
The Effect of Vocational Training on Visually Impaired People’s Quality of Life

Abstract
:1. Introduction
2. Research Materials and Methods
2.1. Design
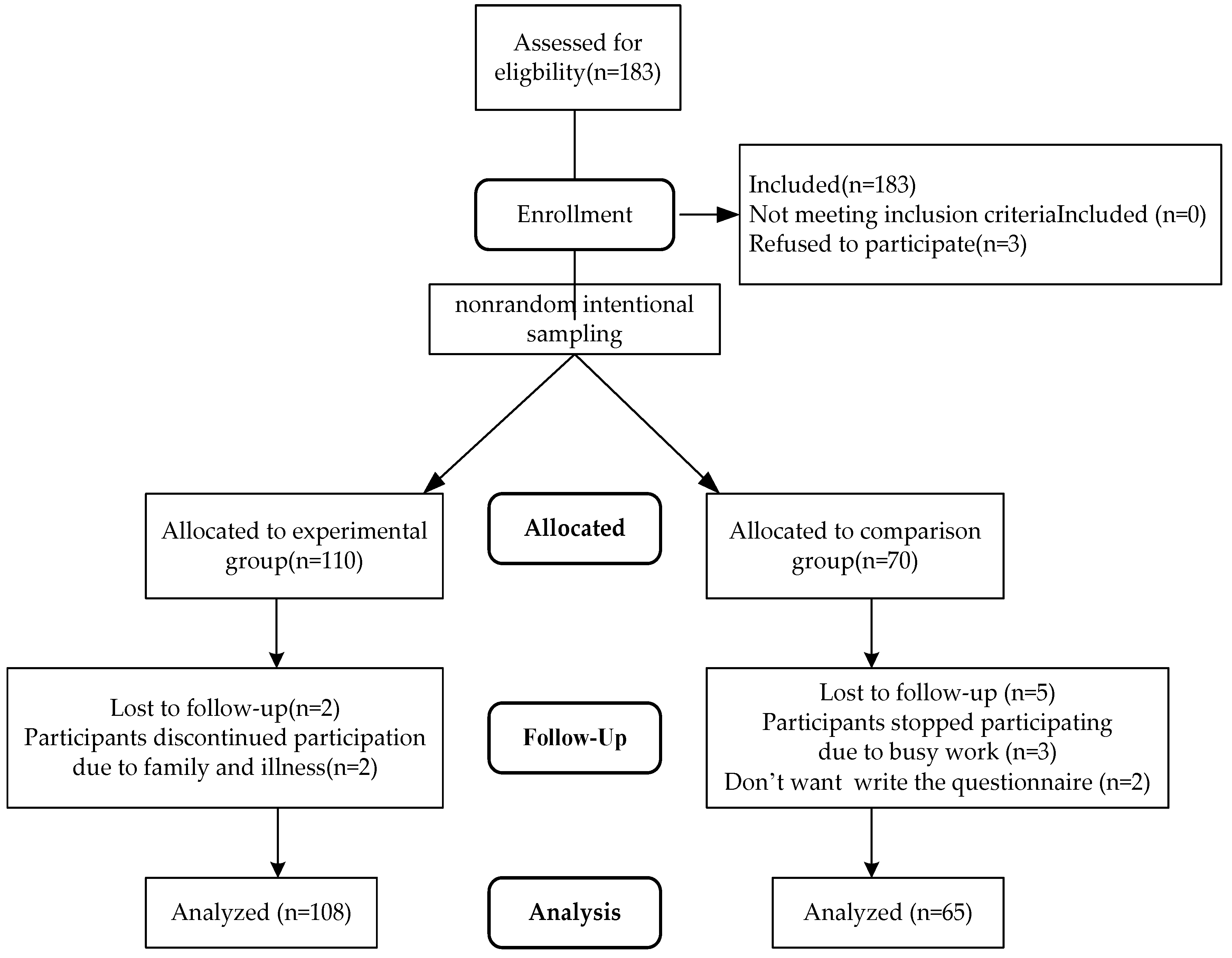
2.2. Recruitment
2.3. Vocational Training Course for The Visually Impaired

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Course Units and Content |
|---|
| Vocational reconstruction Professional competency: Deliver human physiology and professional massage training and guide participants through the requirements the technician certificate examination to strengthen their professional competency |
|
| Basic massage techniques: Effleurage, Petrissage, Friction, Tapotement and Vibrations Massage. |
|
| Targeted action: Train in orientation and action skills. Utilize residual vision and sensory perception to navigate the environment, and master the proper use of assistive devices for independently and safe walking. |
|
| Life reconstruction and Self-care competency: Training to enable individuals with visual impaired to care for themselves in their daily lives |
|
| Information utilization competency: Computer learning for the visually impaired to establish document processing and online information utilization skills |
|
2.4. Measurements
2.4.1. Demographic Information
2.4.2. WHOQOL-BREF TW
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Comparing Personal Characteristics
3.2. Overall and QOL Questionnaire of the Visually Impaired Participants before Vocational Training
3.3. Comparing Pretest and Posttest Scores of the Visually Impaired Participants’ QOL after Vocational Training
3.4. Differences in the Scores of the Experimental and Control Groups on the QOL Questionnaire in Vocational Training
4. Discussion
5. Conclusions and Suggestions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Governments Commit to Accelerate Action to Improve Access to Eye Care Services 2021. Available online: https://www.who.int/news/item/23-07-2021-governments-commit-to-accelerate-action-to-improve-access-to-eye-care-services (accessed on 6 March 2023).
- Bourne, R.R.; Adelson, J.; Flaxman, S.; Briant, P.; Bottone, M.; Vos, T.; Naidoo, K.; Braithwaite, T.; Cicinelli, M.; Jonas, J.; et al. Global Prevalence of blindness and distance and near vision impairment in 2020: Progress towards the vision 2020 targets and what the future holds. Investig. Ophthalmol. Vis. Sci. 2020, 61, 2317. [Google Scholar]
- Sohail, A.; Du, J.; Nawaz Abbasi, B.; Taiwo, A.K. Prevalence, causes, and impact of self-reported vision impairment among older people in China: Findings from the China health and retirement longitudinal study. Br. J. Vis. Impair. 2023, 41, 761–781. [Google Scholar] [CrossRef]
- American Foundation for the Blind (ABF). Facts and Figures on Adults with Vision Loss. Available online: https://www.afb.org/research-and-initiatives/statistics/adults (accessed on 16 March 2023).
- Statista. Number of Individuals Affected with Vision Loss in The United Kingdom from 1990 to 2020, by Severity 2021. Available online: https://www.statista.com/statistics/1200836/vision-impaired-in-the-uk-UK. (accessed on 6 March 2023).
- Ministry of Health and Welfare. Disability Statistics Section. Available online: https://dep.mohw.gov.tw (accessed on 2 February 2023).
- Lew, H.L.; Tanaka, C.; Pogoda, T.K.; Hall, J.W., III. Auditory, vestibular, and visual impairments. In Braddom’s Physical Medicine and Rehabilitation; Elsevier: Washington, DC, USA, 2021; pp. 1101–1120. [Google Scholar]
- Barnes, C. Understanding the social model of disability: Past, present and future. In Routledge Handbook of Disability Studies; Routledge: London, UK, 2019; pp. 14–31. [Google Scholar]
- Jones, N.; Bartlett, H.E.; Cooke, R. An analysis of the impact of visual impairment on activities of daily living and vision-related quality of life in a visually impaired adult population. Br. J. Vis. Impair. 2019, 37, 50–63. [Google Scholar] [CrossRef]
- Sweeting, J.; Merom, D.; Astuti, P.A.S.; Antoun, M.; Edwards, K.; Ding, D. Physical activity interventions for adults who are visually impaired: A systematic review and meta-analysis. BMJ Open 2020, 10, e034036. [Google Scholar] [CrossRef]
- Aghazadeh, F.; Riazi, A.; Kamali, M. The strategies used by visually impaired and blind people in Iran to cope with difficulty performing daily living activities. Arch. Rehabil. 2021, 22, 196–209. [Google Scholar] [CrossRef]
- Demmin, D.L.; Silverstein, S.M. Visual impairment and mental health: Unmet needs and treatment options. Clin. Ophthalmol. 2020, 14, 4229–4251. [Google Scholar] [CrossRef]
- Varadaraj, V.; Friedman, D.S.; Swenor, B.K. Low vision, vision disability, and blindness. In Albert and Jakobiec’s Principles and Practice of Ophthalmology; Springer International Publishing: Cham, Switzerland, 2022; pp. 4945–4957. [Google Scholar]
- Kim, H.N. Older adults with visual disabilities and fear of falling associated with activities of daily living. Int. J. Hum. Factors Ergon. 2021, 8, 64–84. [Google Scholar] [CrossRef]
- Panigrahi, A.; Nageswar Rao, G.; Kumari Konar, A. Vision-related quality of life and its sociodemographic correlates among individuals with visual impairments. J. Vis. Impair. Blind. 2021, 115, 319–328. [Google Scholar] [CrossRef]
- Lund, E.M.; Cmar, J.L. A systematic review of factors related to employment in transition-age youth with visual impairments. Rehabil. Psychol. 2020, 65, 122–136. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Hays, R.D. Health-related quality of life measurement in public health. Annu. Rev. Public. Health 2022, 43, 355–373. [Google Scholar] [CrossRef]
- Lin, C.Y.; Wang, J.D.; Liu, L.F. Can we apply WHOQOL-AGE to Asian population? Verifying its factor structure and psychometric properties in a convenience sample from Taiwan. Front. Public. Health 2020, 8, 575374. [Google Scholar] [CrossRef]
- Yao, G.; Chung, C.W.; Yu, C.F.; Wang, J.D. Development and verification of validity and reliability of the WHOQOLBREF Taiwan version. J. Formos. Med. Assoc. 2022, 101, 342–351. [Google Scholar]
- Chang, C.W.; Su, K.C.; Lu, F.C.; Cheng, H.M.; Cheng, C.Y. Visual function and visual perception among senior citizens with mild cognitive impairment in Taiwan. Healthcare 2021, 10, 20. [Google Scholar] [CrossRef]
- Fang, I.M.; Fang, Y.J.; Hu, H.Y.; Weng, S.H. Association of visual impairment with cognitive decline among older adults in Taiwan. Sci. Rep. 2021, 11, 17593. [Google Scholar] [CrossRef]
- Candy, B.; Armstrong, M.; Flemming, K.; Kupeli, N.; Stone, P.; Vickerstaff, V.; Wilkinson, S. The effectiveness of aromatherapy, massage and reflexology in people with palliative care needs: A systematic review. Palliat. Med. 2020, 34, 179–194. [Google Scholar] [CrossRef]
- Whatley, J.; Perkins, J.; Samuel, C. Reflexology: Exploring the mechanism of action. Complement. Ther. Clin. Pract. 2022, 48, 101606. [Google Scholar] [CrossRef]
- Hasanpour, M.; Mohammadi, M.M.; Shareinia, H. Effects of reflexology on premenstrual syndrome: A systematic review and meta-analysis. Biopsychosoc. Med. 2019, 13, 25. [Google Scholar] [CrossRef]
- Guo, P.P.; Fan, S.L.; Li, P.; Zhang, X.H.; Liu, N.; Wang, J.; Zhang, W. The effectiveness of massage on peri-operative anxiety in adults: A meta-analysis of randomized controlled trials and controlled clinical trials. Complement. Ther. Clin. Pract. 2020, 41, 101240. [Google Scholar] [CrossRef]
- McCullough, J.E.M.; Liddle, S.D.; Sinclair, M.; Close, C.; Hughes, C.M. The physiological and biochemical outcomes associated with a reflexology treatment: A systematic review. Evid. Based Complement. Altern. Med. 2014, 2014, 502123. [Google Scholar] [CrossRef]
- Donoyama, N.; Takeda, F. Mental health and related factors among massage practitioners with visual impaired. Ind. Health 2007, 45, 191–198. [Google Scholar] [CrossRef]
- Shah, K.; Frank, C.R.; Ehrlich, J.R. The association between vision impairment and social participation in community-dwelling adults: A systematic review. Eye 2020, 34, 290–298. [Google Scholar] [CrossRef]
- Zhang, J.D. Using the 108 new curriculum service group curriculum and design to explore the existence of massage technician certificates. Taiwan Educ. Rev. Mon. 2020, 9, 94–97. [Google Scholar]
- Ministry of Health and Welfare. Laws Regulations Database of Taiwan 2021. Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=D0050046 (accessed on 6 March 2023).
- Huang, P.H.; Chang, C.H.S.; Chen, S.T. A multiple case study of the career construction and career development process of people with acquired visual impairment. J. Spec. Educ. 2023, 57, 71–102. [Google Scholar]
- Chan, G. The role of the Hong Kong society for the blind in services to the visually impaired in Hong Kong and the Asian region. U.S. Chin. J. Ophthalmol. 2001, 1, 1–6. [Google Scholar]
- Kimura, A.; Kuribayashi, M.; Mai, D.T.H.; Ichiman, Y. Survey conducted on use of massage room at Nguyen Dinh Chieu school for the blind in Vietnam. TCT Educ. Disabil. 2003, 2, 63–69. [Google Scholar]
- Hu, M.J. Physical therapy education for the visually impaired in the United Kingdom. J. Med. Educ. 2000, 4, 275–284. [Google Scholar]
- Munemo, E.; Tom, T. Problems of unemployment faced by visually impaired people. Greener J. Soc. Sci. 2013, 3, 203–219. [Google Scholar] [CrossRef]
- Cunningham, I. Disabled people and employment: A study of the working lives of visually impaired physio-therapists. Empl. Relat. 2002, 24, 466–468. [Google Scholar]
- Li, X.H.; Xu, S.Q.; Hu, L.J. Protection or restriction: An analysis of the blind massage policy for employment rights of persons with visual impairments in China. J. Vis. Impair. Blind. 2022, 116, 85–95. [Google Scholar] [CrossRef]
- Atkinson, K.; Hutchinson, J.O. Visually impaired physiotherapists: Challenging professional attitudes. Intl. Congr. Ser. 2005, 1282, 908–912. [Google Scholar] [CrossRef]
- China Economic Net. Jobs for the Blind, What Else Can I Do Besides a Massage? Investigate Employment Status of the Blind. Available online: http://www.ce.cn/xwzx/shgj/gdxw/202110/16/t20211016_36998601.shtml (accessed on 22 March 2023).
- Siedlecki, S.L. Quasi-experimental research designs. Clin. Nurse Spec. 2020, 34, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample size determination and power analysis using the G* Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 2013; p. 413. [Google Scholar]
- Chu, H.Y.; Chan, H.S. Loneliness and social support among the middle-aged and elderly people with visual impairment. Int. J. Environ. Res. Public. Health 2022, 19, 14600. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.Y.; Chan, H.S.; Li, W.H. Research on the effectiveness of massage training courses for the visually impaired in career reconstruction. J. Beauty Technol. 2022, 19, 5–21. [Google Scholar]
- Institute for the Blind of Taiwan. Massage Technology Research and Development and Teaching Center. Available online: http://www.ibt.org.tw/RWD01/List.aspx?tid=87 (accessed on 2 February 2022).
- Mu-Kuang Rehabilitation Center for the Blind. Massage Vocational Training for the Visually Impaired. Available online: https://www.mukuang.org.tw/contents/text?id=67 (accessed on 3 March 2022).
- Yao, G.; Wu, C.H. Factorial invariance of the WHOQOL-BREF among disease groups. Qual. Life Res. 2005, 14, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Yao, G. Development and applications of the WHOQOL-Taiwan version. J. Formos. Med. Assoc. 2002, 6, 193–200. [Google Scholar]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; LIVSFORSK network. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef]
- Weisz, G.; Nannestad, B. The World Health Organization and the global standardization of medical training, a history. Glob. Health 2021, 17, 96. [Google Scholar] [CrossRef]
- Lee, M.K.; Oh, J. Health-related quality of life in older adults: Its association with health literacy, self-efficacy, social support, and health-promoting behavior. Healthcare 2020, 8, 407. [Google Scholar] [CrossRef]
- Marques, A.P.; Ramke, J.; Cairns, J.; Butt, T.; Zhang, J.H.; Muirhead, D.; Burton, M.J. Global economic productivity losses from vision impairment and blindness. eClinicalMedicine 2021, 35, 100852. [Google Scholar] [CrossRef]
- Brunes, A.; Heir, T. Visual impairment and depression: Age-specific prevalence, associations with vision loss, and relation to life satisfaction. World J. Psychiatry 2020, 10, 139. [Google Scholar] [CrossRef] [PubMed]
- Assi, L.; Chamseddine, F.; Ibrahim, P.; Sabbagh, H.; Rosman, L.; Congdon, N.; Swenor, B.K. A global assessment of eye health and quality of life: A systematic review of systematic reviews. JAMA Ophthalmol. 2021, 139, 526–541. [Google Scholar] [CrossRef] [PubMed]
- Swenor, B.K.; Lee, M.J.; Varadaraj, V.; Whitson, H.E.; Ramulu, P.Y. Aging with vision loss: A framework for assessing the impact of visual impairment on older adults. Gerontologist 2020, 60, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Lund, E.M.; Cmar, J.L. A systematic review of factors related to employment outcomes for adults with visual impairments. J. Vis. Impair. Blind. 2019, 113, 493–517. [Google Scholar] [CrossRef]
- Frick, K.D.; Foster, A. The magnitude and cost of global blindness: An increasing problem that can be alleviated. Am. J. Ophthalmol. 2023, 135, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Lund, E.M.; Cmar, J.L. Factors related to employment outcomes for vocational rehabilitation consumers with visual impairments: A systematic review. J. Vis. Impair. Blind. 2019, 113, 518–537. [Google Scholar] [CrossRef]
- Cmar, J.L.; McDonnall, M.C. Effectiveness of a job search training program for youth with visual impairments. Career Dev. Transit. Except. Individ. 2019, 42, 214–224. [Google Scholar] [CrossRef]
- Henry, S. Active Imagination, Wellbeing and Ways of Seeing: A Phenomenological Inquiry into Experiences of Adult Learners with Visual Impairments. Ph.D. Dissertation, Lesley University, Cambridge, MA, USA, 2023. [Google Scholar]
- Wrzesińska, M.; Binder, K.; Tabała, K.; Lipert, A.; Miller, E. Burnout and quality of life among massage therapists with visual impaired. J. Occup. Rehabil. 2019, 29, 384–394. [Google Scholar] [CrossRef]
- Dryden, T.; Moyer, C.A. Massage Therapy: Integrating Research and Practice; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Field, T. Massage therapy research review. Complement. Ther. Clin. Pract. 2016, 24, 19–31. [Google Scholar] [CrossRef]
- Heppe, E.C.; Kef, S.; de Moor, M.H.; Schuengel, C. Loneliness in young adults with a visual impaired: Links with perceived social support in a twenty-year longitudinal study. Res. Dev. Disabil. 2020, 101, 103634. [Google Scholar] [CrossRef]
- Brunes, A.; Hansen, M.B.; Heir, T. Post-traumatic stress reactions among individuals with visual impaired: A systematic review. Disabil. Rehabil. 2018, 41, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Hawkley, L.C. Loneliness. In Handbook of Individual Differences in Social Behavior; Leary, M.R., Hoyle, R.H., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 227–240. [Google Scholar]
- Malakpa, S.W. Problems and prospects in employment and job retention of the blind and visually impaired in the United States: A future concern of special education. Int. J. Spec. Educ. 2007, 22, 53–58. [Google Scholar]
- Fernandes, H.; Costa, P.; Filipe, V.; Paredes, H.; Barroso, J. A review of assistive spatial orientation and navigation technologies for the visually impaired. Univers. Access Inf. Soc. 2019, 18, 155–168. [Google Scholar] [CrossRef]
- Zijlstra, G.R.; Ballemans, J.; Kempen, G.I. Orientation and mobility training for adults with low vision: A new standardized approach. Clin. Rehabil. 2013, 27, 3–18. [Google Scholar] [CrossRef]
- Kamali, N.; Ashori, M. The effectiveness of orientation and mobility training on the quality of life for students who are blind in Iran. Br. J. Vis. Impair. 2023, 41, 108–120. [Google Scholar] [CrossRef]
- Kuriakose, B.; Shrestha, R.; Sandnes, F.E. Smartphone navigation support for blind and visually impaired people-a comprehensive analysis of potentials and opportunities. In International Conference on Human-Computer Interaction; Springer International Publishing: New York, NY, USA, 2020; pp. 568–583. [Google Scholar]
- Luu, W.; Kalloniatis, M.; Bartley, E.; Tu, M.; Dillon, L.; Zangerl, B.; Ly, A. A holistic model of low vision care for improving vision-related quality of life. Clin. Exp. Optom. 2020, 103, 733–741. [Google Scholar] [CrossRef]




| Variables | All Participants (N = 173) n (%) | Experimental Group (N = 108) n (%) | Control Group (N = 65) n (%) | χ2 | p | |
|---|---|---|---|---|---|---|
| Age (years) | 20–30 years old | 36 (20.7%) | 23 (21.3%) | 13 (20.1%) | 0.674 | 0.879 |
| 31–40 years old | 40 (22.8%) | 26 (24.1%) | 14 (21.5%) | |||
| 41–50 years old | 60 (34.5%) | 38 (35.2%) | 22 (33.8%) | |||
| 51–60 years old | 37 (22.0%) | 21 (19.4%) | 16 (24.6%) | |||
| Average age | 41.3 | 40.3 | 42.7 | |||
| Gender | Male | 97 (55.5%) | 59 (54.6%) | 38 (58.5%) | 0.242 | 0.639 |
| Female | 76 (43.5%) | 49 (45.4%) | 27 (41.5%) | |||
| Educational level | Junior and below | 20 (11.7%) | 12 (11.1%) | 8 (12.3%) | 1.233 | 0.749 |
| Senior high | 34 (36.0%) | 43 (39.8%) | 21 (32.3%) | |||
| College and university | 83 (48.6%) | 50 (46.3%) | 33 (50.8%) | |||
| Graduate school | 6 (3.5%) | 3 (2.8%) | 3 (4.6%) | |||
| Religion | None | 38 (21.9%) | 21 (19.4%) | 17 (26.1%) | 1.427 | 0.929 |
| Buddhism | 89 (51.4%) | 62 (57.4%) | 27 (41.5%) | |||
| Taoism | 31 (17.9%) | 15 (13.8%) | 16 (24.6%) | |||
| Christianity | 15 (8.7%) | 10 (9.25%) | 5 (7.60%) | |||
| Marital status | Married | 74 (43.2%) | 45 (41.7%) | 29 (44.6%) | 0.374 | 0.856 |
| Single | 80 (46.3%) | 50 (46.3%) | 30 (46.2%) | |||
| Others | 19 (10.6%) | 13 (12.0%) | 6 (9.2%) | |||
| Visual impair reasons | Disease | 83 (47.9%) | 43 (24.9%) | 40 (23.1%) | 0.377 | 0.945 |
| Injury | 29 (16.7%) | 16 (9.3%) | 13 (7.5%) | |||
| Congenital | 61 (35.3%) | 32 (18.5%) | 29 (16.8%) | |||
| Living status | Alone | 29 (16.8%) | 18 (16.7%) | 11 (16.9%) | 0.809 | 0.847 |
| With family members | 127 (73.4%) | 81 (75.0%) | 46 (70.8%) | |||
| With relatives | 8 (4.6%) | 4 (3.7%) | 4 (6.2%) | |||
| Others | 9 (5.2%) | 5 (4.6%) | 4 (6.2%) | |||
| Variables | Mean (SD) | Mean (SD) | Mean (SD) | t-value | p | |
| Quality of life | 3.08 (0.74) | 3.09 (0.36) | 3.07 (0.32) | −1.94 | 0.50 | |
| Variables | Overall | T0 | T1 | ||||
|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | Experimental Group | Control Group | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | p | Mean (SD) | Mean (SD) | p | |
| Quality of life | 49.87 (7.86) | 49.77 (7.73) | 49.97 (7.97) | 0.15 | 60.58 (9.15) | 50.11 (8.26) | 0 .001 |
| Overall | 3.08 (0.74) | 3.09 (0.76) | 3.07 (0.72) | 0.18 | 3.34 (0.81) | 3.10 (0.85) | 0 .001 |
| 1. How would you rate your quality of life? | 3.11 (0.76) | 3.12 (0.87) | 3.10 (0.65) | 0.27 | 3.43 (1.16) | 3.15 (0.96) | 0 .001 |
| 2. How satisfied are you with your health? | 3.06 (0.73) | 3.07 (0.78) | 3.05 (0.68) | 0.36 | 3.25 (0.81) | 3.06 (0.65) | 0 .001 |
| Physical health | 10.82 (2.64) | 10.84 (2.65) | 10.80 (2.63) | 0.23 | 14.44 (2.91) | 11.08 (2.78) | 0.001 |
| 3. How much does physical pain hinder your essential activities? | 2.43 (0.87) | 2.43 (0.75) | 2.42 (0.98) | 0.68 | 2.72 (0.61) | 2.52 (0.87) | 0.001 |
| 4. How essential is medical treatment for your daily functioning? | 2.92 (0.89) | 2.92 (0.84) | 2.92 (0.93) | 0.20 | 4.01 (0.88) | 2.95 (0.83) | 0.001 |
| 10. Do you have enough energy for everyday life? | 3.03 (0.93) | 3.04 (0.92) | 3.01 (0.93) | 0.11 | 3.72 (1.03) | 3.05 (0.84) | 0.001 |
| 15. How well are you able to get around? | 2.68 (0.77) | 2.70 (0.81) | 2.65 (0.73) | 0.09 | 3.42 (1.06) | 2.89 (1.01) | 0.001 |
| 16. How satisfied are you with your sleep? | 3.08 (1.02) | 3.07 (0.98) | 3.10 (1.06) | 0.41 | 3.47 (1.07) | 3.25 (0.98) | 0.001 |
| 17. How content are you with your daily living capabilities? | 2.56 (0.68) | 2.57 (0.69) | 2.54 (0.67) | 0.46 | 3.83 (1.04) | 2.51 (0.64) | 0.001 |
| 18. How satisfied are you with your work capacity? | 2.30 (0.81) | 2.28 (0.73) | 2.32 (0.89) | 0.34 | 4.10 (0.61) | 2.25 (0.72) | 0 .001 |
| Psychological | 12.89 (2.99) | 12.88 (2.98) | 12.89 (2.01) | 0.79 | 16.25 (2.93) | 12.76 (2.97) | 0 .001 |
| 5. How much do you enjoy life? | 2.64 (0.72) | 2.62 (0.69) | 2.66 (0.75) | 0.32 | 4.09 (0.73) | 2.65 (0.88) | 0 .001 |
| 6. To what extent do you feel your life is meaningful? | 3.17 (0.31) | 3.21 (0.35) | 3.12 (0.26) | 0.28 | 4.32 (0.58) | 3.25 (0.79) | 0 .001 |
| 7. How well are you able to concentrate? | 3.20 (0.40) | 3.21 (0.15) | 3.18 (0.65) | 0.26 | 3.58 (0.56) | 3.26 (0.64) | 0 .001 |
| 11. Are you able to accept your bodily appearance? | 3.56 (0.73) | 3.51 (0.68) | 3.61 (0.78) | 0.12 | 4.18 (0.70) | 3.52 (0.68) | 0 .001 |
| 19. How satisfied are you with yourself? | 3.32 (0.41) | 3.31 (0.46) | 3.32 (.035) | 0.42 | 4.15 (0.51) | 3.21 (0.53) | 0 .001 |
| 26. How often do you have negative feelings such as blue mood, despair, anxiety, and depression? | 3.45 (0.68) | 3.48 (0.67) | 3.42 (0.69) | 0.21 | 3.97 (0.84) | 3.25 (0.81) | 0 .001 |
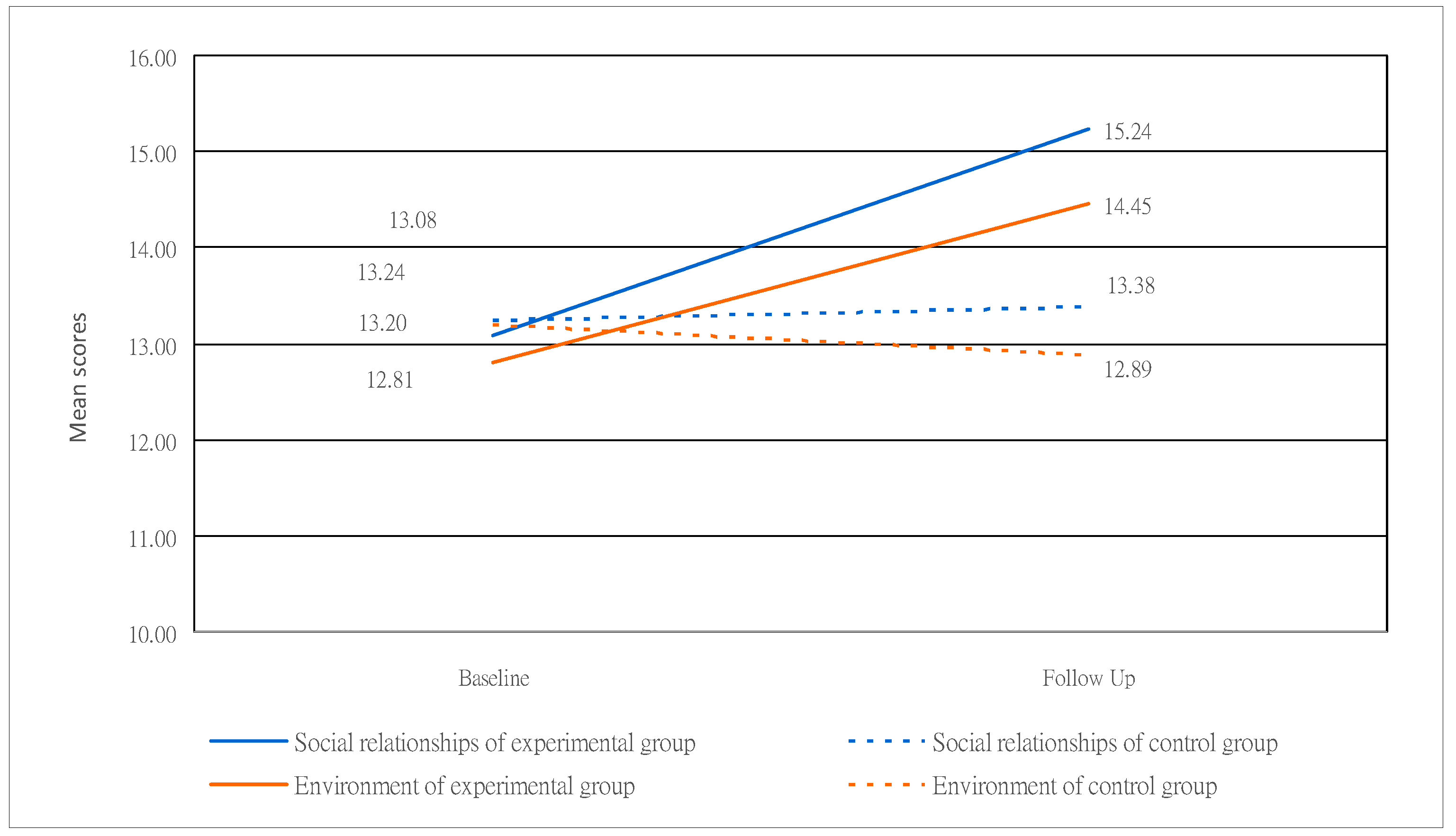
| Social relationships | 13.14 (3.07) | 13.24 (3.08) | 13.20 (3.05) | 0.20 | 15.44 (3.55) | 13.38 (3.45) | 0 .001 |
| 20. How satisfied are you with your personal relationships? | 3.37 (0.91) | 3.36 (0.85) | 3.38 (0.96) | 0.51 | 3.98 (0.83) | 3.35 (0.74) | 0 .001 |
| 21. How satisfied are you with your sex life? | 3.12 (0.82) | 3.12 (0.86) | 3.11 (0.78) | 00.28 | 3.65 (0.91) | 3.21 (0.65) | 0 .001 |
| 22. How content are you with the support from your friends? | 3.55 (1.10) | 3.55 (1.12) | 3.55 (1.08) | 0.85 | 4.15 (0.45) | 3.52 (0.31) | 0 .001 |
| 27. Do you feel respected by others? | 3.20 (0.88) | 3.24 (0.91) | 3.17 (0.84) | 0.19 | 3.75 (0.68) | 3.21 (0.97) | 0 .001 |
| Environment | 12.95 (2.92) | 12.81 (2.87) | 13.08 (2.96) | 0.50 | 14.45 (3.42) | 12.89 (2.63) | 0 .001 |
| 8. How safe do you feel in your daily life? | 2.95 (0.51) | 2.95 (0.53) | 2.95 (0.49) | 0.89 | 3.51 (0.60) | 2.65 (0.95) | 0 .001 |
| 9. How healthy is your physical environment? | 3.17 (1.05) | 3.23 (1.09) | 3.11 (1.01) | 0.11 | 3.13 (0.71) | 3.10 (0.89) | 0.91 |
| 12. Have you enough money to meet your needs? | 2.42 (0.68) | 2.42 (0.64) | 2.41 (0.73) | 0.58 | 3.28 (0.76) | 3.12 (0.97) | 0 .001 |
| 13. How available to you is the information that you need in your day-to-day life? | 2.99 (0.95) | 3.02 (0.98) | 2.85 (0.92) | 0.06 | 3.66 (0.57) | 3.10 (0.53) | 0 .001 |
| 14. To what extent do you have the opportunity for leisure activities? | 2.71 (0.83) | 2.77 (0.98) | 2.65 (0.68) | 0.05 | 3.56 (0.81) | 2.42 (0.85) | 0 .001 |
| 23. How satisfied are you with the conditions of your living place? | 3.57 (1.11) | 3.56 (1.05) | 3.58 (1.16) | 0.17 | 3.56 (0.73) | 3.55 (0.61) | 0.98 |
| 24. How satisfied are you with your access to health services? | 4.16 (0.48) | 4.16 (1.17) | 4.15 (1.18) | 0.13 | 4.15 (0.46) | 4.25 (0.75) | 0.36 |
| 25. How satisfied are you with your transport? | 3.67 (0.97) | 3.45 (0.99) | 3.88 (0.97) | 0.00 | 3.79 (0.72) | 3.86 (0.78) | 0.61 |
| 28. Are you usually able to get the things you like to eat? | 3.63 (0.74) | 3.28 (0.63) | 3.97 (0.88) | 0.00 | 3.91 (0.59) | 3.99 (0.64) | 0.84 |
| Quality of Life | |||||
|---|---|---|---|---|---|
| Variable | Mean (SD) | β | SE | Wald χ2 | p-Value |
| Intercept | 57.40 | 1.56 | 273.98 | <0.001 | |
| Group (EG vs. CG) | 3.45 | 2.39 | 25.46 | 0.142 | |
| Time overall (T1 vs. T0) | −1.21 | 1.01 | 28.39 | 0.113 | |
| EG at T1 | 60.58 (1.15) | ||||
| EG at T0 | 49.77 (1.73) | ||||
| CG at T1 | 50.11 (1.26) | ||||
| CG at T0 | 49.97 (1.79) | ||||
| EG at T1 vs. EG at T0 | 10.81 (1.10) | <0.001 | |||
| CG at T1 vs. CG at T0 | 0.14 (0.02) | 0.601 | |||
| Time * Group overall | |||||
| EG * (T1 vs. T0) vs. CG * (T1 vs. T0) | 5.245 | 1.43 | 184.483 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.-Y.; Chan, H.-S. The Effect of Vocational Training on Visually Impaired People’s Quality of Life. Healthcare 2024, 12, 692. https://doi.org/10.3390/healthcare12060692
Chu H-Y, Chan H-S. The Effect of Vocational Training on Visually Impaired People’s Quality of Life. Healthcare. 2024; 12(6):692. https://doi.org/10.3390/healthcare12060692
Chicago/Turabian StyleChu, Hui-Ying, and Hui-Shan Chan. 2024. "The Effect of Vocational Training on Visually Impaired People’s Quality of Life" Healthcare 12, no. 6: 692. https://doi.org/10.3390/healthcare12060692
APA StyleChu, H.-Y., & Chan, H.-S. (2024). The Effect of Vocational Training on Visually Impaired People’s Quality of Life. Healthcare, 12(6), 692. https://doi.org/10.3390/healthcare12060692