg (SD 3.1). At 12 months, the counselor-initiated treatment lost 2.4 kg (SD 5.0) on average and the self-paced treatment group gained 0.2 kg (SD 5.1). | 7 Yes, 2 No, 1 Unclear; Medium Bias Risk |
| Fukuoka et al., 2015 USA [46] | 61, 30 intervention and 31 controls; 55.2 ± 9.0 years; 77% F and 23% M; BMI 33.3 ± 6.0 kg/m2 | Smartphone app and Omron pedometer | The intervention lasted 5 months and consisted of six in-person sessions and a home-based exercise program. A study-developed mobile phone app and pedometer augmented the intervention and providing self-monitoring tools (recording weight, activity and caloric intake). It was also used to deliver interactive intervention content through daily messages, video clips and quizzes | The control group used the pedometer, but the settings were changed to display the number of steps. No specific step goals were provided. Research staff removed the run-in mobile app from the participant’s iPhone or collected the iPhone if one had been provided | Percentage change in weight and BMI from baseline to 5-month follow-up, hip circumference, objectively measured (via pedometer) PA | The intervention group (n = 30) lost an average of 6.2 (5.9) kg (−6.8% [5.7%]) between baseline and 5-month follow-up compared to the control group’s (n = 31) gain of 0.3 (3.0) kg (0.3% [5.7%]) (p < 0.001). The intervention group had greater reductions in hip circumference (p < 0.001) | 6 yes, 2 no, 2 unclear; Medium Bias Risk |
| Hernández-Reyes et al., 2020 Spain [47] | 90, 45 intervention and 45 controls; 41.5 ± 11.3 years; 100% F; BMI 31.8 ± 5.3 kg/m2 | Automatic push notifications | Objectives for diet and PA through exclusive access to specific functionalities of the app and automatic push notifications on specific days with personalized health-related and motivational messages | No access to functionalities related to the self-monitoring of weight at home, gamification or prescription of PA | Body fat loss, muscle mass and weight loss at 6 months | Receiving notifications during the intervention increased body fat loss (mean −12.9% [SD 6.7] in the intervention group vs. mean −7.0% [SD 5.7] in the control group; p < 0.001) and helped to maintain muscle mass (mean −0.8% [SD 4.5] in the intervention group vs. mean −3.2% [SD 2.8] in the control group; p < 0.018). These variations between groups led to a non-significant difference in weight loss (mean −7.9 kg [SD 3.9] in the intervention group vs. mean −7.1 kg [SD 3.4] in the control group; p > 0.05). | 4 Yes, 3 No, 3 Unclear; High Bias Risk |
| Hong et al., 2022 Republic of Korea [48] | 29, 12 intervention and 17 controls; 80 ± 3.3 years; 100% F; Weight 58.63 ± 8.17 kg | Smartphone, 24-inch LCD display monitor and a smartphone mirroring device (Miracast MRC-01, Actto) | Smartphone mirroring-based telepresence exercise Program with exercise instructor who had a major in exercise physiology, in which participants exercised in their homes for 20–40 min three times a week for 12 weeks. Nutrition advice and fitness monitoring once a month. | Same exercise program at the senior citizen center | Weight loss, body composition and physical function | Weight (p = 0.006) significantly decreased in the control group, body fat percentage decreased significantly in the intervention (p = 0.026) and in the control (p = 0.001) groups, and skeletal muscle mass (p = 0.44) significantly increased in the control group. Two-way repeated-measures ANOVA revealed no significant interaction effects on all variables. | 8 Yes, 0 No, 2 Unclear; Low Bias Risk |
| Hurkmans et al., 2018 Belgium [49] | 102, 80 intervention and 22 controls; 45.5 ± 10.3 years; 70% F and 30% M; BMI 32 ± 2.0 kg/m2 | Smartphone app | All intervention groups received the same advice from a registered dietician and a qualified PA coach during a 12-week period. The methods used included a conventional face-to-face weight loss program, a weight loss app program (app group) and a partial face-to-face and partial app program (combi group) | The control group did not receive any information during the same period | Weight reduction (5% decrease), BMI, metabolic risk factors, dietary pattern and PA | In the conventional group, app group, and combi group, BMI decreased significantly (p = 0.004, p = 0.005, and p < 0.001, respectively), no significant decrease was found in the control group. A significant time x group effect was found for BMI (p = 0.006), with the control group being significantly different compared with all other intervention groups. No significant differences were found between the conventional group and the app group and between the conventional group and the combi group (p = 0.41). However, the combi group had significantly higher decrease in BMI compared with the app group (p = 0.03). | 8 Yes, 0 No, 2 Unclear; Low Bias Risk |
| Hutchesson et al., 2018 Australia [50] | 57, 29 intervention and 28 controls; 27.1 ± 4.7 years; unspecified gender; BMI 29.4 ± 2.5 kg/m2 | Advice via smartphone app, SMS, emails and website | Six-month weight loss program delivered using e-Health technologies only, comprising five delivery modes (website, app, email, text messages and social media) and using social cognitive theory and control theory theoretical frameworks. Participants received automated personalized email feedback from their accredited practicing dietitian. Individualized energy intake and energy expenditure goals were set for each participant based on their estimated energy expenditure and creating a 2500 kJ/day energy deficit to help facilitate a 0.5–1 kg weight loss/week, goals to be achieved by modifying eating and physical habits | No intervention for six months: they were instructed to continue their usual eating and PA habits | Weight change at six months | No significant between-group differences were observed for weight (p > 0.05); significant mean difference favoring the intervention group was observed for body fat (kg) (−3.10 (−5.69, 0.52), p = 0.019). | 8 Yes, 0 No, 2 Unclear; Low Bias Risk |
| Jakicic et al., 2016 USA [51] | 471, 237 intervention and 234 controls; mean 30.9 years; 71% F and 29% M; mean BMI 31.2 kg/m2 | Wearable device and web interface | Low-calorie diet, PA, and group counseling sessions. At 6 months, telephone counseling sessions and text message prompts were added to the interventions, with self-monitoring of diet and PA using a website (standard intervention) or a wearable device (enhanced intervention). Group-based sessions were scheduled weekly for the initial 6 months and monthly between months 7 and 24. | Same intervention but only with self-monitoring; no website or wearable devices | Weight change, body composition | At 24 months, weight loss was 2.4 kg (95% CI, 1.0 to 3.7) lower in the enhanced intervention group compared with the standard intervention group (p = 0.002). In post hoc analysis, the percent weight loss differed significantly between the standard intervention and enhanced intervention groups (p < 0.001). Both groups had significant improvements in body composition, with no significant difference between groups. | 9 Yes, 0 No, 1 Unclear; Low Bias Risk |
| Jiang et al., 2021 China [52] | 272, 136 intervention and 136 controls; 31.8 ± 5 years; 41.2% F and 58.8% M; BMI 32.5 ± 3.5 kg/m2 | Smartphone app and daily online instructions | Six-month intervention. Companion-Intensive Multi-aspect Weight Management (CIMWM) strategy focusing on a combination of online and offline medical interventions with daily lifestyle supervision and guidance of diet and exercise. Participants received an individualized calorie-restricted diet which was developed by registered dietitians. Individualized exercise plans were created by health managers for each participant based on their health status and exercise capacity. Participants in the CIMWM group were provided with two Fit Nutrition Bars daily as well as monthly face-to-face guidance and daily online instructions via the mobile application “Medical Weight Management”, which allowed them to upload data regarding their daily weight, as well as food diaries, lifestyle supervision and guidance of diet and exercise. | Traditional multi-aspect weight management was required to complete daily self-monitoring instead of being offered as daily online instructions | Clinically significant weight loss (defined as weight loss ≥ 5%), anthropometric measures and determination of metabolic indexes | Significant changes in BMI, body fat and skeletal muscle mass-to-visceral fat area ratio from baseline to 6 months were observed between two groups (p < 0.05). | 5 Yes, 2 No, 3 Unclear; Medium Bias Risk |
| Johnson et al., 2019 USA [53] | 30, 20 intervention and 10 controls; 43.2 ± 11 years; BMI 36.1 ± 6.8 kg/m2 | Wireless watches and weight scales to sync with personal smartphones | Participants assigned to the VCIP group received individualized health coaching by a multidisciplinary team (registered dietitian, exercise physiologist, certified athletic trainer and medical doctor) based on data uploaded over the 12-week intervention period | m-health devices; no health coaching sessions, nor team member feedback on steps per day nor calories uploaded | Weight change | There was a significant (p < 0.001) difference for post-intervention weight loss between VC (8.23 kg) compared to IP (3.2 kg) and CG (2.9 kg) | 7 Yes, 1 No, 2 Unclear; Medium Bias Risk |
| Johnston et al., 2013 USA [54] | 292, 147 intervention and 145 controls; 46.5 ± 10.5 years; 90% F and 10% M; BMI 33 ± 3.6 kg/m2 | WW smartphone application and WW online tools | WW program based on food and activity plan, group support and skills to change behavior, followed through weekly meetings. Weights and self-reported use of access modes were measured at baseline and at 3 and 6 months | Self-help group with publicly available printed materials explaining basic dietary and exercise guidelines for safe weight loss | Reductions in BMI and weight | WW subjects lost 4.6 kg and self-help subjects lost 0.6 kg at 6 months. Participants in the WW group significantly decreased their weight (F = 34.5, p < 0.001) and BMI at 6 months (F = 36.7, p < 0.001) compared with those in the self-help group | 6 Yes, 3 No, 1 Unclear; Medium Bias Risk |
| Laing et al., 2014 USA [55] | 212, 105 intervention and 107 controls; 43.1 ± 14.5 years; 73.1% F and 26.9% M; BMI 33.4 ± 7.09 kg/m2 | Smartphone app | 6 months of usual care without (n = 107) or with (n = 105) MyFitnessPal; dietary intake, PA and weight self-monitoring, goal setting, and feedback | Control group patients were free to “choose any activities you’d like to lose weight,” without specifying any particular interventions | Weight loss at 6 months, 3 self-reported behavioral mediators of weight loss (exercise, diet and self-efficacy in weight loss) at baseline and at 3 and 6 months | At 3 months, participants in the control group gained an average of 0.24 kg, whereas those in the intervention group lost 0.03 kg (between-group difference 0.27 kg [95% CI, 1.13 to 0.60 kg]; p = 0.53). At 6 months, participants in the control group gained an average of 0.27 kg and those in the intervention group lost 0.03 kg (between-group difference 0.30 kg [CI, 1.50 to 0.95 kg]; p = 0.63) | 7 Yes, 1 No, 2 Unclear; Medium Bias Risk |
| Lugones-Sanchez et al., 2020 Spain [56] | 440, 231 intervention and 209 controls; 48.1 ± 10 years; 69.3% F and 30.7% M; BMI 32.8 ± 3.4 kg/m2 | Smartphone app (EVIDENT 3 APP) and Smart band (Mi Band 2, Xiaomi) | 3-month intervention with counseling, smartphone app and smart band (Mi Band 2, Xiaomi). After 7 days, subjects were trained to use the device and the app to allow the dietary intake to be self-reported daily and PA data were collected automatically from the smart band. Once all of the daily information was collected, the app integrated the data to create personalized recommendations based on the subjects’ characteristics and specific objectives and goals for weight loss. | Controls only had counseling | Weight loss and changes in some parameters of body composition at baseline and 3 months | The mHealth intervention produced a greater loss of body weight (−1.97 kg, 95% CI −2.39 to −1.54) relative to standard counseling at 3 months (−1.13 kg, 95% CI −1.56 to −0.69): p < 0.01. A significant between-group difference was noted only in BMI (−0.54 kg/m2, 95% CI −0.84 to –0.24); p < 0.01. | 8 Yes, 1 No, 1 Unclear; Low Risk of Bias |
| Lugones-Sanchez et al., 2022 Spain [57] | 650, 318 intervention and 332 controls; 48.3 ± 9.6 years; 68.5% F and 31.5% M;BMI 33.04 ± 3.5 kg/m2 | Smartphone app, wristband, brief counseling | The intervention group received training to use the app and the smart band for 3 months; self-monitoring, tailored feedback and a PA record. The app integrated the data to create personalized healthy food recommendations. The smart band was set to congratulate the user when reaching 10,000 steps/day, and the app displayed this step recommendation | Brief counseling | Weight loss, body composition | At 12 months, significant mean differences were found between groups for weight −0.26 (−1.21 to 0.70), BMI −0.06 (−0.41 to 0.28), waist circumference −0.48 (−1.62 to 0.66), hip circumference −0.69 (−1.62 to 0.25) and body adiposity index −0.33 (−0.77 to 0.11) | 8 Yes, 1 No,1 Unclear; Low Bias Risk |
| Martin et al., 2015 USA [58] | 40, 20 intervention and 20 controls; 44.4 ± 11.8 years; 82.5% F and 17.5% M; BMI 29.8 ± 2.9 kg/m2 | Smartphone app Smartloss and accelerometer | SmartLoss participants (n = 20) were prescribed a 1200 to 1400 kcal/d diet and were provided with a smartphone, body weight scale and accelerometer that wirelessly transmitted body weight and step data to a website. Participants received feedback and treatment recommendations once a week based on their weight graph, while counselors educated each participant that the weight graph was used to objectively quantify adherence to the calorie prescription and to guide counseling and treatment recommendations | Attention-matched health education with health tips on smartphone | Change in body weight and waist circumference | Weight loss was significantly larger in the SmartLoss (least squares mean ± SEM: −9.4 ± 0.5%) compared with the Health Education group (−0.6 ± 0.5%), p < 0.001; Mean ± SEM waist circumference change for the SmartLoss group was 21.6 ± 1.00, 25.3 ± 1.01, and 26.9 ± 1.00 cm while in the Health Education group was 1.3 ± 1.04, 1.7 ± 1.04, and 1.7 ± 1.00 cm at weeks 4, 8, and 12, respectively, p < 0.05. | 6 Yes, 1 No, 3 Unclear; Medium Bias Risk |
| Martínez-Rodríguez et al., 2022 Spain [59] | 80, 40 intervention and 40 controls; 45.7 ± 8.5 years; BMI 32.9 ± 5.1 kg/m2 | Smartphone app | Dietary and activity recommendations provided with a wearable device (Fitbit Charge 2) and the dietary supplement Metabolaid®+ an activity bracelet for monitoring+ smartphone app | Dietary and activity recommendations provided with Fitbit Charge 2 and the dietary supplement + an activity bracelet for monitoring | Weight loss, body composition, anthropometric measurements | Both groups lost a significant amount of body weight (p < 0.001), while the group using the app also lowered their fat mass (p < 0.005). | 3 Yes, 4 No, 3 Unclear; High Bias Risk |
| Nakata et al., 2022 Japan [60] | 141, 72 intervention and 69 controls; 43.2 ± 9.3 years; 26% F and 74% M; BMI 27.6 ± 3.5 kg/m2 | Smartphone app Healthcare, CALO mama Plus | 3-month intervention. Smartphone healthcare application CALO mama Plus registered daily diet, exercise, calculated dietary intake and provided advice using artificial intelligence technology. The participants wore the device for at least 10 h/day for more than 3 days | No intervention; they continued their current lifestyle without any dietary apps | Body weight change over 3 months | The change in body weight was −2.4 ± 4.0 kg and −0.7 ± 3.3 kg in the intervention and control groups, respectively, with a significant between-group difference in body weight change (−1.60 kg; 95% confidence interval −2.83 to −0.38; p = 0.011). | 6 Yes, 3 No, 1 Unclear; Medium Bias Risk |
| Roth et al., 2023 Finland [61] | 150, 77 intervention and 73 controls; 43.4 ± 10.9 years; 91.3% F and 8.7% M; BMI 35.8 ± 3.2 kg/m2 | Smartphone app | 12 months of healthy lifestyle that supported sustainable weight loss through physical therapy and proper nutrition | No app or electronic devices | Weight loss and changes from baseline to 12 months in body fat distribution | The intervention group lost, on average, 7.75% (95% CI: 9.66% to 5.84%) of their initial body weight after 12 months, whereas the weight of the controls did not change (mean = 0.00% [95% CI: 1.98% to 1.99%]); p < 0.001. | 6 Yes, 3 No, 1 Unclear; Medium Bias Risk |
| Saldivar et al., 2021 USA [62] | 371, 185 intervention and 186 controls; 54.1 ± 10.5 years; 82.8% F and 17.2% M; BMI 43.1 ± 9.53 kg/m2 | Smartphone app and text messages | 12-week and 20-week texting program—POWER Program with three text messages per week, which included appointment reminders, health and wellness tips and educational information related to care and disease management. The 12- and 20-week programs allowed patients to set goals around exercise or nutrition. The 20-week program also included motivational, mental health and stress management messages to help encourage healthy lifestyle changes | Only medical group visits without any text messages | Weight loss | Both POWER and POWER + 20-week texting groups had a significant reduction in weight at their final group visit compared to their baseline (POWER, 114 ± 27 kg vs. 112 ± 26 kg, p < 0.001; POWER + 20-week texting, 111 ± 28 kg vs. 109 ± 28 kg, p < 0.01), but not the 12-week texting group (114 ± 29 kg vs. 113 ± 29 kg, p = 0.22), with no differences between the groups. | 3 Yes, 2 No, 5 Unclear; High Bias Risk |
| Spring et al., 2017 USA [63] | 96, 32 Standard, 32 Technology supported, 32 Self-guided; 39.3 ± 11.7 years, 84.4% F and 15.6% M; BMI 34.6 ± 3.0 kg/m2 | Smartphone app ENGAGED and wireless accelerometer | 6 month intervention. STND and TECH groups received eight 90 min in-person weekly group sessions. TECH used a smartphone application with social networking features and wireless accelerometer, and received 2 to 4 personalized messages per week by trained coaches with at least a bachelor’s degree who reviewed the self-monitoring and goal attainment and helped participants solve problems. If fidelity fell below 90%, the coach was retrained by a doctoral-level staff member | Self-guided (SELF) and Standard (STND) used paper diaries to self-monitor diet, activity and weight | Primary weight loss and behavioral adherence | Weight loss was greater for TECH and STND than SELF at 6 months (25.7 kg [95% confidence interval: 27.2 to 24.1] vs. 22.7 kg [95% confidence interval: 25.1 to 20.3], p < 0.05) but not at 12 months. TECH and STND did not differ except that more STND (59%) than TECH (34%) achieved 5% weight loss at 6 months (p < 0.05). | 9 Yes, 1 No, 0 Unclear; Low Bias Risk |
| Stephens et al., 2017 USA [64] | 62, 31 intervention and 31 controls; median 20 years; 71% F and 29% M; BMI 28.5 kg/m2 | Smartphone app | Smartphone application + health coach intervention and counseling sessions, providing health coach with the ability to monitor and track all participant progress on a real-time basis and text messages focused on current diet or PA status. Participants were encouraged to exercise at least 150 min/week at moderate intensity | Counseling session | Weight, BMI, WC, dietary habits, PA habits and self-efficacy for healthy eating and PA at 3 months | The control group gained a slight amount of weight (0.3 kg) from baseline to 3 months, while participants in the Smartphone + Health Coach group lost a significant amount (−1.8 kg, p < 0.01); the difference in weight change between groups was statistically significant (p = 0.026). The smartphone group also had a significant decrease in BMI (p < 0.01) and WC (p < 0.01) | 3 Yes, 2 No, 5 Unclear; High Bias Risk |
| Thomas et al., 2020 USA [65] | 146, 72 intervention and 74 controls; 58.3 ± 10.3 years; 78.1% F and 21.9% M; BMI 91.4 ± 15.6 kg/m2 | Website and smartphone app | 6 months of no-cost access to the online web-based virtual reality program, accessible via website and mobile app. Half of the participants were randomized to also receive the ES) program, which consisted of four separate ‘scenarios’ focused on challenges at home, the workplace, the gym and social gatherings that were made available to participants at weeks 2, 4, 6 and 8, respectively, with daily points goals personalized according to sex, age, starting weight and activity level | Online weight management program alone (WW) | Body weight loss, satisfaction with the weight-loss program | Both groups achieved statistically significant weight loss across the trial, with no difference in mean ± standard error weight loss between WW and WW + ES at 3 months (2.7 ± 1.1 kg vs. 4.2 ± 1.1 kg, respectively; p = 0.086) but greater weight loss in WW + ES at 6 months (2.6 ± 1.3 kg vs. 4.9 ± 1.3 kg, respectively; p = 0.042) | 8 Yes, 0 No, 2 Unclear; Low Bias Risk |
| Thorgeirsson et al., 2022 Iceland [66] | 146, 95 intervention and 51 controls; 46.8 ± 11.7 years; 92.5% F and 7.5%; BMI 36.3 ± 5.2 kg/m2 | Smartphone app Sidekick | Standard treatment supplemented with a digital therapeutic mobile application designed to increase frequency of healthy behaviors through goal-setting, self-monitoring and completion of health-related tasks in nutrition, PA and stress management for 4 months | Standard weekly coaching sessions for 4 months | BMI at 4 months | The weight loss was 3.6% among those treated per-protocol (n = 70), and 1.5% among those not treated per-protocol (n = 76) (p < 0.0001). BMI reductions of 1.4 kg/m2 (treated per-protocol) and 0.5 kg/m2 (not treated per-protocol) (p < 0.0001) were achieved. | 5 Yes, 3 No, 2 Unclear; Medium Bias Risk |
| Vaz et al., 2021 USA [67] | 28, 13 intervention and 15 controls; 43.25 ± 2.48 years; 86% F and 14% M; BMI 34.40 ± 0.96 kg/m2 | A wrist-worn three-axis accelerometer (Fitbit Charge Heart Rate™), a smartscale (Fitbit Aria™) smartphone app Fitbit™ and commercially available messaging and photo-sharing apps | Participants were instructed to step on the smartscale every morning. The app was programmed to automatically send out a reminder to motivate participants to meet the target for PA for that day, based on continuous activity data obtained from the wearable activity tracker, with remote professional coaching by the physician. Participants were instructed to wear the activity tracker as close as possible to 24 h per day, 7 days per week, and any day with <500 recorded steps indicated a tracking problem. They received conventional outpatient weight-management visits every 3 months for 6 months of the duration of the intervention | Controls received only weight-management visits | Change in weight at 6 months, changes in waist circumference | At 6 months, the intervention group experienced a statistically significant weight change of −7.16 ± 1.78 kg (mean ± SE, 95% CI −11.05 to −3.26, p < 0.01), which differed from the weight change in controls (−3.00 ± 1.05 kg (95% CI −5.27 to −0.73, p < 0.05) by −4.16 ± 2.01 kg (95% CI −8.29 to −0.02, p < 0.05). Waist circumference significantly improved (intervention vs. control: p < 0.01). | 6 yes, 2 no, 2 unclear; Medium Bias Risk |
| Zhang et al., 2023 China [68] | 642, 440 intervention and 202 controls; 46.1% F and 53.9% M; 70.1 ± 5.3 years; BMI 27.67 ± 2.63 kg/m2 | Smartphone app | The remote dietary and PA intervention group (group DPI), and the remote PA intervention group (group PI) used the app for health information collection, health assessment, guidance and feedback and follow-up. The treatment duration was 3 months. Nutritional professionals provided one-on-one personalized dietary guidance and feedback to the participants according to their age, gender, weight, food intake, chronic disease situation, choice of food type, and portion size, 3 to 5 times a week | Health education book on a reasonable diet | Weight at day 45 (time 2), and day 90 (time 3) | Compared with groups PI and controls, group DPI showed a significant decrease in weight (−1.56 vs. −0.86 kg and −1.56 vs. −0.66 kg, respectively; p < 0.05) and BMI (−0.61 vs. −0.33 kg/m2 and −0.61 vs. −0.27 kg/m2, respectively; p < 0.05) at time 2. Compared with groups PI and controls, group DPI showed a significant decrease in body weight (−4.11 vs. −1.01 kg and −4.11 vs. −0.83 kg, respectively; p < 0.05) and BMI (−1.61 vs. −0.40 kg/m2 and −1.61 vs. −0.33 kg/m2, respectively; p < 0.05) at time 3. | 9 Yes, 0 No, 1 Unclear; Low Bias Risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Protano, C.; De Giorgi, A.; Valeriani, F.; Mazzeo, E.; Zanni, S.; Cofone, L.; D’Ancona, G.; Hasnaoui, A.; Pindinello, I.; Sabato, M.; et al. Can Digital Technologies Be Useful for Weight Loss in Individuals with Overweight or Obesity? A Systematic Review. Healthcare 2024, 12, 670. https://doi.org/10.3390/healthcare12060670
Protano C, De Giorgi A, Valeriani F, Mazzeo E, Zanni S, Cofone L, D’Ancona G, Hasnaoui A, Pindinello I, Sabato M, et al. Can Digital Technologies Be Useful for Weight Loss in Individuals with Overweight or Obesity? A Systematic Review. Healthcare. 2024; 12(6):670. https://doi.org/10.3390/healthcare12060670
Chicago/Turabian StyleProtano, Carmela, Andrea De Giorgi, Federica Valeriani, Elisa Mazzeo, Stefano Zanni, Luigi Cofone, Gabriele D’Ancona, Anis Hasnaoui, Ivano Pindinello, Marise Sabato, and et al. 2024. "Can Digital Technologies Be Useful for Weight Loss in Individuals with Overweight or Obesity? A Systematic Review" Healthcare 12, no. 6: 670. https://doi.org/10.3390/healthcare12060670
APA StyleProtano, C., De Giorgi, A., Valeriani, F., Mazzeo, E., Zanni, S., Cofone, L., D’Ancona, G., Hasnaoui, A., Pindinello, I., Sabato, M., Ubaldi, F., Volpini, V., Romano Spica, V., Vitali, M., & Gallè, F. (2024). Can Digital Technologies Be Useful for Weight Loss in Individuals with Overweight or Obesity? A Systematic Review. Healthcare, 12(6), 670. https://doi.org/10.3390/healthcare12060670