Chronic Respiratory Disorders and Their Treatment among Older People with Intellectual Disability and/or Autism Spectrum Disorder in Comparison with the General Population



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Health Care Utilization
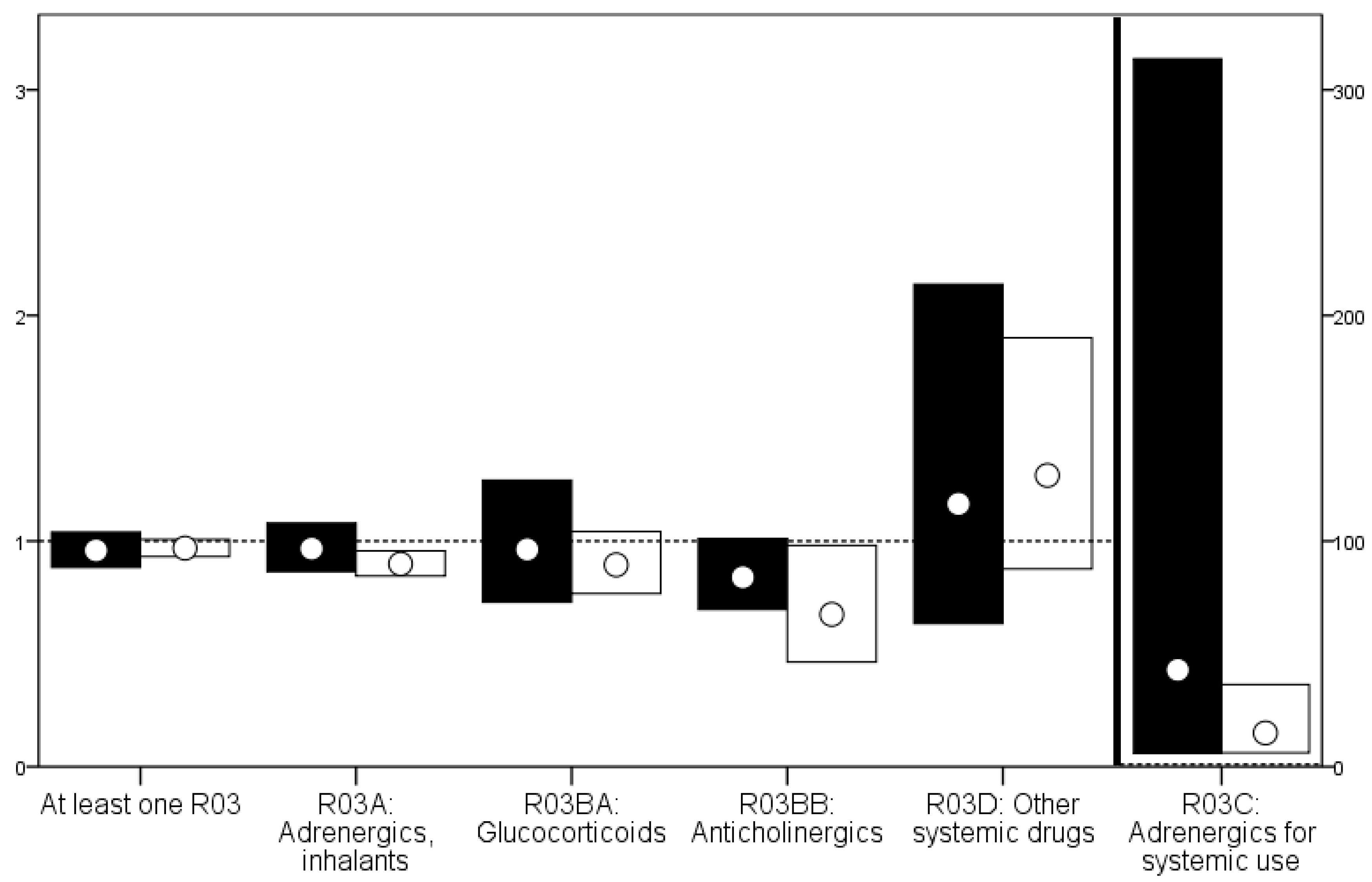
3.2. Drug Prescriptions
3.3. Diagnoses
3.4. Diagnoses vs. Drug Prescriptions
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sandberg, M.; Ahlström, G.; Kristensson, J. Patterns of somatic diagnoses in older people with intellectual disability: A Swedish eleven year case-control study of inpatient data. J. Appl. Res. Intellect. Disabil. 2015, 30, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Venkat, A.; Pastin, R.B.; Hegde, G.G.; Shea, J.M.; Cook, J.T.; Culig, C. An analysis of ED utilization by adults with intellectual disability. Am. J. Emerg. Med. 2011, 29, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.K.; Chen, C.Y.; Broadbent, M.; Stewart, R.; O'Hara, J. Hospital admissions for respiratory system diseases in adults with intellectual disabilities in southeast London: A register-based cohort study. BMJ Open 2017, 7, e014846. [Google Scholar] [CrossRef] [PubMed]
- Skorpen, S.; Nicolaisen, M.; Langballe, E.M. Hospitalisation in adults with intellectual disabilities compared with the general population in Norway. J. Intellect. Disabil. Res. 2016, 60, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Raitasuo, J.; Molsa, P.; Raitasuo, S.; Mattila, K. Deaths among the intellectually disabled: A retrospective study. J. Appl. Res. Intellect. Disabil. 1997, 10, 280–288. [Google Scholar] [CrossRef]
- Tyler, C.V.; Schramm, S.; Karafa, M.; Tang, A.S.; Jain, A. Electronic health record analysis of the primary care of adults with intellectual and other developmental disabilities. J. Policy Pract. Intellect. Disabil. 2010, 7, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Glover, G.; Williams, R.; Heslop, P.; Oyinlola, J.; Grey, J. Mortality in people with intellectual disabilities in England. J. Intellect. Disabil. Res. 2017, 61, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Glasson, E.J.; Sullivan, S.G.; Hussain, R.; Bittles, A.H. An assessment of intellectual disability among aboriginal Australians. J. Intellect. Disabil. Res. 2005, 49, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Durvasula, S.; Beange, H.; Baker, W. Mortality of people with intellectual disability in northern Sydney. J. Intellect. Dev. Disabil. 2002, 27, 255–264. [Google Scholar] [CrossRef]
- Walsh, P.N. Ageing and mental retardation. Curr. Opin. Psychiatry 2002, 15, 509–514. [Google Scholar] [CrossRef]
- Patja, K.; Molsa, P.; Iivanainen, M. Cause-specific mortality of people with intellectual disability in a population-based, 35-year follow-up study. J. Intellect. Disabil. Res. 2001, 45, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Trollor, J.; Srasuebkul, P.; Xu, H.; Howlett, S. Cause of death and potentially avoidable deaths in Australian adults with intellectual disability using retrospective linked data. BMJ Open 2017, 7, e013489. [Google Scholar] [CrossRef] [PubMed]
- Mitra, M.; Clements, K.M.; Zhang, J.Y.; Smith, L.D. Disparities in adverse preconception risk factors between women with and without disabilities. Matern. Child Health J. 2016, 20, 507–515. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.; O’Hara, J. Ill-health and intellectual disabilities. Curr. Opin. Psychiatry 2011, 24, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Gale, L.; Naqvi, H.; Russ, L. Asthma, smoking and bmi in adults with intellectual disabilities: A community-based survey. J. Intellect. Disabil. Res. 2009, 53, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Shah, S.M.; Hosking, F.J.; DeWilde, S.; Harris, T.; Beighton, C.; Cook, D.G. Health characteristics and consultation patterns of people with intellectual disability: A cross-sectional database study in English general practice. Br. J. Gen. Pract. 2016, 66, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.A.; McLean, G.; Guthrie, B.; McConnachie, A.; Mercer, S.; Sullivan, F.; Morrison, J. Multiple physical and mental health comorbidity in adults with intellectual disabilities: Population-based cross-sectional analysis. BMC Fam. Pract. 2015, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- NHS Digital. Health and Care of People with Learning Disabilities: 2014 to 2015. Available online: https://www.gov.uk/government/statistics/health-and-care-of-people-with-learning-disabilities-2014-to-2015 (accessed on 9 December 2016).
- Sturdy, P.M.; Victor, C.R.; Anderson, H.R.; Bland, J.M.; Butland, B.K.; Harrison, B.D.; Peckitt, C.; Taylor, J.C. Psychological, social and health behaviour risk factors for deaths certified as asthma: A national case-control study. Thorax 2002, 57, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Balogh, R.; Brownell, M.; Ouellette-Kuntz, H.; Colantonio, A. Hospitalisation rates for ambulatory care sensitive conditions for persons with and without an intellectual disability-A population perspective. J. Intellect. Disabil. Res. 2010, 54, 820–832. [Google Scholar] [CrossRef] [PubMed]
- Sitilci, T.; Demirgan, S.; Akcay, C.; Kahraman, N.; Koseoglu, B.G.; Erdem, M.A.; Cankaya, A.B. Comparison of patients with and without intellectual disability under general anesthesia: A retrospective study. Niger. J. Clin. Pract. 2017, 20, 438–444. [Google Scholar] [PubMed]
- Kauppi, P.; Linna, M.; Jantunen, J.; Martikainen, J.E.; Haahtela, T.; Pelkonen, A.; Makela, M. Chronic comorbidities contribute to the burden and costs of persistent asthma. Mediators Inflamm. 2015, 2015, 819194. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Carleton, B.C.; Prosser, R.J.; Smith, A.M. The added burden of comorbidity in patients with asthma. J. Asthma 2009, 46, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Mahboub, B.; Alzaabi, A.; Iqbal, M.N.; Salhi, H.; Lahlou, A.; Tariq, L.; El Hasnaoui, A. Comorbidities associated with COPD in the middle east and north Africa region: Association with severity and exacerbations. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 273–280. [Google Scholar] [PubMed]
- Lopez Varela, M.V.; Montes de Oca, M.; Halbert, R.; Muino, A.; Talamo, C.; Perez-Padilla, R.; Jardim, J.R.; Valdivia, G.; Pertuze, J.; Menezes, A.M. Comorbidities and health status in individuals with and without COPD in five Latin American cities: The platino study. Arch. Bronconeumol. 2013, 49, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Lynd, L.D.; FitzGerald, J.M.; Marra, C.A.; Rousseau, R.; Sadatsafavi, M. The added effect of comorbidity on health-related quality of life in patients with asthma. Qual. Life Res. 2015, 24, 2507–2517. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.Y.; Kim, E. Factors contributing to quality of life in COPD patients in South Korea. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, M.; Pitsiou, G.; Manika, K.; Kontou, P.; Zarogoulidis, P.; Sichletidis, L.; Kioumis, I.P. Copd assessment test: A simple tool to evaluate disease severity and response to treatment. COPD 2014, 11, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Axmon, A.; Björne, P.; Nylander, L.; Ahlström, G. Psychiatric diagnoses in older people with intellectual disability in comparison with the general population: A register study. Epidemiol. Psychiatr. Sci. 2017, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sheppard-Jones, K.; Thompson Prout, H.; Kleinert, H. Quality of life dimensions for adults with developmental disabilities: A comparative study. Ment. Retard. 2005, 43, 281–291. [Google Scholar] [CrossRef]
- Davis, S.R.; Durvasula, S.; Merhi, D.; Young, P.M.; Traini, D.; Bosnic-Anticevich, S.Z. Respiratory medication use in an Australian developmental disability clinic population: Messages for health care professionals. Aust. J. Prim. Health 2014, 20, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Davis, S. Asthma in intellectual disability: Are we managing our patients appropriately? Breathe 2016, 12, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.K. Allergy and asthma in the elderly. Semin. Respir. Crit. Care Med. 2010, 31, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Raherison, C.; Girodet, P.O. Epidemiology of COPD. Eur. Respir. Rev. 2009, 18, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Janicki, M.P.; Davidson, P.W.; Henderson, C.M.; McCallion, P.; Taets, J.D.; Force, L.T.; Sulkes, S.B.; Frangenberg, E.; Ladrigan, P.M. Health characteristics and health services utilization in older adults with intellectual disability living in community residences. J. Intellect. Disabil. Res. 2002, 46, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Axmon, A.; Björne, P.; Nylander, L.; Ahlström, G. Psychiatric care utilization among older people with intellectual disability in comparison with the general population: A register study. BMC Psychiatry 2016, 16, 389. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, M.; Ahlström, G.; Axmon, A.; Kristensson, J. Somatic healthcare utilisation patterns among older people with intellectual disability: An 11-year register study. BMC Health Serv. Res. 2016, 16, 642. [Google Scholar] [CrossRef] [PubMed]
- Akinbami, L.J.; Fryar, C.D. Current asthma prevalence by weight status among adults: United States, 2001–2014. NCHS Data Brief. 2016, 239, 1–8. [Google Scholar]
- Ryan-Ibarra, S.; Milet, M.; Lutzker, L.; Rodriguez, D.; Induni, M.; Kreutzer, R. Age, period, and cohort effects in adult lifetime asthma prevalence in California: An application of hierarchical age-period-cohort analysis. Ann. Epidemiol. 2016, 26, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Garcia, M.; Caballero, A.; Jaramillo, C.; Maldonado, D.; Torres-Duque, C.A. Prevalence, risk factors and underdiagnosis of asthma and wheezing in adults 40 years and older: A population-based study. J. Asthma 2015, 52, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Morin, D.; Mérineau-Côté, J.; Ouellette-Kuntz, H.; Tassé, M.; Kerr, M. A comparison of the prevalence of chronic disease among people with and without intellectual disability. Am. J. Intellect. Dev. Disabil. 2012, 117, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Cocks, E.; Thomson, A.; Thoresen, S.; Parsons, R.; Rosenwax, L. Health status and use of medications by adults with intellectual disability in western Australia. J. Intellect. Dev. Disabil. 2016, 41, 87–96. [Google Scholar] [CrossRef]
- McDermott, S.; Moran, R.; Platt, T.; Dasari, S. Variation in health conditions among groups of adults with disabilities in primary care. J. Community Health 2006, 31, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Buist, A.S. Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 2007, 370, 765–773. [Google Scholar] [CrossRef]
- McCarron, M.; Cleary, E.; McCallion, P. Health and health-care utilization of the older population of Ireland: Comparing the intellectual disability population and the general population. Res. Aging 2017, 39, 693–718. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.I.; Ansari, Z.; Vaughan, L.; Matters, H.; Emerson, E. Health and wellbeing of Victorian adults with intellectual disability compared to the general Victorian population. Res. Dev. Disabil. 2013, 34, 4034–4042. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Daly, P.; Smyth, F. Lifestyle and health behaviours of adults with an intellectual disability. J. Intellect. Disabil. Res. 2007, 51, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Purdy, S.; Griffin, T.; Salisbury, C.; Sharp, D. Ambulatory care sensitive conditions: Terminology and disease coding need to be more specific to aid policy makers and clinicians. Public Health 2009, 123, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.; Herring, J.; Lacroix, J.; Levinton, C. Avoidable admissions and repeat admissions: What do they tell us? Healthc. Q. 2007, 10, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Dunn, K.; Hughes-McCormack, L.; Cooper, S.A. Hospital admissions for physical health conditions for people with intellectual disabilities: Systematic review. J. Appl. Res. Intellect. Disabil. 2017. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Primary Diagnosis at Visit | gPop | ID | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Women | Men | Women vs. Men | All | Women | Men | Women vs. Men | ||||
| n (%) | n (%) | n (%) | RR b (95% CI) | n (%) | RR a (95% CI) | n (%) | RR a (95% CI) | n (%) | RR a (95% CI) | RR b (95% CI) | |
| Any | 252 (3) | 119 (3) | 133 (3) | 0.93 (0.73–1.19) | 152 (2) | 0.60 (0.49–0.74) | 77 (2) | 0.65 (0.49–0.96) | 75 (2) | 0.56 (0.43–0.75) | 0.81 (0.59–1.11) |
| Bronchitis, not specified as acute or chronic | 15 (0) | 7 (0) | 8 (0) | 0.95 (0.35–2.63) | 14 (0) | 0.93 (0.45–1.93) | 6 (0) | 0.86 (0.29–2.55) | 8 (0) | 1.00 (0.38–2.66) | 1.11 (0.39–3.20) |
| Simple and mucopurulent chronic bronchitis | 13 (0) | 5 (0) | 8 (0) | 1.34 (0.44–4.08) | <5 | <5 | <5 | ||||
| Unspecified chronic bronchitis | 10 (0) | 8 (0) | <5 | 6 (0) | 0.60 (0.22–1.65) | 5 (0) | 0.63 (0.21–1.91) | <5 | |||
| Emphysema | 10 (0) | <5 | 6 (0) | <5 | <5 | <5 | |||||
| Other chronic obstructive pulmonary disease (COPD) | 137 (2) | 60 (2) | 77 (2) | 1.07 (0.77–1.50) | 64 (1) | 0.47 (0.35–0.63) | 26 (1) | 0.43 (0.27–0.69) | 38 (1) | 0.49 (0.34–0.73) | 1.22 (0.74–2.00) |
| Asthma | 105 (1) | 51 (1) | 54 (1) | 0.88 (0.60–1.29) | 85 (1) | 0.81 (0.61–1.08) | 49 (1) | 0.96 (0.65–1.42) | 36 (1) | 0.67 (0.44–1.01) | 0.61 (0.40–0.94) |
| Status asthmaticus | 10 (0) | <5 | 6 (0) | 6 (0) | 0.60 (0.22–1.65) | <5 | <5 | ||||
| Bronchiectasis | 9 (0) | 6 (0) | <5 | <5 | <5 | <5 | |||||
| Drug | gPop | ID | ||||
|---|---|---|---|---|---|---|
| Total | Women | Men | Total | Women | Men | |
| R03AC02: salbutamol | 299 | 180 | 119 | 255 | 143 | 112 |
| R03AC03: terbutaline | 758 | 421 | 337 | 379 | 218 | 161 |
| R03AC12: salmeterol | 43 | 21 | 22 | 13 | 9 | 4 |
| R03AC13: formoterol | 186 | 102 | 84 | 74 | 40 | 34 |
| R03AC18: indacaterol | 13 | 6 | 7 | 1 | 0 | 1 |
| R03AK06: salmeterol and fluticasone | 141 | 79 | 62 | 86 | 52 | 34 |
| R03AK07: formoterol and budesonide | 472 | 235 | 237 | 203 | 108 | 95 |
| R03AK08: formoterol and beclometasone | 5 | 3 | 2 | 15 | 9 | 6 |
| R03AL02: salbutamol and ipratropium bromide | 32 | 14 | 18 | 77 | 35 | 42 |
| R03BA01: beclometasone | 23 | 12 | 11 | 21 | 6 | 15 |
| R03BA02: budesonide | 633 | 353 | 280 | 314 | 179 | 135 |
| R03BA05: fluticasone | 43 | 23 | 20 | 69 | 39 | 30 |
| R03BA07: mometasone | 26 | 14 | 12 | 6 | 4 | 2 |
| R03BA08: ciclesonide | 1 | 0 | 1 | 0 | 0 | 0 |
| R03BB01: ipratropium bromide | 103 | 56 | 47 | 73 | 30 | 43 |
| R03BB04: tiotropium bromide | 260 | 137 | 123 | 109 | 52 | 57 |
| R03BC01: cromoglicic acid | 11 | 8 | 3 | 0 | 0 | 0 |
| R03CA02: ephedrine | 2 | 1 | 1 | 0 | 0 | 0 |
| R03CC02: salbutamol | 9 | 6 | 3 | 76 | 44 | 32 |
| R03CC03: terbutaline | 14 | 7 | 7 | 176 | 93 | 83 |
| R03CC12: bambuterol | 2 | 1 | 1 | 49 | 28 | 21 |
| R03DA02: choline theophyllinate | 2 | 0 | 2 | 52 | 26 | 26 |
| R03DA04: theophylline | 5 | 3 | 2 | 28 | 12 | 16 |
| R03DC03: montelukast | 86 | 44 | 42 | 61 | 32 | 29 |
| R03DX07: roflumilast | 5 | 0 | 5 | 2 | 1 | 1 |
| Diagnosis | gPop | ID | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Women | Men | Women vs. Men | All | Women | Men | Women vs. Men | ||||
| n (%) | n (%) | n (%) | RR b (95% CI) | n (%) | RR a (95% CI) | n (%) | RR a (95% CI) | n (%) | RR a (95% CI) | RR b (95% CI) | |
| Any | 434 (5) | 205 (6) | 229 (5) | 0.93 (0.78–1.12) | 302 (4) | 0.70 (0.60–0.80) | 158 (4) | 0.77 (0.63–0.94) | 144 (3) | 0.63 (0.51–0.77) | 0.76 (0.61–0.95) |
| Bronchitis, not specified as acute or chronic | 19 (0) | 7 (0) | 12 (0) | 1.43 (0.56–3.63) | 21 (0) | 1.11 (0.60–2.05) | 8 (0) | 1.14 (0.42–3.15) | 13 (0) | 1.08 (0.50–2.37) | 1.34 (0.56–3.33) |
| Simple and mucopurulent chronic bronchitis | 21 (0) | 7 (0) | 14 (0) | 1.69 (0.67–4.13) | <5 | <5 | <5 | ||||
| Unspecified chronic bronchitis | 21 (0) | 13 (0) | 8 (0) | 0.51 (0.21–1.24) | 11 (0) | 0.54 (0.25–1.09) | 8 (0) | 0.62 (0.26–1.48) | <5 | ||
| Emphysema | 19 (0) | 7 (0) | 12 (0) | 1.43 (0.56–3.63) | 5 (0) | 0.26 (0.10–0.70) | <5 | <5 | |||
| Other chronic obstructive pulmonary disease (COPD) | 233 (3) | 104 (3) | 129 (3) | 1.04 (0.80–1.33) | 125 (2) | 0.54 (0.43–0.67) | 53 (1) | 0.51 (0.37–0.71) | 72 (2) | 0.56 (0.42–0.74) | 1.13 (0.80–1.61) |
| Asthma | 219 (3) | 114 (3) | 105 (2) | 0.77 (0.59-1.00) | 187 (2) | 0.85 (0.70–1.04) | 105 (3) | 0.92 (0.71–1.20) | 82 (2) | 0.78 (0.59–1.04) | 0.65 (0.49–0.87) |
| Status asthmaticus | 12 (0) | <5 | 8 (0) | 6 (0) | 0.50 (0.19–1.33) | <5 | <5 | ||||
| Bronchiectasis | 12 (0) | 8 (0) | <5 | <5 | <5 | <5 | |||||
| Drugs | gPop | ID | ||||||
|---|---|---|---|---|---|---|---|---|
| No Diagnosis (n = 7538) | Asthma Only (n = 179, 45% a) | COPD Only (n = 165, 41% a) | Asthma and COPD (n = 54, 14% a) | No Diagnosis (n = 7660) | Asthma Only (n = 89, 32% a) | COPD Only (n = 151, 55% a) | Asthma and COPD (n = 36, 13% a) | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| At least one R03 | 1122 (15) | 156 (87) | 160 (97) | 54 (100) | 698 (9) | 73 (82) | 142 (94) | 35 (97) |
| R03A: Adrenergics, inhalants | 932 (12) | 135 (75) | 157 (95) | 54 (100) | 490 (6) | 65 (73) | 129 (85) | 33 (92) |
| R03BA: Glucocorticoids | 495 (7) | 57 (32) | 110 (67) | 34 (63) | 208 (3) | 25 (28) | 88 (58) | 22 (61) |
| R03BB: Anticholinergics | 141 (2) | 112 (63) | 20 (12) | 39 (72) | 73 (1) | 52 (58) | 18 (12) | 16 (44) |
| R03C: Adrenergics for systemic use | 21 (0) | 1 (1) | 5 (3) | 0 (0) | 194 (3) | 11 (12) | 52 (34) | 12 (33) |
| R03D: Other systemic drugs | 45 (1) | 11 (6) | 26 (16) | 13 (24) | 69 (1) | 10 (11) | 38 (25) | 5 (14) |
| Drug | Men | Women | |
|---|---|---|---|
| COPD | At least one R03 | 0.97 (0.85–1.11) | 0.95 (0.88–1.04) |
| R03A: Adrenergics, inhalants | 1.03 (0.87–1.21) | 0.91 (0.78–1.05) | |
| R03BA: Glucocorticoids | 1.09 (0.75–1.58) | 0.83 (0.54–1.26) | |
| R03BB: Anticholinergics | 0.81 (0.62–1.05) | 0.88 (0.69–1.14) | |
| R03C: Adrenergics for systemic use a | 21.58 (2.86–163) | ||
| R03D: Other systemic drugs | 0.80 (0.36–1.74) | 2.29 (0.81–6.47) | |
| Asthma | At least one R03 | 0.99 (0.93–1.05) | 0.95 (0.90–1.00) |
| R03A: Adrenergics, inhalants | 0.92 (0.83–1.01) | 0.88 (0.82–0.95) | |
| R03BA: Glucocorticoids | 0.88 (0.71–1.10) | 0.91 (0.73–1.12) | |
| R03BB: Anticholinergics | 1.06 (0.62–1.81) | 0.45 (0.26–0.78) | |
| R03C: Adrenergics for systemic use | 9.28 (3.40–25.4) | 38.0 (5.30–272) | |
| R03D: Other systemic drugs | 1.21 (0.68–2.16) | 1.36 (0.80–2.29) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axmon, A.; Höglund, P.; Ahlström, G. Chronic Respiratory Disorders and Their Treatment among Older People with Intellectual Disability and/or Autism Spectrum Disorder in Comparison with the General Population. Healthcare 2017, 5, 40. https://doi.org/10.3390/healthcare5030040
Axmon A, Höglund P, Ahlström G. Chronic Respiratory Disorders and Their Treatment among Older People with Intellectual Disability and/or Autism Spectrum Disorder in Comparison with the General Population. Healthcare. 2017; 5(3):40. https://doi.org/10.3390/healthcare5030040
Chicago/Turabian StyleAxmon, Anna, Peter Höglund, and Gerd Ahlström. 2017. "Chronic Respiratory Disorders and Their Treatment among Older People with Intellectual Disability and/or Autism Spectrum Disorder in Comparison with the General Population" Healthcare 5, no. 3: 40. https://doi.org/10.3390/healthcare5030040
APA StyleAxmon, A., Höglund, P., & Ahlström, G. (2017). Chronic Respiratory Disorders and Their Treatment among Older People with Intellectual Disability and/or Autism Spectrum Disorder in Comparison with the General Population. Healthcare, 5(3), 40. https://doi.org/10.3390/healthcare5030040