
Enhancing Health Literacy and Self-Management in Glaucoma Patients: Evidence from a Nurse-Led Educational Intervention
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Material and Methods
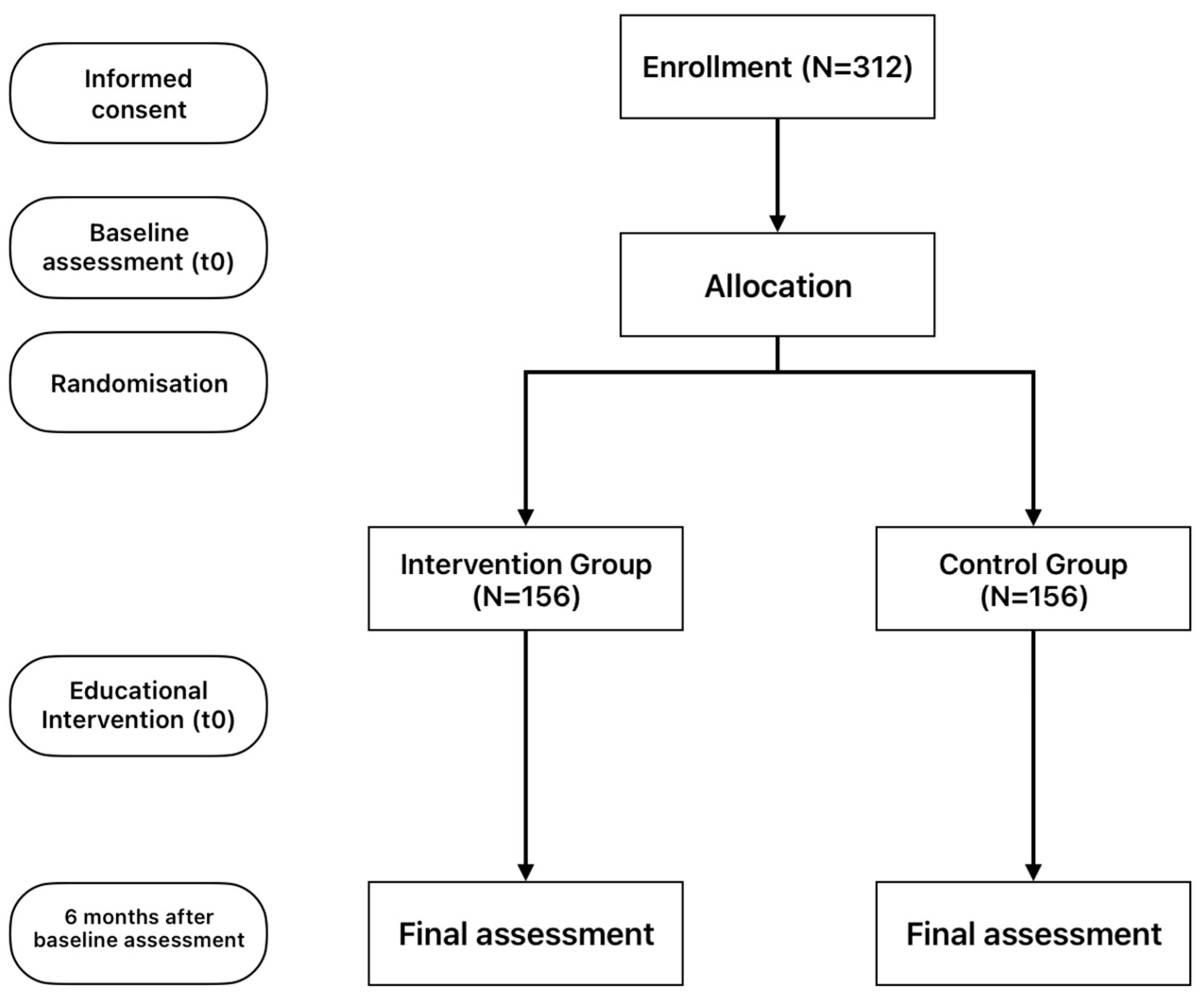
2.1. Study Design
2.2. Description of This Study’s Intervention
2.3. Data Collection and Instruments
2.3.1. European Health Literacy Survey Questionnaire 16 (HLS-EU-16)
2.3.2. The Patient Activation Measure-13 (PAM-13)
2.4. Statistical Analysis
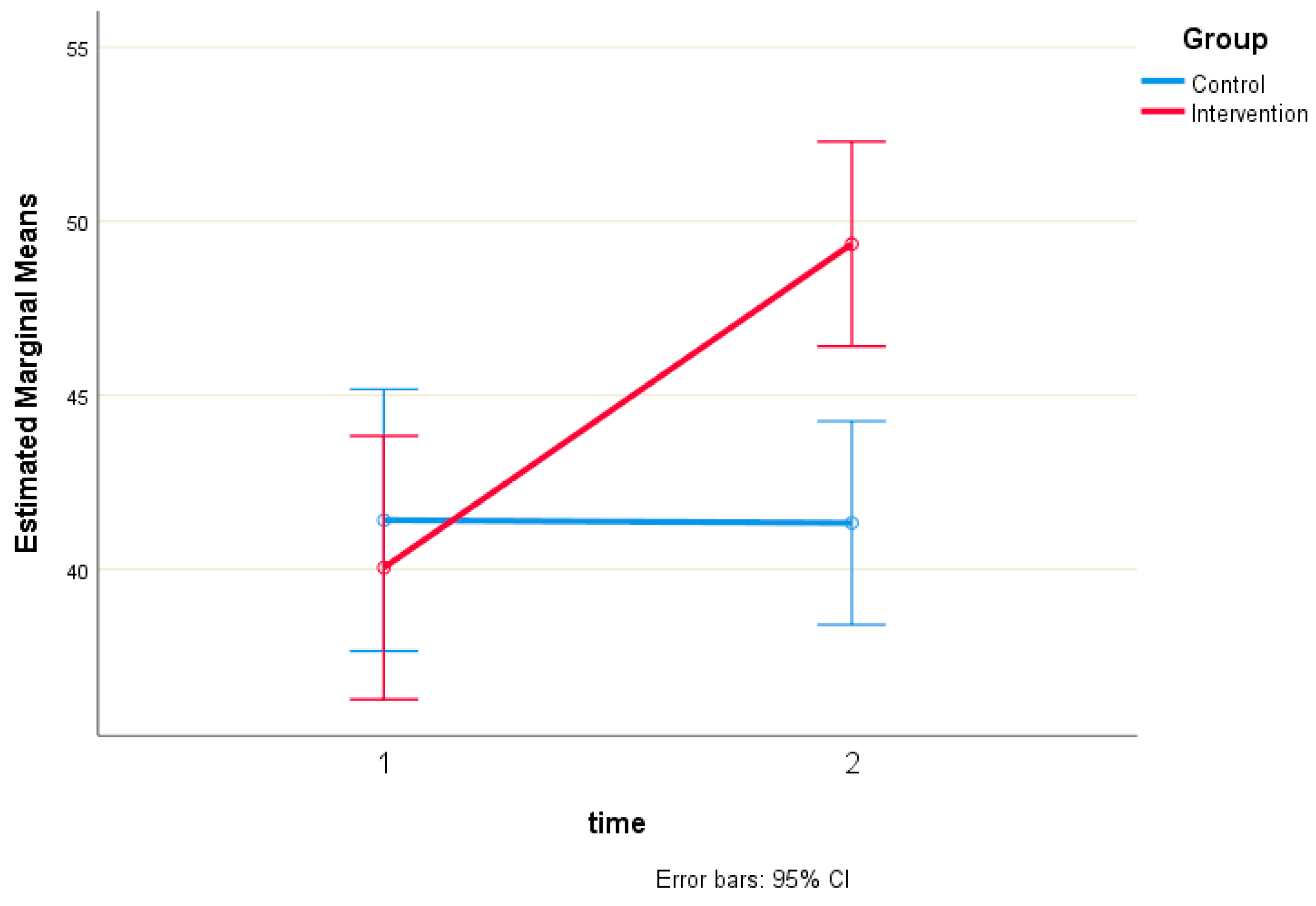
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma: A Review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Baker, D.W.; Wolf, M.S.; Feinglass, J.; Thompson, J.A.; Gazmararian, J.A.; Huang, J. Health literacy and mortality among elderly persons. Arch. Intern. Med. 2007, 167, 1503–1509. [Google Scholar] [CrossRef]
- Newman-Casey, P.A.; Robin, A.L.; Blachley, T.; Farris, K.; Heisler, M.; Resnicow, K.; Lee, P.P. The Most Common Barriers to Glaucoma Medication Adherence: A Cross-Sectional Survey. Ophthalmology 2015, 122, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Muir, K.W.; Lee, P.P. Health literacy and ophthalmic patient education. Surv. Ophthalmol. 2010, 55, 454–459. [Google Scholar] [CrossRef]
- Wolf, M.S.; Gazmararian, J.A.; Baker, D.W. Health literacy and functional health status among older adults. Arch. Intern. Med. 2005, 165, 1946–1952. [Google Scholar] [CrossRef]
- George, A.K.; Homme, R.P.; Stanisic, D.; Tyagi, S.C.; Singh, M. Protecting the aging eye with hydrogen sulfide. Can. J. Physiol. Pharmacol. 2021, 99, 161–170. [Google Scholar] [CrossRef]
- Tsai, J.C.; McClure, C.A.; Ramos, S.E.; Schlundt, D.G.; Pichert, J.W. Compliance barriers in glaucoma: A systematic classification. J. Glaucoma 2003, 12, 393–398. [Google Scholar] [CrossRef]
- Tham, Y.C.; Cheng, C.Y. Associations between chronic systemic diseases and primary open angle glaucoma: An epidemiological perspective. Clin. Exp. Ophthalmol. 2017, 45, 24–32. [Google Scholar] [CrossRef]
- DS, F. Doctor-patient communication, health-related beliefs, and adherence in glaucoma. Results from the Glaucoma Adherence and Persistency Study. Ophthalmology 2008, 115, 1320–1327. [Google Scholar]
- Qu, N.; You, W. Design and fault diagnosis of DCS sintering furnace’s temperature control system for edge computing. PLoS ONE 2021, 16, e0253246. [Google Scholar] [CrossRef]
- Naylor, M.D.; Aiken, L.H.; Kurtzman, E.T.; Olds, D.M.; Hirschman, K.B. The care span: The importance of transitional care in achieving health reform. Health Aff. 2011, 30, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.H.; Mahoney, E.R.; Stockard, J.; Tusler, M. Development and testing of a short form of the patient activation measure. Health Serv. Res. 2005, 40, 1918–1930. [Google Scholar] [CrossRef] [PubMed]
- Sleath, B.; Carpenter, D.M.; Blalock, S.J.; Sayner, R.; Muir, K.W.; Slota, C.; Giangiacomo, A.L.; Hartnett, M.E.; Tudor, G.; Robin, A.L. Applying the resources and supports in self-management framework to examine ophthalmologist-patient communication and glaucoma medication adherence. Health Educ. Res. 2015, 30, 693–705. [Google Scholar] [CrossRef]
- Geitona, M.; Latsou, D.; Toska, A.; Saridi, M. Polypharmacy and Adherence Among Diabetic Patients in Greece. Consult. Pharm. 2018, 33, 562–571. [Google Scholar] [CrossRef]
- Malliarou, M.; Bakola, E.; Nikolentzos, A.; Sarafis, P. Reliability and validity of the Greek translation of the patient assessment of chronic illness care + (PACIC-PLUS GR) survey. BMC Fam. Pr. 2020, 21, 122. [Google Scholar] [CrossRef]
- Achilleos, M.; Merkouris, A.; Charalambous, A.; Papastavrou, E. Medication adherence, self-efficacy and health literacy among patients with glaucoma: A mixed-methods study protocol. BMJ Open 2021, 11, e039788. [Google Scholar] [CrossRef]
- Foster, P.J.; Buhrmann, R.; Quigley, H.A.; Johnson, G.J. The definition and classification of glaucoma in prevalence surveys. Br. J. Ophthalmol. 2002, 86, 238–242. [Google Scholar] [CrossRef]
- Shah, N.N.; Bowd, C.; Medeiros, F.A.; Weinreb, R.N.; Sample, P.A.; Hoffmann, E.M.; Zangwill, L.M. Combining structural and functional testing for detection of glaucoma. Ophthalmology 2006, 113, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an Explanatory Framework in Communication Research: Exploring Parallel, Serial, and Moderated Mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef]
- Finset, A. Patients’ values and preferences and communication about life expectancy: Combining honesty and hope. Patient Educ. Couns. 2017, 100, 1777. [Google Scholar] [CrossRef]
- Efthymiou, A.; Middleton, N.; Charalambous, A.; Papastavrou, E. The Association of Health Literacy and Electronic Health Literacy With Self-Efficacy, Coping, and Caregiving Perceptions Among Carers of People With Dementia: Research Protocol for a Descriptive Correlational Study. JMIR Res. Protoc. 2017, 6, e221. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed]
- Tsichla, L.; Patelarou, E.; Detorakis, E.; Tsilimparis, M.; Skatharoudi, C.; Kalaitzaki, M.; Garedaki, Ε.; Giakoumidakis, K. Translation and Validation of the Greek Version of the Patient Activation Measure-13 in Glaucoma Patients. Hell. J. Nurs. 2024, 63, 69–76. [Google Scholar]
- Moljord, I.E.; Lara-Cabrera, M.L.; Perestelo-Perez, L.; Rivero-Santana, A.; Eriksen, L.; Linaker, O.M. Psychometric properties of the Patient Activation Measure-13 among out-patients waiting for mental health treatment: A validation study in Norway. Patient Educ. Couns. 2015, 98, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Insignia Health, L. Patient Activation Measure (PAM) 13 License Materials; Insignia Health: Portland, OR, USA, 2011. [Google Scholar]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef]
- De Sanctis, V.; Soliman, A.T.; Daar, S.; Di Maio, S.; Elalaily, R.; Fiscina, B.; Kattamis, C. Prevalence, attitude and practice of self-medication among adolescents and the paradigm of dysmenorrhea self-care management in different countries. Acta Biomed. 2020, 91, 182–192. [Google Scholar] [CrossRef]
- Walker, C.; Weeks, A.; McAvoy, B.; Demetriou, E. Exploring the role of self-management programmes in caring for people from culturally and linguistically diverse backgrounds in Melbourne, Australia. Health Expect. 2005, 8, 315–323. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient self-management of chronic disease in primary care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Newland, A.; Cronin, C.; Cook, G.; Whitehead, A. Developing Coaches’ Knowledge of the Athlete–Coach Relationship Through Formal Coach Education: The Perceptions of Football Association Coach Developers. Int. Sport Coach. J. 2023, 11, 341–355. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Osborn, C.Y.; Cavanaugh, K.; Wallston, K.A.; Rothman, R.L. Self-efficacy links health literacy and numeracy to glycemic control. J. Health Commun. 2010, 15 (Suppl. S2), 146–158. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Fontes-Garfias, C.R.; Swanson, K.A.; Cai, H.; Sarkar, R.; Chen, W.; Cutler, M.; et al. Neutralizing Activity of BNT162b2-Elicited Serum. N. Engl. J. Med. 2021, 384, 1466–1468. [Google Scholar] [CrossRef]
- Tsai, J.C. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology 2009, 116, S30–S36. [Google Scholar] [CrossRef]
- Briesen, S.; Geneau, R.; Roberts, H.; Opiyo, J.; Courtright, P. Understanding why patients with cataract refuse free surgery: The influence of rumours in Kenya. Trop. Med. Int. Health 2010, 15, 534–539. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; European, C.H.L.P. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- van der Heide, I.; Uiters, E.; Sørensen, K.; Röthlin, F.; Pelikan, J.; Rademakers, J.; Boshuizen, H.; Consortium, E. Health literacy in Europe: The development and validation of health literacy prediction models. Eur. J. Public Health 2016, 26, 906–911. [Google Scholar] [CrossRef]
- Wang, J.; Thombs, B.D.; Schmid, M.R. The Swiss Health Literacy Survey: Development and psychometric properties of a multidimensional instrument to assess competencies for health. Health Expect. 2014, 17, 396–417. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.A.; O’Donoghue, A.C.; Sullivan, H.W.; Willoughby, J.F.; Squire, C.; Parvanta, S.; Betts, K.R. Communicating efficacy information based on composite scores in direct-to-consumer prescription drug advertising. Patient Educ. Couns. 2016, 99, 583–590. [Google Scholar] [CrossRef]
- Pelikan, J.M.; Ganahl, K.; Van den Broucke, S.; Sørensen, K. Measuring health literacy in Europe: Introducing the European health literacy survey questionnaire (HLS-EU-Q). In International Handbook of Health Literacy; Policy Press: Bristol, UK, 2019; pp. 115–138. [Google Scholar]
- Nutbeam, D.; Muscat, D.M. Health promotion glossary 2021. Health Promot. Int. 2021, 36, 1578–1598. [Google Scholar] [CrossRef] [PubMed]
- Robin, A.L.; Novack, G.D.; Covert, D.W.; Crockett, R.S.; Marcic, T.S. Adherence in glaucoma: Objective measurements of once-daily and adjunctive medication use. Am. J. Ophthalmol. 2007, 144, 533–540. [Google Scholar] [CrossRef]
- Caprioli, J.; Coleman, A.L. Intraocular pressure fluctuation a risk factor for visual field progression at low intraocular pressures in the advanced glaucoma intervention study. Ophthalmology 2008, 115, 1123–1129.e1123. [Google Scholar] [CrossRef] [PubMed]
- Asrani, S.; Zeimer, R.; Wilensky, J.; Gieser, D.; Vitale, S.; Lindenmuth, K. Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma. J. Glaucoma 2000, 9, 134–142. [Google Scholar] [CrossRef]
- Newman-Casey, P.A.; Blachley, T.; Lee, P.P.; Heisler, M.; Farris, K.B.; Stein, J.D. Patterns of Glaucoma Medication Adherence over Four Years of Follow-Up. Ophthalmology 2015, 122, 2010–2021. [Google Scholar] [CrossRef]
- Uji, A.; Yoshimura, N. Application of extended field imaging to optical coherence tomography. Ophthalmology 2015, 122, 1272–1274. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| GROUP | |||||||
|---|---|---|---|---|---|---|---|
| Control | Intervention | Total | |||||
| Count | n % | Count | n % | Count | n % | ||
| Biological sex | Female | 63 | 40.1% | 71 | 45.8% | 134 | 42.9% |
| Male | 94 | 59.9% | 84 | 54.2% | 178 | 57.1% | |
| Education level | Primary | 113 | 72.0% | 115 | 74.2% | 228 | 73.1% |
| Secondary | 20 | 12.7% | 24 | 15.5% | 44 | 14.1% | |
| Tertiary | 24 | 15.3% | 16 | 10.3% | 40 | 12.8% | |
| Comorbidity | No | 13 | 8.3% | 12 | 7.7% | 25 | 8.0% |
| Yes | 144 | 91.7% | 143 | 92.3% | 287 | 92.0% | |
| Intervention-Parts | Short Description | Methods/Tools | Expected Outcomes |
|---|---|---|---|
| Training Session | A 15 min session conducted by the first researcher, covering the disease, its treatment, and long-term management. | Researcher-led informational presentation and active participant discussion. | Enhanced patient understanding of the disease and treatment options. |
| Online Videos | Appropriately selected YouTube videos focusing on disease education, treatment, and self-management techniques (with Greek subtitles). | Videos from the World Glaucoma Association, including: “Understanding Glaucoma; World Glaucoma Week 2022; and “Patient Education Movie—World Glaucoma Week 2021“ | Increased patient understanding of disease management through visual content. |
| Printed Material (Brochure) | Provision of a brochure containing essential information about glaucoma, treatment options, and self-management tips. | Printed brochure with text and graphics for patient education. | Improved patient knowledge regarding glaucoma and self-management strategies. |
| Group | p-Value | ||
|---|---|---|---|
| Control | Intervention | ||
| PAM-13 score (pre) | 41.4 ± 24.2 | 40.1 ± 23.7 | p < 0.001 |
| PAM-13 score (post) | 41.3 ± 24.1 | 49.3 ± 10. 4 | |
| HLS-EU16 score (pre) | 10.3 ± 3.8 | 11.1 ± 3.5 | p < 0.001 |
| HLS-EU16 score (post) | 10.5 ± 3.6 | 12.8 ± 2.6 | |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% Confidence Interval for B | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tolerance | VIF | |||
| (Constant) | −2.113 | 8.847 | −0.239 | 0.811 | −19.521 | 15.296 | |||
| HLS-EU16 score (pre) | 3.307 | 0.318 | 0.510 | 10.391 | 0.000 | 2.681 | 3.933 | 0.974 | 1.026 |
| Group | −3.772 | 2.337 | −0.079 | −1.614 | 0.108 | −8.370 | 0.826 | 0.981 | 1.019 |
| Biological sex | −0.900 | 2.351 | −0.019 | −0.383 | 0.702 | −5.526 | 3.726 | 0.989 | 1.011 |
| Age | 0.104 | 0.090 | 0.062 | 1.156 | 0.249 | −0.073 | 0.281 | 0.804 | 1.243 |
| Education level | 3.863 | 1.844 | 0.114 | 2.095 | 0.037 | 0.235 | 7.492 | 0.794 | 1.259 |
| Comorbidity | −2.495 | 4.271 | −0.028 | −0.584 | 0.560 | −10.900 | 5.910 | 0.996 | 1.004 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% Confidence Interval for B | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tolerance | VIF | |||
| (Constant) | 11.868 | 8.453 | 1.404 | 0.161 | −4.765 | 28.501 | |||
| HLS-EU16 score (post) | 1.261 | 0.330 | 0.222 | 3.818 | 0.000 | 0.611 | 1.912 | 0.870 | 1.150 |
| Group | 5.356 | 2.198 | 0.141 | 2.437 | 0.015 | 1.031 | 9.682 | 0.879 | 1.137 |
| Biological sex | 1.187 | 2.100 | 0.031 | 0.565 | 0.572 | −2.946 | 5.320 | 0.983 | 1.018 |
| Age | 0.093 | 0.080 | 0.070 | 1.165 | 0.245 | −0.064 | 0.250 | 0.810 | 1.235 |
| Education level | 2.736 | 1.636 | 0.102 | 1.673 | 0.095 | −0.482 | 5.955 | 0.801 | 1.249 |
| Comorbidity | 0.312 | 3.811 | 0.004 | 0.082 | 0.935 | −7.187 | 7.810 | 0.992 | 1.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsichla, L.; Patelarou, E.; Detorakis, E.; Tsilimbaris, M.K.; Patelarou, A.E.; Giakoumidakis, K. Enhancing Health Literacy and Self-Management in Glaucoma Patients: Evidence from a Nurse-Led Educational Intervention. Healthcare 2025, 13, 861. https://doi.org/10.3390/healthcare13080861
Tsichla L, Patelarou E, Detorakis E, Tsilimbaris MK, Patelarou AE, Giakoumidakis K. Enhancing Health Literacy and Self-Management in Glaucoma Patients: Evidence from a Nurse-Led Educational Intervention. Healthcare. 2025; 13(8):861. https://doi.org/10.3390/healthcare13080861
Chicago/Turabian StyleTsichla, Lοukia, Evridiki Patelarou, Efstathios Detorakis, Miltiadis K. Tsilimbaris, Athina E. Patelarou, and Konstantinos Giakoumidakis. 2025. "Enhancing Health Literacy and Self-Management in Glaucoma Patients: Evidence from a Nurse-Led Educational Intervention" Healthcare 13, no. 8: 861. https://doi.org/10.3390/healthcare13080861
APA StyleTsichla, L., Patelarou, E., Detorakis, E., Tsilimbaris, M. K., Patelarou, A. E., & Giakoumidakis, K. (2025). Enhancing Health Literacy and Self-Management in Glaucoma Patients: Evidence from a Nurse-Led Educational Intervention. Healthcare, 13(8), 861. https://doi.org/10.3390/healthcare13080861