

Effects of Neuropilates on Functional Outcomes in Chronic Stroke: A Randomized Clinical Trial
 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Measures
2.4.1. General Medical Information
2.4.2. Functional Outcomes
- Functional Independence Measure (FIM) [12] was used to assess functional independence of activities of daily living, and it was the main outcome. It comprises 18 items regarding motor and cognitive daily performance. The score ranges from 1 to 7, with a higher score indicating a higher level of functional independence. Administration was carried out through task observation (eating, grooming, bathing, dressing—upper body, dressing—lower body, toileting, transfers between bed, chair, and wheelchair, toilet, tub/shower, walk and stairs) and an interview (bladder management, bowel management, auditory comprehension, verbal expression, social memory). The minimal clinically important difference values for the FIM in patients post-stroke are 22, 17 and 3 for the total FIM, motor FIM and cognitive FIM, respectively [13].
- Functional Reach Test (FRT) [14] was used to measure the maximum distance an individual can move their gravity towards the limits of their support area (i.e., static balance). In a relaxed standing posture, with the feet at hip height, the person is instructed to do a shoulder flexion up to 90 degrees and to keep the hand extended. The person must go forward as much as they can, and the examiner then records the final distance in centimeters. Two preliminary practice trials were administered to each participant preceding the performance of three FRT trials. The final score was determined by calculating the mean score derived from the three trials.
- Timed ‘Up and Go’ (TUG) [15] was used to measure overall balance and gait speed. The person is asked to get up from a chair, walk 3 m, turn, return to the chair and sit down. The final score is recorded in seconds, with a higher score indicative of a diminished balance.
2.4.3. Upper Limb Performance Outcomes
- Nine Hole Peg Test (NHPT) [16] was used to assess manual dexterity as it is considered a gold-standard test for this outcome. Each participant was asked to place nine pegs on a board with 9 holes and to remove them again, as quickly as possible. The final score is recorded in seconds, with a higher score being indicative of a diminished manual dexterity. Each hand was scored separately.
- Box and Block Test (BBT) [17] was used to assess overall upper limb gross motor performance. It is composed of a wooden box divided in two compartments by a partition, one of which contains 150 wooden blocks. Each participant was asked to move, one by one, as many wooden blocks as possible from one compartment to the other within 60 s. Scores were based on the number of blocks transferred, with higher scores being indicative of a better upper limb performance. Each arm was scored separately.
- Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) [18] was used to assess daily activity and participation according to the 9 domains described in the International Classification of Upper Limb Functioning, Disability, and Health.
2.4.4. Secondary Outcomes
2.5. Statiscal Analysis
3. Results
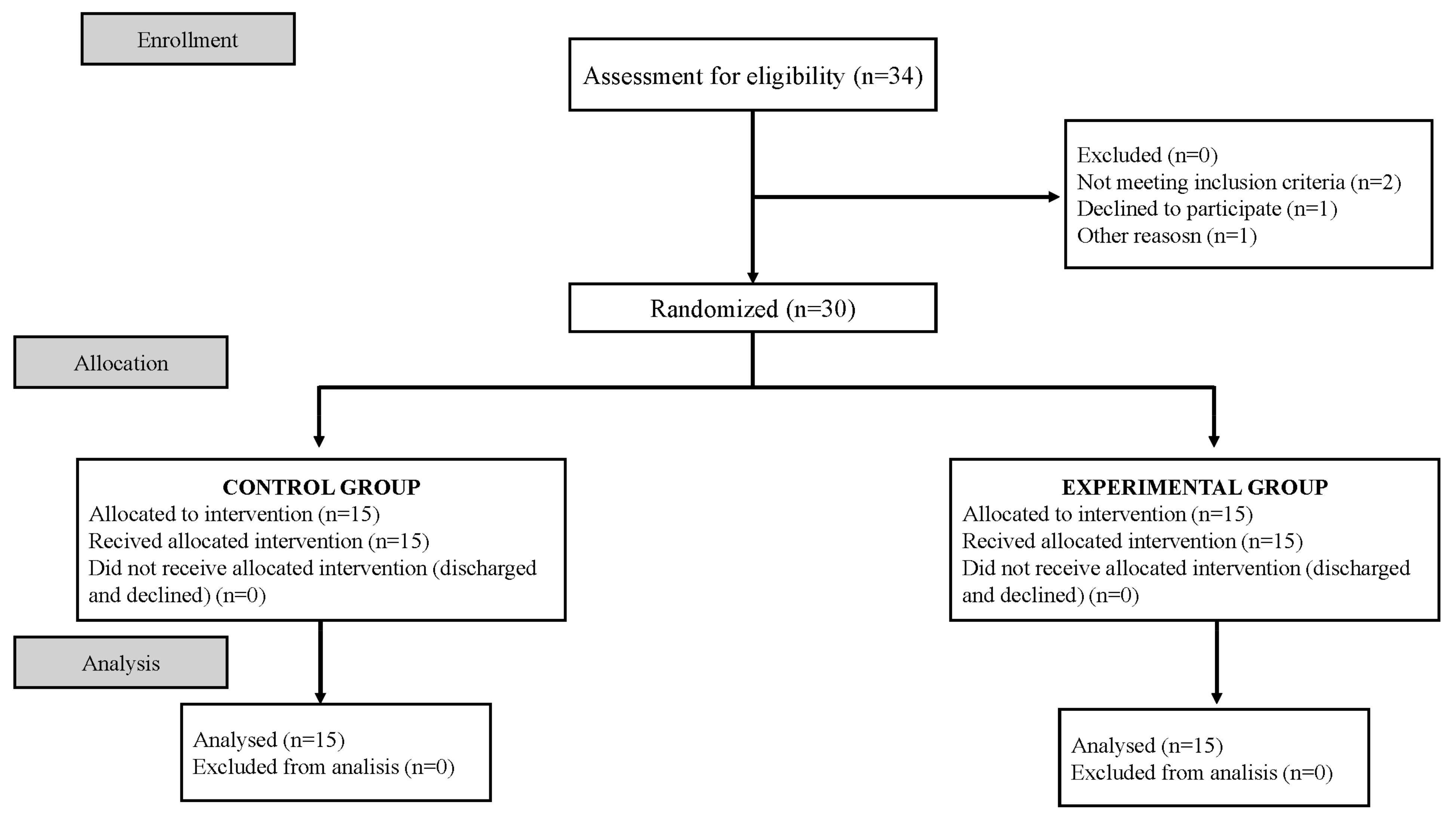
3.1. Attrition Rate
3.2. Baseline Characteristics of Participants
3.3. Effects of the Intervention
Primary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wells, C.; Kolt, G.S.; Bialocerkowski, A. Defining Pilates exercise: A systematic review. Complement. Ther. Med. 2012, 20, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Walter, A.A.; Van Puymbroeck, M.; Bosch, P.; Schmid, A.A. Complementary and integrative health interventions in post-stroke rehabilitation: A systematic PRISMA review. Disabil. Rehabil. 2022, 44, 2223–2232. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, K.; Wu, P.J.; Whillier, S. Is Pilates an effective rehabilitation tool? A systematic review. J. Bodyw. Mov. Ther. 2018, 22, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Cronin, E.; Broderick, P.; Clark, H.; Monaghan, K. What are the effects of pilates in the post stroke population? A systematic literature review & meta-analysis of randomised controlled trials. J. Bodyw. Mov. Ther. 2023, 33, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Withers, G. Modified Pilates Rehabilitation Programme (Manual) Pilates and Neurology. 2009. [Google Scholar]
- Cronin, E.; Monaghan, K. Online neuropilates classes in chronic stroke patients: Protocol for a randomised controlled feasibility study. Contemp. Clin. Trials Commun. 2023, 32, 101068. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Tater, P.; Pandey, S. Post-stroke Movement Disorders: Clinical Spectrum, Pathogenesis, and Management. Neurol. India 2021, 69, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel grouprandomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The global deterioration scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [CrossRef]
- Guillaumesa, S.; O’Callaghanb, C.A. Spanish version of the free OxMaR software for minimization and randomization of clinical trials. Gac. Sanit. 2019, 33, 395–397. [Google Scholar] [CrossRef]
- Martínez-Martín, P.; Fernández-Mayoralas, G.; Frades-Payo, B.; Rojo-Pérez, F.; Petidier, R.; Rodríguez-Rodríguez, V.; Forjaz, M.J.; Prieto-Flores, M.E.; de Pedro-Cuesta, J. Validation of the functional independence scale. Gac. Sanit. 2009, 23, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Beninato, M.; Gill-Body, K.M.; Salles, S.; Stark, P.C.; Black-Schaffer, R.M.; Stein, J. Determination of the minimal clinically important difference in the FIM instrument in patients with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Omaña, H.; Bezaire, K.; Brady, K.; Davies, J.; Louwagie, N.; Power, S.; Santin, S.; Hunter, S.W. Functional Reach Test, Single-Leg Stance Test, and Tinetti Performance-Oriented Mobility Assessment for the Prediction of Falls in Older Adults: A Systematic Review. Phys. Ther. 2021, 101, pzab173. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Fantino, B.; Allali, G.; Muir, S.W.; Montero-Odasso, M.; Annweiler, C. Timed Up and Go test and risk of falls in older adults: A systematic review. J. Nutr. Health Aging 2011, 15, 933–938. [Google Scholar] [CrossRef]
- Moreno-Morente, G.; Hurtado-Pomares, M.; Terol Cantero, M.C. Bibliometric Analysis of Research on the Use of the Nine Hole Peg Test. Int. J. Environ. Res. Public Health 2022, 19, 10080. [Google Scholar] [CrossRef] [PubMed]
- Huertas-Hoyas, E.; Martínez-Piédrola, R.; Sánchez-Herrera-Baeza, P.; Tejeda, S.S.; Máximo-Bocanegra, N.; Camarero, C.S.; Pérez-De-Heredia-Torres, M.; Castrillo, J.M. Alterations in dexterity and manual function in patients with focal hand dystonia. Neurología 2023, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- De Klerk, S.; Buchanan, H.; Jerosch-Herold, C. The validity and clinical utility of the Disabilities of the Arm Shoulder and Hand questionnaire for hand injuries in developing country contexts: A systematic review. J. Hand Ther. 2018, 31, 80–90.e1. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Atrkisson, C.C.; Mendias, R.M. Assessing the client satisfaction questionnaire in English and Spanish. Hisp. J. Behav. Sci. 1984, 6, 385–396. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Otero, P.; Blanco, V.; Attkisson, C.C. Psychometric properties of the Castilian Spanish version of the Client Satisfaction Questionnaire (CSQ-8). Curr. Psychol. 2019, 38, 829–835. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Assessing normal distribution using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef]
- Van Duijnhoven, H.J.R.; Heeren, A.; Peters, M.A.M.; Veerbeek, J.M.; Kwakkel, G.; Geurts, A.C.H.; Weerdesteyn, V. Effects of Exercise Therapy on Balance Capacity in Chronic Stroke: Systematic Review and Meta-Analysis. Stroke 2016, 47, 2603–2610. [Google Scholar] [CrossRef]
- Suputtitada, A.; Suwanwela, N.C.; Tumvitee, S. Effectiveness of constraint-induced movement therapy in chronic stroke patients. J. Med. Assoc. Thail. 2004, 87, 1482–1490. [Google Scholar]
- Díaz-Arribas, M.J.; Martín-Casas, P.; Cano-de-la-Cuerda, R.; Plaza-Manzano, G. Effectiveness of the Bobath concept in the treatment of stroke: A systematic review. Disabil. Rehabil. 2020, 42, 1636–1649. [Google Scholar] [CrossRef]
- Nawaz Malik, A.; Tariq, H.; Afridi, A.; Azam Rathore, F. Technological advancements in stroke rehabilitation. J. Pak. Med. Assoc. 2022, 72, 1672–1674. [Google Scholar]
- Yun, S.M.; Park, S.K.; Sung Lim, H. Influence of pilates training on the quality of life of chronic stroke patients. J. Phys. Ther. Sci. 2017, 29, 1830–1835. [Google Scholar] [CrossRef] [PubMed]
- Sung Lim, H.; Yoon, S. The effects of Pilates exercise on cardiopulmonary function in the chronic stroke patients: A randomized controlled trials. J. Phys. Ther. Sci. 2017, 29, 959–963. [Google Scholar] [CrossRef]
- Shea, S.; Moriello, G. Feasibility and outcomes of a classical Pilates program on lower extremity strength, posture, balance, gait, and quality of life in someone with impairments due to a stroke. J. Bodyw. Mov. Ther. 2014, 18, 332–360. [Google Scholar] [CrossRef]
- Sung Lim, H.; Lim Kim, Y.; Min Lee, S. The effects of Pilates exercise training on static and dynamic balance in chronic stroke patients: A randomized controlled trial. J. Phys. Ther. Sci. 2016, 28, 1819–1824. [Google Scholar] [CrossRef]
- Çoban, F.; Belgen Kaygısız, B.; Selcuk, F. Effect of clinical Pilates training on balance and postural control in patients with Parkinson’s disease: A randomized controlled trial. J. Comp. Eff. Res. 2021, 10, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Eldemir, K.; Guclu-Gunduz, A.; Eldemir, S.; Saygili, F.; Ozkul, C.; Irkec, C. Effects of Pilates-based telerehabilitation on physical performance and quality of life in patients with multiple sclerosis. Disabil. Rehabil. 2023, 6, 1–8. [Google Scholar] [CrossRef]
- Najafi, P.; Hadizadeh, M.; Geok Cheong, J.P.; Motl, R.W.; Abdullah, S.; Mohafez, H.; Poursadeghfard, M. Effects of tele-exercise training on physical and mental health and quality of life in multiple sclerosis: Do the effects differ by modality and clinical disease course? Mult. Scler. Relat. Disord. 2023, 7, 105129. [Google Scholar] [CrossRef] [PubMed]
- Chandan, J.S.; Brown, K.R.; Simms-Williams, N.; Bashir, N.Z.; Camaradou, J.; Heining, D.; Turner, G.M.; Cruz Rivera, S.; Hotham, R.; Minhas, S.; et al. Non-Pharmacological Therapies for Post-Viral Syndromes, Including Long COVID: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3477. [Google Scholar] [CrossRef] [PubMed]
- Belgen Kaygisiz, B.; Çoban, F.; Selcuk, F. The effect of clinical pilates-based physiotherapy program for a Stiff Person Syndrome patient: A case report. Acta Neurol. Belg. 2021, 121, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Jung, K.; Jung, W.S.; Kim, S.W.; Kim, J.; Lim, K. Effects of Online Pilates and Face-to-Face Pilates Intervention on Body Composition, Muscle Mechanical Properties, Cardiometabolic Parameters, Mental Health, and Physical Fitness in Middle-Aged Women with Obesity. Healthcare 2023, 11, 2768. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, S.; Tallett, A.; Witwicki, C.; Hay, H.; Mkandawire, C.; Ogundipe, A.; Ojeer, P.; Whitaker, A.; Thompson, J.; Sizmur, S.; et al. Patient-reported experience measure in sickle cell disease. Arch. Dis. Child. 2018, 103, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Larson, E.; Sharma, J.; Bohren, M.A.; Tunçalp, O. When the patient is the expert: Measuring patient experience and satisfaction with care. Bull. World Health Organ. 2019, 97, 563–569. [Google Scholar] [CrossRef]
- Dias Barbosa, C.; Balp, M.M.; Kulich, K.; Germain, N.; Rofail, D. A literature review to explore the link between treatment satisfaction and adherence, compliance, and persistence. Patient Prefer. Adherence 2012, 6, 39–48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Control Group n = 15 Mean (SD)/N (%) | Experimental Group n = 15 Mean (SD)/N (%) | p Value |
|---|---|---|---|
| Age | 55.7 (16.8) | 58.5 (11.1) | 0.732 |
| Sex | 0.713 | ||
| Male | 8 (53.3) | 9 (60.0) | |
| Female | 7 (47.7) | 6 (40.0) | |
| Months since diagnosis | 50.1 (33.4) | 34.5 (18.0) | 0.128 |
| Stroke | 0.409 | ||
| Hemorrhagic | 10 (66.7) | 12 (80.0) | |
| Ischemic | 5 (33.3) | 3 (20.0) | |
| Hand dominance | 0.624 | ||
| Right | 12 (80.0) | 13 (86.7) | |
| Left | 3 (20.0) | 2 (13.3) | |
| Impaired upper limb | 0.143 | ||
| Right | 9 (60.0) | 5 (33.3) | |
| Left | 6 (40.0) | 10 (66.7) | |
| Occupational Therapy intervention weekly hours | 1.9 (0.3) | 1.6 (0.5) | 0.034 * |
| Physical Therapy intervention weekly hours | 1.7 (0.5) | 1.8 (0.4) | 0.679 |
| FIM a | 68.0 (6.4) | 74.5 (7.7) | 0.018 * |
| FRT b | 2.6 (1.8) | 2.7 (2.0) | 0.847 |
| TUG c | 110.3 (49.6) | 93.4 (26.4) | 0.254 |
| NHPT d (right) | 111.9 (48.1) | 77.0 (31.7) | 0.027 * |
| NHPT d (left) | 90.1 (40.4) | 96.2 (30.8) | 0.645 |
| BBT e (right) | 29.9 (31.0) | 51.3 (31.3) | 0.068 |
| BBT e (left) | 41.6 (29.5) | 28.7 (26.2) | 0.214 |
| DASH disability | 85.3 (8.7) | 86.1 (7.6) | 0.790 |
| DASH occupation | 94.1 (7.5) | 91.1 (8.7) | 0.320 |
| Experimental Group | |||||
|---|---|---|---|---|---|
| Outcomes | Pre-Intervention Score (M [SD]) | Post-Intervention Score (M [SD]) | p Value | Follow-Up Score (M [SD]) | p Value |
| FIM a | 74.5 (7.7) | 82.1 (6.7) | <0.001 * | 82.3 (6.8) | <0.001 * |
| FRT b | 2.7 (2.0) | 5.7 (2.6) | <0.001 * | 5.5 (2.6) | <0.001 * |
| TUG c | 93.4 (26.4) | 91.0 (26.4) | 0.008 * | 87.3 (24.2) | <0.001 * |
| NHPT d (right) | 77.0 (31.7) | 67.5 (20.9) | 0.007 * | 63.2 (18.6) | 0.002 * |
| NHPT d (left) | 96.2 (30.8) | 82.3 (21.7) | <0.001 * | 80.8 (22.4) | <0.001 * |
| BBT e (right) | 51.5 (31.3) | 56.4 (31.3) | <0.001 * | 58.6 (32.6) | 0.427 |
| BBT e (left) | 28.7 (26.2) | 35.7 (27.1) | <0.001 * | 50.1 (54.9) | 0.134 |
| DASH disability | 86.1 (7.6) | 82.3 (7.9) | <0.001 * | 81.7 (7.6) | <0.001 * |
| DASH occupation | 91.1 (8.7) | 86.1 (8.5) | <0.001 * | 85.5 (9.1) | <0.001 * |
| Control group | |||||
| Outcomes | Pre-intervention Score (M [SD]) | Post-intervention score (M [SD]) | p Value | Follow-up score (M [SD]) | p Value |
| FIM a | 68.0 (6.4) | 70.2 (6.5) | 0.002 * | 70.5 (6.5) | 0.002 * |
| FRT b | 2.6 (1.8) | 2.8 (1.7) | 0.098 | 2.6 (1.8) | 0.974 |
| TUG c | 110.3 (49.6) | 108.6 (47.8) | 0.080 | 106.1 (49.6) | 0.064 |
| NHPT d (right) | 111.9 (48.1) | 109.4 (47.3) | <0.001 * | 109.1 (47.5) | 0.007 * |
| NHPT d (left) | 90.1 (40.4) | 89.5 (41.4) | 0.173 | 89.0 (42.3) | 0.289 |
| BBT e (right) | 29.9 (31.0) | 30.8 (31.6) | 0.097 | 35.2 (32.8) | 0.583 |
| BBT e (left) | 41.6 (29.5) | 42.7 (30.1) | 0.048 * | 43.0 (30.6) | 0.022 * |
| DASH disability | 85.3 (8.7) | 84.5 (8.6) | 0.138 | 84.5 (8.7) | 0.200 |
| DASH occupation | 94.1 (7.5) | 93.1 (7.2) | 0.161 | 93.0 (7.3) | 0.136 |
| Post-Intervention | Follow-Up | |||||
|---|---|---|---|---|---|---|
| Outcomes | Inter-Group Difference | [95% CI] | p Value | Inter-Group Difference | [95% CI] | p Value |
| FIM a | 11.9 | [7.0, 16.9] | <0.001 * | 11.7 | [6.8, 16.7] | <0.001 * |
| FRT b | 2.9 | [1.2, 4.5] | 0.001 * | 2.9 | [1.2, 4.6] | 0.001 * |
| TUG c | −17.6 | [−46.4, 11.3] | 0.222 | −18.9 | [−48.1, 10.3] | 0.196 |
| NHPT d (right) | −41.9 | [−69.8, −13.9] | 0.005 * | −45.9 | [−73.6, −18.2] | 0.003 * |
| NHPT d (left) | −7.2 | [−32.3, 17.9] | 0.557 | −8.2 | [−33.9, 17.5] | 0.513 |
| BBT e (right) | 25.6 | [2.1, 49.1] | 0.034 * | 23.4 | [−1.1, 47.9] | 0.060 |
| BBT e (left) | −7.0 | [−28.4, 14.4] | 0.509 | 7.1 | [−26.2, 40.3] | 0.667 |
| DASH disability | −2.2 | [−8.4, 4.0] | 0.471 | −2.8 | [−8.9, 3.3] | 0.355 |
| DASH occupation | −6.9 | [−12.8, −1.0] | 0.023 * | −7.5 | [−13.7, −1.4] | 0.018 * |
| Post-Intervention | Follow-Up | |||
|---|---|---|---|---|
| Outcomes | p Value | Effect Size (η2) | p Value | Effect Size (η2) |
| FIM a | <0.001 * | 0.461 | <0.001 * | 0.435 |
| FRT b | 0.016 * | 0.197 | 0.014 * | 0.203 |
| TUG c | 0.663 | 0.007 | 0.767 | 0.003 |
| NHPT d (right) | 0.013 * | 0.207 | 0.005 * | 0.253 |
| NHPT d (left) | 0.571 | 0.012 | 0.538 | 0.014 |
| BBT e (right) | 0.126 | 0.085 | 0.024 * | 0.174 |
| BBT e (left) | 0.835 | 0.002 | 0.894 | 0.001 |
| DASH disability | 0.867 | 0.001 | 0.958 | <0.001 |
| DASH occupation | 0.189 | 0.063 | 0.152 | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Bravo, C.; Delgado-Lobete, L.; Montes-Montes, R.; Rodríguez-Pérez, M.P.; Trugeda-Pedrajo, N.; Fernández-Gómez, G.; García-Bravo, S. Effects of Neuropilates on Functional Outcomes in Chronic Stroke: A Randomized Clinical Trial. Healthcare 2024, 12, 850. https://doi.org/10.3390/healthcare12080850
García-Bravo C, Delgado-Lobete L, Montes-Montes R, Rodríguez-Pérez MP, Trugeda-Pedrajo N, Fernández-Gómez G, García-Bravo S. Effects of Neuropilates on Functional Outcomes in Chronic Stroke: A Randomized Clinical Trial. Healthcare. 2024; 12(8):850. https://doi.org/10.3390/healthcare12080850
Chicago/Turabian StyleGarcía-Bravo, Cristina, Laura Delgado-Lobete, Rebeca Montes-Montes, Mª Pilar Rodríguez-Pérez, Nuria Trugeda-Pedrajo, Gemma Fernández-Gómez, and Sara García-Bravo. 2024. "Effects of Neuropilates on Functional Outcomes in Chronic Stroke: A Randomized Clinical Trial" Healthcare 12, no. 8: 850. https://doi.org/10.3390/healthcare12080850
APA StyleGarcía-Bravo, C., Delgado-Lobete, L., Montes-Montes, R., Rodríguez-Pérez, M. P., Trugeda-Pedrajo, N., Fernández-Gómez, G., & García-Bravo, S. (2024). Effects of Neuropilates on Functional Outcomes in Chronic Stroke: A Randomized Clinical Trial. Healthcare, 12(8), 850. https://doi.org/10.3390/healthcare12080850