Abstract
Objective: The objective of this study was to determine the effectiveness of the conservative Schroth method in patients with adolescent idiopathic scoliosis. Methods: A total of 34 respondents, 24 male and 10 female, aged between 11 and 16 years, participated in the research. The study was a single-blind randomized trial, in which subjects were divided into control and experimental groups by stratified randomization according to the stratum of the Cobb angle. The control group performed the Schroth method at home without the supervision of Schroth therapists, while the experimental group performed the Schroth method under the supervision of Schroth therapists three times a week for 90 min over eight weeks. Initial and final outcome measurements were performed: Cobb angle, angle of trunk rotation, vital capacity, forced vital capacity, forced expiratory volume in the first second, the percentage of forced expiratory volume in the first second in forced vital capacity, and chest expansion. Results: There was a statistically significant improvement in all measured outcomes in the experimental group, while no statistically significant changes were recorded in the control group. The Cobb angle decreased by 2.12°, while ATR decreased by 2.88°; VC increased by 0.15 L, FVC by 0.13 L, FEV1 by 0.1 L, and CE increased by 0.78 cm. Conclusions: The application of an eight-week therapy program using Schroth method by subjects with adolescent idiopathic scoliosis had statistically significant changes in all measured outcomes in the group that was supervised by Schroth’s therapists, while there was no statistically significant improvement in the group that applied therapy at home without supervision.
1. Introduction
Idiopathic scoliosis is a complex deformity of the spine that develops three-dimensionally and results in the appearance of frontal curves, fixed rotations of the vertebrae, and flattening of the sagittal physiological curves [1]. When scoliosis develops between 10 years of age and the end of growth, it is called adolescent idiopathic scoliosis (AIS) [2]. Despite extensive clinical, epidemiological, and basic science research, the etiopathogenesis of AIS remains unknown [3]. AIS is often seen in multiple members of the same family, strongly suggesting that it has a genetic component [4]. The prevalence of AIS is 2% to 3% in the general population, of which nearly 10% require some form of treatment, and up to 0.1% of these will require surgery [5]. When a diagnosis of scoliosis is made, the primary concern is whether there is an underlying cause and whether the curve will progress. The three main determinants of progression are the gender of the patient, future growth potential, and the size of the curve at the time of diagnosis [6,7,8]. The greater the growth potential and the greater the curve, the greater the likelihood of curve progression. The magnitude of the curve tends to increase throughout the lifespan, but the degree of progression over the lifetime and time at risk vary depending on many factors [9,10]. The Risser score (from 0 to 5) provides a useful estimate of how much skeletal growth remains by assessing the progress of bony fusion of the iliac apophysis [11]. In a study [12], the Risser score was directly correlated with the risk of curve progression. The risk of curve progression can also be assessed by taking into account the gender of the patient and the time of menarche. This information does not ultimately determine whether a particular curve will progress, but only the general risk of curve progression [13,14].
Early diagnosis of scoliosis is essential to initiate a timely and appropriate treatment, preventing potential respiratory, psychological, and social complications associated with the condition [15]. Depending on the magnitude of the curve, treatment approaches consist of different types of exercises, wearing a brace, and surgery for the deformity caused by AIS [16]. Stopping the progression of the curve in puberty, preventing or treating respiratory dysfunction, preventing or treating spinal pain syndrome, and improving aesthetics through postural correction are the main goals of applying various conservative treatments [9]. The most commonly used conservative methods are: Schroth method, scientific exercise approach to scoliosis (SEAS), Lyon method which is combined with Lyon brace, and core stabilization exercises [17,18,19,20,21].
The Schroth method was developed by Katharina Schroth in 1920 and has been continuously improved through the treatment of approximately 3000 cases of scoliosis per year. The principles of active 3D posture correction, corrective breathing and correction of postural perception, form the basis of what is known as the Schroth method as a treatment of scoliosis [22]. The method aims to derotate, elongate, and stabilize the spine through individualized exercises tailored to the patient’s specific curve pattern. A key component of the Schroth method is rotational angular breathing, a specialized technique that encourages expansion of the concave side of the ribcage, which is typically compressed due to scoliosis. Combined with targeted postural adjustments, this breathing technique helps improve lung function, rib mobility, and overall spinal alignment. Additionally, Schroth therapy places a strong emphasis on sensorimotor training, helping patients develop a conscious awareness of their spinal position to actively maintain a corrected posture in daily activities. Schroth’s classification system is derived from Schroth’s principle of dividing the body into blocks [23]. According to Schroth’s classification system, different types of scoliosis always start with a large curve followed by relevant secondary curves [22]. The exercises are customized based on the specific curve pattern, ensuring an individualized approach to treatment. There are numerous studies that confirm the positive effects in the treatment of idiopathic scoliosis using the Schroth method [18,24,25,26,27,28,29,30,31,32]. The primary goal of this study is to evaluate the effectiveness of the Schroth method as a conservative treatment for AIS by assessing its impact on key clinical and functional parameters. Specifically, we aim to determine whether the structured application of Schroth exercises can lead to reduction in spinal curvature (Cobb angle), improvement in trunk alignment (angle of trunk rotation, ATR), and enhancement of pulmonary function (vital capacity, VC; forced vital capacity, FVC; forced expiratory volume in one second, FEV1; and the FEV1/FVC ratio). Additionally, we assess the method’s influence on chest expansion (CE) as an indicator of thoracic mobility and respiratory efficiency. A secondary objective is to compare the effectiveness of supervised Schroth therapy (performed under the guidance of a trained therapist in a clinical setting) versus self-administered home-based Schroth exercises. By examining differences in treatment outcomes between these two approaches, this study seeks to determine whether guided professional supervision leads to superior therapeutic benefits compared to independent practice at home. Based on prior research and clinical experience, we hypothesize that the Schroth method will significantly improve scoliosis-related parameters in AIS patients, leading to: a reduction in Cobb angle, indicating structural improvement in spinal alignment; a decrease in the ATR reflecting better postural symmetry; an increase in VC, FVC, and FEV1, demonstrating improved respiratory function; enhanced CE, suggesting greater thoracic mobility and breathing efficiency. Supervised Schroth therapy will yield superior results compared to self-administered home-based exercises, as professional guidance ensures: more precise execution of exercises with real-time corrections; greater adherence to the prescribed treatment regimen; and improved neuromuscular engagement and postural re-education, leading to more effective long-term results.
2. Materials and Methods
2.1. Study Design
The study was designed as a randomized, single-blind, 1:1 parallel-group trial conducted at Scolio Centar in Novi Sad between March and June 2023. Ethical approval was obtained from the Ethics Committee of the Faculty of Sports and Physical Education at the University of Novi Sad (Approval No: 49-02-04/2023-1). Prior to participation, informed consent was obtained from the parents of all participants. The study included children diagnosed with adolescent idiopathic scoliosis (AIS), aged between 10 and 18 years, with a Cobb angle greater than 10 degrees and a Risser sign between 0 and 5. Participants who had previously undergone any form of scoliosis treatment were excluded from the study. Additional exclusion criteria included the presence of contraindications for exercise, psychological disorders, neuromuscular diseases, and a history of spinal surgery. Throughout the study, participants did not use braces.
2.2. Sample Size and Randomization
The sample size calculation was conducted using G*Power software (version 3.1.9.7, Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) [33]. To achieve a statistical power of 80% (1 − β error probability) at a significance level of α = 0.05, a repeated-measures analysis of variance (ANOVA) was performed. Based on the expected moderate effect size of 0.3, the required sample size was estimated at 24 participants. However, to enhance statistical power and reliability, the study included as many eligible participants as possible without violating the methodological framework, resulting in a total of 34 subjects. Participants were randomly assigned to one of two groups: an experimental group that received supervised Schroth therapy in a clinical setting and a control group that performed Schroth exercises at home without direct supervision. The randomization process was stratified based on the Cobb angle and executed using Microsoft Excel (2016). Allocation concealment was ensured by using sealed envelopes that were opened only at the moment of participant enrollment. To maintain objectivity, all baseline and post-treatment assessments were conducted by a blinded investigator (B.O.), who was unaware of the group assignments throughout the study.
2.3. Outcome Measurements
The primary outcome measure in this study was the Cobb angle, which was assessed using a standard anterior–posterior standing radiograph of the entire spine [34]. The angle of trunk rotation (ATR) was measured with a Bunnell scoliometer while the participant was in a forward bending position, with the device placed centrally over the spine. The ATR is expressed in degrees [35]. Pulmonary function was assessed by measuring vital capacity (VC), forced vital capacity (FVC), and forced expiratory volume in one second (FEV1) using a Spirolab portable spirometer (MIR, Rome, Italy). These pulmonary measurements were performed in an upright position, with each test repeated three times and the average value recorded. Additionally, chest expansion was evaluated manually with a tape measure positioned at the junction between the xiphoid process and the sternum.
2.4. Interventions
The intervention period lasted eight weeks and included a total of 24 sessions. Participants in the experimental group performed supervised Schroth exercises under the guidance of a certified physiotherapist (N.J.), attending 90 min training sessions three times per week. These exercises were specifically designed to improve trunk symmetry and included a combination of stretching, flexion, spinal elongation, derotation, strengthening, and rotational breathing techniques [22]. The control group, on the other hand, received initial instructions from the same physiotherapist on how to perform Schroth exercises independently at home. They were encouraged to practice as consistently as possible, following the prescribed regimen. The full details of the Schroth exercise program are provided in Appendix A.
2.5. Statistical Analysis
Statistical analysis was conducted using SPSS Statistics for Windows (version 26.0, IBM Corp., 2010, Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro–Wilk test, confirming that all measured outcomes followed a normal distribution. To compare baseline characteristics between the experimental and control groups, an independent T-test was used for continuous variables, while categorical variables were analyzed using Pearson’s chi-square test. For ordinal variables, the Mann–Whitney test was applied. To evaluate changes over time and differences between groups, a mixed-model ANOVA was employed. Prior to conducting ANOVA, two key assumptions were tested: Levene’s test for equality of variance and Box’s M test for equality of covariance. The assumption of equal covariances was not met for the VC outcome, and neither assumption was met for the FEV1/FVC ratio. Consequently, Pillai’s trace, a more robust alternative to Wilks’ lambda, was utilized for these analyses [36]. The effect sizes were reported using partial eta squared (η2), with threshold values set at 0.10 for small, 0.25 for medium, and 0.40 for large effect [37]. The level of statistical significance was set at p < 0.05 for all analyses.
3. Results
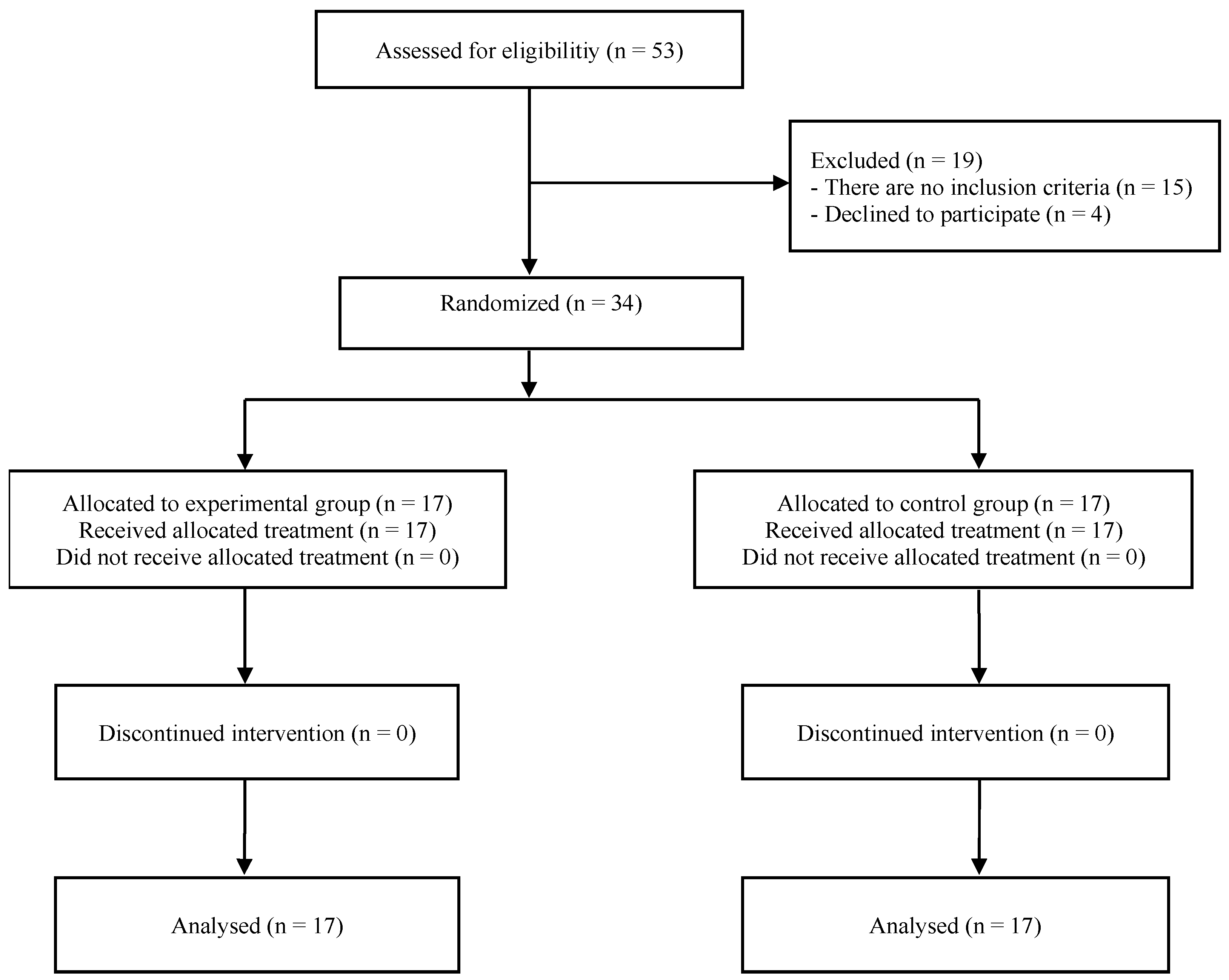
Fifty-three respondents who had scoliosis were admitted to the department, and forty-three respondents met the conditions to be included in the research. After randomization, patients were assigned n = 17 to EG and n = 17 to CG. All subjects who started the study completed the intended treatment in full. The research flow diagram is shown in Figure 1. In a sample of 34 subjects randomly distributed in EG and CG, there was basically no significant difference between the groups in age, weight, Cobb angle, and Risser sign. There was a statistically significant difference in height and body mass index (Table 1). For the Cobb angle, the interaction between group and time showed an effect size of η2 = 0.57, which, according to Cohen’s guidelines, represents a large effect size (Table 2). This indicates a meaningful improvement in spinal curvature in the experimental group, suggesting that the Schroth method is highly effective in correcting spinal deformities compared to the control group. A significant separate (basic) influence of time was also determined, F = 34.51; p = 0.000; η2 = 0.52. Regarding the ATR, the effect size of η2 = 0.61 also falls within the large effect size category (Table 2). This substantial reduction in ATR in the experimental group implies that the Schroth method significantly enhances spinal alignment and posture. A significant separate (basic) influence of time was also determined, F = 46.43; p = 0.000; η2 = 0.59. For respiratory function outcomes, the results were similarly impactful. Vital capacity (VC): The effect size of η2 = 0.53 is considered large, indicating that the Schroth method substantially improves lung capacity (Table 2). A significant separate (basic) influence of time was also determined, F = 50.82; p = 0.000; η2 = 0.61. Forced vital capacity (FVC): With an effect size of η2 = 0.66, this outcome also shows a large effect, suggesting significant benefits to respiratory efficiency (Table 2). A significant separate (basic) effect of time was also determined, F = 78.66; p = 0.000; η2 = 0.71. Forced expiratory volume in one second (FEV1): The large effect size of η2 = 0.67 supports that the Schroth method effectively enhances respiratory muscle strength (Table 2). A significant separate (basic) influence of time was also determined, F = 73.86; p = 0.000; η2 = 0.7. Chest expansion (CE): The effect size of η2 = 0.78 is well above the threshold for a large effect, highlighting the substantial positive impact of the Schroth method on thoracic mobility and respiratory function (Table 2). A significant separate (basic) influence of time was also determined, F = 164.74; p = 0.000; η2 = 0.84. In contrast, the FEV1/FVC ratio showed no significant interaction, with an effect size of η2 = 0.05, which Cohen’s guidelines classify as no effect (Table 2). This suggests that while the Schroth method improves individual respiratory measures, it does not significantly influence the ratio between FEV1 and FVC.
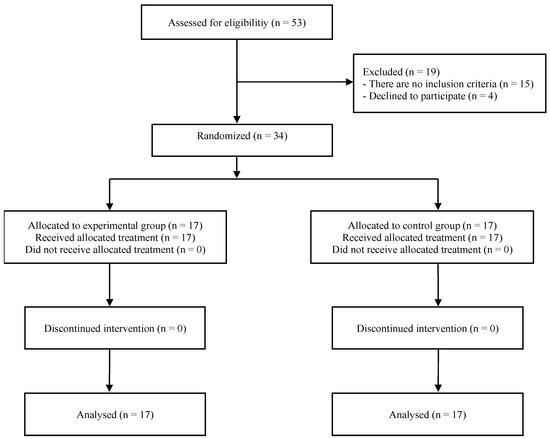
Figure 1.
Flow diagram of the participants.

Table 1.
Demographic and baseline clinical characteristics.
Table 2.
Summary of findings for group–time interaction.
4. Discussion
The results of our research show compliance with the set hypothesis that the application of the Schroth method under the supervision of a physiotherapist in clinical conditions has positive effects in slowing down and stopping scoliosis, reducing the Cobb angle, ATR, and improving pulmonary function. The Schroth method, under the supervision of a physiotherapist in clinical conditions, has better effects than the application of the same method in home conditions.
In the treatment of AIS as a pathology of unknown cause, surgical and non-surgical (conservative) methods are used. Despite the great advances in technology and science, operative approaches to treatment are not completely safe, so the risks of side effects can often lead to abandoning this type of treatment. Timely detection of scoliosis is crucial for preventing serious complications, with rehabilitation specialists playing a vital role in halting the progression of the condition [15]. Of all the conservative methods, the Schroth method has the largest number of published studies. Unlike other scientific fields, the amount of such research is still relatively small, and with this research, we tried to make a small contribution, so that the effects of applying conservative methods (primarily the Schroth method) in the treatment of AIS could be seen in an even better way. The main clinical and prognostic indications in the study of AIS are the Cobb angle and ATR [38]. All approaches and strategies that slow the progression of scoliosis and prevent the need for surgery are important in the treatment of AIS [39]. In our research, the Cobb angle decreased only in the experimental group by 2.12° (from 30.18 ± 8.19° to 28.06 ± 7.99°), which was recorded as statistically significant. Our results are similar to the results of the study [18], which conducted a six-month treatment and recorded the greatest reduction in the Cobb angle in the first six weeks of treatment. This study applied the same weekly intensity as our study. The study by [27], which was the only one like ours to use an eight-week program with three sessions per week, but each lasting 60 min, reported a 2.69° reduction in the Cobb angle in seven subjects, which largely coincides with our results. The study by [40] recorded a reduction in the Cobb angle by 2.65°, after an intensive six-week program carried out in five weekly sessions, and the results of this study largely coincide with our results. Other studies [26,27,28,29,30] report a generally greater reduction in the Cobb angle, and their results do not match our results. A study [41] that also applied an eight-week treatment with core stabilization exercises recorded similar results to ours, while other studies [42,43] that applied this method recorded greater reductions in the Cobb angle. Regarding other exercise-based conservative methods, the study [44] reports similar results to ours, while studies [45] report greater reductions in the Cobb angle. ATR, as the second most important indicator of idiopathic scoliosis and as the first diagnostic procedure, statistically significantly decreased only in EG, by 2.88° (from 11.24 ± 4.18° to 8.35 ± 3.18°). Our results almost completely coincide with the results of a study [30] that reports a reduction in ATR by 2.82°, while the results of other studies [24,28,46] have greater or lesser differences. In curves involving the thoracic spine, the mobility of the chest wall is reduced, and secondary effects of reduced spinal flexibility appear as a disorder [47,48]. VC is inversely correlated with the amount of curvature up to a Cobb angle of 10°. Even when resting VC is found to be normal, reduced exercise capacity is demonstrated even in children with mild curvatures (Cobb angle 5–20°) [49]. With the Schroth method, progress is made through rotational breathing techniques, where inhaled air is directed toward the concave sides of the chest and ribs to lengthen and mobilize the soft tissues in these areas [49]. This process provides the patient with proprioceptive enhancement of the sensation of spinal derotation and also helps to eliminate further inhalation of the convexity. This principle is an essential component of the Schroth method because the muscles in the convex areas are overstretched and unable to retract properly during exhalation [46]. In our research, the aforementioned was confirmed by recording a decrease in the Cobb angle and ATR, followed by an increase in VC, only in EG, by 0.16 l (from 2.81 ± 0.66 to 2.97 ± 0.65), which in our case recorded as a statistically significant increase. A study by [40] noted the same increase in VC after the first six weeks of intensive Schroth therapy. Of the other conservative exercise-based methods, only one study [45], examines this outcome and records a greater increase than our study. VC is a very suitable index for determining restrictive pulmonary function [50] but it is a rarely used outcome in published research. Just as VC is negatively correlated with the size of the curve, so is FVC, another important respiratory parameter, negatively correlated with the size of the curve in AIS [51]. With a greater degree of curvature, there is greater decrease in respiratory function as measured by FVC [52]. The study [53] confirms this correlation. In our case, the increase in FVC was statistically significant only in EG. At the initial measurement, the subjects had an average value of 2.51 L, and at the end of the eight-week treatment 2.63 L, which represents a difference of 0.12 L. The study by [46] recorded an improvement in FVC results by 0.10 L after applying the treatment. The study by [27] recorded better results of FVC by 0.33 L after the application of the Schroth method, which was followed by additional respiratory exercises using the SpiroTiger device (Idiag, Fehraltorf, Switzerland). Using other exercise-based methods, studies [45,54] report greater improvements in this outcome than ours. The recorded reduction of the Cobb angle and ATR, as in the case of VC, led to better results in the final measurement. As in the case of VC and FVC, the ratio of FEV1 is negatively correlated with the size of the curve, which means that a higher degree of the curve is accompanied by a lower value of FEV1 [52]. It is certain that the higher position of the curve reduces all the examined respiratory parameters to a greater degree, which is consistent with what the previously mentioned study stated—that there are greater deficits in patients with a thoracic curve. When idiopathic scoliosis affects the thoracic region, it can cause a rotational deformity that affects the shape and position of the chest. This, in turn, can affect breathing mechanics and potentially lead to reduced pulmonary function. Decreased pulmonary capacity can lead to a decrease in FEV1. In our research, FEV1 increased statistically significantly after treatment only in the experimental group by 0.1 l (from 2.2 ± 0.49 to 2.3 ± 0.48). The study by [46] recorded an improvement in FEV1 results by 0.09 L after applying the treatment. The study by [27] recorded better results of FEV1 by 0.39 L after the application of the Schroth method, which was followed by additional respiratory exercises. As for the previous outcome, studies [45,54] record better results in this outcome as well. As with the previous respiratory parameters, FEV1 increased after the reduction of the Cobb angle and ATR, and in this case, confirmed a negative correlation in relation to the size of the curve. The FEV1/FVC ratio, in the context of idiopathic scoliosis, may be relevant in cases where the curvature of the spine affects the thoracic region and potentially affects pulmonary function. Severe scoliosis can lead to changes in the shape and position of the chest, which can limit pulmonary expansion and compromise respiratory function. In our research, the FEV1/FVC ratio decreased statistically significantly only in the experimental group by 0.01, that is, by 1% (from 0.88 ± 0.01 to 0.87 ± 0.02). In the study by [27], FEV1/FVC ratio increased by 3.76%. Chest expansion (CE) is an important measurement in the evaluation of scoliosis because it provides valuable information about the effect of spinal curvature on respiratory function. AIS, especially when it affects the thoracic region, can lead to changes in the shape and position of the chest, potentially limiting pulmonary expansion during breathing. In our research, CE increased statistically significantly only in the experimental group by 0.78 cm, (from 6.26 ± 0.89 to 7.04 ± 0.84). In the study by [46], CE increased by 1.31 cm. The study by [55] records an increase in CE by 1.27 cm. Limited chest expansion may indicate reduced pulmonary capacity and reduced respiratory function. As scoliosis progresses and the curvature of the spine becomes greater, there may be a restriction of the space available for pulmonary expansion, leading to a decrease in pulmonary volume and potential respiratory limitations. Monitoring chest expansion over time can help healthcare providers monitor changes in respiratory function and determine the progression of respiratory impairment associated with AIS. The number of studies with which we compared our results highlights the limited number of studies that examined pulmonary function in patients with idiopathic scoliosis. The results we obtained in our research are in agreement with the results of our meta-analysis [56,57], which confirmed the positive effects of the Schroth method on patients with idiopathic scoliosis.
4.1. Clinical Implications
Reduction in spinal deformity: The experimental group showed significant decreases in the Cobb angle compared to the control group, emphasizing the effectiveness of the Schroth method in mitigating scoliosis progression. This is crucial for reducing the need for surgical interventions. Improvement in trunk alignment: significant improvements in the ATR were observed in the EG, suggesting enhanced postural symmetry and better cosmetic outcomes, essential for patient confidence and quality of life. Respiratory function enhancement: substantial improvements in VC, FVC, and FEV1 indicate the positive impact of the Schroth method on respiratory health, which is often compromised in AIS due to thoracic deformities.
Limited impact on FEV1/FVC ratio: the lack of significant changes in the FEV1/FVC ratio suggests that while overall respiratory capacity improved, relative airway function remained stable. Improved chest expansion: chest expansion (CE) significantly improved in the EG, reflecting enhanced thoracic mobility and better functional capacity, crucial for physical activity and overall well-being. Feasibility and adherence: the completion rate of 100% in both groups highlights the practicality and acceptability of the Schroth method for adolescents, making it a viable long-term treatment option.
4.2. Recommendations for Future Practice
Integration into routine care: the Schroth method should be incorporated into standard conservative management protocols for AIS to improve spinal alignment and prevent progression. Focus on early intervention: initiating the Schroth method early in the disease process may yield better Cobb angle reduction, trunk rotation, and respiratory function outcomes. Holistic treatment approach: combining the Schroth method with other conservative treatments, such as bracing or physical therapy, may optimize outcomes and address both structural and functional impairments in AIS. Tailored interventions: individualized treatment plans should account for differences in height, body mass index, and severity of scoliosis to maximize the method’s effectiveness. Long-term follow-up: future clinical practice should include long-term monitoring of patients to assess the durability of improvements in spinal curvature, respiratory function, and quality of life. Expanded research: further studies should explore the long-term impacts of the Schroth method, its effectiveness in severe scoliosis cases, and its integration with other therapeutic modalities. Development of guidelines: Evidence-based clinical guidelines should be developed to standardize the application of the Schroth method across healthcare settings.
4.3. Strengths and Limitations
The randomized controlled design ensured a high level of evidence by minimizing bias and improving the reliability of the results. Supervised Schroth therapy allowed for standardized execution of exercises, ensuring adherence and maximizing treatment effectiveness. Comprehensive outcome assessment, including spinal alignment (Cobb angle, angle of trunk rotation) and respiratory function (vital capacity, forced vital capacity, forced expiratory volume in one second, chest expansion), provided a holistic evaluation of the Schroth method’s impact. Complete follow-up with no dropouts increased the validity of the findings, eliminating concerns about attrition bias. This study has several limitations. First, the number of subjects included in the study is relatively small. Second, although the biggest changes were noted in the first weeks of treatment, we could say that eight weeks of treatment is still a short period. Third, after eight weeks of treatment, there was no follow-up period to quantitatively record further changes. Fourth, the lack of a home exercise group means that the study does not address the effectiveness of unsupervised Schroth exercises compared to supervised therapy. Fifth, the absence of a brace-wearing comparison group could provide insights into whether Schroth therapy alone is sufficient for cases requiring conservative management. Our research is the first such research conducted in Serbia, so we hope to correct all these shortcomings in our next research.
5. Conclusions
The results of this randomized controlled trial demonstrate that the Schroth method is an effective conservative treatment for adolescent idiopathic scoliosis, leading to significant improvements in spinal curvature, postural alignment, and respiratory function compared to the control group. Participants in the experimental group, who performed Schroth exercises under therapist supervision, showed a statistically significant reduction in the Cobb angle (p = 0.000) and angle of trunk rotation (p = 0.000), while no significant changes were observed in the control group. This confirms the corrective effect of Schroth-specific exercises on three-dimensional spinal deformity. Furthermore, the Schroth method significantly improved pulmonary function parameters, including vital capacity (p = 0.000), forced vital capacity (p = 0.000), and forced expiratory volume in one second (p = 0.000), suggesting that targeted postural and breathing exercises enhance respiratory mechanics in scoliosis patients. However, the FEV1/FVC ratio did not show significant changes, indicating that while lung volume and expansion improved, the airflow ratio remained stable. A significant increase in chest expansion (p = 0.000) was observed in the experimental group, reinforcing the effectiveness of Schroth-based breathing techniques in improving thoracic mobility and lung capacity. Importantly, all participants completed the intervention, demonstrating high feasibility and adherence to the program. These findings suggest that supervised Schroth therapy is more effective than unsupervised or standard care in managing adolescent idiopathic scoliosis, supporting its integration into conservative treatment protocols (ClinicalTrials.gov ID: NCT06877806).
Author Contributions
Conceptualization, V.D., D.V. and B.O.; methodology, V.D. and M.P.P.; software, D.V.; validation, B.O. and S.P.; formal analysis, N.J. and S.N.; investigation, B.O.; resources, N.J.; data curation, N.J. and S.P.; writing—original draft preparation, V.D.; writing—review and editing, B.R. and S.N.; visualization, V.D. and M.P.P.; supervision, B.O.; project administration, B.R.; funding acquisition, B.O. and B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Provincial Secretariat for Higher Education and Scientific Research of AP Vojvodina, grant number: 142-451-2595.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Faculty of Sports and Physical Education, University of Novi Sad (protocol code 49-02-04/2023-1, approved in 27 February 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Each child’s parent signed an informed consent form before participation.
Data Availability Statement
Any personal or patient data are unavailable due to privacy or ethical restrictions. All other data are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to express our sincere gratitude to Dragan Marinković for his valuable assistance in the registration process, which contributed to the completion of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| IS | Idiopathic scoliosis |
| AIS | Adolescent idiopathic scoliosis |
| CE | Chest expansion |
| CG | Control group |
| FVC | Forced vital capacity |
| FEV1 | Forced expiratory volume in 1 s |
| ATR | Angle of trunk rotation |
| VC | Vital capacity |
| SEAS | Scientific exercises approach to scoliosis |
Appendix A
The following table presents the Schroth experimental program used in the study. This structured program was implemented in the experimental group under the supervision of Schroth therapists.
Table A1.
Schroth Experimental Program.
Table A1.
Schroth Experimental Program.
| Exercise Name | Position | Description (Optional) |
|---|---|---|
| Warm-up | - | General mobilization and activation |
| Side bending | Sitting | Active lateral flexion for scoliosis correction |
| Derotation of the ventral prominence | Supine | Rotation correction of the prominent ribcage |
| Shoulder Counter Traction | Supine | Shoulder stabilization exercise |
| Shoulder Counter Traction | Side | Shoulder traction from a lateral position |
| Shoulder Counter Traction | Prone | Posterior shoulder traction engagement |
| Between two poles | Sitting | Spine elongation and postural awareness |
| Muscle cylinder kneeling | Kneeling | Core engagement and stability training |
| Side plank small | Side-lying | Core and oblique muscle activation |
| Dead bug | Supine | Core stabilization with limb movement |
| Final stretching | - | Flexibility and relaxation exercises |
References
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; De Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [PubMed]
- Asher, M.A.; Burton, D.C. Adolescent idiopathic scoliosis: Natural history and long-term treatment effects. Scoliosis 2006, 1, 2. [Google Scholar] [PubMed]
- Burwell, R.G. Aetiology of idiopathic scoliosis: Current concepts. Pediatr. Rehabil. 2003, 6, 137–170. [Google Scholar]
- Kesling, K.L.; Reinker, K.A. Scoliosis in twins: A meta-analysis of the literature and report of six cases. Spine 1997, 22, 2009–2015. [Google Scholar]
- Lonstein, J.E. Scoliosis: Surgical versus nonsurgical treatment. Clin. Orthop. Relat. Res. 2006, 443, 248–259. [Google Scholar]
- Miller, N.H. Cause and natural history of adolescent idiopathic scoliosis. Orthop. Clin. N. Am. 1999, 30, 343–352. [Google Scholar]
- Dimitrijević, V.; Protic-Gava, B.; Vinaji, T.; Popovic, N. Effects of corrective exercises on kyphotic angle reduction: A systematic review and meta-analysis. Med. Pregl. 2021, 74, 167–173. [Google Scholar]
- Dimitrijević, V.; Šćepanović, T.; Milankov, V.; Milankov, M.; Drid, P. Effects of Corrective Exercises on Lumbar Lordotic Angle Correction: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4906. [Google Scholar] [CrossRef]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Rigo, M.; Weiss, H.R.; the members of the Scientific society On Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis 2005, 1, 4. [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.Y.; Danielsson, A.; Morcuende, J.A. Adolescent Idiopathic Scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar]
- Lonstein, J.E. Adolescent idiopathic scoliosis. Lancet 1994, 344, 1407–1412. [Google Scholar] [CrossRef] [PubMed]
- Lonstein, J.E.; Carlson, J.M. The prediction of curve progression in untreated idiopathic scoliosis during growth. J. Bone Joint Surg. Am. 1984, 66, 1061–1071. [Google Scholar]
- Renshaw, T.S. Idiopathic scoliosis in children. Curr. Opin. Pediatr. 1993, 5, 407–412. [Google Scholar] [PubMed]
- Roach, J.W. Adolescent idiopathic scoliosis. Orthop. Clin. N. Am. 1999, 30, 353–365. [Google Scholar]
- Scaturro, D.; de Sire, A.; Terrana, P.; Costantino, C.; Lauricella, L.; Sannasardo, C.E.; Vitale, F.; Mauro, G.L. Adolescent idiopathic scoliosis screening: Could a school-based assessment protocol be useful for an early diagnosis? J. Back Musculoskelet. Rehabil. 2021, 34, 301–306. [Google Scholar] [PubMed]
- Negrini, S.; Aulisa, A.G.; Aulisa, L.; Circo, A.B.; de Mauroy, J.C.; Durmala, J.; Grivas, T.B.; Knott, P.; Kotwicki, T.; Maruyama, T.; et al. 2011 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 2012, 7, 3. [Google Scholar]
- Ko, K.J.; Kang, S.J. Effects of 12-week core stabilization exercise on the Cobb angle and lumbar muscle strength of adolescents with idiopathic scoliosis. J. Exerc. Rehabil. 2017, 13, 244–249. [Google Scholar] [CrossRef]
- Kuru, T.; Yeldan, I.; Dereli, E.E.; Özdinçler, A.R.; Dikici, F.; Çolak, I. The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: A randomised controlled clinical trial. Clin. Rehabil. 2016, 30, 181–190. [Google Scholar] [CrossRef]
- Lenssinck, M.L.B.; Frijlink, A.C.; Berger, M.Y.; Bierma-Zeinstra, S.M.; Verkerk, K.; Verhagen, A.P. Effect of bracing and other conservative interventions in the treatment of idiopathic scoliosis in adolescents: A systematic review of clinical trials. Phys. Ther. 2005, 85, 1329–1339. [Google Scholar] [CrossRef]
- Negrini, S.; Fusco, C.; Minozzi, S.; Atanasio, S.; Zaina, F.; Romano, M. Exercises reduce the progression rate of adolescent idiopathic scoliosis: Results of a comprehensive systematic review of the literature. Disabil. Rehabil. 2008, 30, 772–785. [Google Scholar]
- Sy, N.; Bettany-Saltikov, J.; Moramarco, M. Evidence for Conservative Treatment of Adolescent Idiopathic Scoliosis—Update 2015. Curr. Pediatr. Rev. 2016, 12, 6–11. [Google Scholar] [PubMed]
- Lehnert-Schroth, C. Three-Dimensional Treatment for Scoliosis: Physiotherapeutic Method for Deformities of the Spine; Martindale Press: Hong Kong, China, 2007; Volume 278. [Google Scholar]
- Weiss, H.R. The method of Katharina Schroth—history, principles and current development. Scoliosis 2011, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Duangkeaw, R.; Laddawong, T.; Numchai, R.; Burawan, P. Effects of three-dimension Schroth exercises and kinesio taping on general mobility of vertebrae, angle of trunk rotation, muscle strength and endurance of trunk, and inspiratory and expiratory muscle strength in children with idiopathic scoliosis. Walailak J. Sci. Technol. 2019, 16, 965–973. [Google Scholar]
- HwangBo, P.-N. Psychological and physical effects of Schroth and Pilates exercise on female high school students with idiopathic scoliosis. J. Korean Phys. Ther. 2016, 28, 364–368. [Google Scholar] [CrossRef]
- Kim, G.; Hwangbo, P.N. Effects of Schroth and Pilates exercises on the Cobb angle and weight distribution of patients with scoliosis. J. Phys. Ther. Sci. 2016, 28, 1012–1015. [Google Scholar]
- Kim, G.; Park, D.-S. The effect of Schroth’s three-dimensional exercises in combination with respiratory muscle exercise on Cobb’s angle and pulmonary function in patients with idiopathic scoliosis. Phys. Ther. Rehabil. Sci. 2017, 6, 113–119. [Google Scholar] [CrossRef]
- Kocaman, H.; Bek, N.; Kaya, M.H.; Büyükturan, B.; Yetiş, M.; Büyükturan, Ö. The effectiveness of two different exercise approaches in adolescent idiopathic scoliosis: A single-blind, randomized-controlled trial. PLoS ONE 2021, 16, e0249492. [Google Scholar] [CrossRef]
- Lee, H.-J.; Lee, S.-M. Effects of Schroth exercise therapy on curvature and body appearance of patients with lumbar idiopathic scoliosis. Phys. Ther. Rehabil. Sci. 2020, 9, 230–237. [Google Scholar]
- Mohamed, R.A.; Yousef, A.M. Impact of Schroth three-dimensional vs. proprioceptive neuromuscular facilitation techniques in adolescent idiopathic scoliosis: A randomized controlled study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7717–7725. [Google Scholar]
- Schreiber, S.; Parent, E.C.; Moez, E.K.; Hedden, D.M.; Hill, D.; Moreau, M.J.; Lou, E.; Watkins, E.M.; Southon, S.C. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis-an assessor and statistician blinded randomized controlled trial: ‘SOSORT 2015 Award Winner’. Scoliosis 2015, 10, 24. [Google Scholar]
- Schreiber, S.; Parent, E.C.; Moez, E.K.; Hedden, D.M.; Hill, D.L.; Moreau, M.; Lou, E.; Watkins, E.M.; Southon, S.C. Schroth physiotherapeutic scoliosis-specific exercises added to the standard of care lead to better Cobb angle outcomes in adolescents with idiopathic scoliosis—An assessor and statistician blinded randomized controlled trial. PLoS ONE 2016, 11, e0168746. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Deacon, P.; Flood, B.M.; Dickson, R.A. Idiopathic scoliosis in three dimensions. A radiographic and morphometric analysis. J. Bone Jt. Surg. Ser. B 1984, 66, 509–512. [Google Scholar] [CrossRef]
- Bunnell, W.P. Selective screening for scoliosis. Clin. Orthop. Relat. Res. 2005, 434, 40–45. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: London, UK, 2013. [Google Scholar] [CrossRef]
- Maher, J.M.; Markey, J.C.; Ebert-May, D. The other half of the story: Effect size analysis in quantitative research. CBE Life Sci. Educ. 2013, 12, 345–351. [Google Scholar]
- Horne, J.P.; Flannery, R.; Usman, S. Adolescent idiopathic scoliosis: Diagnosis and management. Am. Fam. Physician 2014, 89, 193–198. [Google Scholar] [PubMed]
- Nachemson, A.L.; Peterson, L. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J. Bone Jt. Surg. Am. 1995, 77, 815–822. [Google Scholar] [CrossRef]
- Otman, S.; Kose, N.; Yakut, Y. The efficacy of Schroth’s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey. Saudi Med. J. 2005, 90, 277–283. [Google Scholar]
- Park, S.W.; Kwon, J.; Heo, Y.C.; Yu, W. Effect of core stabilization exercise on cobb’s angle and balance of scoliosis patients. Ann. Rom. Soc. Cell Biol. 2021, 25, 922–926. [Google Scholar]
- Park, Y.H.; Park, Y.S.; Lee, Y.T.; Shin, H.S.; Oh, M.K.; Hong, J.; Lee, K.Y. The effect of a core exercise program on Cobb angle and back muscle activity in male students with functional scoliosis: A prospective, randomized, parallel-group, comparative study. J. Int. Med. Res. 2016, 44, 728–734. [Google Scholar]
- Gür Gözde Ayhan, C.; Yakut, Y. The effectiveness of core stabilization exercise in adolescent idiopathic scoliosis: A randomized controlled trial. Prosthet. Orthot. Int. 2017, 41, 303–310. [Google Scholar]
- Langensiepen, S.; Stark, C.; Sobottke, R.; Semler, O.; Franklin, J.; Schraeder, M.; Siewe, J.; Eysel, P.; Schoenau, E. Home-based vibration assisted exercise as a new treatment option for scoliosis—A randomised controlled trial. J. Musculoskelet. Neuronal Interact. 2017, 17, 259–267. [Google Scholar] [PubMed]
- Kumar, A.; Kumar, S.; Sharma, V.; Srivastava, R.N.; Gupta, A.K.; Parihar, A.; Verma, V.; Kumar, D. Efficacy of task oriented exercise program based on ergonomics on cobb’s angle and pulmonary function improvement in adolescent idiopathic scoliosis-a randomized control trial. J. Clin. Diagnostic Res. 2019, 11, YC01–YC04. [Google Scholar] [CrossRef]
- Moramarco, M.; Fadzan, M.; Moramarco, K.; Heller, A.; Righter, S. The Influence of Short-Term Scoliosis-Specific Exercise Rehabilitation on Pulmonary Function in Patients with AIS. Curr. Pediatr. Rev. 2015, 12, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.C. The use of exercises in the treatment of scoliosis: An evidence-based critical review of the literature. Pediatr. Rehabil. 2003, 6, 171–182. [Google Scholar] [CrossRef]
- Lin, M.C.; Liaw, M.Y.; Chen, W.J.; Cheng, P.T.; Wong AM, K.; Chiou, W.K. Pulmonary function and spinal characteristics: Their relationships in persons with idiopathic and postpoliomyelitic scoliosis. Arch. Phys. Med. Rehabil. 2001, 82, 335–341. [Google Scholar] [CrossRef]
- Weiss, H.R. Rehabilitation of adolescent patients with scoliosis—What do we know? A review of the literature. Pediatr. Rehabil. 2003, 6, 183–194. [Google Scholar] [CrossRef]
- Weiss, H.R. Effect of the Exercise Program on the Vital Capacity and Rib Mobility. Spine 1991, 16, 88–93. [Google Scholar] [CrossRef]
- Johari, J.; Sharifudin, M.; Ab Rahman, A.; Omar, A.; Abdullah, A.; Nor, S.; Lam, W.; Yusof, M. Relationship between pulmonary function and degree of spinal deformity, location of apical vertebrae and age among adolescent idiopathic scoliosis patients. Singapore Med. J. 2016, 57, 33–38. [Google Scholar] [CrossRef]
- Vitale, M.G.; Matsumoto, H.; Bye, M.R.; Gomez, J.A.; Booker, W.A.; Hyman, J.E.; Roye, D.P., Jr. A retrospective cohort study of pulmonary function, radiographic measures, and quality of life in children with congenital scoliosis: An evaluation of patient outcomes after early spinal fusion. Spine 2008, 33, 1242–1249. [Google Scholar] [CrossRef]
- León-Morillas, F.; de Oliveira-Sousa, S.L.; Andrade-Ortega, J.A.; Ibáñez-Vera, A.J.; Lomas-Vega, R.; Zagalaz-Anula, N. The type of conservative management could be related to the strength of the inspiratory muscles of adolescents with idiopathic scoliosis—A case series. Children 2021, 8, 1002. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Bin Song, G.; Park, E.C. Effects of Swiss ball exercise and resistance exercise on respiratory function and trunk control ability in patients with scoliosis. J. Phys. Ther. Sci. 2015, 27, 1775–1778. [Google Scholar] [CrossRef] [PubMed]
- Vrećić, A.; Glišić, M.; Živković, V. Significance of Schroth method in the rehabilitation of children with structural idiopathic scoliosis. Med. Podml. 2020, 71, 33–38. [Google Scholar] [CrossRef]
- Dimitrijević, V.; Viduka, D.; Šćepanović, T.; Maksimović, N.; Giustino, V.; Bianco, A.; Drid, P. Effects of Schroth method and core stabilization exercises on idiopathic scoliosis: A systematic review and meta-analysis. Eur. Spine J. 2022, 31, 3500–3511. [Google Scholar] [CrossRef]
- Dimitrijević, V.; Šćepanović, T.; Jevtić, N.; Rašković, B.; Milankov, V.; Milosević, Z.; Ninković, S.S.; Chockalingam, N.; Obradović, B.; Drid, P. Application of the Schroth Method in the Treatment of Idiopathic Scoliosis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 16730. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).