Exploring Primary Healthcare Students and Their Mentors’ Awareness of Mentorship and Clinical Governance as Part of a Local Continuing Professional Development (CPD) Program: Findings of a Quantitative Survey


Abstract
:1. Introduction
“Promotion of a safe environment, research, participation in shaping health policy and in patient and health systems management, and education”.
1.1. Literature Review
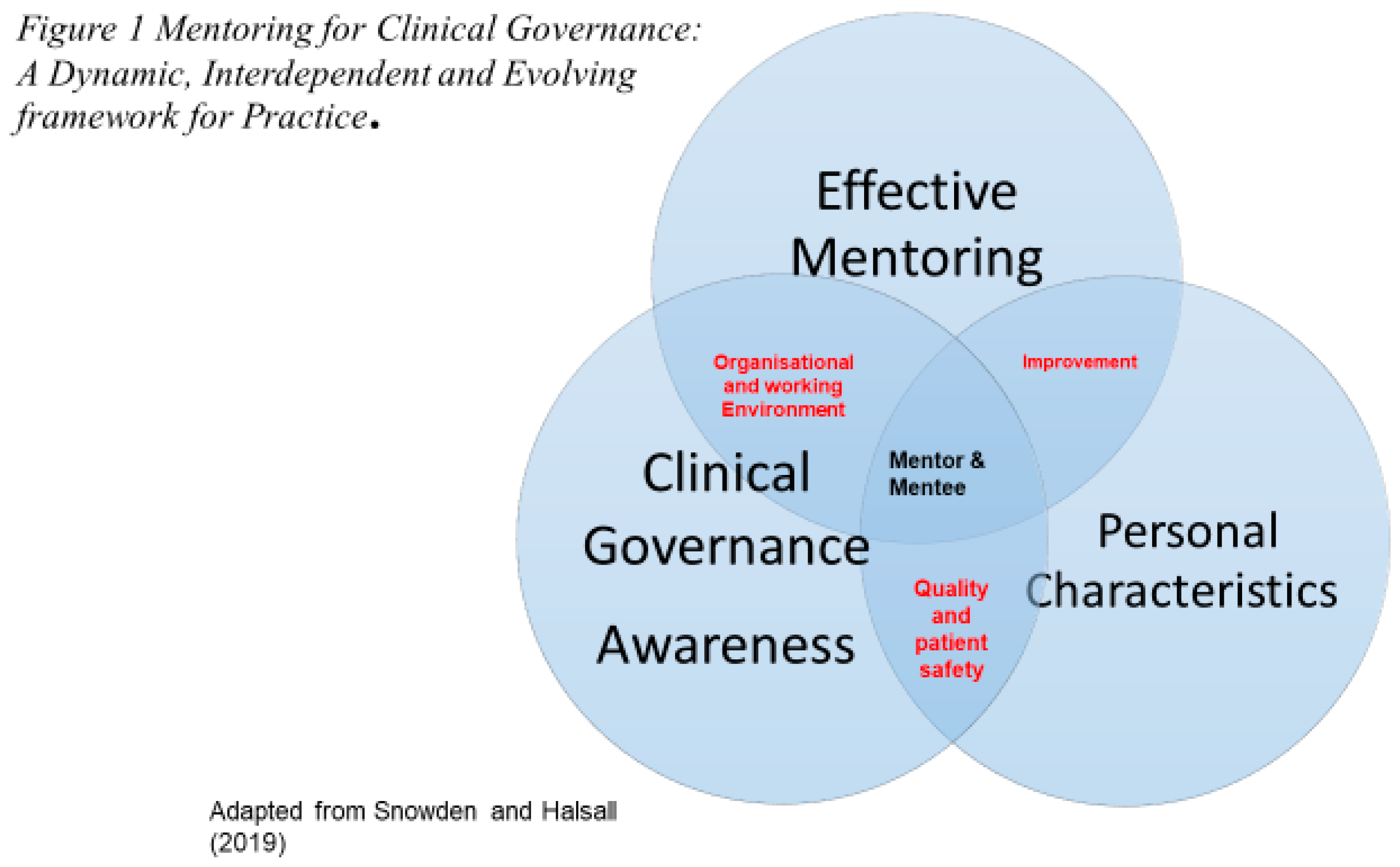
1.1.1. Evolution of Clinical Governance and the Relationship with Mentoring
“A framework through which NHS organizations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish”[20].
1.1.2. Characteristics of Mentoring in Supporting the Application of Clinical Governance
“Highly experienced custodians and advocates of safe, quality and compassionate care providing effective role modelling, guidance, supervision and support to less experienced and aspiring practitioners”[2] (p. 386).
1.2. Aims
- (1)
- To identify the key characteristics of the mentor from the perspective of the mentee and mentor;
- (2)
- To investigate primary healthcare workers awareness of mentorship and clinical governance;
- (3)
- To critically explore the factors that influence mentorship relationship and the application of clinical governance within primary healthcare practice;
- (4)
- To identify the role mentorship plays in facilitating clinical governance in primary healthcare practice;
- (5)
- To establish the role of mentoring and clinical governance in the delivery of CPD of primary healthcare workers.
2. Methodology
2.1. Data Collection
2.2. Instrument
2.3. Sample
3. Results
3.1. Findings from the Mentorship and Clinical Governance Awareness Questionnaire
3.2. Justification for Factors Analysis
3.3. Mentorship and Clinical Governance
4. Discussion
5. Conclusions
6. Recommendations
- Using the newly devised and validated questionnaire to be applied globally across the health and care settings for a larger scale research;
- To further review the key characteristics of mentoring and individual characteristics of the mentor in facilitating clinical governance and patient safety within the clinical learning environment for the mentees through qualitative methodologies;
- To encourage Higher Education Institutions (HEIs) and Nursing Colleges to review existing mentor programs to incorporate ways of highlighting the importance of the mentor in facilitating patient safety and clinical governance within clinical health and care programs.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clinical Human Factors Group (CHHFG). Patient Safety First’s “How to” Guide for implementing Human Factors in Healthcare. Available online: https://chfg.org/how-to-guide-to-human-factors-volume-1/ (accessed on 16 September 2019).
- Ellwood, F.; Snowden, M.; McSherry, R.; Halsall, J.; Hough, D. Mentoring and You. Dent. Nurs. 2016, 12, 386–391. [Google Scholar]
- Paley, J. Social Psychology and the Compassion Deficit. Nurs. Educ. Today 2013, 33, 1451–1452. [Google Scholar] [CrossRef]
- Rolfe, G.; Gardner, L. Invisible Gorillas and Red Herrings: A Response to Paley (2013). Nurs. Educ. Today 2014, 34, 954–957. [Google Scholar] [CrossRef] [PubMed]
- Timmins, F.; de Vries, J.M. Nurses Are Not Bystanders: A Response to Paley. Nurs. Educ. Today 2014, 34, 1269–1271. [Google Scholar] [CrossRef] [PubMed]
- The Mid Staffordshire NHS Foundation Trust Public Inquiry. Available online: https://www.gov.uk/government/publications/report-of-the-mid-staffordshire-nhs-foundation-trust-public-inquiry (accessed on 5 July 2019).
- Independent Inquiry into Care Provided by Mid Staffordshire NHS Foundation Trust January 2005 to March 2009. Available online: https://www.gov.uk/government/publications/independent-inquiry-into-care-provided-by-mid-staffordshire-nhs-foundation-trust-january-2001-to-march-2009 (accessed on 5 July 2019).
- Department of Health. Transforming Care: A national Response to Winterbourne View Hospital Department of Health Review: Final Report. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/213215/final-report.pdf (accessed on 5 July 2018).
- Kirkup, D. Report of the Morcambe Bay Investigation. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/408480/47487_MBI_Accessible_v0.1.pdf (accessed on 5 July 2019).
- Lander, B. Oakden: A shameful Chapter in South Australia’s History. Available online: https://icac.sa.gov.au/system/files/ICAC_Report_Oakden.pdf (accessed on 12 July 2019).
- Harrington, C.; Olney, B.; Carrillo, H.; Kang, T. Nurse Staffing and Deficiencies in the Largest For-Profit Nursing Home Chains and Chains Owned by Private Equity Companies. Health Serv. Res. J. 2012, 47, 106–128. [Google Scholar] [CrossRef] [PubMed]
- Ní Aodha, G. One-Fifth of Irish People Have Witnessed Poor Care for the Elderly. 2017. Available online: https://www.thejournal.ie/nursing-homes-3378787-May2017/ (accessed on 20 September 2019).
- International Council for Nurses. 2019 Nursing Definitions. Available online: https://www.icn.ch/nursing-policy/nursing-definitions (accessed on 5 July 2019).
- Nursing and Midwifery Council. 2019. Available online: https://www.nmc.org.uk/ (accessed on 5 July 2019).
- Nursing and Midwifery Board Australia. Available online: https://www.nursingmidwiferyboard.gov.au/ (accessed on 5 July 2019).
- American Nurses Association. Available online: https://www.nursingworld.org/ana/ (accessed on 5 July 2019).
- Darwin, A. Characteristics ascribed to mentors by their protégés. In The Situational Mentor; Clutterbuck, D., Lane, G., Eds.; Gower Publishing Limited: Burlington, VT, USA, 2004; pp. 1–15. [Google Scholar]
- Darling, L.A.W. What do Nurses Want in a Mentor? J. Nurs. Adm. 1984, 14, 42–44. [Google Scholar] [CrossRef]
- McSherry, R.; Pearce, P. What are the Effective Ways to Translate Clinical Leadership into Health Care Quality Improvement? J. Healthc. Leadersh. 2016, 8, 11–17. [Google Scholar] [CrossRef]
- Department of Health. A New NHS: Modern and Dependable; HMSO: London, UK, 1997.
- Snowden, M.; Ellwood, F.; McSherry, R.; Halsall, J.P.; Hough, D. Clinical governance: A friend or foe to dental care practice in the UK? Int. J. Percept. Public Health 2017, 1, 112–120. [Google Scholar]
- Bray, L.; Nettleton, P. Assessor or mentor? Role confusion in professional education. Nurs. Educ. Today 2007, 27, 848–855. [Google Scholar] [CrossRef]
- Huybrecht, S.; Loeckx, W.; Quaeyhaegens, Y.; De Tobel, D.; Mistiaen, W. Mentoring in Nursing Education: Perceived Characteristics of Mentors and the Consequences of Mentorship. Nur. Educ. Today 2011, 31. [Google Scholar] [CrossRef]
- Gopee, N. Mentoring and Supervision in Healthcare; Sage: London, UK, 2015; pp. 274–278. [Google Scholar]
- Snowden, M.; Halsall, J. Mentorship, Leadership and Research: Their Place within the Social Science Curriculum; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Snowden, M.; Hardy, T. Peer Mentorship and Positive Effects on Student Mentor and Mentee Retention and Academic Success. Widening Particip. Lifelong Learn. 2012, 14, 76–92. [Google Scholar] [CrossRef]
- Eby, L.T.; Allen, T.D.; Evans, S.C.; Ng, T.; Dubois, D.L. Does Mentoring Matter? A Multidisciplinary Meta-Analysis Comparing Mentored and Non-Mentored Individuals. J. Vocat. Behav. 2008, 72, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Snowden, M. Peer Mentoring. Guaranteed Gold? In Mentorship, Leadership and Research: Their Place within the Social Science Curriculum; Snowden, M., Halsall, J., Eds.; Springer International Publishing AG: Basel, Switzerland, 2019; pp. 117–128. [Google Scholar]
- Paglis, L.L.; Green, S.G.; Bauer, T.N. Does Adviser Mentoring Add Value? A Longitudinal Study of Mentoring and Doctoral Student Outcomes. Res. High. Educ. 2006, 47, 451–476. [Google Scholar] [CrossRef]
- Tonisandel, S.; Avery, D.R.; Phillips, M.G. Maximising Returns on Mentoring: Factors Affecting Subsequent Protégé Performance. J. Organ. Behav. 2007, 28, 89–110. [Google Scholar] [CrossRef]
- Williams, A.L.; Phillips, C.J.; Watkins, A.; Rushton, A.B. The Effect of Work Based Mentoring on Patient Outcomes in Musculoskeletal Physiotherapy: Study Protocol for Randomised Controlled Trial. Trials 2014, 15, 409. [Google Scholar] [CrossRef]
- Gray, O.; Brown, D. Evaluating a Nurse Mentor Preparation Programme. Br. J. Nurs. 2016, 25, 2–7. [Google Scholar] [CrossRef]
- Robson, C.; McCartan, K. Real world Research: A Resource for Users of Social Research Methods in Applied Settings, 4th ed.; John Wiley & Sons: London, UK, 2016. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 21.0; IBM Corp: Armonk, NY, USA, 2012. [Google Scholar]
- Timmins, F.; McCabe, C.; McSherry, R. Research awareness: Managerial challenges for nurses in the Republic of Ireland. J. Nurs. Manag. 2012, 20, 224–235. [Google Scholar] [CrossRef]
- World Health Organisation. Nursing and Midwifery Services, Strategies Directions (2002–2008); WHO: Geneva, Switzerland, 2002; Available online: https://www.who.int/hrh/nursing_midwifery/strategic_directions_en.pdf (accessed on 16 September 2019).
- Water, T.; Mccall, E.; Britnell, S.; Rae, M.; Thompson, S.; Mearns, G. Paediatric nurses’ understanding and utilisation of evidence based practice. Nurs. Praxis N. Z. 2018, 34. [Google Scholar]
- Gisbert-Trejo, N.; Landeta, L.; Albizu, E.; Fernández-Ferrín, P. Determining Effective Mentor Characteristics in Inter-Organizational Mentoring for Managers: An Approach Based on Academics’ and Practitioners’ Perspectives. Ind. Commer. Train. 2019, 51, 85–103. [Google Scholar] [CrossRef]
- Nursing and Midwifery Council. Standards for Student Supervision and Assessment. 2018. Available online: https://www.nmc.org.uk/standards-for-education-and-training/standards-for-student-supervision-and-assessment/ (accessed on 9 July 2019).
- Alred, G.; Garvey, B. Learning to produce knowledge—The contribution of mentoring. Mentor. Train. 2000, 8, 261–277. [Google Scholar] [CrossRef]
- Ruth-Sahd, L.A. Reflective Practice: A Critical Analysis of Data-Based Studies and Implications for Nursing Education. J. Nurs. Educ. 2003, 42, 488–497. [Google Scholar] [PubMed]
- Moon, J. Reflection in Learning and Professional Development: Theory and Practice; Routledge Falmer: London, UK, 2013. [Google Scholar]
- Clutterbuck, D. Everyone Needs a Mentor, 5th ed.; CIPD: London, UK, 2014. [Google Scholar]
- Wilson, A.M.E. Mentoring Student Nurses and the Educational Use of Self: A Hermeneutic Phenomenological Study. Nurs. Educ. Today 2014, 34, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Garvey, R.; Stokes, P.; Megginson, D. Coaching and Mentoring: Theory and Practice; Sage: London, UK, 2010; Volume 3, pp. 79–81. [Google Scholar]
- McSherry, R.; Pearce, P. Clinical Governance: A Guide to Implementation for Healthcare Professionals, 3rd ed.; John Wiley & Sons: London, UK, 2011. [Google Scholar]


{kind=link}
| Characteristic | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Not Relevant/Important | Less Relevant/Important | Neutral | Relevant/Important | Very Relevant/Important | |
| 1 | 1/0.9% | 1/0.9% | 16/14% | 35/31% | 59/53% |
| 2 | 1/0.9% | 0 | 6/5% | 38/34% | 66/59% |
| 3 | 1/0.9% | 3/3% | 8/7% | 33/29% | 67/60% |
| 4 | 1/0.9% | 5/4% | 21/19% | 38/34% | 47/42% |
| 5 | 1/0.9% | 4/4% | 26/23% | 49/44% | 32/29% |
| 6 | 1/0.9% | 4/4% | 22/20% | 42/37% | 43/38% |
| 7 | 2/2% | 2/2% | 23/20% | 47/42% | 38/34% |
| 8 | 6/5% | 17/15% | 31/28% | 30/27% | 28/25% |
| 9 | 1/0.9% | 9/8% | 22/20% | 48/43% | 32/29% |
| Characteristic | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Not Relevant/Important | Less Relevant/Important | Neutral | Relevant/Important | Very Relevant/Important | |
| 1 | 1/0.9% | 1.9% | 7/6% | 38/34% | 65/58% |
| 2 | 1/0.9% | 3/3% | 10/9% | 49/44% | 49/44% |
| 3 | 1/0.9% | 4/4% | 30/27% | 49/44% | 28/25% |
| 4 | 1/0.9% | 2/2% | 11/10% | 40/36% | 58/56% |
| 5 | 2/2% | 2/2% | 17/15% | 43/38% | 4/43% |
| 6 | 2/2% | 1/0.9% | 14/12% | 46/41% | 49/44% |
| 7 | 1/0.9% | 2/2% | 29/26% | 49/44% | 31/28% |
| 8 | 1/0.9% | 0 | 6/5% | 38/34% | 67/60% |
| 9 | 1/0.9% | 1/0.9% | 13/12% | 35/31% | 62/55% |
| 10 | 1/0.9% | 1/0.9% | 17/15% | 37/33% | 56/50% |
| 11 | 1/0.9% | 3/3% | 16/14% | 55/49% | 37/33% |
| 12 | 1/0.9% | 0 | 12/11% | 58/52% | 41/37% |
| 13 | 1/0.9% | 2/2% | 12/11% | 51/45% | 46/41% |
| 14 | 2/2% | 1/0.9% | 13/12% | 62/55% | 34/30% |
| 15 | 2/2% | 2/2% | 12/11% | 57/51% | 39/35% |
| 16 | 3/3% | 1/0.9% | 10/9% | 54/48% | 44/39% |
| Question | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree | |
| 1 | 2/2% | 4/4% | 9/8% | 52/46% | 45/40% |
| 2 | 3/3% | 2/2% | 15/13% | 50/45% | 42/37% |
| 3 | 2/2% | 3/3% | 22/20% | 54/48% | 31/28% |
| 4 | 1/0.9% | 3/3% | 19/17% | 62/55% | 27/24% |
| 5 | 1/0.9% | 3/3% | 27/24% | 47/42% | 34/30% |
| 6 | 2/2% | 4/4% | 31/28% | 53/47% | 22/20% |
| 7 | 2/2% | 7/6% | 37/33% | 39/35% | 27/24% |
| 8 | 5/4% | 13/12% | 35/31% | 38/34% | 21/19% |
| 9 | 1/0.9% | 8/7% | 41/37% | 31/28% | 31/28% |
| 10 | 1/0.9% | 10/9% | 30/27% | 42/37% | 28/25% |
| 11 | 2/2% | 7/6% | 33/29% | 51/45% | 19/17% |
| 12 | 2/2% | 8/7% | 20/18% | 54/48% | 28/25% |
| Yes | No | ||||
| 13 | 30/27% | 77/69% | |||
| 14 | 40/36% | 70/62% | |||
| 15 | 51/45% | 59/53% | |||
| 16 * | 39/35% | 73/65% | |||
| 17 * | 32/29% | 80/71% | |||
| 18 * | 26/23% | 86/77% | |||
| 19 * | 25/22% | 87/78% | |||
| 20 * | 33/29% | 79/70% | |||
| 21 * | 30/27% | 81/72% | |||
| 1 | 2 | 3 | 4 | ||
| 22 | 8/7% | 94/84% | 9/8% | 0 | |
| 23 | 1/9% | 103/92% | 6/5% | 0 | |
| Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|
| Characteristics 1: A Facilitatory Adviser | Characteristic 2: Critically Enabling Facilitator | Characteristic 3: A Change Facilitator | Characteristic 4: An Approachable Facilitator |
| Darling (1984) [18] | |||
| Feedback-Giver 0.614 | Standard Prodder 0.611 | Standard Prodder 0.534 | |
| Teacher-Coach 0.518 | |||
| Eye Opener 0.636 | |||
| Door Opener 0.646 | Career Counsellor 0.659 | ||
| Idea-Bouncer 0.552 | |||
| Problem-Solver 0.550 | |||
| Darwin (2004) [17] | |||
| Approachable 0.775 | Friendly 0.535 | ||
| Friendly 0.623 | |||
| No bias and non-judgmental 0.778 | |||
| Patient 0.797 | |||
| Enthusiastic 0.792 | |||
| Negotiation Skills 0.728 | Nice 0.709 | ||
| Trust 0.700 | |||
| Communication 0.748 | |||
| Empathy 0.747 | |||
| Empowering 0.790 | |||
| Confident 0.794 | |||
| Motivation 0.842 | |||
| Reflective 0.783 | |||
| Leadership 0.800 | |||
| Willingness 0.758 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McSherry, R.; Snowden, M. Exploring Primary Healthcare Students and Their Mentors’ Awareness of Mentorship and Clinical Governance as Part of a Local Continuing Professional Development (CPD) Program: Findings of a Quantitative Survey. Healthcare 2019, 7, 113. https://doi.org/10.3390/healthcare7040113
McSherry R, Snowden M. Exploring Primary Healthcare Students and Their Mentors’ Awareness of Mentorship and Clinical Governance as Part of a Local Continuing Professional Development (CPD) Program: Findings of a Quantitative Survey. Healthcare. 2019; 7(4):113. https://doi.org/10.3390/healthcare7040113
Chicago/Turabian StyleMcSherry, Robert, and Michael Snowden. 2019. "Exploring Primary Healthcare Students and Their Mentors’ Awareness of Mentorship and Clinical Governance as Part of a Local Continuing Professional Development (CPD) Program: Findings of a Quantitative Survey" Healthcare 7, no. 4: 113. https://doi.org/10.3390/healthcare7040113