
Validation of the Health Index in the Postoperative Period: Use of the Nursing Outcome Classification to Determine the Health Level

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Development Phase
2.2.1. Construction of a Preliminary Instrument
- Does the nursing outcome include in its label any words found in a health variable or in its definition?
- Does the nursing outcome include in its definition any word found in any health variable or in its definition?
- Does the nursing outcome include in its indicators any words found in a health variable or its definition?
- There had to be coincidences of common concepts between the definition of the health variable and the definition of the NOC label.
- Or, there had to be a conceptual coincidence (synonymous) between the definition of the health variable and the indicators of the NOC label.
2.2.2. Internal Validation: Validation by Experts in the Language of Care
2.3. Validation Phase
2.3.1. External Validation
2.3.2. Clinical Validation
- Inclusion Criteria: 18 years of age or older, signature of informed consent, scheduled surgery and general anesthesia.
- Exclusion criteria: Under 18 years of age, patients incapable of giving consent, people with cognitive impairment, urgent surgeries, local and regional anesthesia, being admitted to the unit before the start of each study cut-off, continuing to be admitted to the unit after the study cut-off and remaining in the unit for more than 7 h.
Sample and Data Collection
Ethical Considerations
Data Analysis
- Contextually significant variables: Physical Functioning, Mental Functioning, Social Functioning, Comfort State, Presence of Signs, Presence of Symptoms, Physical Condition, Mental Condition, Social Condition.
- Contextually non-significant variables: material resource and time resource. This was because the study participants were hospitalized in a health institution. The National Health System in Spain is free and universal [50] so it was assumed that they had the necessary material resources for their care, as well as all their time to take care of themselves.
3. Results
3.1. Instrument Construction
3.2. External and Clinical Validation
3.2.1. External Validation
3.2.2. Clinical Validation
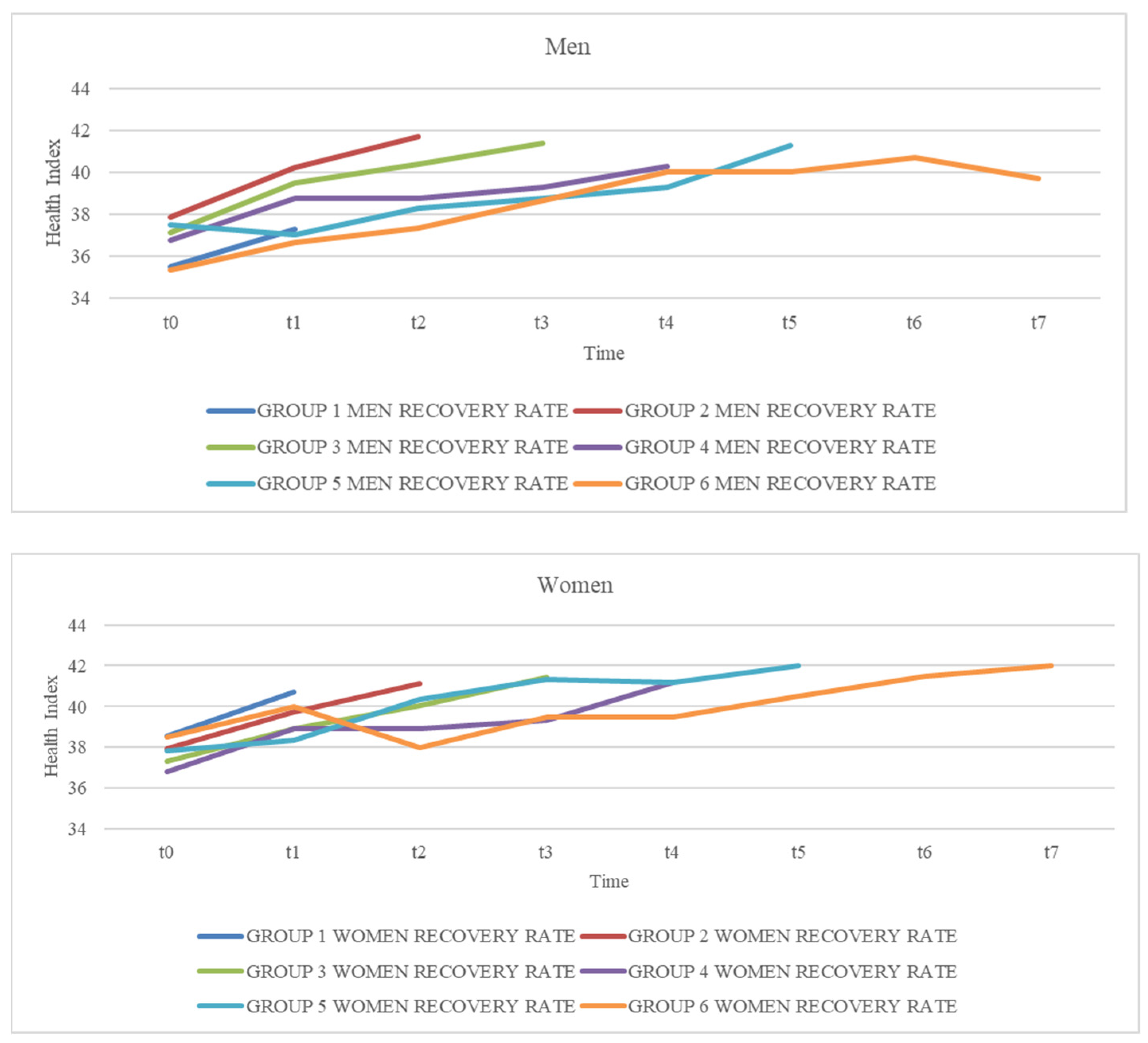
Health Level Evolution
Differential Health Level between Admission and Discharge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Alliance for Patient Safety. Safe Surgery Saves Lives. 2008. Available online: https://iris.who.int/bitstream/handle/10665/70080/WHO_IER_PSP_2008.07_eng.pdf?sequence=1 (accessed on 8 January 2024).
- Aristil, P.M. Manual de Farmacología Básica y Clínica, 6th ed.; McGraw-Hill Interamericana: Mexico City, México, 2015. [Google Scholar]
- Martín Delgado, M.; Gordo Vidal, F. Perioperative intensive care medicine. Med. Intensiv. 2019, 43, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Pérez de la Plaza, E. Terapéutica Quirúrgica Cuidados Preoperatorios; Editorial McGraw-Hill Interamericana de España: Aravaca, Spain, 2013; ISBN 978-84-481-8680-7. [Google Scholar]
- Rincon-Valenzuela, D.A.; Escobar, B. Evidence-based clinical practice manual: Patient preparation for surgery and transfer to the operating room. Rev. Colomb. Anestesiol. 2015, 43, 51–60. [Google Scholar] [CrossRef]
- Goodman, T.; Spry, C. Essentials of Perioperative Nursing; Jones & Bartlett Learning: Burlington, VT, USA, 2016. [Google Scholar]
- Nilsson, U.; Jaensson, M.; Hugelius, K.; Arakelian, E.; Dahlberg, K. A journey to a new stable state—Further development of the postoperative recovery concept from day surgical perspective: A qualitative study. BMJ J. 2020, 10, e037755. [Google Scholar] [CrossRef] [PubMed]
- Allvin, R.; Berg, K.; Idvall, E.; Nilsson, U. Postoperative recovery: A concept analysis. J. Adv. Nurs. 2007, 57, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Larsson, F.; Strömbäck, U.; Gustafsson, S.R.; Engström, A. Postoperative Recovery: Experiences of Patients Who Have Undergone Orthopedic Day Surgery. J. Perianesth. Nurs. 2022, 37, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Odom-Forren, J.; Red, D.B.; Rush, C. Postoperative Distress of Orthopedic Ambulatory Surgery Patients. AORN J. 2017, 105, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Bowyer, A.J.; Royse, C.F. Postoperative recovery and outcomes—What are we measuring and for whom? Anaesthesia. 2016, 71, 72–77. [Google Scholar] [CrossRef]
- Eslava-Schmalbach, J.; Gaitán Duarte, H.; Gómez Restrepo, C. A scale for measuring the quality of post-anaesthetic recovery from the users point of view. Rev. Salud Pública 2006, 8, 52–64. [Google Scholar]
- Kiekkas, P.; Tsekoura, V.; Fligou, F.; Tzenalis, A.; Michalopoulos, E.; Voyagis, G. Missed Nursing Care in the Postanesthesia Care Unit: A Cross-Sectional Study. J. Perianesth. Nurs. 2021, 36, 232–237. [Google Scholar] [CrossRef]
- Ferraz, S.M.; Moreira, J.P.; Mendes, L.C.; Amaral, T.M.; Andrade, A.R.; Santos, A.R.; Abelha, F.J. Evaluation of the quality of recovery and the postoperative health status after elective surgery. Rev. Bras. Anestesiol. 2018, 68, 577–583. [Google Scholar] [CrossRef]
- Borg Card, E.; Wells, N.; Mesko, P.; Eliades, A.; MacDonald, R.; Krezischek, D.A. Perianesthesia Nurses Pain Management Practices: Findings and Recommendations from a National Descriptive Study of Members of the American Society of Perianesthesia Nurses. J. Perianesth. Nurs. 2021, 36, 128–135. [Google Scholar] [CrossRef]
- Whizar-Lugo, V.M.; Santos-Moreno, F. Anestesia General vs. Anestesia Regional en el anciano. Anest. México, 2004; 16, 40–52. [Google Scholar]
- Tornero, C.; Aliaga Font, L.; Belda Nacher, J.; Carmona, P.; Gomar, C.; Roqués, V. Anestesia. Fundamentos y Manejo Clínico; Editorial Médica Panamericana, S.A.: Madrid, Spain, 2015. [Google Scholar]
- Spruce, L. Using a Complementary Intervention to Decrease Postoperative Nausea and Vomiting. AORN J. 2020, 112, 417–418. [Google Scholar] [CrossRef] [PubMed]
- Lenhardt, R. Body temperature regulation and anesthesia. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 157, pp. 635–644. [Google Scholar]
- Beaussier, M.; Raucoules-Aimé, M. Métodos de evaluación y escalas de los estadios del despertar. EMC-Anestesia-Reanimación. 2016, 42, 1–13. [Google Scholar] [CrossRef]
- Strengthening Essential and Emergency Surgical Care and Anaesthesia as Components of Universal Health Coverage. Organización Mundial de la Salud 2015. 68.a ASAMBLEA MUNDIAL DE LA SALUD A68/31Punto 17.1 del Orden del día Provisional. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA68/A68_31-sp.pdf. (accessed on 17 March 2024).
- González Aguña, A.; Fernández Batalla, M.; Gonzalo de Diego, B.; Jiménez Rodríguez, M.L.; Martínez Muñoz, M.L.; Santamaría García, J.M. Care Recommendations for the Chronic Risk of COVID-19: Nursing Intervention for Behaviour Changes. Int. J. Environ. Res. 2022, 19, 8532. [Google Scholar] [CrossRef] [PubMed]
- American Society of PeriAnesthesia Nurses. A Position Statement on Perianesthesia Safety. 2009. Available online: https://www.aspan.org/Portals/88/Clinical%20Practice/Position%20Statements/Retired/Perianes_Safety_2012.pdf?ver=2020-08-21-155911-823 (accessed on 22 December 2023).
- American Society of PeriAnesthesia Nurses™ (ASPAN®). 2021–2022 Perianesthesia Nursing Standards, Practice Recommendations and Interpretive Statements; American Society of PeriAnesthesia Nurses™ (ASPAN®): Cherry Hill, NJ, USA, 2021. [Google Scholar]
- Windle, P.E.; Mamaril, M.; Fossum, S. Perianesthesia Nursing Advocacy: An Influential Voice for Patient Safety. J. Perianesth. Nurs. 2008, 23, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Orem, D.E. Orem Model: Concepts of Nursing in Practice; Masson-Salvat: Barcelona, Spain, 1993. [Google Scholar]
- Herrero Jaén, S. Formalización del Concepto de Salud a Través de la Lógica: Impacto del Lenguaje Formal en las Ciencias de la Salud. ENE Rev. Enferm. 2016, 10. Available online: https://scielo.isciii.es/scielo.php?pid=S1988-348X2016000200006&script=sci_arttext&tlng=en (accessed on 22 December 2023).
- Fernandez-Batalla, M. La Persona en el Continuo del Cuidado: Formalización de las Variables Básicas del Cuidado Implicadas en la Trayectoria de Salud. Unpublished Doctoral Dissertation, University of Alcalá, Alcalá de Henares, Spain, 2018. [Google Scholar]
- Herrero Jaén, S.; Madariaga Casquero, L. Las Variables de Salud y su aplicación en el cálculo del estado de salud de las personas. Rev. ENE Enferm. 2018, 12. Available online: http://ene-enfermeria.org/ojs/index.php/ENE/article/view/875/lcc5v12n3 (accessed on 22 December 2023).
- Moorhead, S.; Swanson, E.; Johnson, M.; Maas, M.L. Nursing Outcomes Classification, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- González Aguña, A.; Fernandez Batalla, M.; Díaz-Tendero Rodríguez, J.; Sarrión Bravo, J.A.; Gonzalo de Diego, B.; Santamaría García, J.M. Validation of a manual of care plans for people hospitalized with COVID-19. Nurs. Open 2021, 8, 3495–3515. [Google Scholar] [CrossRef] [PubMed]
- Official Spanish Gazette. Royal Decree 1093 of 3 September 2010. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2010-14199 (accessed on 17 December 2023).
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Raile Aligood, M. Modelos y Teorías en Enfermería, 10th ed.; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Seo, K.; Song, Y. Development and validation of the self-stigma scale in people with diabetes. Nurs. Open 2020, 5, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Cáceres-Matos, R.; Gil-García, E.; Rivera-Sequeiros, A.; López-Millán, J.M. Design and preliminarily validation of a tool to assess the impact of chronic non-cancer pain on people’s daily life in Spanish-language: PAIN_Integral Scale©. J. Adv. Nurs. 2021, 77, 3553–3570. [Google Scholar] [CrossRef] [PubMed]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- González Aguña, A.; Rodríguez Jiménez, M.L.; Fernández Batalla, M.; Herrero Jaén, S.; Monsalvo San Macario, E.; Real Martínez, V.; Santamaría García, J.M. Nursing Diagnoses for Coronavirus Disease, COVID-19: Identification by Taxonomic Triangulation. Int. J. Nurs. Knowl. 2020, 32, 108–116. [Google Scholar] [CrossRef] [PubMed]
- University of Alcalá. Research Groups. Healthcare Informatics Research. 2021. Available online: https://www.uah.es/es/investigacion/unidades-de-investigacion/grupos-de-investigacion/Investigacion-en-informatica-en-el-cuidado-de-la-salud-MISKC-Healthcare-Informatics-Research (accessed on 18 April 2024).
- Madrid Scientific Society of Care. 2018. Available online: https://socienmadridcuidado.wixsite.com/socmac (accessed on 23 December 2023).
- Kelly, J.; Watson, R. Instrument development and validation of a quality scale for historical research papers (QSHRP): A pilot study. J. Adv. Nurs. 2014, 70, 2964–2967. [Google Scholar] [CrossRef] [PubMed]
- Koch, D.; Kutz, A.; Conca, A.; Wenke, J.; Schuetz, P.; Mueller, B. The relevance, feasibility and benchmarking of nursing quality indicators: A Delphi study. J. Adv. Nurs. 2020, 76, 3483–3494. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Tatano Beck, C. Nursing Research: Generating and assessing Evidence for Nursing Practice, 11th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021. [Google Scholar]
- Vega-Escaño, J.; Barrientos-Trigo, S.; Romero-Sánchez, J.M.; de Diego-Cordero, R.; Porcel- Gálvez, A.M. Development and validation of the operational definitions of the defining characteristics of the nursing diagnosis of insomnia in the occupational health setting. Int. J. Nurs. Knowl. 2020, 31, 275–284. [Google Scholar] [CrossRef] [PubMed]
- González Aguña, A.; Fernández Batalla, M.; Arias Baelo, C.; Monsalvo San Macario, E.; Gonzalo de Diego, B.; Santamaría García, J.M. Usability Evaluation by Nurses of a Knowledge-Based System of Care Plans for People Hospitalized by COVID-19. Comp. Inf. Nurs. 2021, 40, 186–200. [Google Scholar] [CrossRef] [PubMed]
- Severo Ochoa University Hospital. 2018 Annual Report. Annual Report, Madrid Health Service. 2019. Available online: https://www.comunidad.madrid/sites/default/files/doc/sanidad/memo/hosp-memoria_2018_hsvo_ok.pdf (accessed on 16 December 2023).
- Official Journal of the European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016. 2016. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/HTML/?uri=CELEX:32016R0679 (accessed on 16 December 2023).
- Moncho Vasallo, J. Estadística Aplicada a las Ciencias de la Salud; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 15 December 2023).
- Ministry of Health. National Health System. 2012. Available online: https://www.mscbs.gob.es/organizacion/sns/libroSNS.htm (accessed on 21 December 2023).
- Género y Salud. Organización Mundial de la Salud. 2018. Available online: https://www.who.int/es/news-room/fact-sheets/detail/gender (accessed on 16 March 2024).
- Fernández Batalla, M.; Monsalvo San Macario, E.; González Aguña, A.; Herrero Jaén, S.; Gonzalo de Diego, B.; Manrique Anaya, Y.; Jiménez Rodríguez, M.L.; Melguizo Herrera, E.; Santamaría García, J.M. Validation and reliability of the Care Vulnerability Index: A study by interrater agreement and test–retest method. Nurs. Open 2022, 9, 1766–1773. [Google Scholar] [CrossRef]
- Eurostat, the Statistical Office of the European Union. Share of People with Good or Very Good Perceived Health by Sex (sdg_03_20). 2021. Available online: https://ec.europa.eu/eurostat/cache/metadata/en/sdg_03_20_esmsip2.htm (accessed on 10 January 2024).
- Eurostat, the Statistical Office of the European Union. Health Variables of EU-SILC. 2021. Available online: https://ec.europa.eu/eurostat/cache/metadata/EN/hlth_silc_01_esms.htm (accessed on 10 January 2024).
- Morán del Pozo, C. Criterios de puntuación del alta postanestésico. Rev. ENE Enferm. 2017, 11. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1988-348X2017000300015&lng=es&tlng=es (accessed on 20 December 2023).
- Cabedo, N.; Valeroa, R.; Alcón, A.; Gomara, C. Prevalence and characterization of postoperative pain in the Postanaesthesia Care Unit. Rev. Esp. Anestesiol. Reanim. 2017, 64, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Rozman, C.; Cardellach, F. Medicina Interna, 19th ed.; Elsevier: Amsterdam, The Netherlands, 2020; Volume 1. [Google Scholar]
- Vicente Herrero, M.; Delgado Bueno, S.; Brandés Moyá, F.; Ramírez Iñiguez de la Torre, M.; Capdevila García, L. Valoración del dolor. Revisión comparativa de escalas y cuestionarios. Soc. Esp. Dolor. 2018, 25, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Latorre Marco, I.; Solís Muñoz, M.; Falero Ruiz, T.; Larrasquitu Sánchez, A.; Romay Pérez, A.; Millán Santos, I. Validation of the Scale of Behavior Indicators of Pain (ESCID) in critically ill, non-communicative patients under mechanical ventilation: Results of the ESCID scale. Enferm. Intensiv. 2011, 22, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Terceros-Almanza, L.; García Fuentes, C.; Bermejo Aznárez, S.; Prieto del Portillo, I.; Mudarra Reche, C.; Domínguez Aguado, H.; Chico Fernández, M. Prediction of massive bleeding in a prehospital setting: Validation of six scoring systems. Med. Intensiv. 2019, 43, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Aldrete, J.A. Modificaciones y adaptaciones al esquema de recuperación de Aldrete en cirugía ambulatoria, obstétrica, pediátrica y oncológica. Rev. Argent. Anestesiol. 2007, 65, 194–202. [Google Scholar]
- PostopQRS Ltd. Postoperative Quality Recovery Scale. 2020. Available online: https://www.postopqrs.com/ (accessed on 27 December 2023).
- Pérez Herrero, M.; López Álvarez, S.; Fadrique Fuentes, A.; Manzano Lorefice, F.; Bartolomé Bartolomé, C.; González de Zárate, J. Quality of postoperative recovery after breast surgery. General anaesthesia combined with paravertebral versus serratus-intercostal block. Rev. Esp. Anestesiol. Reanim 2016, 63, 564–571. [Google Scholar] [CrossRef]
- González Aguña, A.; Fernández Batalla, M.; Gasco González, S.; Cercas Duque, A.; Jiménez Rodríguez, M.L.; Santamaría García, J.M. Taxonomic Triangulation of Care in Healthcare Protocols: Mapping of Diagnostic Knowledge from Standardized Language. Comp. Inform. Nurs. 2021, 39, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Pulkkinen, M.; Jousela, I.; Sintonen, H.; Engblom, J.; Salanterä, S.; Junttila, K. A randomized clinical trial of a new perioperative practice model on anxiety and health-related quality of life in arthroplasty patients. Nurs. Open 2021, 8, 1593–1605. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro Garcia, T. ICNP®: A standardized terminology for the description of professional nursing practice. Rev. Esc. Enferm. USP 2016, 50, 378–379. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (Total Responding) | N | (%) |
|---|---|---|
| Gender (N = 7) | ||
| Male | 3 | 42.85 |
| Female | 4 | 57.14 |
| Age (N = 7) | ||
| 20–29 | 2 | 28.57 |
| 30–39 | 3 | 42.85 |
| >40 | 2 | 28.57 |
| Years of Nursing Practice (N = 7) | ||
| 1–10 | 5 | 71.42 |
| 11–20 | ||
| 21–30 | 2 | 28.57 |
| Years of Experience in the use of Languages of Care (N = 7) | ||
| 1–10 | 5 | 71.42 |
| 11–20 | 0 | 0 |
| 21–30 | 2 | 28.57 |
| Clinical Position (N = 7) | ||
| Clinical nurse | 6 | 85.71 |
| University teaching | 1 | 14.28 |
| Level of Nursing Education (N = 7) | ||
| Graduate | 7 | 100 |
| Master | 7 | 100 |
| Specialist | 2 | 28.57 |
| PhD | 2 | 28.57 |
| Research Experience (N = 7) | ||
| Master | 7 | 100 |
| Doctorate | 2 | 28.57 |
| Research group | 7 | 100 |
| Clinical research | 6 | 85.71 |
| Group and Sex | t0 | t1 | t2 | t3 | t4 | t5 | t6 | t7 |
|---|---|---|---|---|---|---|---|---|
| Group 1 men recovery rate | 35.5 | 37.25 | ||||||
| Group 1 women recovery rate | 38.57 | 40.71 | ||||||
| Group 2 men recovery rate | 37.83 | 40.20 | 41.66 | |||||
| Group 2 women recovery rate | 37.94 | 39.74 | 41.14 | |||||
| Group 3 men recovery rate | 37.10 | 39.50 | 40.37 | 41.37 | ||||
| Group 3 women recovery rate | 37.31 | 38.93 | 40.03 | 41.43 | ||||
| Group 4 men recovery rate | 36.75 | 38.75 | 38.75 | 39.25 | 40.25 | |||
| Group 4 women recovery rate | 36.80 | 38.90 | 38.90 | 39.30 | 41.20 | |||
| Group 5 men recovery rate | 37.50 | 37.00 | 38.25 | 38.75 | 39.25 | 41.25 | ||
| Group 5 women recovery rate | 37.83 | 38.33 | 40.33 | 41.33 | 41.16 | 42.00 | ||
| Group 6 men recovery rate | 35.33 | 36.66 | 37.33 | 38.66 | 40.00 | 40.00 | 40.66 | 39.66 |
| Group 6 women recovery rate | 38.50 | 40.00 | 38.00 | 39.50 | 39.50 | 40.50 | 41.50 | 42.00 |
| Health Variables | Score scale | Women | Men | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Admission | Discharge | Admission | Discharge | ||||||
| fi | fri% | fi | fri% | fi | fri% | fi | fri % | ||
| Physical Functioning | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0% |
| 2 | 1 | 1.08% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 41 | 44.56% | 3 | 3.26% | 21 | 44.68% | 2 | 4.25% | |
| 4 | 50 | 54.34% | 84 | 91.30% | 26 | 55.31% | 45 | 95.74% | |
| 5 | 0 | 0.00% | 5 | 5% | 0 | 0.00% | 0 | 0.00% | |
| Mental Functioning | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 1 | 2.12% | 0 | 0.00% | |
| 3 | 12 | 13.04% | 0 | 0.00% | 6 | 12.76% | 1 | 2.12% | |
| 4 | 69 | 75.00% | 13 | 14.13% | 35 | 74.46% | 5 | 10.63% | |
| 5 | 11 | 11.95% | 79 | 85.86% | 5 | 10.63% | 41 | 87.23% | |
| Social Functioning | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 1 | 2.12% | 0 | 0.00% | |
| 3 | 7 | 7.60% | 0 | 0.00% | 3 | 6.38% | 0 | 0.00% | |
| 4 | 46 | 50.00% | 4 | 4.34% | 22 | 46.80% | 5 | 10.63% | |
| 5 | 39 | 42.39% | 88 | 96% | 21 | 44.68% | 42 | 89.36% | |
| Comfort Status | 1 | 1 | 1.08% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 4 | 4.34% | 0 | 0.00% | 1 | 2.12% | 0 | 0.00% | |
| 3 | 30 | 32.60% | 3 | 3.26% | 19 | 40.42% | 1 | 2.12% | |
| 4 | 52 | 56.52% | 59 | 64.13% | 24 | 51.06% | 32 | 68.08% | |
| 5 | 5 | 5.43% | 30 | 32.60% | 3 | 6.38% | 14 | 29.78% | |
| Signs Presence | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 11 | 11.95% | 1 | 1.08% | 5 | 10.63% | 0 | 0.00% | |
| 4 | 61 | 66.30% | 28 | 30.43% | 33 | 70.21% | 19 | 40.42% | |
| 5 | 20 | 21.73% | 63 | 68.47% | 9 | 19.14% | 28 | 59.57% | |
| Symptoms Presence | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 1 | 1.08% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 17 | 18.47% | 2 | 2.17% | 13 | 27.65% | 0 | 0.00% | |
| 4 | 66 | 71.73% | 61 | 66.30% | 33 | 70.21% | 26 | 55.31% | |
| 5 | 8 | 8.69% | 29 | 31.52% | 1 | 2.12% | 21 | 44.68% | |
| Physical Condition | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 6 | 6.52% | 7 | 7.60% | 8 | 17.02% | 8 | 17.02% | |
| 4 | 53 | 57.60% | 50 | 54.34% | 25 | 53.19% | 26 | 55.31% | |
| 5 | 33 | 35.86% | 35 | 38.04% | 14 | 29.78% | 13 | 27.65% | |
| Mental Condition | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 4 | 7 | 7.60% | 8 | 8.69% | 6 | 12.76% | 6 | 12.76% | |
| 5 | 85 | 92.39% | 84 | 91.30% | 41 | 87.23% | 41 | 87.23% | |
| Social Condition | 1 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 2 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |
| 3 | 0 | 0.00% | 0 | 0.00% | 1 | 2.12% | 1 | 2.12% | |
| 4 | 2 | 2.17% | 2 | 2.17% | 0 | 0.00% | 0 | 0.00% | |
| 5 | 90 | 97.82% | 90 | 97.82% | 46 | 97.87% | 46 | 97.87% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrero Jaén, S.; González Aguña, A.; Fernández Batalla, M.; Gonzalo de Diego, B.; Sierra Ortega, A.; Rocha Martínez, M.d.M.; Barchino Plata, R.; Jiménez Rodríguez, M.L.; Santamaría García, J.M. Validation of the Health Index in the Postoperative Period: Use of the Nursing Outcome Classification to Determine the Health Level. Healthcare 2024, 12, 862. https://doi.org/10.3390/healthcare12080862
Herrero Jaén S, González Aguña A, Fernández Batalla M, Gonzalo de Diego B, Sierra Ortega A, Rocha Martínez MdM, Barchino Plata R, Jiménez Rodríguez ML, Santamaría García JM. Validation of the Health Index in the Postoperative Period: Use of the Nursing Outcome Classification to Determine the Health Level. Healthcare. 2024; 12(8):862. https://doi.org/10.3390/healthcare12080862
Chicago/Turabian StyleHerrero Jaén, Sara, Alexandra González Aguña, Marta Fernández Batalla, Blanca Gonzalo de Diego, Andrea Sierra Ortega, María del Mar Rocha Martínez, Roberto Barchino Plata, María Lourdes Jiménez Rodríguez, and José María Santamaría García. 2024. "Validation of the Health Index in the Postoperative Period: Use of the Nursing Outcome Classification to Determine the Health Level" Healthcare 12, no. 8: 862. https://doi.org/10.3390/healthcare12080862
APA StyleHerrero Jaén, S., González Aguña, A., Fernández Batalla, M., Gonzalo de Diego, B., Sierra Ortega, A., Rocha Martínez, M. d. M., Barchino Plata, R., Jiménez Rodríguez, M. L., & Santamaría García, J. M. (2024). Validation of the Health Index in the Postoperative Period: Use of the Nursing Outcome Classification to Determine the Health Level. Healthcare, 12(8), 862. https://doi.org/10.3390/healthcare12080862