
Effects of Telerehabilitation on Pain and Disability in Patients with Chronic Neck Pain: A Systematic Review and Meta-Analysis

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality of Included Studies
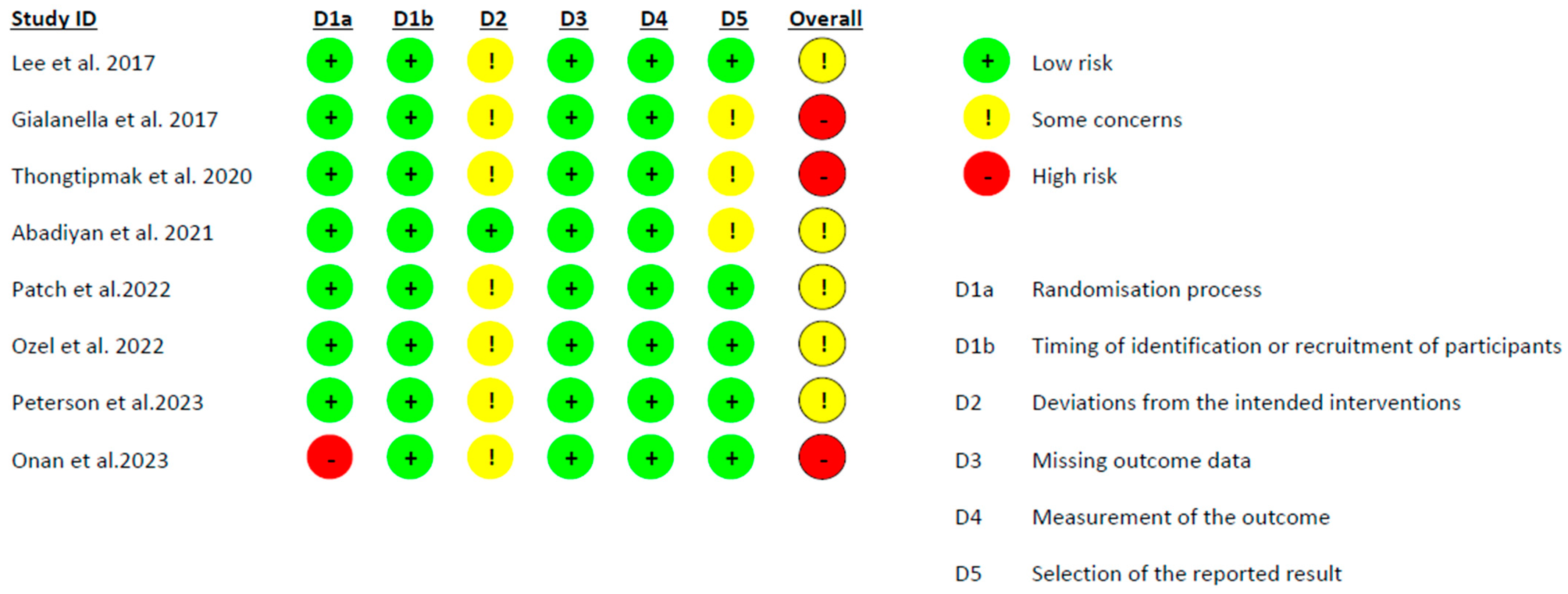
2.6. Risk of Bias of Included Studies
2.7. Statistical Analysis
3. Results
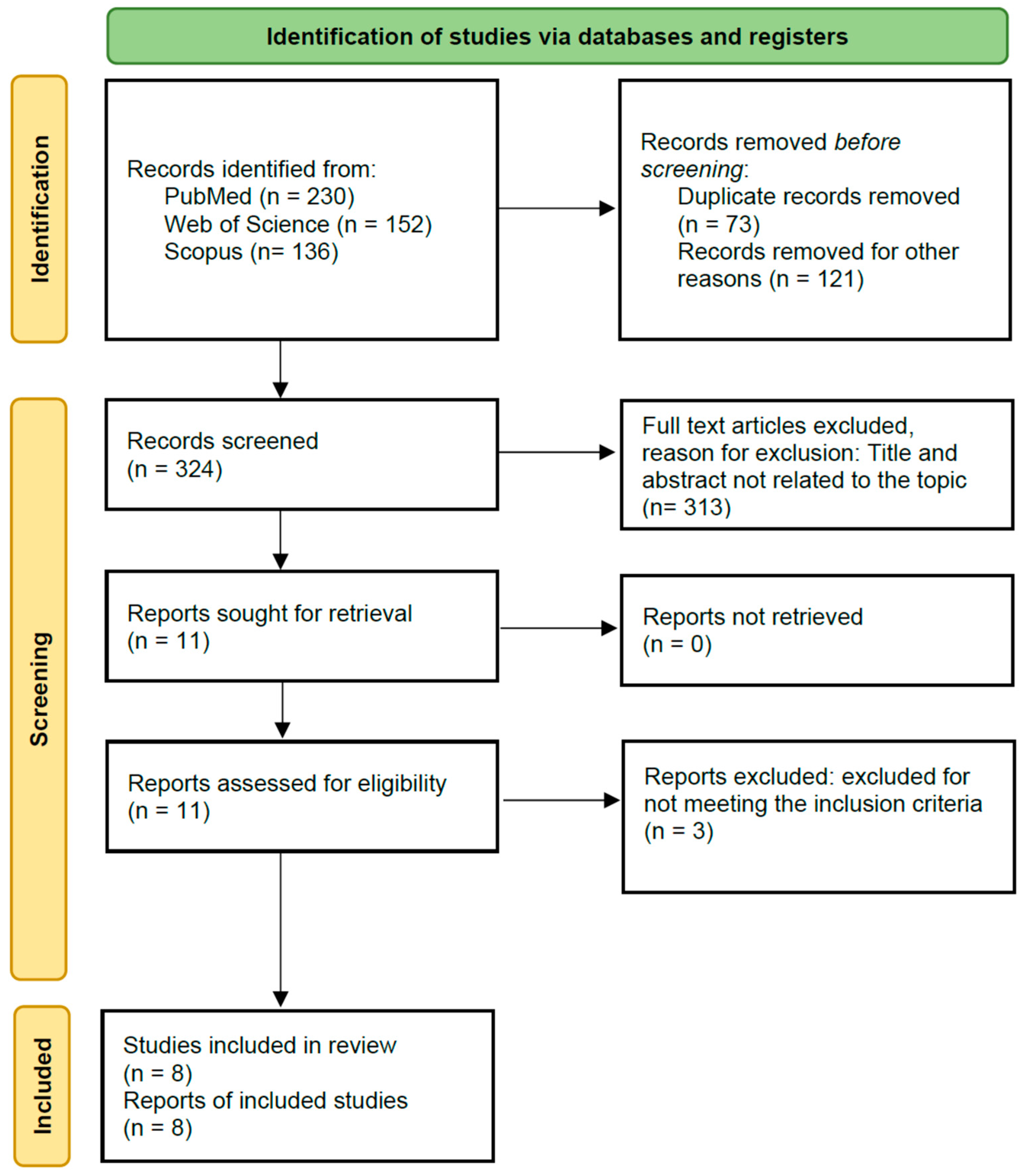
3.1. Search Selection
3.2. Characteristics of Studies
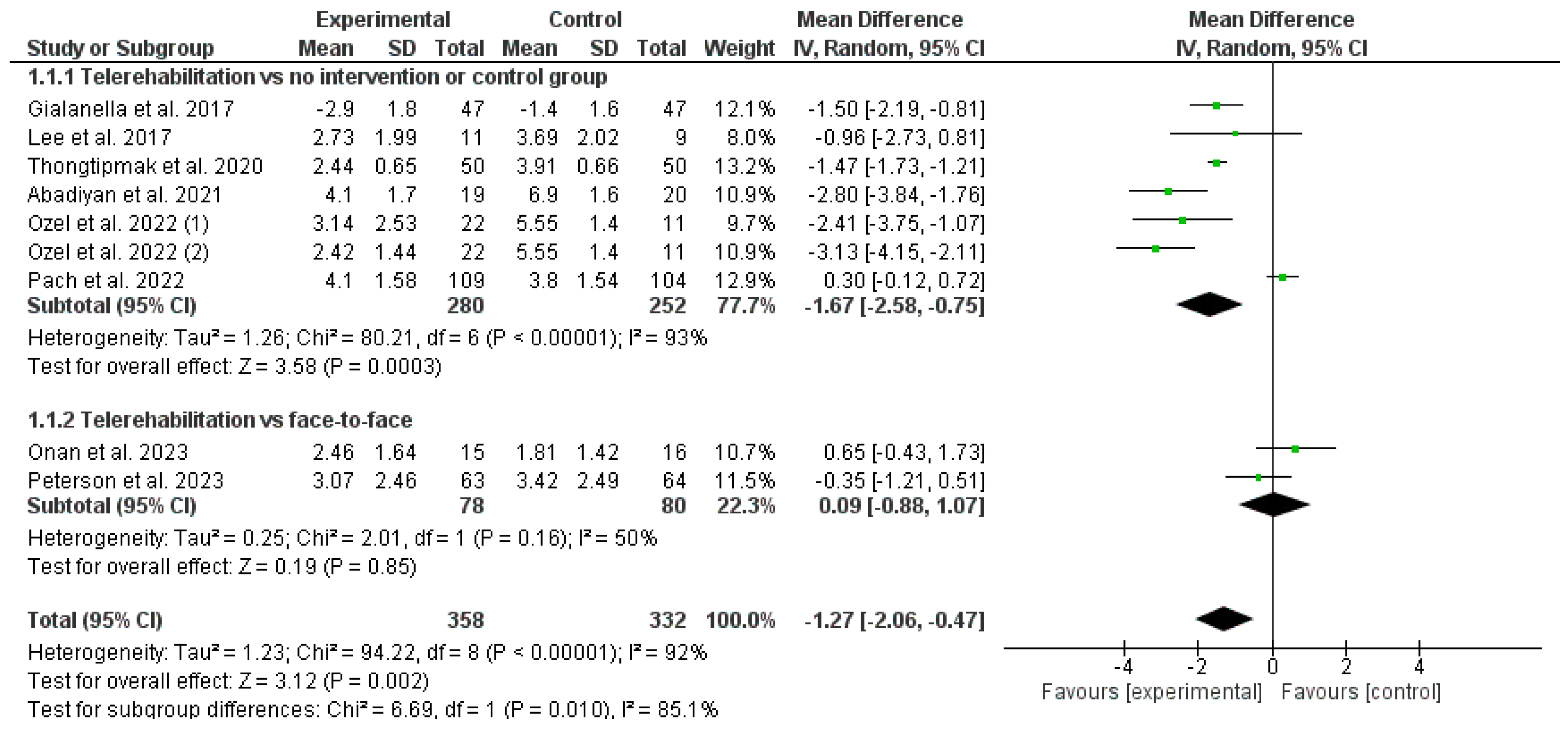
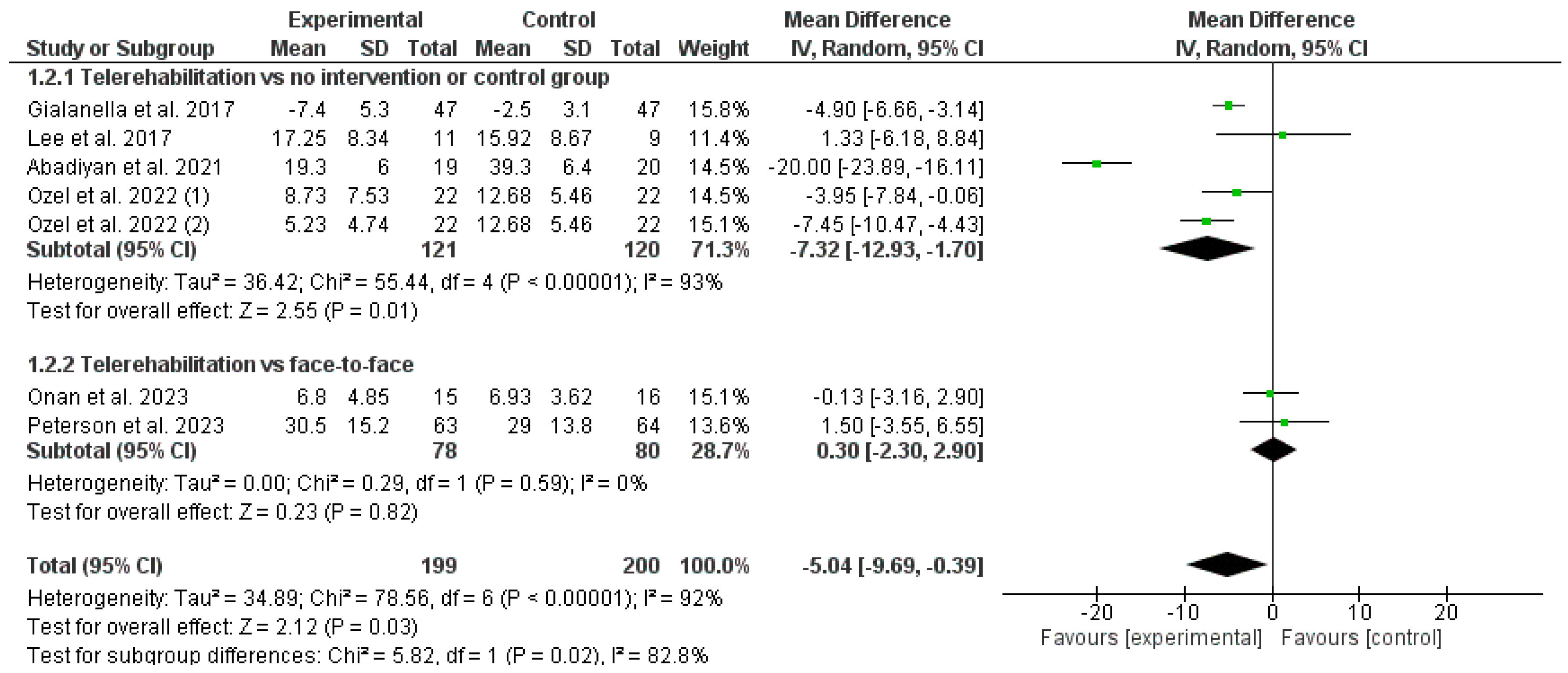
3.3. Results Obtained in Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 26. [Google Scholar] [CrossRef] [PubMed]
- Ris Hansen, I.; Barbero, M.; Falla, D.; Larsen, M.H.; Kraft, M.N.; Søgaard, K.; Juul-Kristensen, B. The relation between pain extent and quality-of-life, psychological factors and neck function in patients with chronic neck pain. Man. Ther. 2016, 25, e73–e74. [Google Scholar] [CrossRef]
- Asiri, F.; Reddy, R.S.; Tedla, J.S.; Al Mohiza, M.A.; Alshahrani, M.S.; Govindappa, S.C.; Sangadala, D.R. Kinesiophobia and its correlations with pain, proprioception, and functional performance among individuals with chronic neck pain. PLoS ONE 2021, 16, e0254262. [Google Scholar] [CrossRef] [PubMed]
- Arribas-Romano, A.; Fernández-Carnero, J.; González-Zamorano, Y.; Rodríguez-Lagos, L.; Gurdiel-Álvarez, F.; Molina-Álvarez, M.; Morales Tejera, D.; Mercado, F. Conditioned pain modulation and psychological factors in young adults with recurrent or chronic neck pain. Pain Pract. 2023, 24, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Farrell, S.F.; de Zoete, R.M.J.; Cabot, P.J.; Sterling, M. Systemic inflammatory markers in neck pain: A systematic review with meta-analysis. Eur. J. Pain 2020, 24, 1666–1686. [Google Scholar] [CrossRef] [PubMed]
- Ortego, G.; Lluch, E.; Herrero, P.; Boudreau, S.A.; Doménech-garcía, V. Profiling and Association over Time between Disability and Pain Features in Patients with Chronic Nonspecific Neck Pain: A Longitudinal Study. J. Clin. Med. 2022, 11, 1346. [Google Scholar] [CrossRef] [PubMed]
- Multanen, J.; Häkkinen, A.; Kautiainen, H.; Ylinen, J. Associations of neck muscle strength and cervical spine mobility with future neck pain and disability: A prospective 16-year study. BMC Musculoskelet. Disord. 2021, 22, 911. [Google Scholar] [CrossRef] [PubMed]
- Weigl, M.; Letzel, J.; Angst, F. Prognostic factors for the improvement of pain and disability following multidisciplinary rehabilitation in patients with chronic neck pain. BMC Musculoskelet. Disord. 2021, 22, 330. [Google Scholar] [CrossRef]
- Fejer, R.; Hartvigsen, J. Neck pain and disability due to neck pain: What is the relation? Eur. Spine J. 2008, 17, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Misailidou, V.; Malliou, P.; Beneka, A.; Karagiannidis, A.; Godolias, G. Assessment of patients with neck pain: A review of definitions, selection criteria, and measurement tools. J. Chiropr. Med. 2010, 9, 49–59. [Google Scholar] [CrossRef]
- Vernon, H. The Neck Disability Index: State-of-the-art, 1991–2008. J. Manip. Physiol. Ther. 2008, 31, 491–502. [Google Scholar] [CrossRef]
- Saltychev, M.; Mattie, R.; McCormick, Z.; Laimi, K. Psychometric properties of the neck disability index amongst patients with chronic neck pain using item response theory. Disabil. Rehabil. 2018, 40, 2116–2121. [Google Scholar] [CrossRef] [PubMed]
- Mahtta, D.; Daher, M.; Lee, M.T.; Sayani, S.; Shishehbor, M.; Virani, S.S. Promise and Perils of Telehealth in the Current Era. Curr. Cardiol. Rep. 2021, 23, 115. [Google Scholar] [CrossRef] [PubMed]
- Shachar, C.; Engel, J.; Elwyn, G. Implications for Telehealth in a Postpandemic Future: Regulatory and Privacy Issues. JAMA J. Am. Med. Assoc. 2020, 323, 2375–2376. [Google Scholar] [CrossRef] [PubMed]
- Perimal-Lewis, L.; Williams, P.A.H.; Mudd, G.; Gunasekara, G. Virtual care: The future for telehealth. Telehealth Innov. Remote Healthc. Serv. Deliv. Glob. Telehealth 2021, 277, 106–113. [Google Scholar] [CrossRef]
- Haque, S.N. Telehealth beyond COVID-19. Psychiatr. Serv. 2021, 72, 100–103. [Google Scholar] [CrossRef] [PubMed]
- de Araújo Vieira, L.M.S.M.; de Andrade, M.A.; de Oliveira Sato, T. Telerehabilitation for musculoskeletal pain—An overview of systematic reviews. Digit. Health 2023, 9, 20552076231164242. [Google Scholar] [CrossRef]
- Seron, P.; Oliveros, M.J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef] [PubMed]
- Timurtaş, E.; Selçuk, H.; Uğur Canöz, E.; Inceer, M.; Batar, S.; Demirbüken, İ.; Polat, M.G. Synchronous and asynchronous telerehabilitation methods produce similar benefits in individuals with non-specific neck pain. Arch. Orthop. Trauma Surg. 2024, 144, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Updated March 2011; The Cochrane Collaboration: London, UK, 2015; Available online: www.cochrane-handbook.org (accessed on 14 October 2023).
- Gialanella, B.; Ettori, T.; Faustini, S.; Baratti, D.; Bernocchi, P.; Comini, L.; Scalvini, S. Home-Based Telemedicine in Patients with Chronic Neck Pain. Am. J. Phys. Med. Rehabil. 2017, 96, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, M.; Lim, T.; Kim, T.; Kim, S.; Suh, D.; Lee, S.; Yoon, B. Effectiveness of an application-based neck exercise as a pain management tool for office workers with chronic neck pain and functional disability: A pilot randomized trial. Eur. J. Integr. Med. 2017, 12, 87–92. [Google Scholar] [CrossRef]
- Thongtipmak, S.; Buranruk, O.; Eungpinichpong, W.; Konharn, K. Immediate Effects and Acceptability of an Application-Based Stretching Exercise Incorporating Deep Slow Breathing for Neck Pain Self-management. Healthc. Inform. Res. 2020, 26, 50–60. [Google Scholar] [CrossRef]
- Abadiyan, F.; Hadadnezhad, M.; Khosrokiani, Z.; Letafatkar, A.; Akhshik, H. Adding a smartphone app to global postural re-education to improve neck pain, posture, quality of life, and endurance in people with nonspecific neck pain: A randomized controlled trial. Trials 2021, 22, 274. [Google Scholar] [CrossRef] [PubMed]
- Özel, M.; Kaya Ciddi, P. The effectiveness of telerehabilitation-based structured exercise therapy for chronic nonspecific neck pain: A randomized controlled trial. J. Telemed. Telecare 2022, 1357633X221095782. [Google Scholar] [CrossRef] [PubMed]
- Pach, D.; Blödt, S.; Wang, J.; Keller, T.; Bergmann, B.; Rogge, A.A.; Barth, J.; Icke, K.; Roll, S.; Witt, C.M. App-Based Relaxation Exercises for Patients with Chronic Neck Pain: Pragmatic Randomized Trial. JMIR mHealth uHealth 2022, 10, e31482. [Google Scholar] [CrossRef] [PubMed]
- Onan, D.; Ulger, O.; Martelletti, P. Effects of spinal stabilization exercises delivered using telerehabilitation on outcomes in patients with chronic neck pain: A randomized controlled trial. Expert Rev. Neurother. 2023, 23, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Peterson, G.; Peolsson, A. Efficacy of Neck-Specific Exercise With Internet Support Versus Neck-Specific Exercise at a Physiotherapy Clinic in Chronic Whiplash-Associated Disorders: Multicenter Randomized Controlled Noninferiority Trial. J. Med. Internet Res. 2023, 25, e43888. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef] [PubMed]
- Saunders, L.D.; Soomro, G.M.; Buckingham, J.; Jamtvedt, G.; Raina, P. Assessing the methodological quality of nonrandomized intervention studies. West. J. Nurs. Res. 2003, 25, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, J.K.F.; Weeks, L.; Sterneet, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Dwan, K.; Kirkham, J.; Paton, R.W.; Morley, E.; Newton, A.W.; Perry, D.C. Splinting for the non-operative management of developmental dysplasia of the hip (DDH) in children under six months of age. Cochrane Database Syst. Rev. 2022, 10, CD012717. [Google Scholar] [CrossRef] [PubMed]
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ligero, M.; Moral-Munoz, J.A.; Salazar, A.; Failde, I. mHealth Intervention for Improving Pain, Quality of Life, and Functional Disability in Patients with Chronic Pain: Systematic Review. JMIR mHealth uHealth 2023, 11, e40844. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, A.C.; Uddin, R.; Schröder-Pfeifer, P.; Holl, F.; Swoboda, W.; Schiltenwolf, M. Mobile application-based interventions for chronic pain patients: A systematic review and meta-analysis of effectiveness. J. Clin. Med. 2020, 9, 3557. [Google Scholar] [CrossRef] [PubMed]
- Isernia, S.; Pagliari, C.; Morici, N.; Toccafondi, A.; Banfi, P.I.; Rossetto, F.; Borgnis, F.; Tavanelli, M.; Brambilla, L.; Baglio, F. Telerehabilitation Approaches for People with Chronic Heart Failure: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 64. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.; Bruning, J.; Morris, N.; Mandrusiak, A.; Russell, T. A systematic review of the effects of telerehabilitation in patients with cardiopulmonary diseases. J. Cardiopulm. Rehabil. Prev. 2015, 35, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.Y.L.; Wong, A.K.C.; Hung, T.T.M.; Yan, J.; Yang, S. Nurse-led Telehealth Intervention for Rehabilitation (Telerehabilitation) Among Community-Dwelling Patients With Chronic Diseases: Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e40364. [Google Scholar] [CrossRef] [PubMed]
- Tchero, H.; Teguo, M.T.; Lannuzel, A.; Rusch, E. Telerehabilitation for stroke survivors: Systematic review and meta-analysis. J. Med. Internet Res. 2018, 20, e10867. [Google Scholar] [CrossRef] [PubMed]
- Lara-Palomo, I.C.; Gil-Martínez, E.; Ramírez-García, J.D.; Capel-Alcaraz, A.M.; García-López, H.; Castro-Sánchez, A.M.; Antequera-Soler, E. Efficacy of e-Health Interventions in Patients with Chronic Low-Back Pain: A Systematic Review with Meta-Analysis. Telemed. e-Health 2022, 28, 1734–1752. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Q.; Long, Y.; Peng, W.J.; Gong, C.; Liu, Y.Q.; Peng, X.M.; Zhong, Y.B.; Luo, Y.; Wang, M.Y. The Efficacy and Safety of Telerehabilitation for Fibromyalgia: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2023, 25, e42090. [Google Scholar] [CrossRef] [PubMed]
- Niknejad, N.; Ismail, W.; Bahari, M.; Nazari, B. Understanding Telerehabilitation Technology to Evaluate Stakeholders’ Adoption of Telerehabilitation Services: A Systematic Literature Review and Directions for Further Research. Arch. Phys. Med. Rehabil. 2021, 102, 1390–1403. [Google Scholar] [CrossRef] [PubMed]
- Pramuka, M.; Van Roosmalen, L. Telerehabilitation Technologies: Accessibility and Usability. Int. J. Telerehabil. 2009, 1, 85. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B.; Galea, M.P.; Kesselring, J.; Khan, F. Effectiveness of telerehabilitation interventions in persons with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2015, 4, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Moulaei, K.; Sheikhtaheri, A.; Nezhad, M.S.; Haghdoost, A.A.; Gheysari, M.; Bahaadinbeigy, K. Telerehabilitation for upper limb disabilities: A scoping review on functions, outcomes, and evaluation methods. Arch. Public Health 2022, 80, 196. [Google Scholar] [CrossRef] [PubMed]
- Appleby, E.; Gill, S.T.; Hayes, L.K.; Walker, T.L.; Walsh, M.; Kumar, S. Effectiveness of telerehabilitation in the management of adults with stroke: A systematic review. PLoS ONE 2019, 14, e0225150. [Google Scholar] [CrossRef] [PubMed]
- Hailey, D.; Roine, R.; Ohinmaa, A.; Dennett, L. Evidence of benefit from telerehabilitation in routine care: A systematic review. J. Telemed. Telecare 2011, 17, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.M.; Dhakal, R.; Halpin, S.J.; Hariharan, R.; O’Connor, R.J.; Allsop, M.; Sivan, M. Telerehabilitation for individuals with spinal cord injury in low-and middle-income countries: A systematic review of the literature. Spinal Cord 2022, 60, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, W.; Groen, W.G.; Aaronson, N.K.; Van Harten, W.H. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: Relevance for cancer survivors. J. Med. Internet Res. 2013, 15, e2281. [Google Scholar] [CrossRef] [PubMed]
- Gregersen, T.L.; Green, A.; Frausing, E.; Ringbæk, T.; Brøndum, E.; Ulrik, C.S. Do telemedical interventions improve quality of life in patients with COPD? A systematic review. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 809–822. [Google Scholar] [CrossRef]
- de Moraes, É.B.; Santos Garcia, J.B.; de Macedo Antunes, J.; Daher, D.V.; Seixas, F.L.; Muniz Ferrari, M.F. Chronic Pain Management during the COVID-19 Pandemic: A Scoping Review. Pain Manag. Nurs. 2021, 22, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Emerick, T.; Alter, B.; Jarquin, S.; Brancolini, S.; Bernstein, C.; Luong, K.; Morrisseyand, S.; Wasan, A. Telemedicine for Chronic Pain in the COVID-19 Era and beyond. Pain Med. 2020, 21, 1743–1748. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Nalamasu, R.; Pergolizzi, J.V.; Gharibo, C. Pain Management during the COVID-19 Pandemic. Pain Ther. 2020, 9, 453–466. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Study Design/Groups | Sample Size per Group n (% Women) | Age Years Mean ± SD | Duration of Pain Months Mean ± SD | Pain Intensity Mean (0–10) ± SD | Downs and Black Score |
|---|---|---|---|---|---|---|
| Gialanella et al. (2017) [22] | RCT/2 Groups | TG: 47 (89.3) CG: 47 (89.3) | TG: 56.0 ± 14.0 CG: 60.1 ± 11.0 | NR | TG: 6.8 ± 1.3 CG: 6.6 ± 1.5 | 23 |
| Lee et al. (2017) [23] | Pilot RCT/2 Groups | TG: 11 (55) CG: 9 (45) | TG: 27.09 ± 4.83 CG: 27.56 ± 4.67 | TG: 50.81 ± 71.72 CG: 35.33 ± 18.11 | TG: 5.20 ± 2.19 CG: 4.02 ± 1.75 | 16 |
| Thongtipmak et al. (2020) [24] | RCT/2 Groups | TG: 50 (82) CG: 50 (76) | TG: 22.86 ± 1.99 CG: 22.68 ± 2.23 | NR | TG: 3.97 ± 0.74 CG: 4.06 ± 0.68 | 18 |
| Abadiyan et al. (2021) [25] | RCT/3 Groups | TG: 20 (50) CG: 20 (50) | TG: 41.3 ± 8.1 CG: 37.4 ± 9.8 | NR | TG: 7.3 ± 0.9 CG: 6.4 ± 1.8 | 21 |
| Ozel et al. (2022) [26] | RTC/3 Groups | TG1: 22 (72.7) TG2: 22 (77.3) CG: 22 (59.1) | TG1: 36.23 ± 12.45 TG2: 34.18 ± 13.03 CG: 39.2 7 ± 15.46 | NR | TG1: 6.77 TG2: 4.86 CG: 5.55 | 18 |
| Pach et al. (2022) [27] | RTC/2 Groups | TG: 110 (67.3) CG: 110 (71.8) | TG: 37.9 ± 11 CG: 39.8 ± 11.6 | TG: 79.2 ± 74.8 CG: 86.4 ± 97.7 | TG: 5.7 ± 1.4 CG: 5.8 ± 1.3 | 20 |
| Onan et al. (2023) [28] | RCT/2 Groups | TG: 15 (73.3) CG: 16 (68.7) | TG: 37.4 ± 10.58 CG: 39.5 ± 10.96 | TG: 36 CG: 60 | TG: 7.13 ± 1.92 CG: 6.75 ± 1.98 | 16 |
| Peterson et al. (2023) [29] | RTC/2 Groups | TG: 70 (79) CG: 70 (79) | TG: 40.4 ± 11.6 CG: 40.5 ± 11.4 | TG: 27.4 ± 21.0 CG: 25.2 ± 15.5 | TG: 5.77 ± 1.87 CG: 5.86 ± 1.70 | 19 |
| Study (Year) | Experimental Intervention Design and Support | Telerehabilitation Components | Intervention Duration and Frequency Weeks Days/Week | Telehealth Setting, and Supervision | Comparator Group | Main Results |
|---|---|---|---|---|---|---|
| Gialanella et al. (2017) [22] | Telerehabilitation isolated via phone calls | -Education content -Symptom and mood monitoring -Physical activity monitoring and personalized feedback -Education in self-management skills -Tele-consultation with healthcare professionals -Remote decision support system -Therapeutic exercise program | 24 w 5 d/w 20 min | Home Fortnightly scheduled phone calls | Exercise recommendation | Pain (VAS): TG ** > CG ** (p < 0.001) Disability (NDI): TG ** > CG ** (p < 0.001) |
| Lee et al. (2017) [23] | Telerehabilitation isolated via smartphone app + phone calls | -Education content -Symptom and mood monitoring -Physical activity monitoring and personalized feedback -Therapeutic exercise program | 8 w 2 d/w 10–15 min | Work setting Supervised | Brochure to correct the posture | Pain (VAS): TG * > CG (p < 0.05) Disability (NDI): TG * > CG (p < 0.05) Fear-avoidance belief (FABQ): -Physical activity: TG vs. CG (NSD) -Work: TG vs. CG * (p < 0.05) -Health-related quality of life (SF-36): TG vs. CG (NSD) |
| Thongtipmak et al. (2020) [24] | Telerehabilitation isolated via a smartphone app | -Education content -Symptom and mood monitoring -Tele-education in self-management skills -Therapeutic exercise program | 15–20 min | Home Supervised | No intervention | Pain (VAS): TG ** > CG * (p < 0.001) |
| Abadiyan et al. (2021) [25] | Telerehabilitation via smartphone app combined with a presential exercise program | -Physical activity monitoring and personalized feedback -Therapeutic exercise program | 8 w 4 d/w 50 min | Home Supervised | Usual care | TG-CG Pain (VAS): TG > CG *; p < 0031 Disability (NDI): TG vs. CG (NSD) Quality of life (SF-36): TG > CG *; p < 0.001 |
| Ozel et al. (2022) [26] | Telerehabilitation via videoconference | -Physical activity monitoring and personalized feedback -Education in self-management skills -Tele-consultation with healthcare professionals -Therapeutic exercise program | 4 w 4 d/w 20 min | Home Bi-weekly individual online sessions | No intervention | TG1 vs. CG: Pain (VAS): TG1 ** > CG (p < 0.001) Disability (NDI): TG1 ** vs. CG (NSD) TG2 vs. CG: Pain (VAS): TG2 ** > CG (p < 0.001) Disability (NDI): TG2 ** > CG (p < 0.001) |
| Pach et al. (2022) [27] | Telerehabilitation via smartphone app | -Symptom and mood monitoring -Education in self-management skills -Therapeutic exercise program | 7 d/w 15 min | Home Supervised | Usual care and app for data entry only | Pain intensity (NRS): TG ** > CG (p < 0.05) Neck Disability (NDI): TG ** vs. CG (NSD) General and physical health (WHOQOL-BREF): TG ** vs. CG (NSD) |
| Onan et al. (2023) [28] | Telerehabilitation via videoconference | -Physical activity monitoring and personalized feedback -Tele-consultation with healthcare professionals -Therapeutic exercise program | 8 w 3 d/w 45 min | Home Supervised | Supervised presential exercises | Pain (VAS): TG vs. CG (NSD) Neck Disability (NDI): TG vs. CG (NSD) |
| Peterson et al. (2023) [29] | Telerehabilitation via videoconference | -Physical activity monitoring and personalized feedback -Education in self-management skills -Therapeutic exercise program | 4 w 4 d/w 20 min | Home Unsupervised | Supervised presential exercises | Pain (NRS): TG ** > CG (NSD) Neck Disability (NDI): TG ** > CG (NSD) General and physical health status (WHOQOL-BREF): TG ** vs. CG (NSD) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenza-Peña, G.; Calvache-Mateo, A.; Valenza, M.C.; Granados-Santiago, M.; Raya-Benítez, J.; Cabrera-Martos, I.; Díaz-Mohedo, E. Effects of Telerehabilitation on Pain and Disability in Patients with Chronic Neck Pain: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 796. https://doi.org/10.3390/healthcare12070796
Valenza-Peña G, Calvache-Mateo A, Valenza MC, Granados-Santiago M, Raya-Benítez J, Cabrera-Martos I, Díaz-Mohedo E. Effects of Telerehabilitation on Pain and Disability in Patients with Chronic Neck Pain: A Systematic Review and Meta-Analysis. Healthcare. 2024; 12(7):796. https://doi.org/10.3390/healthcare12070796
Chicago/Turabian StyleValenza-Peña, Geraldine, Andrés Calvache-Mateo, Marie Carmen Valenza, María Granados-Santiago, Julia Raya-Benítez, Irene Cabrera-Martos, and Esther Díaz-Mohedo. 2024. "Effects of Telerehabilitation on Pain and Disability in Patients with Chronic Neck Pain: A Systematic Review and Meta-Analysis" Healthcare 12, no. 7: 796. https://doi.org/10.3390/healthcare12070796
APA StyleValenza-Peña, G., Calvache-Mateo, A., Valenza, M. C., Granados-Santiago, M., Raya-Benítez, J., Cabrera-Martos, I., & Díaz-Mohedo, E. (2024). Effects of Telerehabilitation on Pain and Disability in Patients with Chronic Neck Pain: A Systematic Review and Meta-Analysis. Healthcare, 12(7), 796. https://doi.org/10.3390/healthcare12070796