
Network Analysis of Sexual Well-Being in Women with Heart Failure: The Psychocardiological Perspective



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of the Studied Sample
3.2. Network Edge Analysis
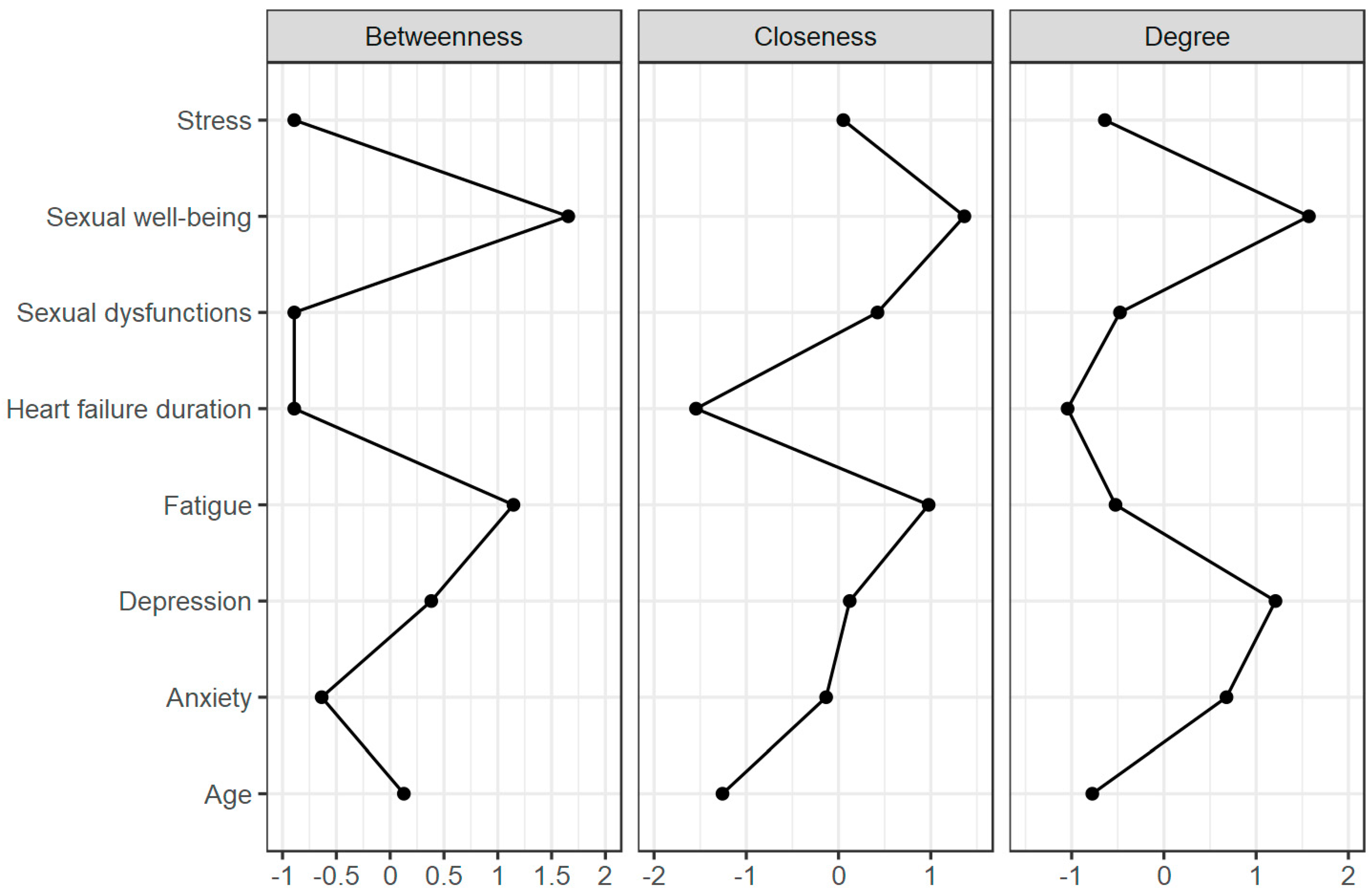
3.3. Network Centrality Analysis
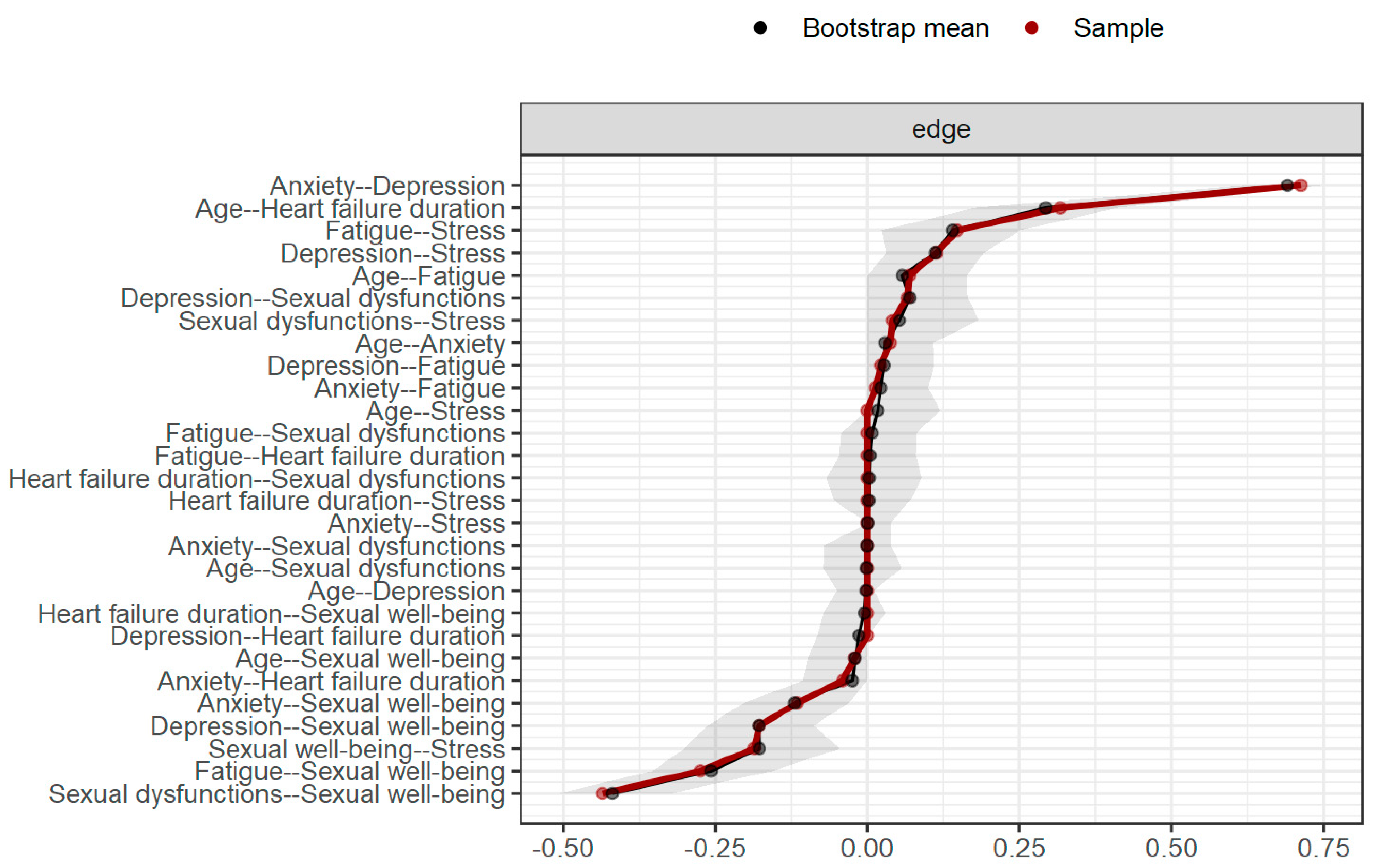
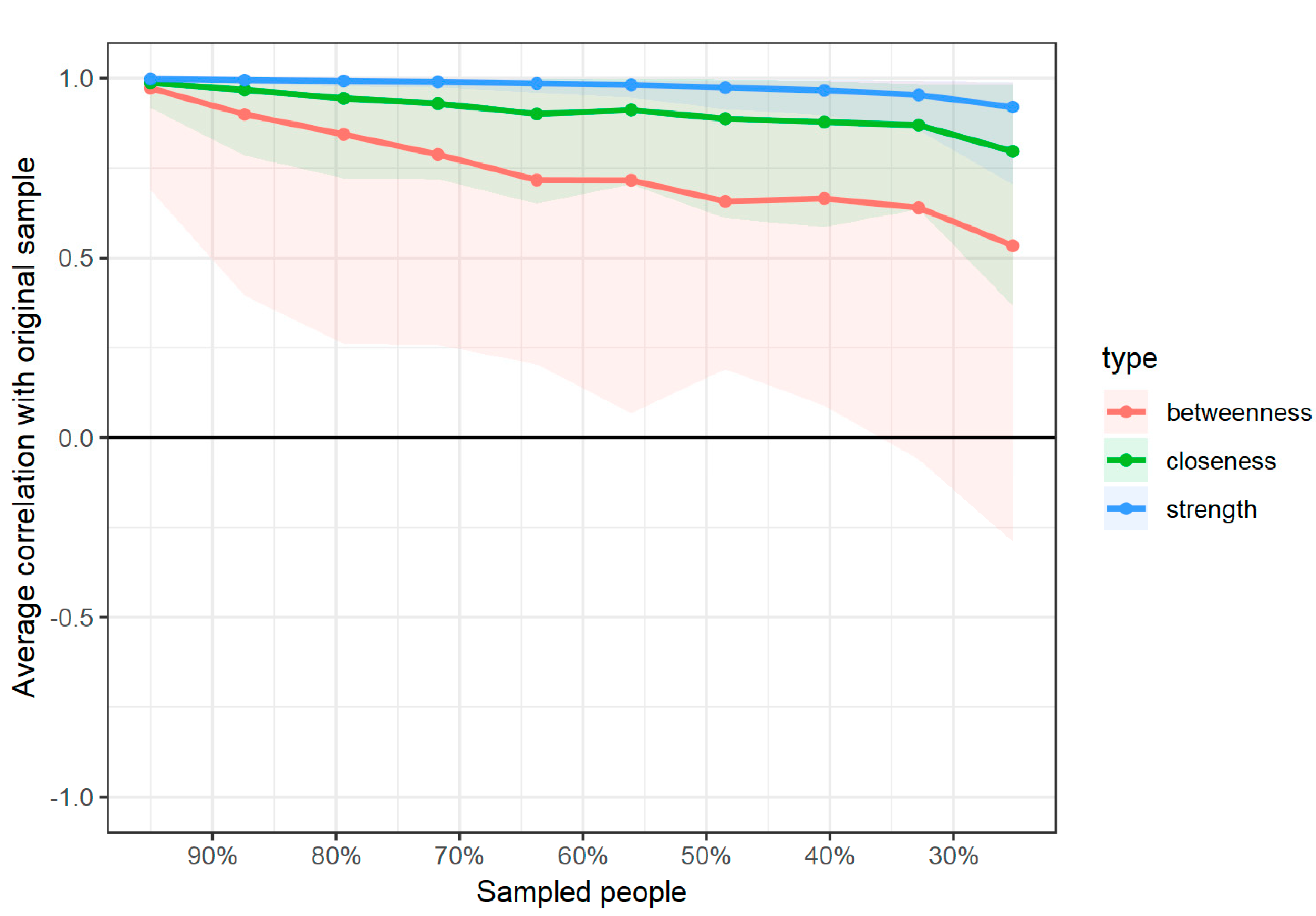
3.4. Edge and Centrality Stability Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seferović, P.M.; Vardas, P.; Jankowska, E.A.; Maggioni, A.P.; Timmis, A.; Milinković, I.; Polovina, M.; Gale, C.P.; Lund, L.H.; Lopatin, Y. The Heart Failure Association Atlas: Heart Failure Epidemiology and Management Statistics 2019. Eur. J. Heart Fail. 2021. Online First. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; AlKatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The Global Epidemiology of Hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Gerymski, R. Relationships of Meaning Resources and Illness Perception with Quality of Life in People with Heart Failure: The Mediating Role of Coping. Doctoral Dissertation, Opole University, Opole, Poland, 2024. [Google Scholar]
- Leszek, P.; Zaleska-Kociecka, M.; Was, D.; Witczak, K.; Bartolik, K.; Rolska-Wojcik, P.; Brukalo, K.; Maruszewski, B.; Kleinork, A. Real World Heart Failure Epidemiology and Outcome: A Population-Based Analysis of 1,990,162 Heart Failure Patients. Eur. Heart J. 2020, 41, ehaa946-0968. [Google Scholar] [CrossRef]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of Heart Failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef] [PubMed]
- Baert, A.; Pardaens, S.; De Smedt, D.; Puddu, P.E.; Ciancarelli, M.C.; Dawodu, A.; De Sutter, J.; De Bacquer, D.; Clays, E. Sexual Activity in Heart Failure Patients: Information Needs and Association with Health-Related Quality of Life. Int. J. Environ. Res. Public. Health 2019, 16, 1570. [Google Scholar] [CrossRef]
- Jackson, S.E.; Firth, J.; Veronese, N.; Stubbs, B.; Koyanagi, A.; Yang, L.; Smith, L. Decline in Sexuality and Wellbeing in Older Adults: A Population-Based Study. J. Affect. Disord. 2019, 245, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, K.R.; Lewis, R.; O’Sullivan, L.F.; Fortenberry, J.D. What Is Sexual Wellbeing and Why Does It Matter for Public Health? Lancet Public Health 2021, 6, e608–e613. [Google Scholar] [CrossRef] [PubMed]
- Gerymski, R. Short Sexual Well-Being Scale—A Cross-Sectional Validation among Transgender and Cisgender People. Health Psychol. Rep. 2021, 9, 276–287. [Google Scholar] [CrossRef]
- Stephenson, K.R.; Meston, C.M. Differentiating Components of Sexual Well-Being in Women: Are Sexual Satisfaction and Sexual Distress Independent Constructs? J. Sex. Med. 2010, 7, 2458–2468. [Google Scholar] [CrossRef]
- Mitchell, K.R.; Palmer, M.J.; Lewis, R.; Bosó Pérez, R.; Maxwell, K.J.; Macdowall, W.; Reid, D.; Bonell, C.; Mercer, C.H.; Sonnenberg, P.; et al. Development and Validation of a Brief Measure of Sexual Wellbeing for Population Surveys: The Natsal Sexual Wellbeing Measure (Natsal-SW). J. Sex Res. 2023, 1–11. [Google Scholar] [CrossRef]
- Gerymski, R.; Magoń, W. Chemsex and Sexual Well-Being in Young Polish Men. Int. J. Environ. Res. Public. Health 2023, 20, 6163. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, A.; Hazell, E. Sexual Well-Being in Cancer and Palliative Care: An Assessment of Healthcare Professionals’ Current Practice and Training Needs. BMJ Support. Palliat. Care 2017, 7, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Gerymski, R.; Cisek, A.; Dymecka, J. Seksualny Dobrostan a Satysfakcja z Życia Osób z Niepełnosprawnością Ruchową: Moderacyjna Rola Samooceny [Sexual Well-Being and Life Satisfaction of People with Motor Disabilities: The Moderating Role of Self-Esteem]. J. Sex. Ment. Health 2022, 20, 1–7. [Google Scholar] [CrossRef]
- Furmańska, J.; Koziarska, D.; Szcześniak, M.; Rzepa, T.; Nowacki, P. Sexual Satisfaction, Self-Esteem and Acceptance of Illness among Relapse-Remitting Multiple Sclerosis Patients. Adv. Psychiatry Neurol. 2017, 26, 236–245. [Google Scholar] [CrossRef]
- Wylomanski, S.; Bouquin, R.; Hanf, M.; Winer, N.; Dréno, B.; Rouzier, R.; Quéreux, G. Sexual Well-Being in Patients with Vulvar Disease: Results from a Preliminary Prospective Matched Case–Control Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 106–110. [Google Scholar] [CrossRef]
- Gerymski, R.; Szeląg, M. Sexual Well-Being in Individuals with Schizophrenia: A Pilot Study on the Role of Self-Esteem and Acceptance of Illness. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1318–1329. [Google Scholar] [CrossRef]
- Eleuteri, S.; Aminoff, D.; Lucidi, F.; Violani, C.; Grano, C. Sexual Well-Being in Adolescent and Young Adults Born with Arm: The Perspective of the Patients. Pediatr. Surg. Int. 2019, 35, 945–951. [Google Scholar] [CrossRef]
- Altıok, M.; Yılmaz, M. Opinions of Individuals Who Have Had Myocardial Infarction about Sex. Sex. Disabil. 2011, 29, 263–273. [Google Scholar] [CrossRef]
- Drory, Y.; Kravetz, S.; Weingarten, M. Comparison of Sexual Activity of Women and Men after a First Acute Myocardial Infarction. Am. J. Cardiol. 2000, 85, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.; Sardinha, A.; Araújo, C.G.S. Sexual Activity and Heart Patients: A Contemporary Perspective. Can. J. Cardiol. 2016, 32, 410–420. [Google Scholar] [CrossRef]
- Træen, B.; Samara, O. Sexual Dysfunction and Sexual Well-Being in People with Heart Disease. Sex. Relatsh. Ther. 2007, 22, 193–208. [Google Scholar] [CrossRef]
- Reese, J.B.; Shelby, R.A.; Taylor, K.L. Sexual Quality of Life in Patients Undergoing Coronary Artery Bypass Graft Surgery. Psychol. Health 2012, 27, 721–736. [Google Scholar] [CrossRef]
- Firoozjaei, I.T.; Taghadosi, M.; Sadat, Z. Determining the Sexual Quality of Life and Related Factors in Patients Referred to the Department of Cardiac Rehabilitation: A Cross-Sectional Study. Int. J. Reprod. Biomed. 2021, 19, 261. [Google Scholar]
- Tang, W.-R.; Yu, C.-Y.; Yeh, S.-J. Fatigue and Its Related Factors in Patients with Chronic Heart Failure. J. Clin. Nurs. 2010, 19, 69–78. [Google Scholar] [CrossRef]
- Polikandrioti, M.; Kalafatakis, F.; Koutelekos, I.; Kokoularis, D. Fatigue in Heart Failure Outpatients: Levels, Associated Factors, and the Impact on Quality of Life. Arch. Med. Sci.-Atheroscler. Dis. 2019, 4, 103–112. [Google Scholar] [CrossRef]
- Sheffler, J.L.; Schmiege, S.J.; Sussman, J.; Bekelman, D.B. A Longitudinal Analysis of the Relationships between Depression, Fatigue, and Pain in Patients with Heart Failure. Aging Ment. Health 2021, 25, 2272–2278. [Google Scholar] [CrossRef]
- Aggelopoulou, Z.; Fotos, N.V.; Chatziefstratiou, A.A.; Giakoumidakis, K.; Elefsiniotis, I.; Brokalaki, H. The Level of Anxiety, Depression and Quality of Life among Patients with Heart Failure in Greece. Appl. Nurs. Res. 2017, 34, 52–56. [Google Scholar] [CrossRef]
- Iozzia, G.; de Miranda Azevedo, R.; van der Harst, P.; Rosmalen, J.G.M.; de Jonge, P.; Roest, A.M. Association of Recognized and Unrecognized Myocardial Infarction With Depressive and Anxiety Disorders in 125,988 Individuals: A Report of the Lifelines Cohort Study. Psychosom. Med. 2020, 82, 736. [Google Scholar] [CrossRef]
- Eastwood, J.-A.; Moser, D.K.; Riegel, B.J.; Albert, N.M.; Pressler, S.; Chung, M.L.; Dunbar, S.; Wu, J.-R.; Lennie, T.A. Commonalities and Differences in Correlates of Depressive Symptoms in Men and Women with Heart Failure. Eur. J. Cardiovasc. Nurs. 2012, 11, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wen, Y.; Peng, H.; Zhu, H.; Wang, W.E.; Zhou, J. Gender Differences in Anxiety, Depression, Insomnia, and Quality of Life in Heart Failure With Preserved Ejection Fraction: A Multicenter, Cross-Sectional Study. J. Cardiovasc. Nurs. 2023, 38, 425. [Google Scholar] [CrossRef]
- Tsabedze, N.; Kinsey, J.-L.H.; Mpanya, D.; Mogashoa, V.; Klug, E.; Manga, P. The Prevalence of Depression, Stress and Anxiety Symptoms in Patients with Chronic Heart Failure. Int. J. Ment. Health Syst. 2021, 15, 44. [Google Scholar] [CrossRef]
- Salyer, J.; Flattery, M.; Lyon, D.E. Heart Failure Symptom Clusters and Quality of Life. Heart Lung 2019, 48, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-W.; Chen, T.-Y.; Cheng, S.-M.; Lin, W.-S.; Friedmann, E.; Thomas, S.A. Gender Differences in the Predictors of Depression among Patients with Heart Failure. Eur. J. Cardiovasc. Nurs. 2014, 13, 320–328. [Google Scholar] [CrossRef]
- Piepenburg, S.M.; Faller, H.; Störk, S.; Ertl, G.; Angermann, C.E. Symptom Patterns and Clinical Outcomes in Women versus Men with Systolic Heart Failure and Depression. Clin. Res. Cardiol. 2019, 108, 244–253. [Google Scholar] [CrossRef]
- Sobczak, M.; Kasprzak, J.D.; Drygas, W. Psychocardiology—Introduction to a New Scientific Discipline. Pol. Heart J. 2011, 69, 838–843. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Michielsen, H.J.; De Vries, J.; Van Heck, G.L.; Van De Vijver, F.J.R.; Sijtsma, K. Examination of the Dimensionality of Fatigue. Eur. J. Psychol. Assess. 2004, 20, 39–48. [Google Scholar] [CrossRef]
- Constantin, M.A.; Schuurman, N.K.; Vermunt, J.K. A General Monte Carlo Method for Sample Size Analysis in the Context of Network Models. Psychol. Methods 2023. [Google Scholar] [CrossRef] [PubMed]
- Constantin, M.A.; Cramer, A.O.J. Sample Size Recommendations for Estimating Cross-Sectional Network Models; Tilburg University: Tilburg, The Netherlands, 2018. [Google Scholar]
- Hevey, D. Network Analysis: A Brief Overview and Tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S. Network Psychometrics. Doctoral Dissertation, University of Amsterdam, Amsterdam, The Netherlands, 2017. [Google Scholar]
- Epskamp, S.; Fried, E.I. A Tutorial on Regularized Partial Correlation Networks. Psychol. Methods 2018, 23, 617–634. [Google Scholar] [CrossRef] [PubMed]
- JASP—Jeffreys’s Amazing Statistics Program, version 0.11.1.0; The JASP Team: Amsterdam, The Netherlands, 2024.
- Burger, J.; Isvoranu, A.-M.; Lunansky, G.; Haslbeck, J.; Epskamp, S.; Hoekstra, R.H.; Fried, E.I.; Borsboom, D.; Blanken, T.F. Reporting Standards for Psychological Network Analyses in Cross-Sectional Data. Psychol. Methods 2022, 28, 806–824. [Google Scholar] [CrossRef]
- Epskamp, S. Brief Report on Estimating Regularized Gaussian Networks from Continuous and Ordinal Data. arXiv 2016, arXiv:1606.05771. [Google Scholar]
- Dalege, J.; Borsboom, D.; Van Harreveld, F.; Van Der Maas, H.L.J. Network Analysis on Attitudes: A Brief Tutorial. Soc. Psychol. Personal. Sci. 2017, 8, 528–537. [Google Scholar] [CrossRef]
- Levine, G.N.; Steinke, E.E.; Bakaeen, F.G.; Bozkurt, B.; Cheitlin, M.D.; Conti, J.B.; Foster, E.; Jaarsma, T.; Kloner, R.A.; Lange, R.A.; et al. Sexual Activity and Cardiovascular Disease. Circulation 2012, 125, 1058–1072. [Google Scholar] [CrossRef]
- Moser, D.K.; Dracup, K.; Evangelista, L.S.; Zambroski, C.H.; Lennie, T.A.; Chung, M.L.; Doering, L.V.; Westlake, C.; Heo, S. Comparison of Prevalence of Symptoms of Depression, Anxiety, and Hostility in Elderly Patients with Heart Failure, Myocardial Infarction, and a Coronary Artery Bypass Graft. Heart Lung 2010, 39, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.; Le Grande, M.; Alvarenga, M.; Worcester, M.; Jackson, A. Anxiety and Depression after a Cardiac Event: Prevalence and Predictors. Front. Psychol. 2020, 10, 502260. [Google Scholar] [CrossRef] [PubMed]
- Petrowski, K.; Kliem, S.; Sadler, M.; Meuret, A.E.; Ritz, T.; Brähler, E. Factor Structure and Psychometric Properties of the English Version of the Trier Inventory for Chronic Stress (TICS-E). BMC Med. Res. Methodol. 2018, 18, 18. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Uhl, G.A. Chronic Stress as a Mediator of Acute Stress: The Case of Hurricane Hugo. J. Appl. Soc. Psychol. 1993, 23, 1263–1284. [Google Scholar] [CrossRef]
- Metz, M.E.; McCarthy, B.W. The “Good-Enough Sex” Model for Couple Sexual Satisfaction. Sex. Relatsh. Ther. 2007, 22, 351–362. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M | SD | Me | Min | Max | |
|---|---|---|---|---|---|
| Age | 45.48 | 7.65 | 46.00 | 18.00 | 59.00 |
| Heart failure duration | 3.54 | 1.94 | 3.00 | 1.00 | 7.00 |
| Number of sexual dysfunctions | 1.13 | 1.20 | 1.00 | 0.00 | 3.00 |
| n | % | ||||
| Gender | |||||
| Women | 262 | 100.00% | |||
| Men | 0 | 0.00% | |||
| Place of residence | |||||
| Town/city | 179 | 68.32% | |||
| Village | 83 | 31.68% | |||
| Marital status | |||||
| Married | 163 | 62.21% | |||
| Informal relationship | 91 | 34.73% | |||
| Single | 8 | 3.05% | |||
| Education | |||||
| ISCED 6–8: Tetriary: Bachelors and higher (in Poland: wyższe) | 170 | 64.89% | |||
| ISCED 3: Upper Secondary: High School (in Poland: średnie) | 92 | 35.11% | |||
| Employment status | |||||
| Employed | 212 | 80.92% | |||
| Unemployed | 50 | 19.08% | |||
| Lifestyle information | |||||
| Alcohol consumption | 207 | 79.01% | |||
| Smoking tobacco cigarettes | 31 | 11.83% | |||
| Smoking e-cigarettes | 21 | 8.02% | |||
| Physical activity—swimming | 17 | 6.49% | |||
| Physical activity—bicycle riding | 11 | 4.20% | |||
| Physical activity—walking | 49 | 18.70% | |||
| Being under the care of a cardiology clinic | 195 | 74.43% | |||
| Being under the care of a psychologist | 25 | 9.54% | |||
| Being under the care of a psychiatrist | 7 | 2.67% | |||
| Being hospitalized in the past 6 months | 0 | 0.00% | |||
| Cardiological diagnosis | |||||
| Heart failure (NYHA II & III) | 262 | 100.00% | |||
| Coronary heart disease | 104 | 39.69% | |||
| Primary hypertension | 233 | 88.93% | |||
| Secondary hypertension | 9 | 3.44% | |||
| Myocardial infarction | 3 | 1.15% | |||
| Type 1 diabetes | 8 | 3.05% | |||
| Type 2 diabetes | 22 | 8.40% | |||
| Atherosclerosis | 48 | 18.32% | |||
| Other diseases and illnesses | |||||
| Depression | 23 | 8.78% | |||
| Hypothyroidism | 19 | 7.25% | |||
| Psoriasis | 4 | 1.53% | |||
| Insulin resistance | 1 | 0.38% | |||
| Implanted devices | |||||
| Cardiac resynchronization therapy (CRT) | 1 | 0.38% | |||
| Implantable cardioverter–defibrillator (ICD) | 3 | 1.15% | |||
| Pharmacotherapy * | |||||
| Metoprolol | 21 | 8.02% | |||
| Spironolactone | 17 | 6.49% | |||
| Perindopril | 13 | 4.96% | |||
| k of Nodes | k of Non-Zero Edges | Sparsity | |||||
|---|---|---|---|---|---|---|---|
| 8 | 17/28 | 0.393 | |||||
| Age | HF Duration | Fatigue | Depression | Anxiety | Stress | Sexual Dysfunctions | |
| Age | - | ||||||
| HF duration | 0.317 | - | |||||
| Fatigue | 0.069 | - | - | ||||
| Depression | - | - | 0.022 | - | |||
| Anxiety | 0.037 | −0.041 | 0.013 | 0.713 | - | ||
| Stress | - | - | 0.148 | 0.114 | - | - | |
| Sexual dysfunctions | - | - | - | 0.066 | - | 0.041 | - |
| Sexual well-being | −0.021 | - | −0.275 | −0.177 | −0.115 | −0.186 | −0.436 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerymski, R.; Latusek-Mierzwa, M. Network Analysis of Sexual Well-Being in Women with Heart Failure: The Psychocardiological Perspective. Healthcare 2024, 12, 817. https://doi.org/10.3390/healthcare12080817
Gerymski R, Latusek-Mierzwa M. Network Analysis of Sexual Well-Being in Women with Heart Failure: The Psychocardiological Perspective. Healthcare. 2024; 12(8):817. https://doi.org/10.3390/healthcare12080817
Chicago/Turabian StyleGerymski, Rafał, and Maria Latusek-Mierzwa. 2024. "Network Analysis of Sexual Well-Being in Women with Heart Failure: The Psychocardiological Perspective" Healthcare 12, no. 8: 817. https://doi.org/10.3390/healthcare12080817