
Echoes of Support: A Qualitative Meta-Synthesis of Caregiver Narratives in Lung Cancer Care



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Quality Assessment
2.3. Qualitative Meta-Synthesis Methods
3. Results
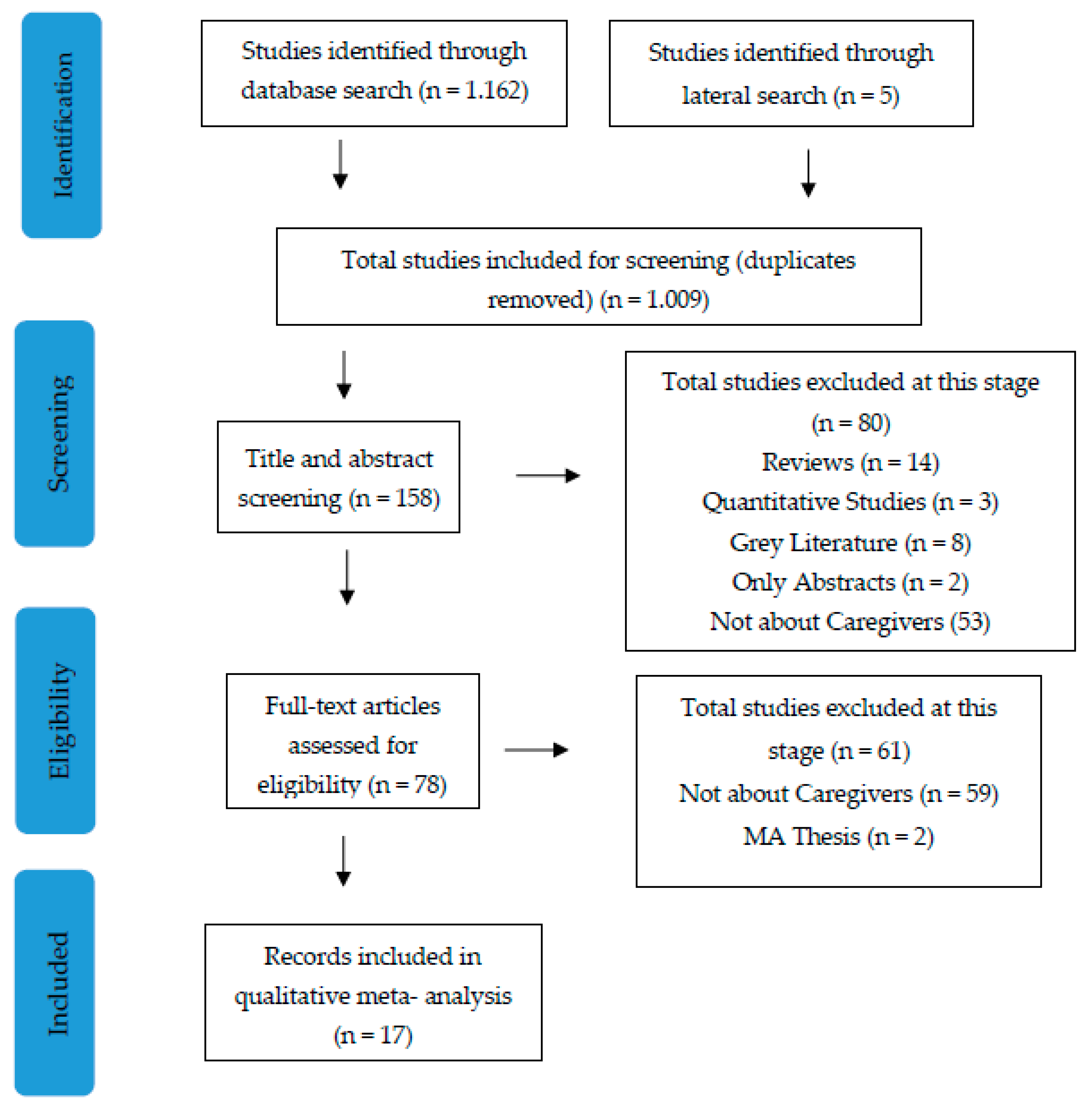
3.1. Characteristics of Included Studies
3.2. Information Accessibility
“We have a kind of reticence to ask our treating specialist questions. They do not like it when you ask a question.”[26]
‘I think it is very good to be able to ask a physician questions online. It’s a smaller step to take than calling or talking to your treating specialist.’[26]
3.3. Dual Roles and Family Dynamics
“getting him to the medical appointments, getting him his medication, and then also dealing with the financial aspects of it. Making sure that all his disability forms are filled in so he can get his check on time.”[30]
“[the situation due to the disease] stresses you out of course …. Psychologically and, I would also say, physically. Because you … must help more than usual. And then you are just doubly challenged.”[35]
“Yes, I finally gave in … (the participant laughed), yes, I even washed the clothes and everything what housewife usually did because she was too weak, lack of energy … thank God I helped.”[36]
3.4. Coping with Emotional Challenges and Uncertainty
“It’s overwhelming. So, I try not to think about it, like when you feel this stuff coming on, all these questions, and they all congregate at once, you know. Especially when it’s 4 AM in the morning when you’re laying in bed, and there’s all these questions.”[25]
“I’m trying to occupy him so he doesn’t think… I make him go shopping with me, or I tell him, ‘let’s go for a ride. I don’t want to stay in the house.’ Or we’ll go in the backyard and sit under a tree and just talk.”[30]
“I do that meditation tape before bed. That seems to help me a lot in trying to sleep. Because it calms me down.”[25]
“And then we became very religious now. Every night we pray the rosary. And every Wednesday we go to church.”[25]
‘Yes, today not tomorrow. I could never look forward, not not look forward but I don’t think about what’s going to happen tomorrow. I always think about what’s going to happen today. I wake up, how is she?’[33]
3.5. Need for Support Networks
“No support for me at all. Zero, I would say. I don’t think anyone has ever in the whole process asked me how I was coping with it. Like we don’t count. Like people don’t think that we’re affected by it.”[27]
‘I don’t know what to do with the situation. If I was having a bad day, I’d basically keep it to myself.’[28]
“We are going to forbid her from going back, because when you go to a place for support, and you come back and you’re more depressed than when you went, I… do not take that brand of support.”[31]
‘I … probably wouldn’t have time to attend anything or talk to anybody.’[28]
4. Discussion
Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. The ENTREQ Checklist
| Item | Guide and Description | Reported on Page # |
| Aim | State the research question the synthesis addresses | 2 |
| Synthesis methodology | Identify the synthesis methodology or theoretical framework which underpins the synthesis, and describe the rationale for choice of methodology (e.g., meta-ethnography, thematic synthesis, critical interpretive synthesis, grounded theory synthesis, realist synthesis, meta-aggregation, meta-study, framework synthesis). | 2–3 |
| Approach to searching | Indicate whether the search was pre-planned (comprehensive search strategies to seek all available studies) or iterative (to seek all available concepts until theoretical saturation is achieved). | 2–3 |
| Inclusion criteria | Specify the inclusion/exclusion criteria (e.g., in terms of population, language, year limits, type of publication, study type). | 3 |
| Data sources | Describe the information sources used (e.g., electronic databases (MEDLINE, EMBASE, CINAHL, psychINFO, Econlit), the grey literature databases (digital thesis, policy reports), relevant organizational websites, experts, information specialists, generic web searches (Google Scholar), hand searching, reference lists) and when the searches were conducted; provide the rationale for using the data sources. | 2–3 |
| Electronic search strategy | Describe the literature search (e.g., provide electronic search strategies with population terms, clinical or health topic terms, experiential or social phenomena-related terms, filters for qualitative research, and search limits). | 3–4 |
| Study screening methods | Describe the process of study screening and sifting (e.g., title, abstract and full text review, number of independent reviewers who screened studies) | 3–4 |
| Study characteristics | Present the characteristics of the included studies (e.g., year of publication, country, population, number of participants, data collection, methodology, analysis, research questions). | 5 (Table 1) |
| Study selection results | Identify the number of studies screened and provide reasons for study exclusion (e.g., for comprehensive searching, provide numbers of studies screened and reasons for exclusion indicated in a figure/flowchart; for iterative searching, describe reasons for study exclusion and inclusion based on modifications to the research question and/or contribution to theory development). | 2–4 and Figure 1 |
| Rationale for appraisal | Describe the rationale and approach used to appraise the included studies or selected findings (e.g., assessment of conduct (validity and robustness), assessment of reporting (transparency), assessment of content and utility of the findings). | 3 |
| Appraisal items | State the tools, frameworks, and criteria used to appraise the studies or selected findings (e.g., Existing tools: CASP, QARI, COREQ, Mays and Pope [30]; reviewer developed tools; describe the domains assessed: research team, study design, data analysis and interpretations, reporting). | 3 and Appendix B |
| Appraisal process | Indicate whether the appraisal was conducted independently by more than one reviewer and if consensus was required. | 3–4 |
| Appraisal results | Present results of the quality assessment and indicate which articles, if any, were weighted/excluded based on the assessment and provide the rationale. | Appendix B |
| Data extraction | Indicate which sections of the primary studies were analyzed and how the data were extracted from the primary studies (e.g., all text under the headings “results/conclusions” were extracted electronically and entered into a computer software). | 3–4 |
| Software | State the computer software used, if any. | 3–4 |
| Number of reviewers | Identify who was involved in coding and analysis. | 3–4 |
| Coding | Describe the process for coding of data (e.g., line-by-line coding to search for concepts). | 3–4 |
| Study comparison | Describe how were comparisons made within and across studies (e.g., subsequent studies were coded into pre-existing concepts, and new concepts were created when deemed necessary). | 3–4 |
| Derivation of themes | Explain whether the process of deriving the themes or constructs was inductive or deductive. | 3–4 |
| Quotations | Provide quotations from the primary studies to illustrate themes/constructs, and identify whether the quotations were participant quotations or the author’s interpretation | 6–8 |
| Synthesis output | Present rich, compelling, and useful results that go beyond a summary of the primary studies (e.g., new interpretation, models of evidence, conceptual models, analytical framework, development of a new theory or construct). | 6–11 |
Appendix B. CASP Quality Assessment
| Author (Year) | 1. Was There a Clear Statement of the Aims of the Research? | 2. Is a Qualitative Methodology Appropriate? | 3. Was the Research Design Appropriate to Address the Aims of the Research? | 4. Was the Recruitment Strategy Appropriate to the Aims of the Research? | 5. Was the Data Collected in a Way that Addressed the Research Issue? | 6. Has the Relationship between Researcher and Participants been Adequately Considered? | 7. Have Ethical Issues Been Taken into Consideration? | 8. Was the Data Analysis Sufficiently Rigorous? | 9. Is There a Clear Statement of Findings? | 10. How Valuable Is the Research? |
| Cochrane et al., 2022 [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Kedia et al., 2015 [21] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Fitch, 2020 [22] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Otty et al., 2023 [23] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Kedia et al., 2018 [24] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Hendriksen et al., 2019 [25] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Schook et al., 2014 [26] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Occhipinti et al., 2018 [27] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Lee et al., 2022 [28] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Ryan et al., 2008 [29] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Mosher et al., 2013 [30] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Mosher et al., 2015 [31] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Xue et al., 2022 [32] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Shilling et al., 2017 [33] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Keimweiss et al., 2023 [34] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Seibel et al., 2023 [35] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
| Sihombing et al., 2019 [36] | Yes | Yes | Yes | Yes | Yes | Cannot tell | Yes | Yes | Yes | Yes |
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA. Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Hirdes, J.P.; Freeman, S.; Smith, T.F.; Stolee, P. Predictors of caregiver distress among palliative home care clients in Ontario: Evidence based on the interRAI Palliative Care. Palliat. Support. Care 2012, 10, 155–163. [Google Scholar] [CrossRef]
- Schubart, J.R.; Kinzie, M.B.; Farace, E. Caring for the brain tumor patient: Family caregiver burden and unmet needs. Neuro-oncology 2008, 10, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Stigimura, H.; Yang, P. Long-term survivorship in lung cancer: A review. Chest 2006, 129, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Girgis, A. Supportive care needs: Are patients with lung cancer a neglected population? Psycho-Oncology 2006, 15, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Shaffer, K.M.; Carver, C.S.; Cannady, R.S. Quality of life of family caregivers 8 years after a relative’s cancer diagnosis: Follow-up of the National Quality of Life Survey for Caregivers. Psycho-Oncology 2016, 25, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Krishnasamy, M.; Wells, M.; Wilkie, E. Patients and carer experiences of care provision after a diagnosis of lung cancer in Scotland. Support. Care Cancer 2007, 15, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Fujinami, R.; Sun, V.; Zachariah, F.; Uman, G.; Grant, M.; Ferrell, B. Family caregivers’ distress levels related to quality of life, burden, and preparedness. Psycho-Oncology 2015, 24, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, A.; Ascherfeld, L.; Marx, G.; Bokemeyer, C.; Bergelt, C.; Oechsle, K. Quality of life, psychological burden, needs, and satisfaction during specialized inpatient palliative care in family caregivers of advanced cancer patients. BMC Palliat. Care 2017, 16, 31. [Google Scholar] [CrossRef]
- Nightingale, C.L.; Steffen, L.E.; Tooze, J.A.; Petty, W.; Danhauer, S.C.; Badr, H.; Weaver, K.E. Lung Cancer Patient and Caregiver Health Vulnerabilities and Interest in Health Promotion Interventions: An Exploratory Study. Glob. Adv. Health Med. 2019, 8, 2164956119865160. [Google Scholar] [CrossRef]
- Jassem, J.; Penrod, J.; Goren, A.; Gilloteau, I. Caring for relatives with lung cancer in Europe: An evaluation of caregivers’ experience. Qual. Life Res. 2015, 24, 2843–2852. [Google Scholar] [CrossRef]
- Northouse, L.L.; Katapodi, M.C.; Song, L.; Zhang, L.; Mood, D.W. Interventions with Family Caregivers of Cancer Patients: Meta-Analysis of Randomized Trials. CA Cancer J. Clin. 2010, 60, 317–339. [Google Scholar] [CrossRef]
- Ferrell, B.; Wittenberg, E. A review of family caregiving intervention trials in oncology. CA. Cancer J. Clin. 2017, 67, 318–325. [Google Scholar] [CrossRef]
- Kedia, S.; Collins, A.; Dillon, P.J.; Akkus, C.; Ward, K.D.; Jackson, B.M. Psychosocial interventions for informal caregivers of lung cancer patients: A systematic review. Psycho-Oncology 2020, 29, 251–262. [Google Scholar] [CrossRef]
- Aubin, M.; Vézina, L.; Verreault, R.; Simard, S.; Desbiens, J.-F.; Tremblay, L.; Dumont, S.; Dogba, M.J.; Gagnon, P. A randomized clinical trial assessing a pragmatic intervention to improve supportive care for family caregivers of patients with lung cancer. Palliat. Support. Care 2021, 19, 146–153. [Google Scholar] [CrossRef]
- Sun, V.; Raz, D.J.; Erhunmwunsee, L.; Ruel, N.; Carranza, J.; Prieto, R.; Ferrell, B.; Krouse, R.S.; McCorkle, R.; Kim, J.Y. Improving family caregiver and patient outcomes in lung cancer surgery: Study protocol for a randomized trial of the multimedia self-management (MSM) intervention. Contemp. Clin. Trials 2019, 83, 88–96. [Google Scholar] [CrossRef]
- Sandelowski, M.; Barroso, J. Handbook for Synthesizing Qualitative Research; Springer Publishing Company: London, UK, 2006. [Google Scholar]
- Thorne, S.; Jensen, L.; Kearney, M.H.; Noblit, G.; Sandelowski, M. Qualitative Metasynthesis: Reflections on Methodological Orientation and Ideological Agenda. Qual. Health Res. 2004, 14, 1342–1365. [Google Scholar] [CrossRef]
- Sandelowski, M. From Meta-Synthesis to Method: Appraising the Qualitative Research Synthesis Report. In Reviewing Research Evidence for Nursing Practice; Blackwell Publishing Ltd.: Oxford, UK, 2007; pp. 88–111. [Google Scholar]
- Cochrane, A.; Gallagher, P.; Dunne, S. “You just need to learn”: A qualitative study on the information needs of family caregivers of people with lung cancer. Eur. J. Oncol. Nurs. 2022, 56, 102082. [Google Scholar] [CrossRef]
- Kedia, S.K.; Ward, K.D.; Digney, S.A.; Jackson, B.M.; Nellum, A.L.; McHugh, L.; Roark, K.S.; Osborne, O.T.; Crossley, F.J.; Faris, N.; et al. ‘One-stop shop’: Lung cancer patients’ and caregivers’ perceptions of multidisciplinary care in a community healthcare setting. Transl. Lung Cancer Res. 2015, 4, 456–464. [Google Scholar]
- Fitch, M.I. Exploring Experiences of Survivors and Caregivers Regarding Lung Cancer Diagnosis, Treatment, and Survivorship. J. Patient Exp. 2020, 7, 193–199. [Google Scholar] [CrossRef]
- Otty, Z.; Brown, A.; Larkins, S.; Evans, R.; Sabesan, S. Patient and carer experiences of lung cancer referral pathway in a regional health service: A qualitative study. Intern. Med. J. 2023, 53, 2016–2027. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Ward, K.; Digney, S.; Jackson, B.; Collins, A.; Rugless Stewart, F.; Faris, N.; Roark, K.; Osarogiagbon, R.U. Qualitative assessment of organizational barriers to optimal lung cancer care in a community hospital setting in the United States. J. Community Support. Oncol 2018, 16, 89–96. [Google Scholar] [CrossRef]
- Hendriksen, E.; Rivera, A.; Williams, E.; Lee, E.; Sporn, N.; Cases, M.G.; Palesh, O. Manifestations of anxiety and coping strategies in patients with metastatic lung cancer and their family caregivers: A qualitative study. Psychol. Health 2019, 34, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Schook, R.M.; Linssen, C.; Schramel, F.M.; Festen, J.; Lammers, E.; Smit, E.F.; Postmus, P.E.; Westerman, M.J. Why do patients and caregivers seek answers from the Internet and online lung specialists? A qualitative study. J. Med. Internet Res. 2014, 16, e37. [Google Scholar] [CrossRef]
- Occhipinti, S.; Dunn, J.; O’Connell, D.; Garvey, G.; Valery, P.; Ball, D.; Fong, K.; Vinod, S.; Chambers, S. Lung Cancer Stigma across the Social Network: Patient and Caregiver Perspectives. J. Thorac. Oncol. 2018, 13, 1443–1453. [Google Scholar] [CrossRef]
- Lee, C.T.; Gonsalves, C.L.; Gao-Kang, J.; Pickrell, W.G.; Barker, R.F. Resource utilization among informal caregiver of lung cancer patients undergoing treatment. Patient Exp. J. 2022, 9, 103–118. [Google Scholar] [CrossRef]
- Ryan, P.; Howell, V.; Jones, J.; Hardy, E. Lung cancer, caring for the caregivers. A qualitative study of providing pro-active social support targeted to the carers of patients with lung cancer. Palliat. Med. 2008, 22, 233–238. [Google Scholar] [CrossRef]
- Mosher, C.E.; Jaynes, H.A.; Hanna, N.; Ostroff, J.S. Distressed family caregivers of lung cancer patients: An examination of psychosocial and practical challenges. Support. Care Cancer 2013, 21, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Mosher, C.E.; Ott, M.A.; Hanna, N.; Jalal, S.I.; Champion, V.L. Coping with physical and psychological symptoms: A qualitative study of advanced lung cancer patients and their family caregivers. Support. Care Cancer 2015, 23, 2053–2060. [Google Scholar] [CrossRef]
- Xue, M.; Chen, X.; Zhao, H.; Zhao, Y.; Li, J.; Chen, W. Understanding the experiences of older caregivers of patients with lung cancer during palliative chemotherapy in China: A qualitative study. Support. Care Cancer 2022, 30, 8011–8018. [Google Scholar] [CrossRef]
- Shilling, V.; Starkings, R.; Jenkins, V.; Fallowfield, L. The pervasive nature of uncertainty—A qualitative study of patients with advanced cancer and their informal caregivers. J. Cancer Surviv. 2017, 11, 590–603. [Google Scholar] [CrossRef] [PubMed]
- Keimweiss, S.; Gurolnick, A.; Grant, S.; Burris, J.; Studts, J.; Lewis-Thames, M. “Just give it to us straight!”: A qualitative analysis of midwestern rural lung cancer survivors and caregivers about survivorship care experiences. J. Cancer Surviv. 2023. [Google Scholar] [CrossRef]
- Seibel, K.; Sauer, B.; Wagner, B.; Becker, G. “Scanxiety” and a sense of control: The perspective of lung cancer survivors and their caregivers on follow-up—A qualitative study. BMC Psychol. 2023, 11, 119. [Google Scholar] [CrossRef]
- Sihombing, Y.; Waluyo, A.; Yona, S. The experience of caring for an advanced lung cancer spouse: Vulnerable journey of caregiving. Enferm. Clin. 2019, 29, 891–896. [Google Scholar] [CrossRef]
- Thiessen, M.; Raffin Bouchal, S.; Tang, P.A.; Sinclair, S. Navigating the Cancer Journey Using Web-Based Information: Grounded Theory Emerging From the Lived Experience of Cancer Patients and Informal Caregivers With Implications for Web-Based Content Design. JMIR Cancer 2023, 9, e41740. [Google Scholar] [CrossRef]
- Kinnane, N.A.; Milne, D.J. The role of the Internet in supporting and informing carers of people with cancer: A literature review. Support. Care Cancer 2010, 18, 1123–1136. [Google Scholar] [CrossRef]
- Washington, K.T.; Craig, K.W.; Parker Oliver, D.; Ruggeri, J.S.; Brunk, S.R.; Goldstein, A.K.; Demiris, G. Family caregivers’ perspectives on communication with cancer care providers. J. Psychosoc. Oncol. 2019, 37, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Kwame, A.; Petrucka, P.M. A literature-based study of patient-centered care and communication in nurse-patient interactions: Barriers, facilitators, and the way forward. BMC Nurs. 2021, 20, 158. [Google Scholar] [CrossRef] [PubMed]
- Palmer Kelly, E.; Meara, A.; Hyer, M.; Payne, N.; Pawlik, T.M. Understanding the Type of Support Offered within the Caregiver, Family, and Spiritual/Religious Contexts of Cancer Patients. J. Pain Symptom Manag. 2019, 58, 56–64. [Google Scholar] [CrossRef]
- Breitbart, W. Spirituality and meaning in supportive care: Spirituality- and meaning-centered group psychotherapy interventions in advanced cancer. Support. Care Cancer 2002, 10, 272–280. [Google Scholar] [CrossRef]
- Edwards, A.; Pang, N.; Shiu, V.; Chan, C. Review: The understanding of spirituality and the potential role of spiritual care in end-of-life and palliative care: A meta-study of qualitative research. Palliat. Med. 2010, 24, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Tuzzio, L.; Berry, A.L.; Gleason, K.; Barrow, J.; Bayliss, E.A.; Gray, M.F.; Delate, T.; Bermet, Z.; Uratsu, C.S.; Grant, R.W.; et al. Aligning care with the personal values of patients with complex care needs. Health Serv. Res. 2021, 56, 1037–1044. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Country | Caregiver Sample Size | Data Collection Method | Analytical Approach |
|---|---|---|---|---|
| Cochrane et al., 2022 [20] | Ireland | 9 | Semi-structured interviews | Thematic analysis |
| Kedia et al., 2015 [21] | USA | 24 | Focus groups | Grounded theory |
| Fitch, 2020 [22] | USA | 4 | Semi-structured interviews | Content analysis |
| Otty et al., 2023 [23] | Australia | 19 | Semi-structured interviews | Thematic analysis |
| Kedia et al., 2018 [24] | USA | 24 | Focus groups | Creswell’s 7-step analysis framework |
| Hendriksen et al., 2019 [25] | USA | 10 | Semi-structured interviews | Grounded theory |
| Schook et al., 2014 [26] | The Netherlands | 20 | Semi-structured interviews | Thematic analysis |
| Occhipinti et al., 2018 [27] | Australia | 12 | Semi-structured interviews | Thematic analysis |
| Lee et al., 2022 [28] | Canada | 20 | Semi-structured interviews | Content analysis |
| Ryan et al., 2008 [29] | UK | 20 | Semi-structured interviews | Thematic analysis |
| Mosher et al., 2013 [30] | USA | 21 | Semi-structured interviews | Thematic analysis |
| Mosher et al., 2015 [31] | USA | 21 | Semi-structured interviews | Thematic analysis |
| Xue et al., 2022 [32] | China | 18 | Semi-structured interviews | Content analysis |
| Shilling et al., 2017 [33] | UK | 6 | Semi-structured interviews | Thematic analysis |
| Keimweiss et al., 2023 [34] | USA | 5 | Semi-structured interviews | Thematic analysis |
| Seibel et al., 2023 [35] | Germany | 17 | Semi-structured interviews | Content analysis |
| Sihombing et al., 2019 [36] | Indonesia | 9 | Semi-structured interviews | Content analysis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tragantzopoulou, P.; Giannouli, V. Echoes of Support: A Qualitative Meta-Synthesis of Caregiver Narratives in Lung Cancer Care. Healthcare 2024, 12, 828. https://doi.org/10.3390/healthcare12080828
Tragantzopoulou P, Giannouli V. Echoes of Support: A Qualitative Meta-Synthesis of Caregiver Narratives in Lung Cancer Care. Healthcare. 2024; 12(8):828. https://doi.org/10.3390/healthcare12080828
Chicago/Turabian StyleTragantzopoulou, Panagiota, and Vaitsa Giannouli. 2024. "Echoes of Support: A Qualitative Meta-Synthesis of Caregiver Narratives in Lung Cancer Care" Healthcare 12, no. 8: 828. https://doi.org/10.3390/healthcare12080828
APA StyleTragantzopoulou, P., & Giannouli, V. (2024). Echoes of Support: A Qualitative Meta-Synthesis of Caregiver Narratives in Lung Cancer Care. Healthcare, 12(8), 828. https://doi.org/10.3390/healthcare12080828