
The Partnering with Patients Model of Nursing Interventions: A First Step to a Practice Theory


Abstract
:1. The Partnering with Patients Model of Nursing Interventions: A First Step to a Practice Theory
2. Background
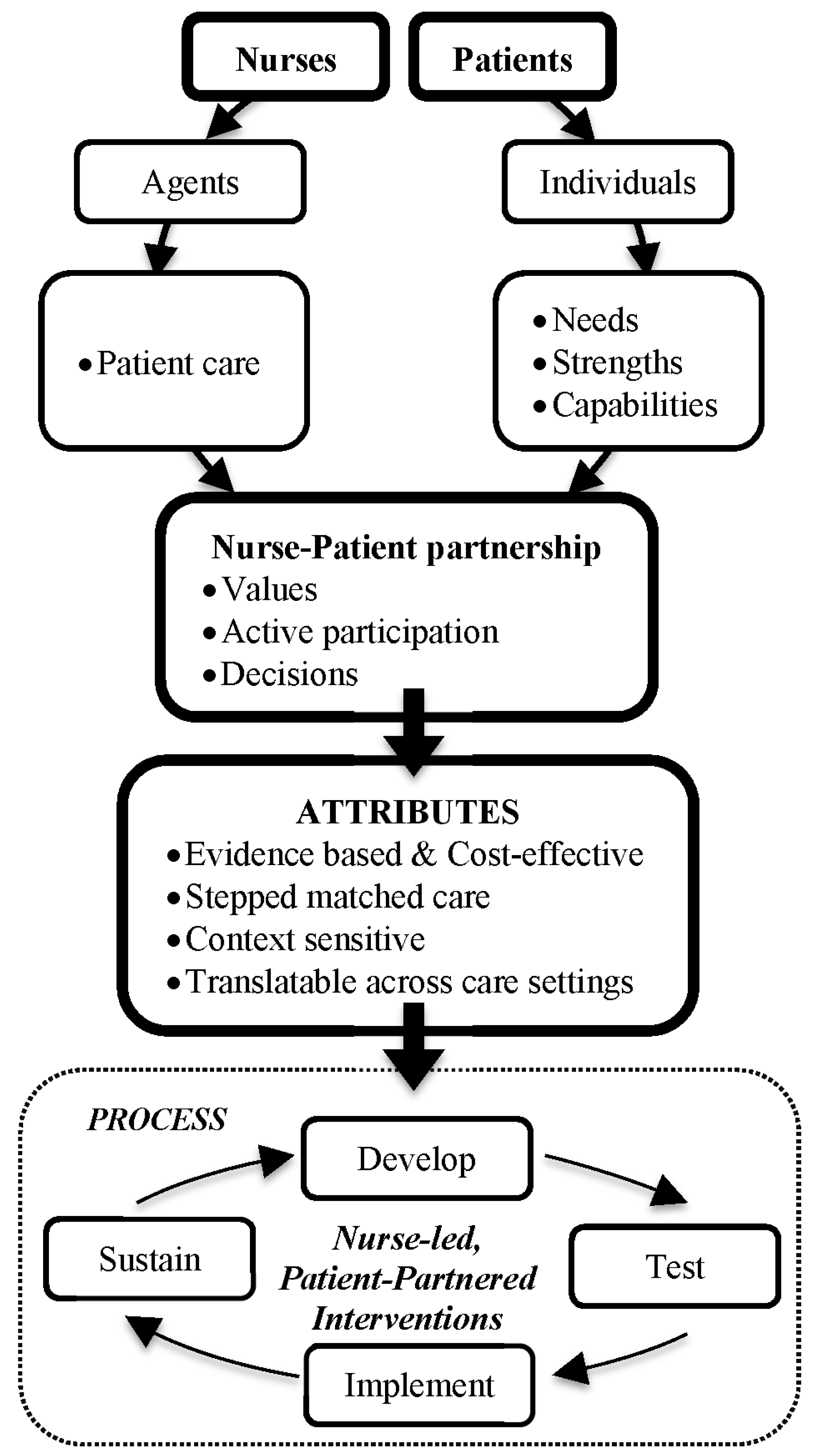
3. The Partnering with Patients Model of Nursing Interventions (PPM-NI)
- People are valued as individuals. As such, their individual strengths and capabilities need to be understood, as these will facilitate active participation in their care;
- Nurses are ‘agents’ who have the capacity to make decisions and act on them to meet the needs of individual patient care (i.e., to deliver an intervention); and
- Nursing care centres on the needs of the person in the moment and how these needs can be met through the care partnership.
- Evidence based;
- Cost effective;
- Patient centred, delivered by nurses in partnership with patients;
- Stepped or tailored to the individuals’ needs, capabilities, goals and to the context, including family involvement;
- Developed and tested in collaboration with end-users (i.e., patients and nurses);
- Applicable across settings; and
- Multi-level, adapted to different levels of intervention targets (patient, ward/department, organisation).

4. Case Study: Joan

{kind=link}
{kind=link}
| Concept | Factors |
|---|---|
| Evidence-based | What level of evidence is available to support the intervention? To what extent does expert consensus guide the intervention? Is there emerging empirical data to support the proposed approach? |
| Cost effective | Considerations of intervention costs and outcomes for patient/family to demonstrate “value for money” and increase sustainability. To what extent are efficiencies evident in the use of resources? |
| Active Partnership | How do both nurses and patients influence the intervention process? Is this process bi-directional? To what extent are patient and nurse values considered in the intervention approach? How is this expressed? Are values explicit or implied? |
| Stepped or Tailored care | Does the intervention respond to patient need in a systematic way? What algorithms and stepping rules are available to direct care in a patient centred approach? To what extend are family involved? |
| Developed and tested with end-users | Were end-users involved in the development and testing of the intervention? How did end users influence the intervention? |
| Translatable across settings | To what extent can the intervention be translated across settings that may vary by geography; care focus; and culture? |
| Multi-level | To what extent does the intervention respond to the context of both the patient and the nurse? Is there a clear pathway to develop, test, implement and sustain the intervention? |

5. Implications for Nursing Practice
6. Recommendations for Nursing Research
- Patients’ perceptions and experiences: Research is needed to understand whether the consumers of nursing interventions can recognise when a PPM-NI approach to their nursing care is experienced. This may be aided by associated work, for example, a comprehensive review of instruments to measure person-centred care noted that while there is no universally accepted definition of the term, and approaches to measure it (or its components) included patient preferences, patient experiences and patient outcomes [26]. Methods to better understand PCC include the use of surveys, interviews (either group or individual) and observation [26]. It may be that for both qualitative research and quantitative research, measuring PCC may help to inform future developments in the PPM-NI.
- Nurses’ perceptions and experiences: Research is also needed to assess nurses’ perception of the applicability of the PPM-NI model to their practice, and to more deeply explore the various concepts in the model and their inter-woven relationships. It may be for example that certain aspects of the model require further refinement, or the relationships between concepts are more complex or multifactorial than we have described here. Integrated knowledge translation, whereby potential research knowledge users are engaged in the entire research process, may be a useful approach [27]. The use of process evaluations alongside the testing of new interventions based on the PPM-NI model may be useful to gain nurses’ perceptions and experiences. Process evaluations [28], also referred to as realist evaluations [29], help to better understand how, for whom and under what conditions our interventions work [28,29]. That is, involving end users in efforts to test and refine the PPM-NI may be warranted.
- Outcomes of PPM-NI consistent care: Research is needed to test whether PPM-NI based nursing interventions are more effective than care that is not reflective of this model, measured both at the health outcome level, and also at a resource use/cost-effectiveness measure. We hypothesise that PPM-NI care will ultimately lead to lower health resource use of both nursing time and intervention costs because more appropriate and timely care will be delivered. In this area, in addition to using explanatory randomised controlled trial (RCT) design to test efficacy, pragmatic trials to test effectiveness may be particularly valuable [30,31]. Pragmatic trials are particularly well suited for testing nursing interventions in several ways. First, they focus on effectiveness in usual circumstances or practice. Second, interventions are applied in a flexible way, as they would be in clinical practice. Finally, research findings are generally directly relevant to patients, clinicians and decision makers. Sackett suggests that pragmatic trials answer the question “Does this treatment improve patient-important outcomes when applied by typical clinicians to typical patients?” [30].
7. Conclusions
Author Contributions
Conflicts of Interest
References
- Moore, W.E. The Professions: Roles and Rules; Russell Sage Foundation: New York, NY, USA, 1970; p. 56. [Google Scholar]
- Flexner, A. Is social work a profession? In Proceedings of the National Conference of Charities and Corrections, Baltimore, MD, USA, 12–19 May 1915; pp. 578–581.
- Cogan, M.L. Toward a definition of profession. Harv. Educ. Rev. 1953, 23, 33–50. [Google Scholar]
- Walker, L.O.; Avant, K.C. Strategies for Theory Construction in Nursing, 2nd ed.; Appleton & Lange: Norwalk, CT, USA, 1988; p. 11. [Google Scholar]
- McCrae, N. Whither nursing models? The value of nursing theory in the context of evidence-based practice and multidisciplinary health care. J. Adv. Nurs. 2012, 68, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, S.K.; Crowley, D.M. The discipline of nursing. Nursing Outlook 1978, 26, 113–120. [Google Scholar] [PubMed]
- Fawcett, J.; Desanto-Madeya, S. Contemporary Nursing Knowledge: Analysis and Evaluation of Nursing Models and Theories; FA Davis Company: Philadelphia, PA, USA, 2013. [Google Scholar]
- Im, E.O. Development of situation-specific theories: An integrative approach. Adv. Nurs. Sci. 2005, 28, 137–151. [Google Scholar] [CrossRef]
- Im, E.O.; Meleis, A.I. A situation-specific theory of Korean immigrant women’s menopausal transition. Image J. Nurs. Scholarsh. 1999, 31, 333–338. [Google Scholar] [CrossRef]
- Im, E.O.; Chang, S.J. Current trends in nursing theories. J. Nurs. Scholarsh. 2012, 44, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Medical Research Council. Developing and Evaluating Complex Interventions; MRC: London, UK, 2008. [Google Scholar]
- Corry, M.; Clarke, M.; While, A.; Lalor, J. Developing complex interventions for nursing: Critical review of key guidelines. J. Clin. Nurs. 2013, 22, 2366–2386. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Mcintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new medical research council guideline. Int. J. Nurs. Stud. 2013, 50, 585–592. [Google Scholar] [CrossRef] [PubMed]
- McCormack, B.; McCance, T. Person-Centred Nursing; Theory and Practice; Wiley and Blackwell: London, UK, 2010. [Google Scholar]
- Ekman, I.; Wolf, A.; Olsson, L.E.; Taft, C.; Dudas, K.; Schaufelberger, M.; Swedberg, K. Effects of person-centred care in patients with chronic heart failure: The PCC-HF study. Eur. Heart J. 2012, 33, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Lusk, J.M.; Fater, K. A concept analysis of patient-centered care. Nurs. Forum 2013, 48, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, M.C. Wellbeing, contracts and capabilities. In Rethinking Wellbeing; Manderson, L., Ed.; API Network: Perth, Australia, 2005; pp. 27–45. [Google Scholar]
- Sen, A. Development as Freedon; Alfred A. Knopf: New York, NY, USA, 1999. [Google Scholar]
- Pringle, D.; Doran, D. Patient outcomes as an accountability. In Nursing-Sensitive Outcomes; Doran, D., Ed.; Jones & Bartlett: London, UK, 2003; pp. 1–26. [Google Scholar]
- Burston, S.; Chaboyer, W.; Gillespie, B. Nurse-sensitive indicators suitable to reflect nursing care quality: A review and discussion of issues. J. Clin. Nurs. 2014, 23, 1785–1795. [Google Scholar] [CrossRef] [PubMed]
- Clarke, A. What are the components of complex interventions in healthcare? Theorizing approaches to parts, powers and the whole intervention. Soc. Sci. Med. 2013, 93, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Moyle, W.; Cooke, M.; Beattie, E.; Jones, C.; Klein, B.; Cook, G.; Gray, C. Exploring the effect of companion robots on emotional expression in older adults with dementia: A pilot randomized controlled trial. J. Gerontol. Nurs. 2013, 39, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Shibata, T. Living with seal robots: Its sociopsychological and physiological influences on the elderly at a care house. IEEE Trans. Robot. 2007, 23, 972–980. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Yoder, L.H.; Kirkley, D.; McFall, D.C.; Kirksey, K.M.; StalBaum, A.L.; Sellers, D. Staff nurses’ use of research to facilitate evidence-based practice. Am. J. Nurs. 2014, 114, 26–37. [Google Scholar] [CrossRef] [PubMed]
- De Silva, D. Helping Measure Person-Centred Care; Foundation, H., Ed.; Health Foundation: London, UK, 2014. [Google Scholar]
- Canadian Institutes of Health Research. Available online: http://www.cihr-irsc.gc.ca/e/193.html (accessed on 23 July 2014).
- Grant, A.; Treweek, S.; Dreischulte, T.; Foy, R.; Guthrie, B. Process evaluations for cluster-randomised trials of complex interventions: A proposed framework for design and reporting. Trials 2013. [Google Scholar] [CrossRef]
- Bonell, C.; Fletcher, A.; Morton, M.; Lorenc, T.; Moore, L. Realist randomised controlled trials: A new approach to evaluating complex public health interventions. Soc. Sci. Med. 2012, 75, 2299–2306. [Google Scholar] [CrossRef]
- Sackett, D.L. Clinician-trialist rounds: 16. Mind your explanatory and pragmatic attitudes!—Part 1: What? Clin. Trials 2013, 10, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L. Clinician-trialist rounds: 17. Mind your explanatory and pragmatic attitudes! Part 2: How? Clin. Trials 2013, 10, 633–636. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moyle, W.; Rickard, C.M.; Chambers, S.K.; Chaboyer, W. The Partnering with Patients Model of Nursing Interventions: A First Step to a Practice Theory. Healthcare 2015, 3, 252-262. https://doi.org/10.3390/healthcare3020252
Moyle W, Rickard CM, Chambers SK, Chaboyer W. The Partnering with Patients Model of Nursing Interventions: A First Step to a Practice Theory. Healthcare. 2015; 3(2):252-262. https://doi.org/10.3390/healthcare3020252
Chicago/Turabian StyleMoyle, Wendy, Claire M. Rickard, Suzanne K. Chambers, and Wendy Chaboyer. 2015. "The Partnering with Patients Model of Nursing Interventions: A First Step to a Practice Theory" Healthcare 3, no. 2: 252-262. https://doi.org/10.3390/healthcare3020252