

Impact of a Discontinuous Training Program on Sedentary Behavior in Italian Type 2 Diabetes Older Patients: The Results of the TRIPL-A Randomized Controlled Trial

 ,
,  , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Material and Methods
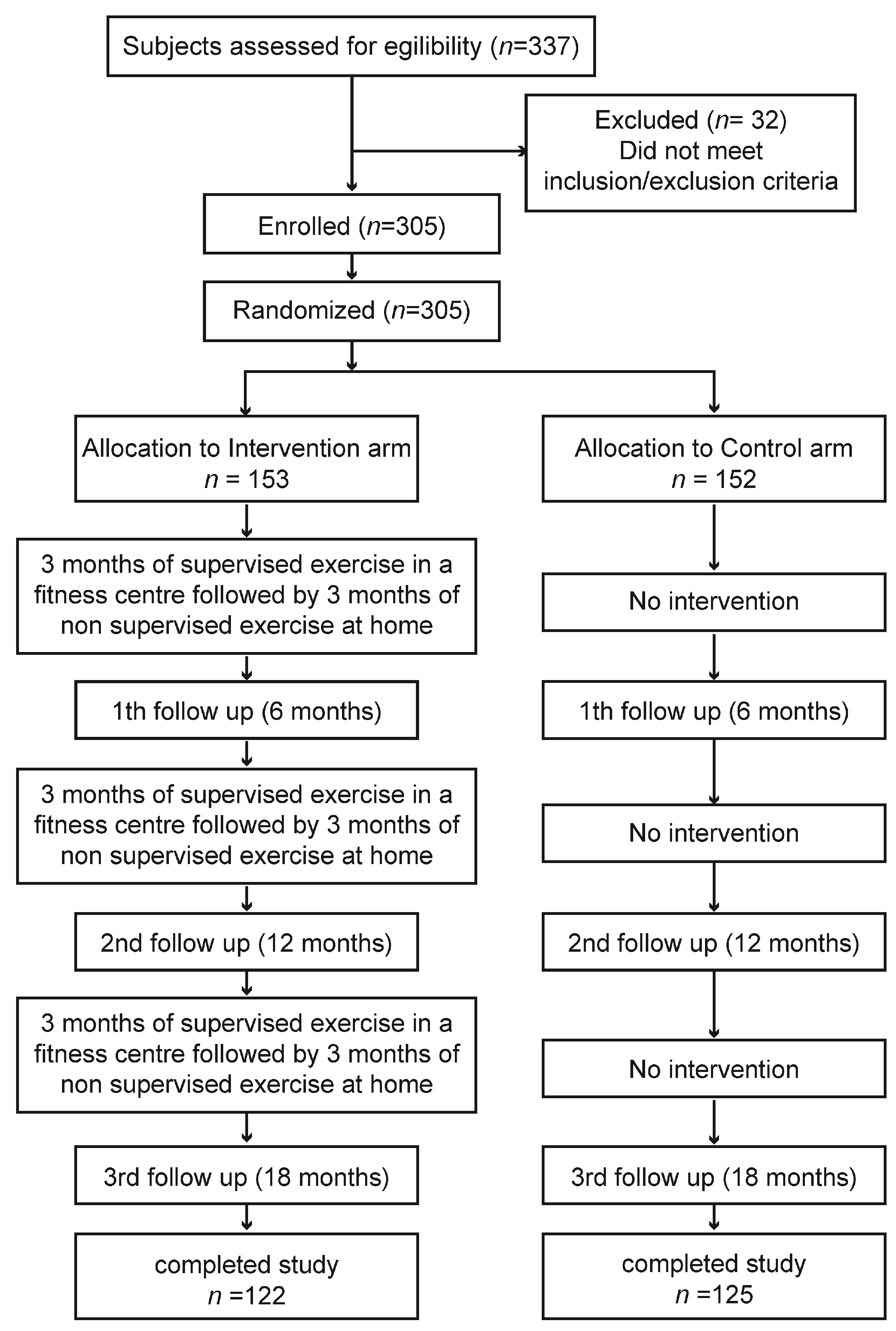
2.1. Study Design
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
- Receiving any drug that could affect heart rate, such as β-blockers.
- Chronic obstructive pulmonary disease.
- Severe cardiovascular disease (including New York Heart Association class III or IV congestive heart failure), clinically significant valvular disease, history of cardiac arrest, presence of an implantable defibrillator, or uncontrolled angina.
- History of myocardial infarction, transient ischemic attack, or stroke in the six months before enrolment.
- Life expectancy <6 months.
- A condition that might harm the subjects’ health during the participation in the trial.
2.3. Intervention
2.3.1. Intervention Arm
2.3.2. Control Arm
2.4. Outcome Measures
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
- Evaluation of physical performance by Long Distance Corridor Walk (LDCW) test [33]. The test has also been validated for estimating maximum oxygen consumption (VO2max) in the 60–91 age group. The test includes a first warm-up phase of 2 min and a second phase in which the subject is asked to walk as fast as possible, back and forth, in a 20 m long path, for 400 m.
- Fasting glucose, HbA1c.
- Body mass index (BMI = Kg/m2), waist and hip circumference, systolic and diastolic blood pressure (mmHg), resting heart rate (beats/min).
- Quality of life is measured using the Euro-QoL Index (EQ-5D-5L) [34].
- Sleep–wake disturbances are measured by the Pittsburgh Sleep Quality Index (PSQI) [35].
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Billot, M.; Calvani, R.; Urtamo, A.; Sanchez-Sanchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [PubMed]
- Rice, N.E.; Lang, I.A.; Henley, W.; Melzer, D. Baby boomers nearing retirement: The healthiest generation? Rejuvenation Res. 2010, 13, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Torres, S.; Fahey, T.D.; Rivera, M.A. Adherence to Exercise Programs in Older Adults: Informative Report. Gerontol. Geriatr. Med. 2019, 5, 2333721418823604. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of change. J. Clin. Psychol. 2011, 67, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef]
- Espinoza, M.A.; Abbott, T.; Passi, A.; Balmaceda, C. Health and economic effects on patients with type 2 diabetes mellitus in the long run: Predictions for the Chilean population. Diabetol. Metab. Syndr. 2022, 14, 155. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Lu, J.; Yoong, S.Q.; Tan, Y.Q.; Kusuyama, J.; Wu, X.V. Effect of Aerobic and Resistant Exercise Intervention on Inflammaging of Type 2 Diabetes Mellitus in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2022, 23, 823–830.e13. [Google Scholar] [CrossRef]
- Annibalini, G.; Lucertini, F.; Agostini, D.; Vallorani, L.; Gioacchini, A.; Barbieri, E.; Guescini, M.; Casadei, L.; Passalia, A.; Del Sal, M.; et al. Concurrent Aerobic and Resistance Training Has Anti-Inflammatory Effects and Increases Both Plasma and Leukocyte Levels of IGF-1 in Late Middle-Aged Type 2 Diabetic Patients. Oxid. Med. Cell Longev. 2017, 2017, 3937842. [Google Scholar] [CrossRef]
- American Diabetes Association. 4. Foundations of care: Education, nutrition, physical activity, smoking cessation, psychosocial care, and immunization. Diabetes Care 2015, 38 (Suppl. S1), S20–S30. [Google Scholar] [CrossRef]
- Rajado, A.T.; Silva, N.; Esteves, F.; Brito, D.; Binnie, A.; Araujo, I.M.; Nobrega, C.; Braganca, J.; Castelo-Branco, P.; Consortium, A.S. How can we modulate aging through nutrition and physical exercise? An epigenetic approach. Aging 2023, 15, 3191–3217. [Google Scholar] [CrossRef] [PubMed]
- Antonicelli, R.; Spazzafumo, L.; Scalvini, S.; Olivieri, F.; Matassini, M.V.; Parati, G.; Del Sindaco, D.; Gallo, R.; Lattanzio, F. Exercise: A “new drug” for elderly patients with chronic heart failure. Aging 2016, 8, 860–872. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Friedenreich, C.M.; Leitzmann, M.F.; Buman, M.P.; Lambert, E.; Willumsen, J.; Bull, F. Global Public Health Guidelines on Physical Activity and Sedentary Behavior for People Living With Chronic Conditions: A Call to Action. J. Phys. Act. Health 2021, 18, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.R.; Francis, D.P.; Soares, J.; Weightman, A.L.; Foster, C. Community wide interventions for increasing physical activity. Cochrane Database Syst. Rev. 2015, 1, CD008366. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.; Ritter, P.L.; Villa, F.J.; Armas, J. Community-based peer-led diabetes self-management: A randomized trial. Diabetes Educ. 2009, 35, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, H.; Siersma, V.; Olivarius, N.F. Fitness consultations in routine care of patients with type 2 diabetes in general practice: An 18-month non-randomised intervention study. BMC Fam. Pract. 2010, 11, 83. [Google Scholar] [CrossRef] [PubMed]
- Avery, L.; Flynn, D.; van Wersch, A.; Sniehotta, F.F.; Trenell, M.I. Changing physical activity behavior in type 2 diabetes: A systematic review and meta-analysis of behavioral interventions. Diabetes Care 2012, 35, 2681–2689. [Google Scholar] [CrossRef] [PubMed]
- Anokye, N.K.; Trueman, P.; Green, C.; Pavey, T.G.; Hillsdon, M.; Taylor, R.S. The cost-effectiveness of exercise referral schemes. BMC Public Health 2011, 11, 954. [Google Scholar] [CrossRef] [PubMed]
- Pavey, T.G.; Taylor, A.H.; Fox, K.R.; Hillsdon, M.; Anokye, N.; Campbell, J.L.; Foster, C.; Green, C.; Moxham, T.; Mutrie, N.; et al. Effect of exercise referral schemes in primary care on physical activity and improving health outcomes: Systematic review and meta-analysis. BMJ 2011, 343, d6462. [Google Scholar] [CrossRef]
- Ingram, W.; Webb, D.; Taylor, R.S.; Anokye, N.; Yardley, L.; Jolly, K.; Mutrie, N.; Campbell, J.L.; Dean, S.G.; Greaves, C.; et al. Multicentred randomised controlled trial of an augmented exercise referral scheme using web-based behavioural support in individuals with metabolic, musculoskeletal and mental health conditions: Protocol for the e-coachER trial. BMJ Open 2018, 8, e022382. [Google Scholar] [CrossRef]
- Jennings, C.A.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Effectiveness of a web-based physical activity intervention for adults with Type 2 diabetes-a randomised controlled trial. Prev. Med. 2014, 60, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.P.; Durant, N.; Agne, A.A.; Cherrington, A.L. Internet interventions to support lifestyle modification for diabetes management: A systematic review of the evidence. J. Diabetes Complicat. 2014, 28, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Lucertini, F.; Ferri Marini, C.; Sisti, D.; Stocchi, V.; Federici, A.; Gregorio, F.; Piangerelli, D.; Chiatti, C.; Cherubini, A.; Boemi, M.; et al. Discontinuously supervised aerobic training vs. physical activity promotion in the self-management of type 2 diabetes in older Italian patients: Design and methods of the ‘TRIPL-A’ randomized controlled trial. BMC Geriatr. 2019, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Klaren, R.E.; Hubbard, E.A.; Motl, R.W. Efficacy of a behavioral intervention for reducing sedentary behavior in persons with multiple sclerosis: A pilot examination. Am. J. Prev. Med. 2014, 47, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Segura-Jimenez, V.; Munguia-Izquierdo, D.; Camiletti-Moiron, D.; Alvarez-Gallardo, I.C.; Ortega, F.B.; Ruiz, J.R.; Delgado-Fernandez, M. Comparison of the International Physical Activity Questionnaire (IPAQ) with a multi-sensor armband accelerometer in women with fibromyalgia: The al-Andalus project. Clin. Exp. Rheumatol. 2013, 31, S94–S101. [Google Scholar]
- Tomioka, K.; Iwamoto, J.; Saeki, K.; Okamoto, N. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) in elderly adults: The Fujiwara-kyo Study. J. Epidemiol. 2011, 21, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Tran, D.V.; Lee, A.H.; Au, T.B.; Nguyen, C.T.; Hoang, D.V. Reliability and validity of the International Physical Activity Questionnaire-Short Form for older adults in Vietnam. Health Promot. J. Austr 2013, 24, 126–131. [Google Scholar] [CrossRef] [PubMed]
- WHO. Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; WHO: Geneva, Switzerland, 2004; Volume 1. [Google Scholar]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal modeling of the relationship between age and maximal heart rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef]
- Gunnar, B. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998; Volume 104. [Google Scholar]
- Motl, R.W.; Sasaki, J.E.; Cederberg, K.L.; Jeng, B. Validity of sitting time scores from the International Physical Activity Questionnaire-Short Form in multiple sclerosis. Rehabil. Psychol. 2019, 64, 463–468. [Google Scholar] [CrossRef]
- Simonsick, E.M.; Montgomery, P.S.; Newman, A.B.; Bauer, D.C.; Harris, T. Measuring fitness in healthy older adults: The Health ABC Long Distance Corridor Walk. J. Am. Geriatr. Soc. 2001, 49, 1544–1548. [Google Scholar] [CrossRef]
- Thiel, D.M.; Al Sayah, F.; Vallance, J.K.; Johnson, S.T.; Johnson, J.A. Association between Physical Activity and Health-Related Quality of Life in Adults with Type 2 Diabetes. Can. J. Diabetes 2017, 41, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martin, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- Foong, Y.C.; Aitken, D.; Winzenberg, T.; Otahal, P.; Scott, D.; Jones, G. The association between physical activity and reduced body fat lessens with age—Results from a cross-sectional study in community-dwelling older adults. Exp. Gerontol. 2014, 55, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Creber, A.; Leo, D.G.; Buckley, B.J.R.; Chowdhury, M.; Harrison, S.L.; Isanejad, M.; Lane, D.A.; TAILOR investigators. Use of telemonitoring in patient self-management of chronic disease: A qualitative meta-synthesis. BMC Cardiovasc. Disord. 2023, 23, 469. [Google Scholar] [CrossRef] [PubMed]
- Alothman, S.; Yahya, A.; Rucker, J.; Kluding, P.M. Effectiveness of Interventions for Promoting Objectively Measured Physical Activity of Adults With Type 2 Diabetes: A Systematic Review. J. Phys. Act. Health 2017, 14, 408–415. [Google Scholar] [CrossRef]
- Raihan, N.; Cogburn, M. Stages of Change Theory; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Hayes, A.M.; Laurenceau, J.P.; Feldman, G.; Strauss, J.L.; Cardaciotto, L. Change is not always linear: The study of nonlinear and discontinuous patterns of change in psychotherapy. Clin. Psychol. Rev. 2007, 27, 715–723. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports, M.; et al. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef]
- Gagliardi, C.; Santini, S.; Piccinini, F.; Fabbietti, P.; di Rosa, M. A pilot programme evaluation of social farming horticultural and occupational activities for older people in Italy. Health Soc. Care Community 2019, 27, 207–214. [Google Scholar] [CrossRef]
- Morowatisharifabad, M.A.; Abdolkarimi, M.; Asadpour, M.; Fathollahi, M.S.; Balaee, P. Study on Social Support for Exercise and Its Impact on the Level of Physical Activity of Patients with Type 2 Diabetes. Open Access Maced. J. Med. Sci. 2019, 7, 143–147. [Google Scholar] [CrossRef]
- Reynolds, C.F., 3rd; Jeste, D.V.; Sachdev, P.S.; Blazer, D.G. Mental health care for older adults: Recent advances and new directions in clinical practice and research. World Psychiatry 2022, 21, 336–363. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Period 1 | Period 2 | Period 3 | Period 4 | Period 5 | Period 6 | |
|---|---|---|---|---|---|---|
| S | NS | S | NS | S | NS | |
| Intensity (%HRR range) | 40–50 | 50 | 45–55 | 55 | 50–60 | 60 |
| Duration (minute range) | 20–30 | 30 | 30–40 | 40 | 40–50 | 50 |
| Variable | Total (n = 305) | Control (n = 152) | Intervention (n = 153) | p |
|---|---|---|---|---|
| Gender female, n (%) | 164 (53.8) | 89 (58.6) | 75 (49.0) | 0.095 |
| Age, mean ± SD | 68.7 ± 4.1 | 68.5 ± 4.8 | 68.8 ± 3.3 | 0.650 |
| Study degree, n (%) | 0.707 | |||
| Primary school diploma | 88 (28.9) | 42 (27.7) | 46 (30.3) | |
| Middle school diploma | 81 (26.4) | 46 (30.1) | 34 (22.4) | |
| High school diploma | 119 (39.0) | 55 (36.1) | 64 (42.1) | |
| University degree | 17 (5.7) | 9 (6.0) | 8 (5.3) | |
| Older adults can reach TRIPL-A gym independently by car, n (%) | 264 (86.7) | 127 (83.8) | 137 (89.5) | 0.147 |
| Body mass index (kg/m2), mean ± SD | 29.6 ± 6.0 | 29.6 ± 7.1 | 29.6 ± 4.7 | 0.975 |
| Systolic blood pressure (mm/Hg), mean ± SD | 135.2 ± 16.6 | 136.5 ± 18.2 | 133.9 ± 14.9 | 0.185 |
| Diastolic blood pressure (mm/Hg), mean ± SD | 74.7 ± 8.4 | 74.4 ± 8.9 | 75.0 ± 7.9 | 0.583 |
| Heart rate (bpm), mean ± SD | 76.0 ± 12.4 | 75.3 ± 11.7 | 76.6 ± 13.0 | 0.363 |
| Waist circumference (cm), mean ± SD | 104.2 ± 13.6 | 104.1 ± 14.0 | 104.2 ± 13.4 | 0.940 |
| Hip circumference (cm), mean ± SD | 108.8 ± 14.4 | 108.9 ± 15.4 | 108.7 ± 13.3 | 0.911 |
| Arm circumference (cm), mean ± SD | 30.4 ± 3.7 | 30.3 ± 3.7 | 30.6 ± 3.6 | 0.556 |
| Calf circumference (cm), mean ± SD | 37.1 ± 4.1 | 36.9 ± 4.2 | 37.4 ± 4.1 | 0.285 |
| Fasting glucose, (mg/dL), mean ± SD | 135.1 ± 41.3 | 136.2 ± 34.5 | 134.3 ± 36.7 | 0.832 |
| Hba1c, (%), mean ± SD | 7.2 ± 1.4 | 7.1 ± 1.5 | 7.3 ± 1.1 | 0.281 |
| Total cholesterol, (mg/dL), mean ± SD | 170.7 ± 32.5 | 165.5 ± 34.9 | 177.1 ± 28.4 | 0.059 |
| Joint pain, n (%) | 141 (46.2) | 70 (46.1) | 71 (46.4) | 0.951 |
| Pain in the lower limbs, n (%) | 108 (35.4) | 61 (40.1) | 47 (30.7) | 0.086 |
| Age when T2D was diagnosed? mean ± SD | 55.8 ± 14.0 | 55.7 ± 13.8 | 55.8 ± 14.2 | 0.933 |
| Liver disease, n (%) | 6 (2.0) | 4 (2.7) | 2 (1.3) | 0.400 |
| Hypercholesterolemia, n (%) | 122 (40.1) | 61 (40.0) | 61 (40.1) | 0.981 |
| History of cancer, n (%) | 10 (3.3) | 4 (2.7) | 6 (4.0) | 0.534 |
| Hypertension, n (%) | 170 (55.6) | 94 (62.0) | 75 (49.3) | 0.031 |
| Osteoarthritis/Osteoporosis, n (%) | 16 (5.3) | 9 (6.0) | 7 (4.6) | 0.588 |
| History of femur fracture, n (%) | 4 (1.3) | 2 (1.3) | 2 (1.3) | 0.989 |
| Retinopathy, n (%) | 39 (12.9) | 25 (16.7) | 14 (9.2) | 0.053 |
| Peripheral vascular disease, n (%) | 13 (4.3) | 10 (6.7) | 3 (2.0) | 0.082 |
| Nephropathy, n (%) | 12 (4.0) | 9 (6.0) | 3 (2.0) | 0.073 |
| Chronic kidney disease, n (%) | 6 (2.0) | 5 (3.3) | 1 (0.7) | 0.096 |
| Smoke, n (%) | 0.882 | |||
| ex | 134 (43.9) | 67 (44.1) | 67 (43.6) | |
| no | 124 (40.5) | 60 (39.3) | 64 (41.6) | |
| yes | 48 (15.7) | 25 (16.6) | 23 (14.8) | |
| EQ-5D-5L | ||||
| Movement ability problems, n (%) | 51 (16.7) | 31 (20.1) | 20 (13.3) | 0.115 |
| Personal care problems, n (%) | 13 (4.4) | 8 (5.4) | 5 (3.3) | 0.381 |
| Problems with usual activities, n (%) | 30 (9.7) | 17 (11.4) | 13 (8.7) | 0.430 |
| Pain or discomfort, n (%) | 136 (44.5) | 70 (47.0) | 66 (43.7) | 0.569 |
| Anxiety or depression, n (%) | 109 (35.9) | 58 (38.1) | 52 (33.8) | 0.440 |
| State of health today, mean ± SD | 73.2 ± 15.0 | 73.0 ± 15.1 | 73.5 ± 14.8 | 0.770 |
| PSQI, mean ± SD | 6.0 ± 3.4 | 6.2 ± 3.7 | 5.8 ± 2.9 | 0.315 |
| LDCW time, mean ± SD | 325.1 ± 64.0 | 331.4 ± 65.2 | 315.7 ± 61.4 | 0.071 |
| LDCW VO2max, mean ± SD | 17.1 ± 3.8 | 16.8 ± 3.9 | 17.2 ± 3.3 | 0.079 |
| Baseline | 6th Months | 12th Months | 18th Months | F | p Group | F | p Time | F | p Interaction | |
|---|---|---|---|---|---|---|---|---|---|---|
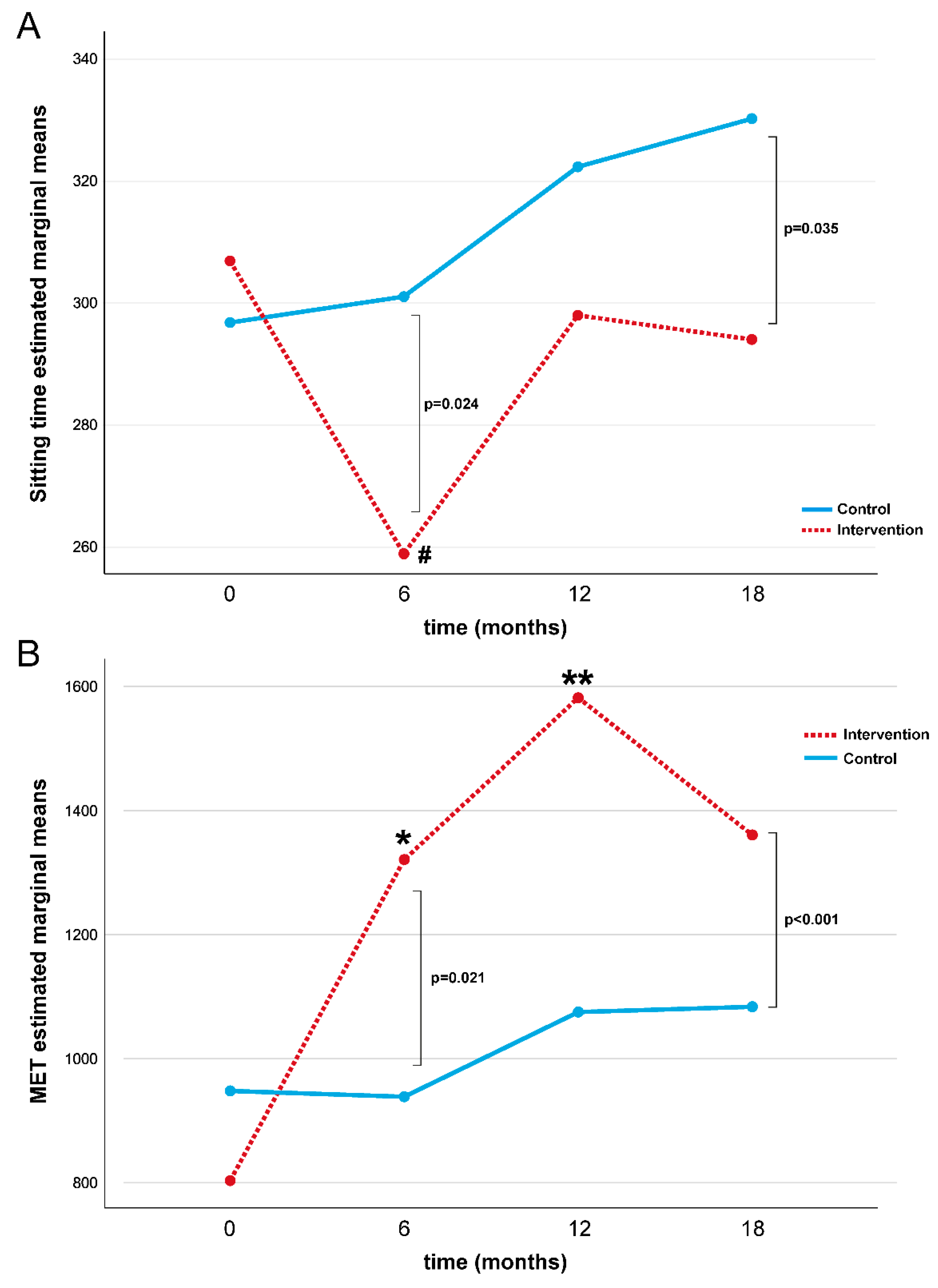
| ST (min) | 2.063 | 0.152 | 7.831 | <0.001 | 3.099 | 0.028 | ||||
| Intervention | 306.8 (164.6) | 251.0 (107.5) | 273.6 (108.5) | 283.1 (103.0) | ||||||
| Control | 296.7 (180.5) | 301.5 (158.5) | 323.0 (171.2) | 331.3 (143.3) | ||||||
| MET (min/week) | 8.218 | 0.005 | 16.471 | <0.001 | 4.670 | 0.004 | ||||
| Intervention | 803.3 (967.2) | 1321.2 (1183.9) | 1581.6 (1404.2) | 1360.9 (1117.1) | ||||||
| Control | 948.1 (1124.2) | 938.6 (1065.2) | 1075.3 (1149.5) | 1083.8 (1296.3) |
| Baseline | 6th Month | 12th Month | 18th Month | F | p Group | F | p Time | F | p Interaction | |
|---|---|---|---|---|---|---|---|---|---|---|
| Glucose (mg/dL) | 3.351 | 0.068 | 4.962 | 0.002 | 1.251 | 0.292 | ||||
| Intervention | 140.7 (30.5) | 144.4 (36.9) | 134.2 (36.3) | 133.1 (28.4) | ||||||
| Control | 134.9 (27.4) | 130.6 (26.8) | 133.3 (27.2) | 129.2 (24.7) | ||||||
| HbA1c (%) | 0.905 | 0.342 | 5.063 | 0.002 | 0.998 | 0.394 | ||||
| Intervention | 7.3 (1.1) | 7.0 (1.0) | 7.0 (1.0) | 7.1 (1.0) | ||||||
| Control | 7.1 (1.0) | 7.0 (1.0) | 7.0 (1.0) | 7.0 (0.9) | ||||||
| LDCW time | 1.137 | 0.290 | 0.988 | 0.403 | 0.876 | 0.458 | ||||
| Intervention | 318.7 ± 60.7 | 304.9 ± 43.0 | 306.8 ± 46.3 | 301.1 ± 42.5 | ||||||
| Control | 332.6 ± 67.1 | 321.3 ± 48.0 | 325.5 ± 41.8 | 326.7 ± 50.4 | ||||||
| LDCW VO2max | 1.311 | 0.311 | 2.110 | 0.115 | 0.175 | 0.913 | ||||
| Intervention | 17.5 ± 3.6 | 18.2 ± 2.4 | 18.0 ± 2.7 | 18.4 ± 2.4 | ||||||
| Control | 16.6 ± 4.0 | 17.3 ± 2.8 | 17.0 ± 2.5 | 16.5 ± 2.1 | ||||||
| PSQI | 0.997 | 0.997 | 0.733 | 0.534 | 0.406 | 0.749 | ||||
| Intervention | 5.8 ± 2.9 | 6.0 ± 3.2 | 6.2 ± 3.4 | 6.5 ± 3.1 | ||||||
| Control | 6.2 ± 3.7 | 5.7 ± 3.4 | 6.1 ± 3.5 | 6.0 ± 3.2 | ||||||
| EQ-5D-5L | 1.282 | 0.280 | 1.303 | 0.274 | 0.696 | 0.555 | ||||
| Intervention | 73.5 ± 14.6 | 74.0 ± 15.0 | 71.5 ± 17.2 | 75.5 ± 13.5 | ||||||
| Control | 73.0 ± 15.1 | 72.4 ± 16.0 | 71.1 ± 16.7 | 71.0 ± 14.7 |
| Women (n = 164) | Excluding Subjects with Diabetic Complications (n = 167) | Excluding Subjects with Hypertension (n = 96) | ||||
|---|---|---|---|---|---|---|
| F | p Value | F | p Value | F | p Value | |
| ST (min) | ||||||
| Group | 0.404 | 0.526 | 0.238 | 0.626 | 0.211 | 0.647 |
| Time | 5.267 | 0.002 | 6.681 | <0.001 | 4.141 | 0.007 |
| Interaction | 2.688 | 0.049 | 3.326 | 0.020 | 2.677 | 0.048 |
| MET (min/week) | ||||||
| Group | 7.205 | 0.008 | 3.369 | 0.020 | 2.300 | 0.133 |
| Time | 17.818 | <0.001 | 13.824 | <0.001 | 6.716 | <0.001 |
| Interaction | 2.839 | 0.041 | 6.100 | 0.014 | 2.825 | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonfigli, A.R.; Gagliardi, C.; Protic, O.; Lamedica, A.M.; Luconi, M.P.; Turchi, F.; Tortato, E.; Di Rosa, M.; Lucertini, F.; Spazzafumo, L. Impact of a Discontinuous Training Program on Sedentary Behavior in Italian Type 2 Diabetes Older Patients: The Results of the TRIPL-A Randomized Controlled Trial. Healthcare 2024, 12, 848. https://doi.org/10.3390/healthcare12080848
Bonfigli AR, Gagliardi C, Protic O, Lamedica AM, Luconi MP, Turchi F, Tortato E, Di Rosa M, Lucertini F, Spazzafumo L. Impact of a Discontinuous Training Program on Sedentary Behavior in Italian Type 2 Diabetes Older Patients: The Results of the TRIPL-A Randomized Controlled Trial. Healthcare. 2024; 12(8):848. https://doi.org/10.3390/healthcare12080848
Chicago/Turabian StyleBonfigli, Anna Rita, Cristina Gagliardi, Olga Protic, Adrianapia Maria Lamedica, Maria Paola Luconi, Federica Turchi, Elena Tortato, Mirko Di Rosa, Francesco Lucertini, and Liana Spazzafumo. 2024. "Impact of a Discontinuous Training Program on Sedentary Behavior in Italian Type 2 Diabetes Older Patients: The Results of the TRIPL-A Randomized Controlled Trial" Healthcare 12, no. 8: 848. https://doi.org/10.3390/healthcare12080848
APA StyleBonfigli, A. R., Gagliardi, C., Protic, O., Lamedica, A. M., Luconi, M. P., Turchi, F., Tortato, E., Di Rosa, M., Lucertini, F., & Spazzafumo, L. (2024). Impact of a Discontinuous Training Program on Sedentary Behavior in Italian Type 2 Diabetes Older Patients: The Results of the TRIPL-A Randomized Controlled Trial. Healthcare, 12(8), 848. https://doi.org/10.3390/healthcare12080848