

Exploring Early, Middle, and Late Loss in Basic Activities of Daily Living among Nursing Home Residents: A Multicenter Observational Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
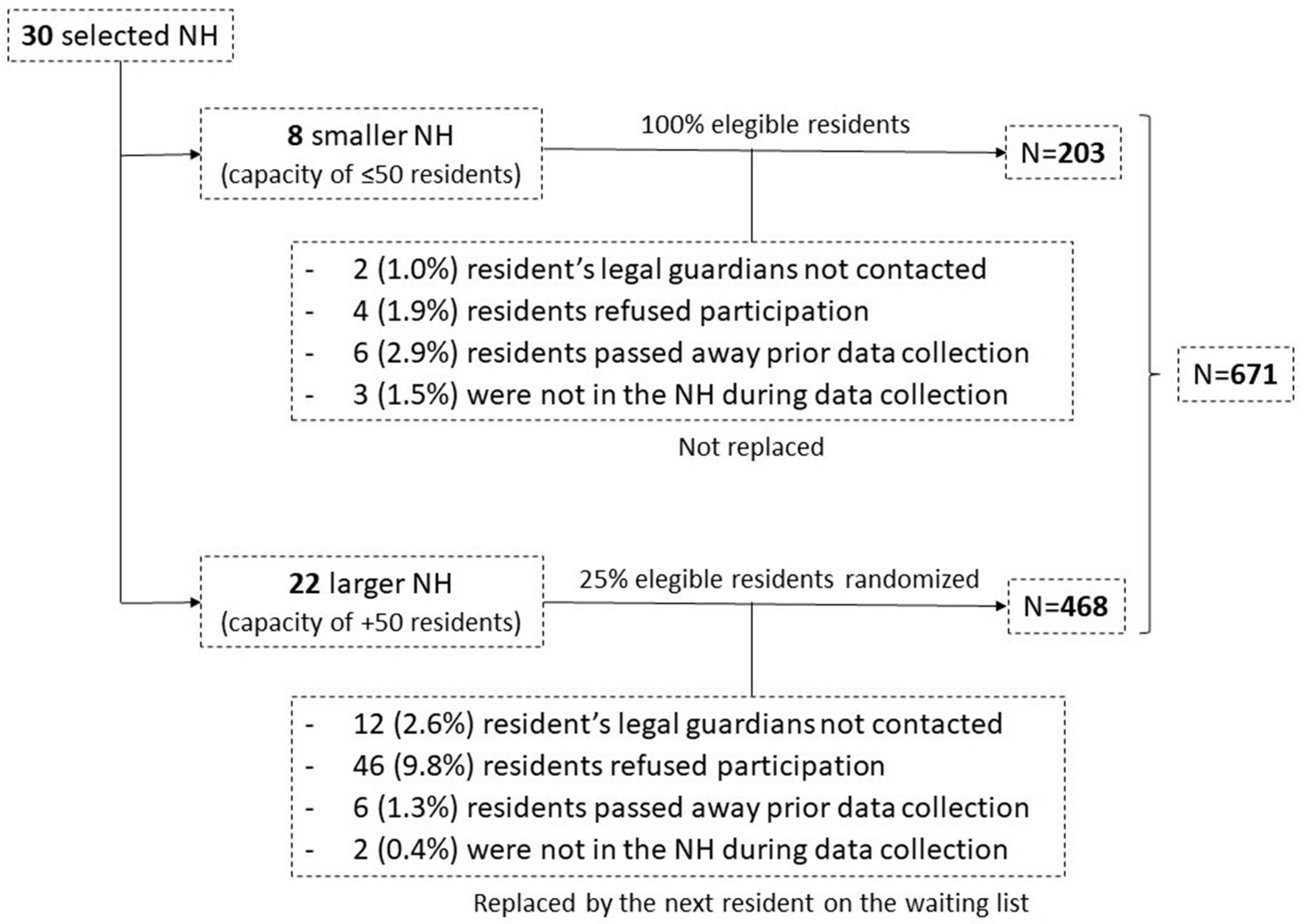
2.2. Sample
2.3. Study Procedures
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Sample Characteristics
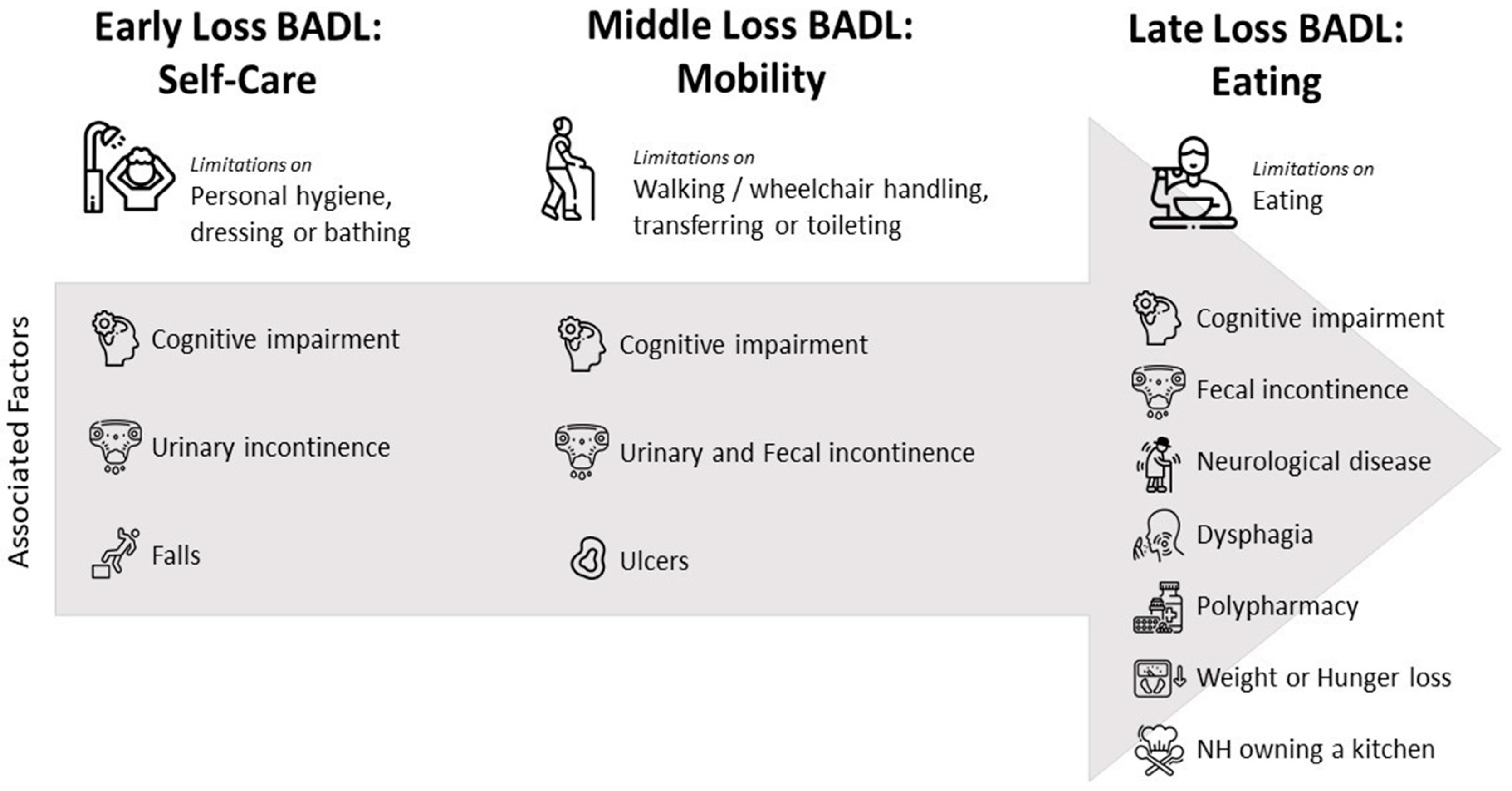
3.2. Factors Associated with Early-Loss BADLs: Self-Care
3.3. Factors Influencing Middle-Loss BADLs: Mobility
3.4. Factors Related to the Late-Loss BADL: Eating
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontologist 2015, 55, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing Populations: The Challenges Ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.R. An International Perspective on Long Term Care: Focus on Nursing Homes. J. Am. Med. Dir. Assoc. 2011, 12, 487–492.e1. [Google Scholar] [CrossRef] [PubMed]
- Gaugler, J.E.; Duval, S.; Anderson, K.A.; Kane, R.L. Predicting Nursing Home Admission in the U.S: A Meta-Analysis. BMC Geriatr. 2007, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Reuben, D.B.; Solomon, D.H. Assessment in Geriatrics. Of Caveats and Names. J. Am. Geriatr. Soc. 1989, 37, 570–572. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Martin, P.; Jerez-Roig, J.; Rierola-Fochs, S.; Oliveira, V.R.; Farrés-Godayol, P.; Bezerra de Souza, D.L.; Giné-Garriga, M.; Booth, J.; Skelton, D.A.; Minobes-Molina, E. Incidence and Predictive Factors of Functional Decline in Older People Living in Nursing Homes: A Systematic Review. J. Am. Med. Dir. Assoc. 2022, 23, 1815–1825.e9. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.K.; Wittrup-Jensen, K.U.; Lolk, A.; Andersen, K.; Kragh-Sørensen, P. Ability to Perform Activities of Daily Living Is the Main Factor Affecting Quality of Life in Patients with Dementia. Health Qual. Life Outcomes 2004, 2, 52. [Google Scholar] [CrossRef] [PubMed]
- Kruse, R.L.; Petroski, G.F.; Mehr, D.R.; Banaszak-Holl, J.; Intrator, O. Activity of Daily Living Trajectories Surrounding Acute Hospitalization of Long-Stay Nursing Home Residents. J. Am. Geriatr. Soc. 2013, 61, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- de Meijer, C.A.M.; Koopmanschap, M.A.; Koolman, X.H.E.; van Doorslaer, E.K.A. The Role of Disability in Explaining Long-Term Care Utilization. Med. Care 2009, 47, 1156–1163. [Google Scholar] [CrossRef]
- Yeh, K.-P.; Lin, M.-H.; Liu, L.-K.; Chen, L.-Y.; Peng, L.-N.; Chen, L.-K. Functional Decline and Mortality in Long-Term Care Settings: Static and Dynamic Approach. J. Clin. Gerontol. Geriatr. 2014, 5, 13–17. [Google Scholar] [CrossRef]
- Cornelis, E.; Gorus, E.; Van Schelvergem, N.; De Vriendt, P. The Relationship between Basic, Instrumental, and Advanced Activities of Daily Living and Executive Functioning in Geriatric Patients with Neurocognitive Disorders. Int. J. Geriatr. Psychiatry 2019, 34, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Levy, C.R.; Zargoush, M.; Williams, A.E.; Williams, A.R.; Giang, P.; Wojtusiak, J.; Kheirbek, R.E.; Alemi, F. Sequence of Functional Loss and Recovery in Nursing Homes. Gerontologist 2016, 56, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. the index of adl: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Gerrard, P. The Hierarchy of the Activities of Daily Living in the Katz Index in Residents of Skilled Nursing Facilities. J. Geriatr. Phys. Ther. 2013, 36, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs within the MDS. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M546–M553. [Google Scholar] [CrossRef]
- Jerez-Roig, J.; de Brito Macedo Ferreira, L.M.; Torres de Araújo, J.R.; Costa Lima, K. Dynamics of Activities of Daily Living Performance in Institutionalized Older Adults: A Two-Year Longitudinal Study. Disabil. Health J. 2017, 10, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Menegazzi, G.; Tullio, A.; Zigotti Fuso, M.; Hayter, M.; Watson, R. Functional Decline in Residents Living in Nursing Homes: A Systematic Review of the Literature. J. Am. Med. Dir. Assoc. 2016, 17, 694–705. [Google Scholar] [CrossRef] [PubMed]
- Kingston, A.; Collerton, J.; Davies, K.; Bond, J.; Robinson, L.; Jagger, C. Losing the Ability in Activities of Daily Living in the Oldest Old: A Hierarchic Disability Scale from the Newcastle 85+ Study. PLoS ONE 2012, 7, e31665. [Google Scholar] [CrossRef] [PubMed]
- Delva, F.; Edjolo, A.; Peres, K.; Berr, C.; Barberger-Gateau, P.; Dartigues, J.F. Hierarchical Structure of the Activities of Daily Living Scale in Dementia. J. Nutr. Health Aging 2014, 18, 698–704. [Google Scholar] [CrossRef]
- Sun, Q.; Jiang, N.; Lu, N.; Lou, V.W.Q. Bidirectional Relationship between Cognitive Function and Loss Hierarchy of Activities of Daily Living among Older Adults with Disabilities in Urban China: A Cross-Lagged Analysis. BMJ Open 2022, 12, e057211. [Google Scholar] [CrossRef]
- Brown, R.T.; Diaz-Ramirez, L.G.; Boscardin, W.J.; Cappola, A.R.; Lee, S.J.; Steinman, M.A. Changes in the Hierarchy of Functional Impairment From Middle Age to Older Age. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 1577–1584. [Google Scholar] [CrossRef]
- Watson, R.; Palese, A.; Zuttion, R.; Ferrario, B.; Ponta, S.; Hayter, M. Identifying Longitudinal Sustainable Hierarchies in Activities of Daily Living. Arch. Gerontol. Geriatr. 2017, 71, 122–128. [Google Scholar] [CrossRef]
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 7 July 2023).
- Amblàs-Novellas, J.; Coll-Planas, L.; Jerez-Roig, J.; López, D.; Martori, J.C.; Ramon-Aribau, A.; Comas-Herrera, A.; Moreno-Martin, P.; Solé-Casals, M.; Máiz-Mazuela, C.; et al. Evaluation of the Impact of the COVID-19 Pandemic on People and Organisations in Long-Term Care Facilities of Catalonia and Proposals for Improving the Care Model: The Resicovid-19 Project. J. Long-Term Care 2024, 1–13. [Google Scholar] [CrossRef]
- STROBE. STROBE. Available online: https://www.strobe-statement.org/ (accessed on 31 October 2023).
- Shah, S.; Vanclay, F.; Cooper, B. Improving the Sensitivity of the Barthel Index for Stroke Rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Schulc, E.; Pallauf, M.; Mueller, G.; Wildbahner, T.; Them, C. Is the Barthel Index an Adequate Assessment Tool for Identifying a Risk Group in Elderly People Living at Home? Int. J. Nurs. Clin. Pract. 2015, 2, 140. [Google Scholar] [CrossRef]
- Amblàs-Novellas, J.; Martori, J.C.; Espaulella, J.; Oller, R.; Molist-Brunet, N.; Inzitari, M.; Romero-Ortuno, R. Frail-VIG Index: A Concise Frailty Evaluation Tool for Rapid Geriatric Assessment. BMC Geriatr. 2018, 18, 29. [Google Scholar] [CrossRef] [PubMed]
- Aprahamian, I.; Cezar, N.O.dC.; Izbicki, R.; Lin, S.M.; Paulo, D.L.V.; Fattori, A.; Biella, M.M.; Jacob Filho, W.; Yassuda, M.S. Screening for Frailty with the FRAIL Scale: A Comparison With the Phenotype Criteria. J. Am. Med. Dir. Assoc. 2017, 18, 592–596. [Google Scholar] [CrossRef]
- Reisberg, B.; Ferris, S.H.; De Leon, M.J.; Crook, T. The Global Deterioration Scale for Assessment of Primary Degenerative Dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [CrossRef]
- Klusch, L. The MDS 3.0 and Its Impact on Bladder and Bowel Care. Provider 2012, 38, 33, 35, 37. [Google Scholar]
- Liu, W.; Unick, J.; Galik, E.; Resnick, B. Barthel Index of Activities of Daily Living: Item Response Theory Analysis of Ratings for Long-Term Care Residents. Nurs. Res. 2015, 64, 88–99. [Google Scholar] [CrossRef]
- Lane, N.E.; Wodchis, W.P.; Boyd, C.M.; Stukel, T.A. Disability in Long-Term Care Residents Explained by Prevalent Geriatric Syndromes, Not Long-Term Care Home Characteristics: A Cross-Sectional Study. BMC Geriatr. 2017, 17, 49. [Google Scholar] [CrossRef] [PubMed]
- Lindbergh, C.A.; Dishman, R.K.; Miller, L.S. Functional Disability in Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Neuropsychol. Rev. 2016, 26, 129–159. [Google Scholar] [CrossRef] [PubMed]
- Musa, M.K.; Saga, S.; Blekken, L.E.; Harris, R.; Goodman, C.; Norton, C. The Prevalence, Incidence, and Correlates of Fecal Incontinence Among Older People Residing in Care Homes: A Systematic Review. J. Am. Med. Dir. Assoc. 2019, 20, 956–962.e8. [Google Scholar] [CrossRef] [PubMed]
- Jerez-Roig, J.; Souza, D.L.B.; Amaral, F.L.J.S.; Lima, K.C. Prevalence of Fecal Incontinence (FI) and Associated Factors in Institutionalized Older Adults. Arch. Gerontol. Geriatr. 2015, 60, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Offermans, M.P.W.; Du Moulin, M.F.M.T.; Hamers, J.P.H.; Dassen, T.; Halfens, R.J.G. Prevalence of Urinary Incontinence and Associated Risk Factors in Nursing Home Residents: A Systematic Review. Neurourol. Urodyn. 2009, 28, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Olagundoye, O.; Odusanya, B.; Kung, J.Y.; Gibson, W.; Wagg, A. A Scoping Review of Risk Factors for Urinary Incontinence in Older Men. BMC Geriatr. 2023, 23, 534. [Google Scholar] [CrossRef] [PubMed]
- Coll-Planas, L.; Denkinger, M.D.; Nikolaus, T. Relationship of Urinary Incontinence and Late-Life Disability: Implications for Clinical Work and Research in Geriatrics. Z. Gerontol. Geriatr. 2008, 41, 283–290. [Google Scholar] [CrossRef]
- Wang, J.; Kane, R.L.; Eberly, L.E.; Virnig, B.A.; Chang, L.-H. The Effects of Resident and Nursing Home Characteristics on Activities of Daily Living. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64A, 473–480. [Google Scholar] [CrossRef]
- Sze, T.W.; Leng, C.Y.; Lin, S.K.S. The Effectiveness of Physical Restraints in Reducing Falls among Adults in Acute Care Hospitals and Nursing Homes: A Systematic Review. JBI Evid. Synth. 2012, 10, 307. [Google Scholar] [CrossRef]
- Gulka, H.J.; Patel, V.; Arora, T.; McArthur, C.; Iaboni, A. Efficacy and Generalizability of Falls Prevention Interventions in Nursing Homes: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1024–1035.e4. [Google Scholar] [CrossRef]
- Coleman, S.; Gorecki, C.; Nelson, E.A.; Closs, S.J.; Defloor, T.; Halfens, R.; Farrin, A.; Brown, J.; Schoonhoven, L.; Nixon, J. Patient Risk Factors for Pressure Ulcer Development: Systematic Review. Int. J. Nurs. Stud. 2013, 50, 974–1003. [Google Scholar] [CrossRef] [PubMed]
- Hajhosseini, B.; Longaker, M.T.; Gurtner, G.C. Pressure Injury. Ann. Surg. 2020, 271, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.P.; Patricia, W.S. A Systematic Review of Economic Evaluations Assessing Interventions Aimed at Preventing or Treating Pressure Ulcers. Int. J. Nurs. Stud. 2015, 52, 769–788. [Google Scholar] [CrossRef] [PubMed]
- Amir, Y.; Lohrmann, C.; Halfens, R.J.; Schols, J.M. Pressure Ulcers in Four Indonesian Hospitals: Prevalence, Patient Characteristics, Ulcer Characteristics, Prevention and Treatment. Int. Wound J. 2016, 14, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Recio-Saucedo, A.; Dall’Ora, C.; Maruotti, A.; Ball, J.; Briggs, J.; Meredith, P.; Redfern, O.C.; Kovacs, C.; Prytherch, D.; Smith, G.B.; et al. What Impact Does Nursing Care Left Undone Have on Patient Outcomes? Review of the Literature. J. Clin. Nurs. 2018, 27, 2248–2259. [Google Scholar] [CrossRef] [PubMed]
- Francke, A.L.; Smit, M.C.; de Veer, A.J.; Mistiaen, P. Factors Influencing the Implementation of Clinical Guidelines for Health Care Professionals: A Systematic Meta-Review. BMC Med. Inf. Decis. Mak. 2008, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Bressan, V.; Hayter, M.; Watson, R. Enhancing Independent Eating among Older Adults with Dementia: A Scoping Review of the State of the Conceptual and Research Literature. BMC Nurs. 2020, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.-C.R.; Spencer, J.-C.; Ho, M.-H.; Kasa, A.S.; Ataiza, C.; Lambert, K.; Chang, C.-C. Effectiveness of Interventions on Feeding Difficulties among People with Dementia: A Systematic Review and Meta-Analysis. Australas. J. Ageing 2023, 42, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Grassetti, L.; Bandera, D.; Zuttion, R.; Ferrario, B.; Ponta, S.; Hayter, M.; Watson, R. High Feeding Dependence Prevalence in Residents Living in Italian Nursing Homes Requires New Policies: Findings from a Regionally Based Cross-Sectional Study. Health Policy 2018, 122, 301–308. [Google Scholar] [CrossRef]
- Chekani, F.; Bali, V.; Aparasu, R.R. Functional Status of Elderly Nursing Home Residents with Parkinson’s Disease. J. Park. Dis. 2016, 6, 617–624. [Google Scholar] [CrossRef]
- Fostinelli, S.; De Amicis, R.; Leone, A.; Giustizieri, V.; Binetti, G.; Bertoli, S.; Battezzati, A.; Cappa, S.F. Eating Behavior in Aging and Dementia: The Need for a Comprehensive Assessment. Front. Nutr. 2020, 7, 604488. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, C.; Niznik, J.; Li, A. Deprescribing Research in Nursing Home Residents Using Routinely Collected Healthcare Data: A Conceptual Framework. BMC Geriatr. 2023, 23, 469. [Google Scholar] [CrossRef] [PubMed]
- Roe, B.; Flanagan, L.; Maden, M. Systematic Review of Systematic Reviews for the Management of Urinary Incontinence and Promotion of Continence Using Conservative Behavioural Approaches in Older People in Care Homes. J. Adv. Nurs. 2015, 71, 1464–1483. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015.
- Buma, L.E.; Vluggen, S.; Zwakhalen, S.; Kempen, G.I.J.M.; Metzelthin, S.F. Effects on Clients’ Daily Functioning and Common Features of Reablement Interventions: A Systematic Literature Review. Eur. J. Ageing 2022, 19, 903–929. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, R.; Beerens, H.C.; van Rossum, E.; Verbeek, H.; Hamers, J.P.H. Editorial: Rethinking the Staff-Quality Relationship in Nursing Homes. J. Nutr. Health Aging 2018, 22, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Cremer, S.; Vluggen, S.; de Man-Van-Ginkel, J.M.; Metzelthin, S.F.; Zwakhalen, S.M.; Bleijlevens, M.H.C. Effective Nursing Interventions in ADL Care Affecting Independence and Comfort—A Systematic Review. Geriatr. Nurs. 2023, 52, 73–90. [Google Scholar] [CrossRef] [PubMed]
- Verstraten, C.C.J.M.M.; Metzelthin, S.F.; Schoonhoven, L.; Schuurmans, M.J.; de Man-van Ginkel, J.M. Optimizing Patients’ Functional Status during Daily Nursing Care Interventions: A Systematic Review. Res. Nurs. Health 2020, 43, 478–488. [Google Scholar] [CrossRef]
- Izquierdo, M.; Fiatarone Singh, M. Promoting Resilience in the Face of Ageing and Disease: The Central Role of Exercise and Physical Activity. Ageing Res. Rev. 2023, 88, 101940. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Saco-Ledo, G.; Morales, J.S.; Gallardo-Gómez, D.; Morales-Palomo, F.; López-Ortiz, S.; Rivas-Baeza, B.; Castillo-García, A.; Jiménez-Pavón, D.; Santos-Lozano, A.; et al. Effects of Physical Exercise on Physical Function in Older Adults in Residential Care: A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials. Lancet Healthy Longev. 2023, 4, e247–e256. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable (Non-Missing N) | Frequency (%)/Mean (Standard Deviation) |
|---|---|
| Sociodemographic variables | |
| Sex (671) | |
| Female | 503 (75.0%) |
| Age (670) | 85.87 (±8.75) |
| Institutionalization months (671) | 36.55 (±42.36) |
| Education level (606) | |
| Illiterate | 105 (15.6%) |
| Marital Status (671) | |
| Married/In a relationship | 106 (15.8%) |
| Health variables | |
| Days of room isolation due to COVID-19 (635) | 20.77 (±27.74) |
| Physical restraint (635) | 102 (16.1%) |
| Resident COVID-19 infection history (634) | 425 (63.3%) |
| Cancer (671) | 59 (8.8%) |
| Neurological disease (671) | 217 (32.3%) |
| Digestive disease (671) | 40 (6.0%) |
| Renal disease (671) | 142 (21.2%) |
| Cardiac disease (670) | 288 (43.0%) |
| Severe mental disorder (670) | 107 (16.0%) |
| Intellectual disability (671) | 41 (6.1%) |
| Polypharmacy (670) | 581 (86.7%) |
| Weight loss or appetite loss (671) | 100 (14.9%) |
| Pain symptoms (671) | 183 (27.3%) |
| Shortness of breath (671) | 50 (7.5%) |
| Confusion or behavior disorder (670) | 160 (23.9%) |
| Multiple falls or serious fall (670) | 84 (12.5%) |
| Ulcer or chronic wound (670) | 57 (8.5%) |
| Dysphagia (670) | 86 (12.8%) |
| Urinary continence (669) | |
| Continent | 175 (26.1%) |
| Usually continent | 121 (18.0%) |
| Occasionally incontinent | 17 (2.5%) |
| Often incontinent | 35 (5.2%) |
| Always incontinent | 312 (46.5%) |
| Not classifiable | 2 (0.3%) |
| Fecal continence (662) | |
| Continent | 351 (52.3%) |
| Usually continent | 79 (11.8%) |
| Occasionally incontinent | 7 (1.0%) |
| Often incontinent | 5 (0.7%) |
| Always incontinent | 223 (33.2%) |
| Not classifiable | 4 (0.6%) |
| Constipation (668) | 263 (39.2%) |
| Vision impairment (668) | 85 (12.7%) |
| Hearing impairment (667) | 119 (17.8%) |
| Anxiety or depression symptoms (671) | 224 (33.4%) |
| Loneliness or social isolation (671) | 177 (26.4%) |
| Cognition [GDS] (671) | |
| GDS 1 | 136 (20.3%) |
| GDS 2 | 60 (8.9%) |
| GDS 3 | 62 (9.2%) |
| GDS 4 | 87 (13.0%) |
| GDS 5 | 76 (11.3%) |
| GDS 6 | 161 (24.0%) |
| GDS 7 | 89 (13.3%) |
| BADL dependance [Barthel] (671) | 36.3 (±26.9) |
| Bathing | 579 (86.3%) |
| Climbing stairs | 548 (81.7%) |
| Dressing | 526 (78.4%) |
| Personal hygiene | 486 (72.4%) |
| Toileting | 434 (64.7%) |
| Walking | 356 (53.1%) |
| Wheelchair handling (287) | 237 (82.6%) |
| Transferring | 344 (51.3%) |
| Eating | 173 (25.8%) |
| Institutionalization variables | |
| Residents’ outdoor accessibility (671) | 655 (97.6%) |
| Resident’s garden-like area accessibility (655) | 471 (71.9%) |
| Food service arrangement (671) | |
| Own kitchen | 532 (79.3%) |
| Catering service | 139 (20.7%) |
| Ownership (for profit) (671) | 538 (80.2%) |
| NH size [number of beds] (630) | 52.98 (±29.80) |
| Small (≤50 beds) | 266 (42.2%) |
| Middle (51–100 beds) | 329 (52.2%) |
| Large (˃100 beds) | 35 (5.6%) |
| Shared rooms per total rooms [%] (630) | 69.18 (±27.79) |
| Shared toilet per total toilets [%] (630) | 52.42 (±32.54) |
| Registered nurses’ ratio [hours/resident] (587) | 1.34 (±1.04) |
| Physical therapists’ ratio [hours/resident] (587) | 0.58 (±0.42) |
| Occupational therapists’ ratio [hours/resident] (587) | 0.19 (±0.17) |
| Psychologists’ ratio [hours/resident] (587) | 0.33 (±0.23) |
| Social workers’ ratio [hours/resident] (587) | 0.43 (±0.21) |
| Caregivers’ ratio [hours/resident] (587) | 11.82 (±4.78) |
| Nursing assistants’ ratio [hours/resident] (587) | 1.35 (±5.63) |
| Leisure monitors’ ratio [hours/resident] (587) | 0.05 (±0.13) |
| Geriatricians’ ratio [hours/resident] (587) | 0.19 (±0.12) |
| Total professionals’ ratio [hours/resident] (587) | 16.26 (±5.30) |
| Dependent | Independent/Minimal Help | p | OR (95% CI) | p | OR (95% CI) | |
|---|---|---|---|---|---|---|
| Variable | Frequency (%) or Mean (SD) | (Bivariate Analysis) | (Multivariate Analysis) | |||
| Sex (female) | 447 (89.6%) | 52 (10.4%) | 0.929 | 0.97 (0.57–1.74) | 0.066 | 0.54 (0.28–1.04) |
| Age | 86.1 (±8.6) | 69 (±83.4) | 0.041 | 17,484.50 | 0.375 | 1.01 (0.98–1.04) |
| Urinary continence | 349 (96.1%) | 14 (3.9%) | <0.001 | 5.61 (3.05–10.33) | <0.001 | 1.42 (1.17–1.72) |
| Cognition (GDS 2–6) | 497 (93.8%) | 33 (6.2%) | <0.001 | 5.42 (3.23–9.11) | <0.001 | 1.67 (1.41–1.99) |
| Multiple falls or serious fall | 80 (96.4%) | 3 (3.6%) | 0.031 | 3.41 (1.05–11.11) | 0.050 | 3.42 (1.00–11.64) |
| Fecal continence | 234 (98.7%) | 3 (1.3%) | <0.001 | 14.26 (4.43–45.89) | ||
| Residents’ outdoor accessibility | 589 (90.6%) | 61 (9.4%) | <0.001 | 9.66 (3.50–26.64) | ||
| Dysphagia | 84 (98.8%) | 1 (1.2%) | 0.003 | 11.16 (1.53–81.43) | ||
| Ulcer or chronic wound | 56 (98.2%) | 1 (1.8%) | 0.026 | 7.052 (0.96–51.76) | ||
| Confusion or behavior disorder | 148 (94.3%) | 9 (5.7%) | 0.029 | 2.20 (1.07–4.55) | ||
| NH type (private) | 471 (88.4%) | 62 (11.6%) | 0.031 | 0.42 (0.19–0.95) | ||
| Intellectual disability | 33 (80.5%) | 8 (19.5%) | 0.047 | 0.446 (0.20–1.01) | ||
| Neurological disease | 199 (93.0%) | 15 (7.0%) | 0.051 | 1.80 (0.99–3.27) | ||
| Weight loss or appetite loss | 94 (94.9%) | 5 (5.1%) | 0.060 | 2.39 (0.94–6.10) | ||
| Days of room isolation due to COVID-19 | 21.3 (±28.0) | 15.1 (±24.7) | 0.065 | 15,851.00 | ||
| Education level (illiterate) | 89 (85.6%) | 15 (14.4%) | 0.081 | 0.58 (0.31–1.08) | ||
| Marital status (married or in a relationship) | 100 (94.3%) | 6 (5.7%) | 0.083 | 2.11 (0.89–5.02) | ||
| Institutionalization months | 37.0 (±41.8) | 31.6 (±45.0) | 0.089 | 17,964.00 | ||
| Food service arrangement (catering service) | 128 (92.8%) | 10 (7.2%) | 0.178 | 1.61 (0.80–3.24) | ||
| R2 = 28.0% | ||||||
| Dependent | Independent | p | OR (95% CI) | p | OR (95% CI) | |
|---|---|---|---|---|---|---|
| Variable | Frequency (%) or Mean (SD) | (Bivariate Analysis) | (Multivariate Analysis) | |||
| Sex (female) | 304 (60.4%) | 199 (39.6%) | 0.374 | 1.17 (0.82–1.67) | 0.827 | 0.95 (0.63–1.45) |
| Age | 86.6 (±8.7) | 84.8 (±8.8) | 0.003 | 46,841.50 | 0.970 | 1.00 (0.99–1.03) |
| Fecal incontinence (occasionally or always) | 205 (85.8%) | 34 (14.2%) | <0.001 | 7.40 (4.92–11.15) | <0.001 | 1.41 (1.22–1.63) |
| Ulcer or chronic wound | 51 (89.5%) | 6 (10.5%) | <0.001 | 6.47 (2.74–15.31) | 0.003 | 4.01 (1.60–10.03) |
| Cognition (GDS 2–6) | 340 (63.6%) | 195 (36.4%) | <0.001 | 2.28 (1.55–3.33) | 0.008 | 1.14 (1.03–1.25) |
| Urinary incontinence (occasionally or always) | 275 (75.1%) | 91 (24.9%) | <0.001 | 4.56 (3.27–6.35) | 0.020 | 1.17 (1.02–1.33) |
| Physical restraint | 90 (8.2%) | 12 (11.8%) | <0.001 | 6.48 (3.46–12.11) | ||
| Severe mental disorder | 48 (44.9%) | 59 (55.1%) | <0.001 | 0.50 (0.33–0.75) | ||
| Dysphagia | 68 (79.1%) | 18 (20.9%) | <0.001 | 2.89 (1.68–4.98) | ||
| Residents’ outdoor accessibility | 396 (60.5%) | 259 (39.5%) | <0.001 | 6.63 (1.87–23.48) | ||
| Confusion or behavior disorder | 111 (69.4%) | 49 (30.6%) | 0.004 | 1.75 (1.20–2.55) | ||
| Institutionalization months | 38.0 (±41.2) | 34.5 (±43.9) | 0.023 | 48,356.50 | ||
| Constipation | 170 (64.6%) | 93 (35.4%) | 0.023 | 1.25 (1.05–1.99) | ||
| Caregivers per residents (%) | 33.5 (±13.2) | 32.2 (±13.0) | 0.042 | 37,477.50 | ||
| Days of room isolation due to COVID-19 | 22.0 (±27.9) | 19.0 (±27.5) | 0.047 | 53,036.00 | ||
| Weight loss or appetite loss | 68 (68.0%) | 32 (32.0%) | 0.059 | 1.54 (0.98–2.42) | ||
| Intellectual disability | 19 (46.3%) | 22 (53.7%) | 0.077 | 0.57 (0.30–1.07) | ||
| Vision impairment (0–10) | 0.9 (±2.8) | 0.6 (±2.0) | 0.081 | 51,318.00 | ||
| Anxiety or depression symptoms | 123 (54.9%) | 101 (45.1%) | 0.089 | 0.76 (0.55–1.04) | ||
| Food service arrangement (catering service) | 91 (65.5%) | 48 (34.5%) | 0.105 | 1.38 (0.93–2.04) | ||
| Neurological disease | 138 (63.6%) | 79 (36.4%) | 0.132 | 1.29 (0.93–1.80) | ||
| Resident COVID-19 infection history | 259 (60.9%) | 166 (39.1%) | 0.185 | 1.25 (0.90–1.75) | ||
| Polypharmacy | 340 (58.5%) | 241 (41.5%) | 0.234 | 0.75 (0.47–1.20) | ||
| Education level (illiterate) | 68 (64.8%) | 37 (35.2%) | 0.250 | 1.33 (0.86–2.06) | ||
| Dependent | Independent/Minimal Help | p | OR (95% CI) or U Mann-Whitney | p | OR (95% CI) | |
|---|---|---|---|---|---|---|
| Variable | Frequency (%) or Mean (SD) | (Bivariate Analysis) | (Multivariate Analysis) | |||
| Sex (female) | 151 (30.0%) | 352 (70.0%) | 0.046 | 1.52 (1.01–2.29) | 0.117 | 1.52 (0.90–2.56) |
| Age | 85.9 (±8.8) | 85.9 (±8.7) | 0.947 | 45,159.0 | 0.152 | 0.98 (0.96–1.01) |
| Fecal incontinence (occasionally and always) | 133 (55.6%) | 106 (44.4%) | <0.001 | 8.74 (5.96–12.81) | <0.001 | 1.56 (1.38–1.77) |
| Food service arrangement (catering service) | 67 (48.2%) | 72 (51.8%) | <0.001 | 3.16 (2.14–4.67) | <0.001 | 4.28 (2.60–7.05) |
| Neurological disease | 79 (36.4%) | 138 (63.6%) | <0.001 | 1.81 (1.28–2.57) | <0.001 | 2.11 (1.36–3.28) |
| Cognition (GDS 2–6) | 159 (38.5%) | 254 (61.5%) | <0.001 | 2.66 (1.60–4.42) | <0.001 | 1.31 (1.16–1.48) |
| Dysphagia | 59 (58.1%) | 36 (41.9%) | <0.001 | 4.489 (2.81–7.18) | 0.009 | 2.16 (1.21–3.87) |
| Polypharmacy | 150 (25.8%) | 431 (74.2%) | <0.001 | 0.47 (0.30–0.74) | 0.016 | 0.49 (0.27–0.88) |
| Weight loss or appetite loss | 41 (41.0%) | 59 (59.0%) | 0.002 | 2.004 (1.29–3.11) | 0.026 | 1.90 (1.08–3.35) |
| Physical restraint | 49 (48.0%) | 53 (52.0%) | <0.001 | 2.96 (1.91–4.57) | ||
| Confusion or behavior disorder | 64 (40.0%) | 96 (60.0%) | <0.001 | 2.08 (1.43–3.02) | ||
| Ulcer or chronic wound | 33 (57.9%) | 24 (42.1%) | <0.001 | 4.063 (2.33–7.09) | ||
| Urinary incontinence (occasionally or always) | 143 (39.1%) | 223 (60.9%) | <0.001 | 3.878 (2.630–5.72) | ||
| NH type (private) | 132 (24.5%) | 406 (75.5%) | <0.001 | 0.45 (0.30–0.66) | ||
| Shared toilets per total toilets (%) | 59.3 (±31.0) | 49.8 (±32.8) | <0.001 | 335,500.0 | ||
| Caregivers per residents (%) | 35.3 (±11.0) | 31.9 (±13.8) | <0.001 | 27,046.5 | ||
| Doctors per residents (%) | 0.5 (±0.3) | 0.4 (±0.3) | 0.005 | 29,910.0 | ||
| Anxiety or depression symptoms | 49 (21.9%) | 175 (78.1%) | 0.012 | 0.62 (0.43–0.90) | ||
| Renal disease | 28 (19.7%) | 114 (80.3%) | 0.013 | 0.57 (0.36–0.89) | ||
| Residents’ garden-like area accessibility | 147 (31.2%) | 324 (68.8%) | 0.016 | 1.633 (1.09–2.44) | ||
| Shortness of breath (0–10) | 0.2 (±1.0) | 0.5 (±1.7) | 0.046 | 43,354.5 | ||
| Marital status (married or in a relationship) | 38 (35.8%) | 68 (64.2%) | 0.050 | 1.55 (1.00–2.40) | ||
| Residents’ outdoor accessibility | 187 (28.5%) | 468 (71.5%) | 0.050 | 5.994 (0.79–45.70) | ||
| Days of room isolation due to COVID-19 | 22.2 (±27.3) | 20.2 (±27.9) | 0.069 | 36,710.5 | ||
| Institutionalization months | 38.2 (±40.7) | 35.9 (±43.0) | 0.111 | 42,492.5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Martin, P.; Minobes-Molina, E.; Carbó-Cardeña, A.; Masó-Aguado, M.; Solé-Casals, M.; Torrents-Solé, M.; Bort-Roig, J.; Amblàs-Novellas, J.; Gómez-Batiste, X.; Jerez-Roig, J. Exploring Early, Middle, and Late Loss in Basic Activities of Daily Living among Nursing Home Residents: A Multicenter Observational Study. Healthcare 2024, 12, 810. https://doi.org/10.3390/healthcare12080810
Moreno-Martin P, Minobes-Molina E, Carbó-Cardeña A, Masó-Aguado M, Solé-Casals M, Torrents-Solé M, Bort-Roig J, Amblàs-Novellas J, Gómez-Batiste X, Jerez-Roig J. Exploring Early, Middle, and Late Loss in Basic Activities of Daily Living among Nursing Home Residents: A Multicenter Observational Study. Healthcare. 2024; 12(8):810. https://doi.org/10.3390/healthcare12080810
Chicago/Turabian StyleMoreno-Martin, Pau, Eduard Minobes-Molina, Aina Carbó-Cardeña, Montse Masó-Aguado, Montserrat Solé-Casals, Meritxell Torrents-Solé, Judit Bort-Roig, Jordi Amblàs-Novellas, Xavier Gómez-Batiste, and Javier Jerez-Roig. 2024. "Exploring Early, Middle, and Late Loss in Basic Activities of Daily Living among Nursing Home Residents: A Multicenter Observational Study" Healthcare 12, no. 8: 810. https://doi.org/10.3390/healthcare12080810
APA StyleMoreno-Martin, P., Minobes-Molina, E., Carbó-Cardeña, A., Masó-Aguado, M., Solé-Casals, M., Torrents-Solé, M., Bort-Roig, J., Amblàs-Novellas, J., Gómez-Batiste, X., & Jerez-Roig, J. (2024). Exploring Early, Middle, and Late Loss in Basic Activities of Daily Living among Nursing Home Residents: A Multicenter Observational Study. Healthcare, 12(8), 810. https://doi.org/10.3390/healthcare12080810