How Professional and Market Logics and the Conflict between Institutional Demands Affect Hospital Accreditation Compliance: A Multiple-Case Study in Brazil


Abstract
:1. Introduction
2. Theoretical Framework
2.1. Isomorphism, Dissimilarity, and Institutional Logics
2.2. Hospital Accreditation as an Institutional Standard
2.3. Institutional Logics Constituting the Hospital Accreditation Process
2.4. How Do Hospitals Respond to the Hospital Accreditation Process?
3. Materials and Methods
3.1. Selection of Hospitals, Participants, and Field Research
3.2. Ethical Considerations
3.3. Measures

{kind=link}
| Categories | Definitions of Dimensions for Each Category | Questions |
|---|---|---|
| Institutional Logics [2,12,23,37] | Professional Logic: Emphasizes healthcare professionals’ performance, advocating the quality of services, patient, and professional safety, and ensuring reputation and protection. Risks to this logic include compromised care quality and potential errors. | (a) Do you support implementing accreditation in the hospital? What improvements could accreditation bring to the hospital? (b) Can you identify the main challenges encountered during the accreditation process? (c) When choosing to join the Hospital Accreditation program, were there differences of opinions or any conflict among management members? (d) What were the main obstacles/problems that the hospital faced by the hospital during the adoption process? |
| Market Logic: Focuses on the organization’s financial performance and market status. Key objectives include profit generation and organizational growth. The main threatening mechanisms are poor financial results, decreased performance, operational efficiency, and increased costs. | ||
| Objective of Adoption [19,48] | Legitimacy: Aims to gain greater acceptance, respect, and status by stakeholders, including customers, suppliers, and competitors. | (a) When did the institution decide to pursue Hospital Accreditation? (b) How would you define Hospital Accreditation? What does it mean to you? (c) What factors influenced the decision to pursue Hospital Accreditation? Were there alternative options? (d) Why do you consider Hospital Accreditation important to the institution? (e) What did the institution hope to achieve by adopting Hospital Accreditation? |
| Efficiency: Concentrates on enhancing the technical aspects of its operations, such as reducing costs, improving procedures, and increasing productivity. | ||
| Strategic Responses [19,20,21,22] | Conformity: Involves full adherence to the Hospital Accreditation Program, maintaining compliance with the precepts and protocols required even post-certification. | (a) Were all requirements strictly met, or could they have been met through alternative methods? (b) After obtaining certification, were all processes maintained? (c) When the hospital is reassessed, what challenges arise? (d) Do you believe everyone in your department meets all the standards required by accreditation daily? (e) If you were visited by a certification agency auditor today, do you think the hospital would be accredited again? |
| Non-conformity: The hospital predominantly rejects the practices established by the Hospital Accreditation program, retaining only those already practiced or having less impact than competing logics. | ||
| Customization: Primarily adopts the practices established by the Hospital Accreditation program but modifies them to suit the hospital’s actual needs. | ||
| Nature of Demands [14,23,33] | Origin in the Means: Conflicts arise during the accreditation process, mainly in its implementation and organizational reproduction. | (a) What were the main obstacles/problems that the hospital faced during the adoption process? (b) Why did the institution decide to pursue Hospital Accreditation? Were there alternative options? (c) Who made the decision? |
| Origin in Goals: Actions contrary to the decision to adopt accreditation; obstacles arise during the decision-making phase before implementation. |
3.4. Categorization of Interview Excerpts
3.5. Analytical Strategy
4. Results
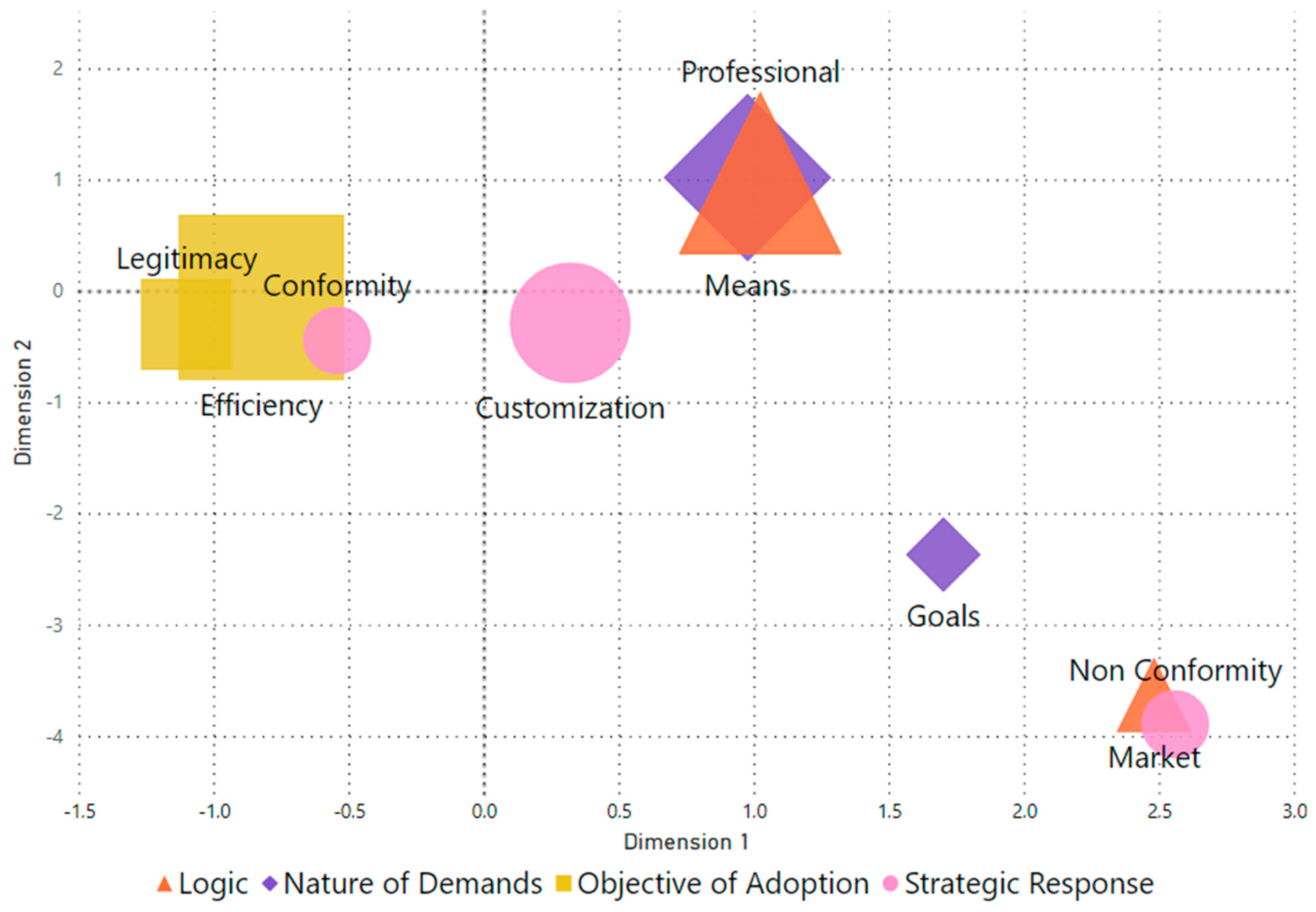
4.1. The Convergence of Logics, Nature of Demands, Objectives and Strategic Responses
4.2. The Expression of Professional and Market Logics in Accreditation
“It is a certification that assesses whether the hospital meets the requirements [outlined] in the accreditation manual, with the aim of [ensuring] patient safety and organizational enhancement.”(CBA Auditor)
“The auditor uses a checklist to evaluate the hospital based on the manual’s requirements. The score is determined by the degree of compliance for each assessed item, with a potential score [ranging from] zero, five, or ten.”(Hospital manager C)
“The biggest difficulty is the commitment of the medical staff. They say they don’t need to improve because they’re already very skilled. It’s hard for physicians to recognize that they need to improve. Even scientific evidence shows that physicians are the last to comply with certification requirements. For this reason, when the certification process starts, the hospital immediately begins the work of convincing the medical staff.”(Hospital manager B)
“The biggest challenge was aligning the activities required for certification with all the professionals in a harmonious way. Because we nurses depended on other professionals to complete our activities, it hindered the certification process.”(Nurse 1 from hospital C)
“The patient is the most important person in this hospital. I work for the patient. Everything I do is for the patient. So we had to adapt some of the things stated in the manual with the patient in mind.”(Hospital manager A)
“In 2001, there was a very stormy period in the hospital management, which led to the dismissal of many people. As a result, the accreditation process stalled for months.”(Hospital manager C)
“At a certain point, changes had to be made in my sector to meet the certification requirements. However, the significant expenses required for these changes were not immediately authorized, resulting in a delay of the accreditation process until the hospital met the necessary criteria.”(Nurse 2 at Hospital C)
4.3. Balancing Legitimacy and Efficiency in Hospital Accreditation
“The hospital aimed to enhance both the performance of its professionals and its operational processes. Its interest was adopting a certification model that is widely recognized as effective in its purpose of providing quality and safety in healthcare delivery.”(Hospital Manager B)
“The hospital has always been committed to providing [high-]quality medical care that exceeds patient expectations.”(Hospital manager B)
“It is a voluntary assessment process in which a healthcare organization, such as a hospital, agrees to submit its administrative and care processes to certification standards. If the hospital achieves the required compliance, it earns a seal, which means it has [established] a patient quality and safety program that sets it apart positively from its counterparts.”(Hospital manager B)
“The patient sees the certification procedures but does not grasp their importance. I believe there is a lack of information […] Many [patients] find it strange to wear wristbands and may even complain about it. However, the clients don’t know that it is part of an accreditation protocol that increases the safety and care quality.”(Hospital manager A)
4.4. Conformity, Customization, and Non-Compliance in Hospital Accreditation
“[…] in my routine, I had no trouble [implementing] many changes, especially because I was admitted while the accreditation was being implemented.”(Physiotherapist at hospital B)
“[…] you can’t fake all the protocols at all. You need to have an organized process. Now… it’s logical that, after the assessments are completed, you relax… After all, you can’t monitor everyone all the time, so it’s very difficult for you to maintain all the protocols. People tend to customize, so you have to keep working.”(Hospital manager A)
“It is very difficult to get the accreditation certificate. But it is ten times harder to maintain it. We lose and regain processes all the time. We have to be sensitive and aware [to discern] when we lose the process. When we lose, everybody loses, it happens. You have to see if you are missing an important process that will affect something significant. It’s difficult to maintain it. It is hard to attain it, but that’s not the hardest part.”(Hospital manager D)
“[…] There was a period when they had to make changes in my department that required a substantial financial investment, which was not immediately approved, so the accreditation process was halted for a while until the hospital fulfilled the requirements.”(Nurse 1 Hospital A)
4.5. Conflicts over Means and Goals in Hospital Accreditation
“During the accreditation process, there were changes in leadership. Until the new management understood and ratified the process […], there were several elections along the way […] changes in nursing leadership, changes in nursing directors […] Then, there was a discontinuity, a disrupture in the process.”(Hospital manager C)
“Shortly after José Serra became the Minister of Health, he mandated that we obtain certification from ONA. Despite our belief that the CBA is superior to ONA for several reasons, we underwent evaluation by ONA under the Ministry’s directive. After the change in government, we no longer required ONA and reverted to JCI (CBA). Later, we scheduled a visit and obtained accreditation through CBA.”(Hospital manager C)
“[Researcher’s question] Did the hospital’s certification by ONA owe to external pressure? [Manager D’s answer] Yes. Otherwise, we wouldn’t have changed. With the change in management and, consequently, the change in certification, there were days when 29 auditors were working at the same time. We couldn’t work. It was a very troubled period.”(Hospital manager D)
“The accreditation manual was updated last year, so we anticipate that the accreditation process will be less challenging next year. However, some workers have abandoned certain procedures. When you are close to achieving certification, you may need to catch up on these procedures to successfully obtain it. Therefore, the process is slow and requires a systematic approach. It demands organization […].”(Hospital manager A)
“For instance, I saw a hospital that had been ISO-certified for eight years. When they kicked off the accreditation process, they already had well-structured documentation. But it still took them almost three years to achieve accreditation. Since there is so much more detail about patient care but not necessarily about documentation, I saw [the case of] a hospital that took nine years. But with great difficulty [anyway].”(ONA Auditor)
“The hospitals I worked at achieved accreditation. Three private hospitals where I started working from the first day. One took two and a half years, another three and a half years, and the third three years. All three attained accreditation certification. In this one public hospital, I worked for seven years on the accreditation process. After I left, it took another two years to complete the accreditation […].”(CBA Auditor)
“Over time, of course, you will say that there was no resistance… Of course, there was some resistance, but [it was] because it was the will of management, and we said it was something important, people understood. So, the decoding [the idea] that this [process] is going to improve the quality of patient care is important. So, obviously, when we are visited today, there is no stress… But it was stressful. My God, how is this or that process? That no longer exists because it has already become part of everyday life.”(Hospital manager A)
“The accreditation certificate is sometimes seen as a bargain. If the worker does what is required, then he wants something else. They don’t have to want anything! When we explained to them that what the protocol requires is what we must do.”(Hospital manager A)
5. Developing Empirical Propositions on Logic Conflicts and Demand Nature in Hospital Accreditation
“Sometimes we have to include bosses in these groups if they are not contributing effectively.”(Hospital manager C)
“The mobility of professionals has made it difficult, not just for physicians. In the administration, there is often a sentiment of resistance towards these professionals [physicians].”(Hospital manager D)
“We only stopped the process when we had to put off the auditors’ visit to evaluate the protocols, for in the last week, we had to make many adjustments that required a huge expense. This took a while to be approved.”(Hospital manager D)
“Obtaining the hospital accreditation certificate is not cheap. It’s not cheap because it involves money that must be paid for the methodology. It involves paying for international certification agency auditors. When we have a problem with the budget, this creates an interruption in the process.”(Hospital manager C)
6. Discussion
6.1. Summary of Findings and Theoretical and Practical Implications
6.2. Limitations and Suggestions for Future Studies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Analytical Category Scores (MCA)
| Variable | Category | Dimension 1 | Dimension 2 | Frequency |
| Adoption Objective | Efficiency | −0.8257674762 | −0.0533433566 | 28 |
| Adoption Objective | Legitimacy | −1.103079125 | −0.294654722 | 7 |
| Strategic Response | Conformity | −0.544897165 | −0.438805406 | 3 |
| Strategic Response | Customization | 0.318283225 | −0.281455581 | 14 |
| Strategic Response | Non-Conformity | 2.557873692 | −3.887091214 | 3 |
| Institutional Logic | Market | 2.479505625 | −3.627207731 | 4 |
| Institutional Logic | Professional | 1.02216587 | 1.063648106 | 27 |
| Nature of Demands | Means | 0.974744716 | 1.024762878 | 29 |
| Nature of Demands | Goals | 1.699802394 | −2.365275414 | 4 |
References
- Anthony, D.L.; Appari, A.; Johnson, M.E. Institutionalizing HIPAA Compliance. J. Health Soc. Behav. 2014, 55, 108–124. [Google Scholar] [CrossRef] [PubMed]
- Conceição, A.; Picoito, C.; Major, M. Implementing an Hospital Accreditation Programme in a Context of NPM Reforms: Pressures and Conflicting Logics. Public. Money Manag. 2022, 44, 244–251. [Google Scholar] [CrossRef]
- Corrêa, J.; Turrioni, J.; Mello, C.; Santos, A.; da Silva, C.; de Almeida, F. Development of a System Measurement Model of the Brazilian Hospital Accreditation System. Int. J. Environ. Res. Public Health 2018, 15, 2520. [Google Scholar] [CrossRef] [PubMed]
- Mansour, W.; Boyd, A.; Walshe, K. The Development of Hospital Accreditation in Low- and Middle-Income Countries: A Literature Review. Health Policy Plan. 2020, 35, 684–700. [Google Scholar] [CrossRef] [PubMed]
- Mosadeghrad, A.M. Hospital Accreditation: The Good, the Bad, and the Ugly. Int. J. Healthc. Manag. 2021, 14, 1597–1601. [Google Scholar] [CrossRef]
- El-Jardali, F.; Jamal, D.; Dimassi, H.; Ammar, W.; Tchaghchaghian, V. The Impact of Hospital Accreditation on Quality of Care: Perception of Lebanese Nurses. Int. J. Qual. Health Care 2007, 20, 363–371. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, J.L.C.; Gabriel, C.S.; Fertonani, H.P.; Matsuda, L.M. Management Changes Resulting from Hospital Accreditation. Rev. Lat. Am. Enferm. 2017, 25, e2851. [Google Scholar] [CrossRef]
- Brubakk, K.; Vist, G.E.; Bukholm, G.; Barach, P.; Tjomsland, O. A Systematic Review of Hospital Accreditation: The Challenges of Measuring Complex Intervention Effects. BMC Health Serv. Res. 2015, 15, 280. [Google Scholar] [CrossRef]
- Greenfield, D.; Braithwaite, J. Health Sector Accreditation Research: A Systematic Review. Int. J. Qual. Health Care 2008, 20, 172–183. [Google Scholar] [CrossRef]
- Cain, C.L. Agency and Change in Healthcare Organizations: Workers’ Attempts to Navigate Multiple Logics in Hospice Care. J. Health Soc. Behav. 2019, 60, 3–17. [Google Scholar] [CrossRef]
- Friedland, R.; Alford, R. Bringing Society Back in: Symbols, Practices, and Institutional Contradictions. In The New Institutionalism in Organizational Analysis; Powell, W.W., DiMaggio, P.J., Eds.; University of Chicago Press: Chicago, IL, USA, 1991; pp. 232–263. [Google Scholar]
- Thornton, P.H.; Ocasio, W.; Lounsbury, M. The Institutional Logics Perspective; Oxford University Press: Oxford, UK, 2012; ISBN 9780199601936. [Google Scholar]
- Andersson, T.; Liff, R. Co-Optation as a Response to Competing Institutional Logics: Professionals and Managers in Healthcare. J. Prof. Organ. 2018, 5, 71–87. [Google Scholar] [CrossRef]
- Cappellaro, G.; Tracey, P.; Greenwood, R. From Logic Acceptance to Logic Rejection: The Process of Destabilization in Hybrid Organizations. Organ. Sci. 2020, 31, 415–438. [Google Scholar] [CrossRef]
- Kodeih, F.; Greenwood, R. Responding to Institutional Complexity: The Role of Identity. Organ. Stud. 2014, 35, 7–39. [Google Scholar] [CrossRef]
- Kyratsis, Y.; Atun, R.; Phillips, N.; Tracey, P.; George, G. Health Systems in Transition: Professional Identity Work in the Context of Shifting Institutional Logics. Acad. Manag. J. 2017, 60, 610–641. [Google Scholar] [CrossRef]
- Pouthier, V.; Steele, C.W.J.; Ocasio, W. From Agents to Principles: The Changing Relationship between Hospitalist Identity and Logics of Health Care. In Institutional Logics in Action, Part A; Emerald Group Publishing Limited: Bingley, UK, pp. 203–241.
- Reay, T.; Goodrick, E.; Casebeer, A.; Hinings, C.R. (Bob) Legitimizing New Practices in Primary Health Care. Health Care Manag. Rev. 2013, 38, 9–19. [Google Scholar] [CrossRef]
- Yang, C.-W.; Fang, S.-C.; Huang, W.-M. Isomorphic Pressures, Institutional Strategies, and Knowledge Creation in the Health Care Sector. Health Care Manag. Rev. 2007, 32, 263–270. [Google Scholar] [CrossRef]
- Gray, C.S.; Berta, W.; Deber, R.; Lum, J. Organizational Responses to Accountability Requirements. Health Care Manag. Rev. 2017, 42, 65–75. [Google Scholar] [CrossRef]
- Oliver, C. Strategic Responses to Institutional Processes. Acad. Manag. Rev. 1991, 16, 145. [Google Scholar] [CrossRef]
- Da Silva, B.N.; Abbas, K.; Crubellate, J.M. Lógicas Institucionais Na Mensuração e Gestão de Custos Em Hospitais Acreditados. Contab. Gestão Governança 2021, 24, 349–369. [Google Scholar] [CrossRef]
- Pache, A.-C.; Santos, F. When Worlds Collide: The Internal Dynamics of Organizational Responses to Conflicting Institutional Demands. Acad. Manag. Rev. 2010, 35, 455–476. [Google Scholar] [CrossRef]
- Riessman, C.K. Strategic Uses of Narrative in the Presentation of Self and Illness: A Research Note. Soc. Sci. Med. 1990, 30, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Friedland, R.; Mohr, J.W.; Roose, H.; Gardinali, P. The Institutional Logics of Love: Measuring Intimate Life. Theory Soc. 2014, 43, 333–370. [Google Scholar] [CrossRef]
- Besharov, M.L.; Smith, W.K. Multiple Institutional Logics in Organizations: Explaining Their Varied Nature and Implications. Acad. Manag. Rev. 2014, 39, 364–381. [Google Scholar] [CrossRef]
- Skelcher, C.; Smith, S.R. Theorizing Hybridity: Institutional Logics, Complex Organizations, and Actor Identities: The Case of Nonprofits. Public Adm. 2015, 93, 433–448. [Google Scholar] [CrossRef]
- Waldorff, S.B.; Reay, T.; Goodrick, E. A Tale of Two Countries: How Different Constellations of Logics Impact Action. In Institutional Logics in Action, Part A; Emerald Group Publishing Limited: Bingley, UK, 2013; Volume 39, pp. 99–129. [Google Scholar]
- DiMaggio, P.J.; Powell, W.W. The Iron Cage Revisited: Institutional Isomorphism and Collective Rationality in Organizational Fields. Am. Sociol. Rev. 1983, 48, 147–160. [Google Scholar] [CrossRef]
- Boxenbaum, E.; Jonsson, S. Isomorphism, Diffusion and Decoupling: Concept Evolution and Theoretical Challenges. In The Sage Handbook of Organizational Institutionalism; Sage Publications: London, UK, 2017; Volume 2, pp. 77–101. [Google Scholar]
- Alford, R.; Friedland, R. Powers of Theory: Capitalism, the State, and Democracy; Cambridge University Press: Cambridge, UK, 1985. [Google Scholar]
- Thornton, P.H.; Ocasio, W. Institutional Logics. In The SAGE Handbook of Organizational Institutionalism; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2008; pp. 99–128. [Google Scholar]
- Pache, A.-C.; Santos, F. Inside the Hybrid Organization: Selective Coupling as a Response to Competing Institutional Logics. Acad. Manag. J. 2013, 56, 972–1001. [Google Scholar] [CrossRef]
- Shea, C.M.; Turner, K.; Albritton, J.; Reiter, K.L. Contextual Factors That Influence Quality Improvement Implementation in Primary Care: The Role of Organizations, Teams, and Individuals. Health Care Manag. Rev. 2018, 43, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Ruef, M.; Scott, W.R. A Multidimensional Model of Organizational Legitimacy: Hospital Survival in Changing Institutional Environments. Adm. Sci. Q. 1998, 43, 877. [Google Scholar] [CrossRef]
- Westphal, J.D.; Gulati, R.; Shortell, S.M. Customization or Conformity? An Institutional and Network Perspective on the Content and Consequences of TQM Adoption. Adm. Sci. Q. 1997, 42, 366. [Google Scholar] [CrossRef]
- Rossoni, L.; Poli, I.T.; Fogliatti de Sinay, M.C.; Aguiar de Araújo, G. Materiality of Sustainable Practices and the Institutional Logics of Adoption: A Comparative Study of Chemical Road Transportation Companies. J. Clean. Prod. 2020, 246, 119058. [Google Scholar] [CrossRef]
- Scott, W.R. Institutions and Organizations: Ideas and Interests; SAGE: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Borowska, M.; Religioni, U.; Augustynowicz, A. Patients’ Opinions on the Quality of Services in Hospital Wards in Poland. Int. J. Environ. Res. Public Health 2022, 20, 412. [Google Scholar] [CrossRef] [PubMed]
- Quartz-Topp, J.; Sanne, J.M.; Pöstges, H. Hybrid Practices as a Means to Implement Quality Improvement: A Comparative Qualitative Study in a Dutch and Swedish Hospital. Health Care Manag. Rev. 2018, 43, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Feldman, L.B.; Gatto, M.A.F.; Cunha, I.C.K.O. História Da Evolução Da Qualidade Hospitalar: Dos Padrões a Acreditação. Acta Paul. Enferm. 2005, 18, 213–219. [Google Scholar] [CrossRef]
- Alonso, L.B.N.; Droval, C.; Ferneda, E.; Emidio, L. Acreditação Hospitalar e a Gestão Da Qualidade Dos Processos Assistenciais. Perspect. Gestão Conhecimento 2014, 4, 34–49. [Google Scholar]
- Rossoni, L.; Teixeira, R.M. A Interação Dos Relacionamentos Com Os Recursos e a Legitimidade No Processo de Criação de Uma Organização Social. Cadernos EBAPE.BR 2008, 6, 1–19. [Google Scholar] [CrossRef]
- Scott, W.R. Health Care Organizations in the 1980s: The Convergence of Public and Professional Control Systems. In Organizational Environments: Ritual and Rationality; Sage Publications: Thousand Oaks, CA, USA, 1983. [Google Scholar]
- Scott, W.R. Institutional Change and Healthcare Organizations: From Professional Dominance to Managed Care; University of Chicago Press: Chicago, IL, USA, 2000. [Google Scholar]
- Scott, W.R. Lords of the Dance: Professionals as Institutional Agents. Organ. Stud. 2008, 29, 219–238. [Google Scholar] [CrossRef]
- Suchman, M.C. Managing Legitimacy: Strategic and Institutional Approaches. Acad. Manag. Rev. 1995, 20, 571. [Google Scholar] [CrossRef]
- Meyer, J.W.; Rowan, B. Institutionalized Organizations: Formal Structure as Myth and Ceremony. Am. J. Sociol. 1977, 83, 340. [Google Scholar] [CrossRef]
- de Acreditação-ONA, O.N. Manual Brasileiro de Acreditação Hospitalar; ONA: Toronto, ON, USA, 2014. [Google Scholar]
- Mohr, J.W.; White, H.C. How to Model an Institution. Theory Soc. 2008, 37, 485–512. [Google Scholar] [CrossRef]
- Breiger, R.L.; Mohr, J.W. Institutional Logics from the Aggregation of Organizational Networks: Operational Procedures for the Analysis of Counted Data. Comput. Math. Organ. Theory 2004, 10, 17–43. [Google Scholar] [CrossRef]
- Flick, U. An Introduction to Qualitative Research; Sage Publications: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Yin, R. Case Study Research: Design and Methods; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Eisenhardt, K.M.; Graebner, M.E. Theory Building from Cases: Opportunities And Challenges. Acad. Manag. J. 2007, 50, 25–32. [Google Scholar] [CrossRef]
- Reay, T.; Jones, C. Qualitatively Capturing Institutional Logics. Strateg. Organ. 2016, 14, 441–454. [Google Scholar] [CrossRef]
- Eisenhardt, K.M.; Graebner, M.E.; Sonenshein, S. Grand Challenges and Inductive Methods: Rigor without Rigor Mortis. Acad. Manag. J. 2016, 59, 1113–1123. [Google Scholar] [CrossRef]
- Cunliffe, A.L.; Alcadipani, R. The Politics of Access in Fieldwork. Organ. Res. Methods 2016, 19, 535–561. [Google Scholar] [CrossRef]
- Crowe, S.; Cresswell, K.; Robertson, A.; Huby, G.; Avery, A.; Sheikh, A. The case study approach. BMC Med. Res. Methodol. 2011, 11, 100. [Google Scholar] [CrossRef] [PubMed]
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2019; ISBN 9781506395661. [Google Scholar]
- Weber, K.; Patel, H.; Heinze, K.L. From Cultural Repertoires to Institutional Logics: A Content-Analytic Method; Emerald Group Publishing Limited: Bingley, UK, 2013; pp. 351–382. [Google Scholar]
- Krippendorff, K. The Reliability of Generating Data; Chapman and Hall/CRC: Boca Raton, FL, USA, 2022; ISBN 9781003112020. [Google Scholar]
- Oleinik, A. Mixing Quantitative and Qualitative Content Analysis: Triangulation at Work. Qual. Quant. 2011, 45, 859–873. [Google Scholar] [CrossRef]
- Stamenkov, G. Recommendations for Improving Research Quality: Relationships among Constructs, Verbs in Hypotheses, Theoretical Perspectives, and Triangulation. Qual. Quant. 2023, 57, 2923–2946. [Google Scholar] [CrossRef]
- Di Franco, G. Multiple Correspondence Analysis: One Only or Several Techniques? Qual. Quant. 2016, 50, 1299–1315. [Google Scholar] [CrossRef]
- Bourdieu, P. Distinction: A Social Critique of the Judgment of Taste; Harvard University Press: Cambridge, UK, 2002. [Google Scholar]
- Weise, A.; Büchter, R.B.; Pieper, D.; Mathes, T. Assessing Transferability in Systematic Reviews of Health Economic Evaluations—A Review of Methodological Guidance. BMC Med. Res. Methodol. 2022, 22, 52. [Google Scholar] [CrossRef]
- Hays, D.G.; McKibben, W.B. Promoting Rigorous Research: Generalizability and Qualitative Research. J. Couns. Dev. 2021, 99, 178–188. [Google Scholar] [CrossRef]
- Tsang, E.W.K. Generalizing from Research Findings: The Merits of Case Studies. Int. J. Manag. Rev. 2014, 16, 369–383. [Google Scholar] [CrossRef]
- de Oliveira, J.L.C.; Matsuda, L.M. Disqualification of Certification by Hospital Accreditation: Perceptions of Professional Staff. Texto Contexto-Enferm. 2016, 25. [Google Scholar] [CrossRef]
- de Sousa Vilela, G.; Ferraz, C.M.L.C.; de Araújo Moreira, D.; Brito, M.J.M. Expressões Da Ética e Do Di Stresse Moral Na Prática Do Enfermeiro Intensivista. Acta Paul. Enferm. 2021, 34, 406–415. [Google Scholar] [CrossRef]
- Lewis, K.; Hinchcliff, R. Hospital Accreditation: An Umbrella Review. Int. J. Qual. Health Care 2023, 35, mzad007. [Google Scholar] [CrossRef] [PubMed]
- Arman, R.; Liff, R.; Wikström, E. The Hierarchization of Competing Logics in Psychiatric Care in Sweden. Scand. J. Manag. 2014, 30, 282–291. [Google Scholar] [CrossRef]
- Xing, Y.; Liu, Y.; Lattemann, C. Institutional Logics and Social Enterprises: Entry Mode Choices of Foreign Hospitals in China. J. World Bus. 2020, 55, 100974. [Google Scholar] [CrossRef]
- Tolbert, P.S.; Zucker, L.G. Institutional Sources of Change in the Formal Structure of Organizations: The Diffusion of Civil Service Reform, 1880–1935. Adm. Sci. Q. 1983, 28, 22. [Google Scholar] [CrossRef]
- Scott, W.R.; Meyer, J.W. The Organization of Societal Sectors: Propositions and Early Evidence. In The New Institutionalism in Organizational Analysis; Powell, W.W., DiMaggio, P., Eds.; University of Chicago Press: Chicago, IL, USA, 1991; pp. 108–142. [Google Scholar]

| Logic | Market | Professional |
|---|---|---|
| Guidance | Focuses on business strategies, market competition, and return on investment. | Based on norms and standards established by professional health associations and bodies. |
| Main Emphasis | Maximizing operational efficiency and financial profitability. | Providing high-quality healthcare based on best practices and professional standards. |
| Motivation | Obtaining profit, optimizing resources, and expanding the market. | Commitment to professional ethics, continuous improvement in the quality of care, and patient well-being. |
| Threats | Increased costs and loss of customers. | Reduction in the quality of services and professional malpractice. |
| Basis of authority | Owners, investors, and managers. | Professionals with the most outstanding technical and scientific reputations, especially physicians and nurses. |
| Source of Legitimacy | Position of the hospital in the market compared to other competitors. | Status of the hospital in the professional community, available resources, and structure quality. |
| Performance Measurement | Based on financial indicators such as profit margins, revenue, and market share. | Based on quality indicators, patient satisfaction, and adherence to professional standards. |
| Decision Making | Considerations regarding efficiency, competition, and financial return often guide strategic decisions. | Physicians and healthcare professionals frequently make clinical and operational decisions to meet patient needs best. |
| Organizational structure | Organizational structure is often oriented toward management, finance, and operations functions. | Organizations are often structured around medical specialties and multidisciplinary teams. |
| Relationship with Patients | Attention to customer satisfaction, attracting and retaining patients, and maximizing the customer life cycle. | Focus on providing high-quality care and building trusting relationships with patients. |
| Regulation | Subject to government regulations, including compliance with health laws and healthcare regulations. | Subject to professional regulations, standards of practice, and healthcare licensing bodies. |
| Underlying Logic | Managerial | Healthcare |
| Hospital, Nature, Year of Foundation and Accreditor | Interviewed | Number of Interviews | Total Recording Time |
|---|---|---|---|
| A (Private), 1988, ONA | Manager A | 4 | 236 min |
| Physician A | 2 | 54 min | |
| Nurse 1 A | 2 | 55 min | |
| Nurse 2 A | 3 | 41 min | |
| B (Private), 1930, CBA | Manager B | 4 | 190 min |
| Physician B | 1 | 25 min | |
| Physiotherapist B | 2 | 74 min | |
| Nurse B | 1 | 22 min | |
| C (Public), 1994, ONA | Manager C | 5 | 274 min |
| Physician C | 2 | 49 min | |
| Nurse 1 C | 1 | 81 min | |
| Nurse 2 C | 3 | 171 min | |
| D (Public), 1900, CBA | Manager D | 4 | 212 min |
| Physician 1 D | 1 | 12 min | |
| Physician 2 D | 2 | 44 min | |
| Nurse 2 C | 2 | 87 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, T.M.R.d.; Rossoni, L. How Professional and Market Logics and the Conflict between Institutional Demands Affect Hospital Accreditation Compliance: A Multiple-Case Study in Brazil. Healthcare 2024, 12, 914. https://doi.org/10.3390/healthcare12090914
Silva TMRd, Rossoni L. How Professional and Market Logics and the Conflict between Institutional Demands Affect Hospital Accreditation Compliance: A Multiple-Case Study in Brazil. Healthcare. 2024; 12(9):914. https://doi.org/10.3390/healthcare12090914
Chicago/Turabian StyleSilva, Tiago Martins Ramos da, and Luciano Rossoni. 2024. "How Professional and Market Logics and the Conflict between Institutional Demands Affect Hospital Accreditation Compliance: A Multiple-Case Study in Brazil" Healthcare 12, no. 9: 914. https://doi.org/10.3390/healthcare12090914
APA StyleSilva, T. M. R. d., & Rossoni, L. (2024). How Professional and Market Logics and the Conflict between Institutional Demands Affect Hospital Accreditation Compliance: A Multiple-Case Study in Brazil. Healthcare, 12(9), 914. https://doi.org/10.3390/healthcare12090914