
Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience

Abstract
:1. Introduction
2. Methodology
2.1. Overview
2.1.1. Peer Support Network
2.1.2. Embrace
2.1.3. Busy Box
2.1.4. Best Face Forward
2.1.5. Genetics for Life
2.1.6. Health Care Symposia
2.2. Sampling and Constructs
2.3. Analyses

{kind=link}
| Mean | SD | n | % | |
|---|---|---|---|---|
| Demographics | ||||
| Age | 49.03 | 10.26 | ||
| Marital Status | ||||
| Married/Living as Married | 93 | 69.92 | ||
| Single | 23 | 17.29 | ||
| Divorced/Separated/Widowed | 14 | 10.53 | ||
| No Response | 3 | 2.26 | ||
| Religious Affiliation | ||||
| Jewish | 117 | 87.97 | ||
| Non-Jewish | 12 | 9.02 | ||
| No Response | 4 | 3.01 | ||
| Clinical Characteristics | ||||
| Age at Cancer Diagnosis (if applicable; years) | 44.77 | 9.47 | ||
| Cancer Status at Survey * | ||||
| Breast or Ovarian Cancer Survivor | 87 | 65.41 | ||
| At Risk or BRCA1/2 Mutation Carrier | 33 | 24.81 | ||
| Living with Breast and/or Ovarian Cancer | 19 | 14.29 | ||
| Recently Diagnosed with Breast Cancer | 15 | 11.28 | ||
| No Response or Other | 14 | 10.53 | ||
| Family Composition | ||||
| Number of Children | ||||
| 0 | 33 | 24.81 | ||
| 1 or more | 95 | 71.43 | ||
| No Response | 5 | 3.76 | ||
| Age(s) of Child(ren) * (if applicable; years) | ||||
| 0–17 | 64 | 48.12 | ||
| 18 or Older | 58 | 43.61 | ||
| Role at Sharsheret | ||||
| Peer Supporters | 23 | 17.29 | ||
| Resources/Year | Resources/Constituent | |||||||
|---|---|---|---|---|---|---|---|---|
| Year (n, %) | Peer Support Network | Embrace | Busy Box | Best Face Forward | Genetics for Life | Health Care Symposia | Other | Total |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | M (SD) | |
| 2010 (101, 29) | 64 (31) | 4 (2) | 23 (11) | 16 (8) | 18 (9) | 47 (22) | 37 (18) | 2.06 (1.28) |
| 2012 (113, 33) | 58 (26) | 9 (4) | 29 (13) | 23 (10) | 27 (12) | 47 (21) | 30 (13) | 1.97 (1.31) |
| 2013 (133, 38) | 58 (21) | 7 (3) | 28 (10) | 30 (11) | 25 (9) | 37 (13) | 96 (34) | 2.11 (1.43) |
| Total (347, 100) | 180 (25) | 20 (2.81) | 80 (11) | 69 (10) | 70 (10) | 131 (18) | 163 (23) | 2.05 (1.35) |
| Resource (# of Satisfaction Items) | Satisfaction Score M (SD) |
|---|---|
| Peer Support Network (3 items) | 95.2 (0.17) |
| Embrace (5 items) | 100.0 (0.00) |
| Busy Box (3 items) | 95.5 (0.19) |
| Best Face Forward (4 items) | 92.9 (0.26) |
| Genetics for Life (4 items) | 97.9 (0.71) |
| Health Care Symposia (2 items) | 98.0 (0.12) |
| Overall Satisfaction (per constituent) | 96.3 (0.13) |
3. Results and Discussion
3.1. Sample Characteristics
3.1.1. How Are Constituents Referred?
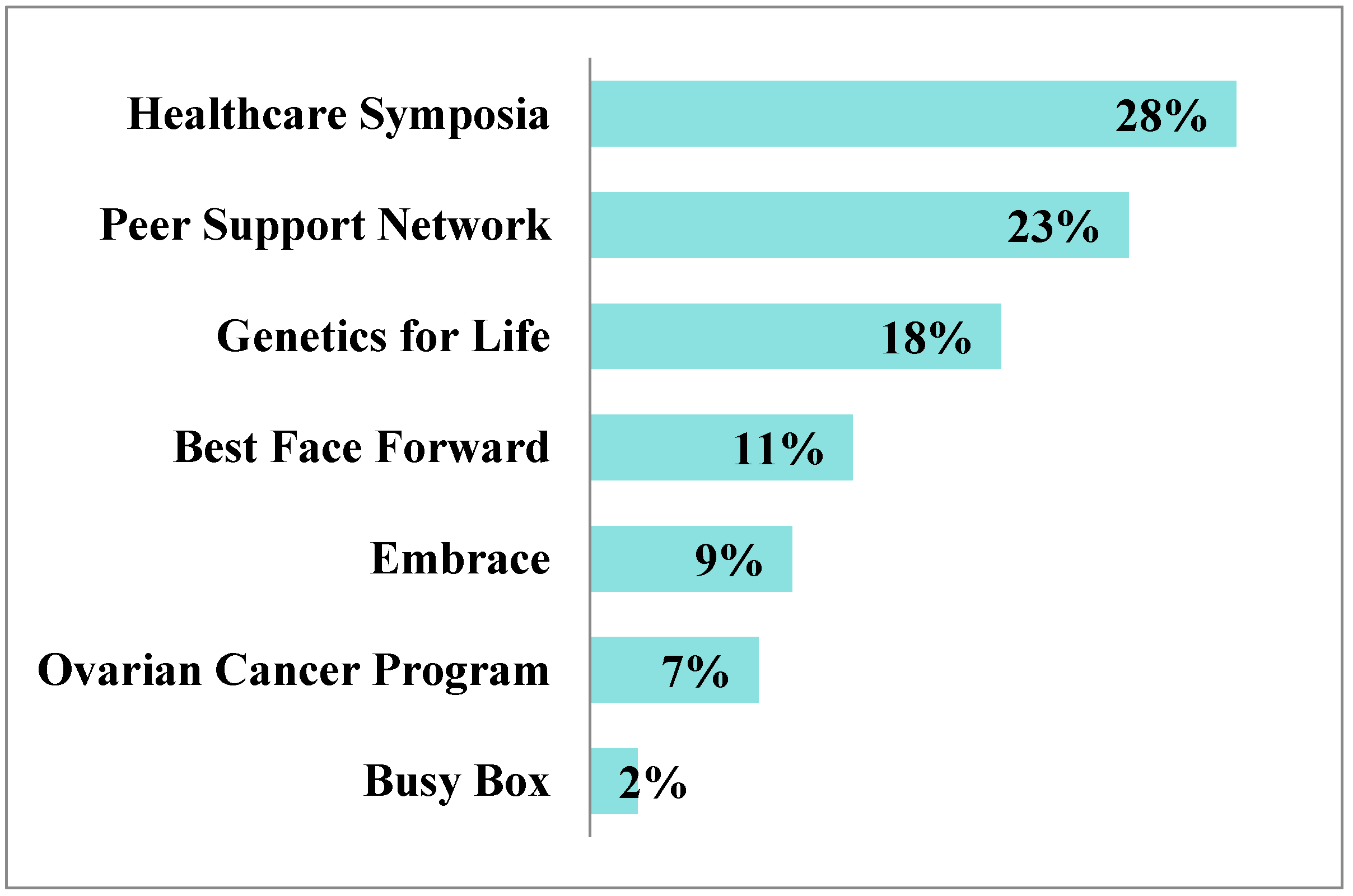
3.1.2. What Programs Do Constituents Engage With?
3.1.3. How Satisfied Are Constituents with the Resource(s) they Engaged With?
3.1.4. What Additional Needs Arise for Constituents?

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kohler, B.A.; Sherman, R.L.; Howlader, N.; Jemal, A.; Ryerson, A.B.; Henry, K.A.; Boscoe, F.P.; Cronin, K.A.; Lake, A.; Noone, A.M.; et al. Annual report to the nation on the status of cancer, 1975–2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]
- Lee, H.B.; Han, W. Unique features of young age breast cancer and its management. J. Breast Cancer 2014, 17, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Antoniou, A.C.; Easton, D.F.; Garcia-Closas, M. Genetic susceptibility to breast cancer. Mol. Oncol. 2010, 4, 174–191. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Parmigiani, G. Meta-analysis of BRCA1 and BRCA2 penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Amir, E.; Freedman, O.; Seruga, B.; Evans, D. Assessing women at high risk of breast cancer: A review of risk assessment models. J. Natl. Cancer Inst. 2010, 102, 680–691. [Google Scholar] [CrossRef] [PubMed]
- Stewart, B.W.; Wild, C.P. World Cancer Report 2014; International Agency for Research on Cancer: Geneva, Switzerland, 2014. [Google Scholar]
- Werner-Lin, A. Formal and informal support needs of young women with BRCA mutations. J. Psychosoc. Oncol. 2008, 26, 111–133. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Poll, A.; Llacuachaqui, M.; Nanda, S.; Tulman, A.; Mian, N.; Sun, P.; Narod, S.A. Patient satisfaction and cancer-related distress among unselected Jewish women undergoing genetic testing for BRCA1 and BRCA2. Clin. Genet. 2010, 78, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Hasson-Ohayon, I.; Braun, M.; Galinsky, D.; Baider, L. Religiosity and hope: A path for women coping with a diagnosis of breast cancer. Psychosomatics 2009, 50, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Coleman-Brueckheimer, K.; Spitzer, J.; Koffman, J. Involvement of Rabbinic and communal authorities in decision-making by haredi Jews in the UK with breast cancer: An interpretative phenomenological analysis. Soc. Sci. Med. 2009, 68, 323–333. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force Final Recommendation Statement. BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing. Available online: http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing (accessed on 24 February 2015).
- Manchanda, R.; Loggenberg, K.; Sanderson, S.; Burnell, M.; Wardle, J.; Gessler, S.; Side, L.; Balogun, N.; Desai, R.; Kumar, A.; et al. Population testing for cancer predisposing BRCA1/BRCA2 mutations in the Ashkenazi-Jewish community: A randomized controlled trial. J. Natl. Cancer Inst. 2014, 107. [Google Scholar] [CrossRef]
- Grann, V.R.; Whang, W.; Jacobson, J.S.; Heitjan, D.F.; Antman, K.H.; Neugut, A.I. Benefits and costs of screening Ashkenazi Jewish women for BRCA1 and BRCA2. J. Clin. Oncol. 1999, 17, 494–500. [Google Scholar] [PubMed]
- King, M.C.; Levy-Lahad, E.; Lahad, A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA 2014, 312, 1091–1092. [Google Scholar] [CrossRef] [PubMed]
- Khoury, M.J.; McCabe, L.L.; McCabe, E.R. Population screening in the age of genomic medicine. N. Engl. J. Med. 2003, 348, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, L.S.; Weeks, J.C.; Klar, N.; Garber, J.E. A population-based study of Ashkenazi Jewish women’s attitudes toward genetic discrimination and BRCA1/2 testing. Genet. Med. 2002, 4, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Brandt-Rauf, S.I.; Raveis, V.H.; Drummond, N.F.; Conte, J.A.; Rothman, S.M. Ashkenazi Jews and breast cancer: The consequences of linking ethnic identity to genetic disease. Am. J. Public Health 2006, 96, 1979–1988. [Google Scholar] [CrossRef] [PubMed]
- Navarro de Souza, A.; Groleau, D.; Loiselle, C.G.; Foulkes, W.D.; Wong, N. Cultural aspects of healthy BRCA carriers from two ethnocultural groups. Qual. Health Res. 2014, 24, 665–681. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.A.; Warner, E.; Meschino, W.S.; Hunter, J.; Abdolell, M.; Glendon, G.; Andrulis, I.L.; Goodwin, P.J. Perceptions of Ashkenazi Jewish breast cancer patients on genetic testing for mutations in BRCA1 and BRCA2. Clin. Genet. 2000, 57, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, W.S.; Jiang, H.; Dellefave, L.; Rademaker, A.W. Cost-effectiveness of population-based BRCA1/2 testing and ovarian cancer prevention for Ashkenazi Jews: A call for dialogue. Genet. Med. 2009, 11, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, R.; Legood, R.; Burnell, M.; McGuire, A.; Raikou, M.; Loggenberg, K.; Wardle, J.; Sanderson, S.; Gessler, S.; Side, L.; et al. Cost-effectiveness of population screening for BRCA mutations in Ashkenazi Jewish women compared with family history-based testing. J. Natl. Cancer Inst. 2014, 107. [Google Scholar] [CrossRef]
- DeMarco, T.A.; Peshkin, B.N.; Valdimarsdottir, H.B.; Patenaude, A.F.; Schneider, K.A.; Tercyak, K.P. Role of parenting relationship quality in communicating about maternal BRCA1/2 genetic test results with children. J. Genet. Couns. 2008, 17, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Tercyak, K.P.; Peshkin, B.N.; Demarco, T.A.; Patenaude, A.F.; Schneider, K.A.; Garber, J.E.; Valdimarsdottir, H.B.; Schwartz, M.D. Information needs of mothers regarding communicating BRCA1/2 cancer genetic test results to their children. Genet. Test. 2007, 11, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Peshkin, B.N.; Demarco, T.A.; Tercyak, K.P. On the development of a decision support intervention for mothers undergoing BRCA1/2 cancer genetic testing regarding communicating test results to their children. Fam. Cancer. 2010, 9, 89–97. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion, Division of Population Health. Health-Related Quality of Life Concepts. Available online: http://www.cdc.gov/hrqol/concept.htm (accessed on 24 February 2015).
- Centers for Disease Control and Prevention. Measuring Healthy Days. Available online: http://www.cdc.gov/hrqol/pdfs/mhd.pdf (accessed on 24 February 2015).
- Gandek, B.; Sinclair, S.J.; Kosinski, M.; Ware, J.E., Jr. Psychometric evaluation of the SF-36 health survey in Medicare managed care. Health Care Financ. Rev. 2004, 25, 5–25. [Google Scholar] [PubMed]
- McHorney, C.A. Health status assessment methods for adults: Past accomplishments and future challenges. Annu. Rev. Public Health 1999, 20, 309–335. [Google Scholar] [CrossRef] [PubMed]
- Selim, A.J.; Rogers, W.; Fleishman, J.A.; Qian, S.X.; Fincke, B.G.; Rothendler, J.A.; Kazis, L.E. Updated U.S. population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual. Life Res. 2009, 18, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Heaney, C.A.; Israel, B.A. Social networks and social support. In Health Behavior and Health Education: Theory, Research, and Practice; Jossey-Bass: New York, NY, USA, 2008; Volume 4, pp. 189–210. [Google Scholar]
- Iwelunmor, J.; Newsome, V.; Airhihenbuwa, C.O. Framing the impact of culture on health: A systematic review of the PEN-3 cultural model and its application in public health research and interventions. Ethn. Health 2014, 19, 20–46. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, V.B.; Williams, K.P.; Harrison, T.M.; Jennings, Y.; Lucas, W.; Stephen, J.; Robinson, D.; Mandelblatt, J.S.; Taylor, K.L. Development of decision-support intervention for Black women with breast cancer. Psychooncology 2010, 19, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Haynes, V.; Escoffery, C.; Wilkerson, C.; Bell, R.; Flowers, L. Adaptation of a cervical cancer education program for African Americans in the faith-based community, Atlanta, Georgia, 2012. Prev. Chronic Dis. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Framework for program evaluation in public health. MMWR Recomm. Rep. 1999, 48, 1–40. [Google Scholar]
- Meiser, B.; Eisenbruch, M.; Barlow-Stewart, K.; Tucker, K.; Steel, Z.; Goldstein, D. Cultural aspects of cancer genetics: Setting a research agenda. J. Med. Genet. 2001, 38, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Neta, G.; Sanchez, M.A.; Chambers, D.A.; Phillips, S.M.; Leyva, B.; Cynkin, L.; Farrell, M.M.; Heurtin-Roberts, S.; Vinson, C. Implementation science in cancer prevention and control: A decade of grant funding by the National Cancer Institute and future directions. Implement. Sci. 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; You, J.; Man, J.; Loh, A.; Young, L. Evaluating a culturally tailored peer-mentoring and education pilot intervention among Chinese breast cancer survivors using a mixed-methods approach. Oncol. Nurs. Forum. 2014, 41, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, V.B.; Wallington, S.F.; Willey, S.C.; Hampton, R.M.; Lucas, W.; Jennings, Y.; Horton, S.; Muzeck, N.; Cocilovo, C.; Isaacs, C. A peer-led decision support intervention improves decision outcomes in black women with breast cancer. J. Cancer Educ. 2013, 28, 262–269. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tercyak, K.P.; Silber, E.; Johnson, A.C.; Fleischmann, A.; Murphy, S.E.; Mays, D.; O’Neill, S.C.; Sharkey, C.M.; Shoretz, R. Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience. Healthcare 2015, 3, 324-337. https://doi.org/10.3390/healthcare3020324
Tercyak KP, Silber E, Johnson AC, Fleischmann A, Murphy SE, Mays D, O’Neill SC, Sharkey CM, Shoretz R. Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience. Healthcare. 2015; 3(2):324-337. https://doi.org/10.3390/healthcare3020324
Chicago/Turabian StyleTercyak, Kenneth P., Elana Silber, Andrea C. Johnson, Adina Fleischmann, Sarah E. Murphy, Darren Mays, Suzanne C. O’Neill, Christina M. Sharkey, and Rochelle Shoretz. 2015. "Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience" Healthcare 3, no. 2: 324-337. https://doi.org/10.3390/healthcare3020324
APA StyleTercyak, K. P., Silber, E., Johnson, A. C., Fleischmann, A., Murphy, S. E., Mays, D., O’Neill, S. C., Sharkey, C. M., & Shoretz, R. (2015). Survey on Addressing the Information and Support Needs of Jewish Women at Increased Risk for or Diagnosed with Breast Cancer: The Sharsheret Experience. Healthcare, 3(2), 324-337. https://doi.org/10.3390/healthcare3020324