The Impact of the Moderating Effect of Psychological Health Status on Nurse Healthcare Management Information System Usage Intention


Abstract
:1. Introduction
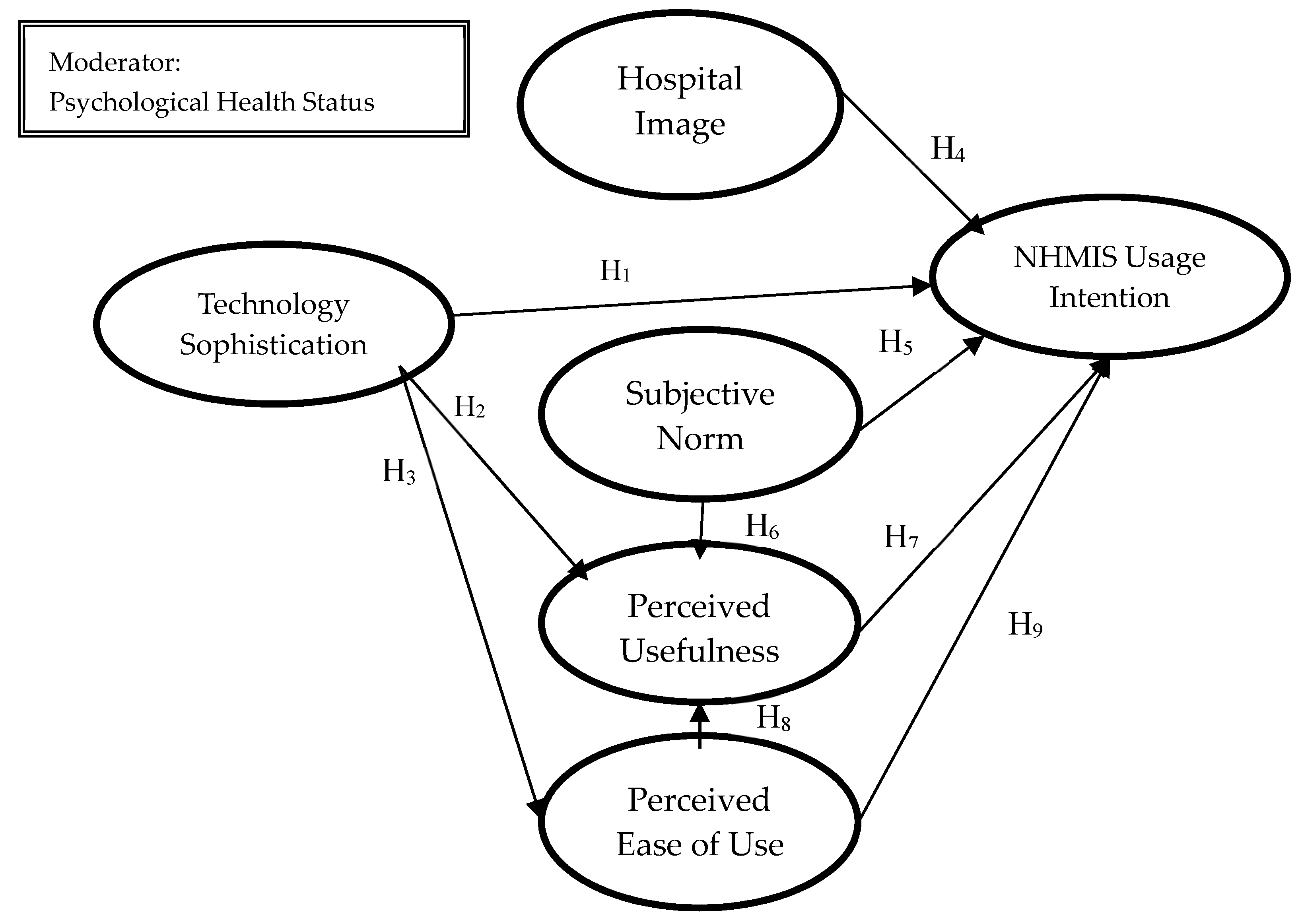
2. Theoretical Framework, Hypotheses, and Rationale
2.1. Technology Sophistication
2.2. Hospital Image
2.3. Subjective Norm
2.4. The Original Technology Acceptance Model
2.5. Psychological Health Status
3. Methods
3.1. Design and Participants
3.2. Questionnaire Design, Expert Panel, and Pilot Test
3.3. Measures
3.4. Data Analysis Tools
4. Results
4.1. Descriptive Results
4.2. Reliability Test Results
4.3. Test of the Hypothesized Model
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Qian, Q.-W.; Zhong, X.-F.; Tao, F.-B. Suicidal behavior and subhealth among High School students in Bengbu City. Chin. J. Public Health 2009, 25, 1151–1152. [Google Scholar]
- Fei, Z.F. Main physiological indexes and comprehensive imaging evaluation of sub-health state. Acta Univ. Tradit. Med. Sin. Pharmacol. Shanghai 2008, 122, 6–11. [Google Scholar]
- Thompson, T.G.; Brailer, D.J. The Decade of Health Information Technology: Delivering Consumer-Centric and Information-Rich Health Care; US Department of Health and Human Services: Washington, DC, USA, 2004.
- Blumenthal, D.; Glaser, J.P. Information technology comes to medicine. N. Engl. J. Med. 2007, 356, 2527–2534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.-H.; Wang, S.-C.; Lin, L.-M. Mobile computing acceptance factors in the healthcare industry: A structural equation model. Int. J. Med. Inf. 2007, 76, 66–77. [Google Scholar] [CrossRef]
- Angst, C.M.; Agarwal, R. Getting Personal About Electronic Health Records: Modeling the Beliefs of Personal Health Record Users and Non-Users; Robert H. Smith School Research Paper No. RHS-06-007; Springer: Cham, Switzerland, 2006. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Wadie, N.; Lanouar, C. An exploration of Facebook. com adoption in Tunisia using Technology Acceptance Model (Tam) and Theory of Reasoned Action (Tra). Interdiscip. J. Contemp. Res. Bus. 2012, 4, 948–968. [Google Scholar]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the Technology Acceptance Model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Bala, H. Technology Acceptance Model 3 and a research agenda on interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V. Determinants of perceived ease of use: Integrating control, intrinsic motivation, and emotion into the Technology Acceptance Model. Inf. Syst. Res. 2000, 11, 342–365. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Long, Y.; Zhang, T.; Niu, X.H.; Sun, W.; Shan, G.L.; Wang, Z.Z. Sub-Health status of the young and middle-aged populations and the relationships among sub-health, sleepness and personality in Hubei Province, China. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua Liuxingbingxue Zazhi 2010, 31, 970–974. [Google Scholar]
- Holden, R.J.; Karsh, B.T. The Technology Acceptance Model: Its past and its future in health care. J. Biomed. Inf. 2010, 43, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, C. The effects of national culture values on consumer acceptance of e-commerce: Online shoppers in China. Inf. Manag. 2009, 46, 294–301. [Google Scholar] [CrossRef]
- King, W.R.; He, J. A meta-analysis of the Technology Acceptance Model. Inf. Manag. 2006, 43, 740–755. [Google Scholar] [CrossRef]
- Lee, Y.; Kozar, K.A.; Larsen, K.R.T. The Technology Acceptance Model: Past, present, and future. Commun. Assoc. Inf. Syst. 2003, 12, 50. [Google Scholar] [CrossRef]
- Marangunić, N.; Granić, A. Technology Acceptance Model: A literature review from 1986 to 2013. Univers. Access Inf. Soc. 2015, 14, 81–95. [Google Scholar] [CrossRef]
- Ooi, K.-B.; Tan, G.W. Mobile Technology Acceptance Model: An investigation using mobile users to explore smartphone credit card. Expert Syst. Appl. 2016, 59, 33–46. [Google Scholar] [CrossRef]
- Wu, J.-H.; Wang, S.-C. What drives mobile commerce? An empirical evaluation of the revised Technology Acceptance Model. Inf. Manag. 2005, 42, 719–729. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Todd, P. Decomposition and crossover effects in the Theory of Planned Behavior: A study of consumer adoption intentions. Int. J. Res. Mark. 1995, 12, 137–155. [Google Scholar] [CrossRef]
- Bandura, A. Social Cognitive Theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-R.; Tseng, H.S. Factors that influence acceptance of web-based e-learning systems for the in-service education of junior High School teachers in Taiwan. Eval. Program Plan. 2012, 35, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Raleting, T.; Nel, J. Determinants of low-income non-users attitude towards wig mobile phone banking: Evidence from South Africa. Afr. J. Bus. Manag. 2011, 5, 212–223. [Google Scholar]
- Park, N. Adoption and use of computer-based voip phone service: Toward an integrated model. In Proceedings of the Annual Meeting of the International Communication Association, Montreal, QC, Canada, 22–26 May 2008. [Google Scholar]
- Hernández, B.; Jiménez, J.; Martín, M.J. Customer behavior in electronic commerce: The moderating effect of e-purchasing experience. J. Bus. Res. 2010, 63, 964–971. [Google Scholar] [CrossRef]
- Eastin, M.S.; LaRose, R. Internet self-efficacy and the psychology of the digital divide. J. Comput. Mediat. Commun. 2000, 6. [Google Scholar] [CrossRef]
- Akinci, F.; Esatoglu, A.E.; Tengilimoglu, D.; Parsons, A. Hospital choice factors: A case study in Turkey. Health Mark. Q. 2005, 22, 3–19. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Misconceptions about the fishbein model: Reflections on a study by Songer-Nocks. J. Exp. Soc. Psychol. 1976, 12, 579–584. [Google Scholar] [CrossRef]
- Karahanna, E.; Straub, D.W.; Chervany, N.L. Information technology adoption across time: A cross-sectional comparison of pre-adoption and post-adoption beliefs. MIS Q. 1999, 23, 183–213. [Google Scholar] [CrossRef]
- Davis, F.D. User acceptance of information technology: System characteristics, user perceptions and behavioral impacts. Int. J. Man Mach. Stud. 1993, 38, 475–487. [Google Scholar] [CrossRef] [Green Version]
- Adams, A.D.; Nelson, R.R.; Todd, P.A. Perceived usefulness, ease of use, and usage of information technology: A replication. MIS Q. 1992, 16, 227–247. [Google Scholar] [CrossRef]
- Legris, P.; Ingham, J.; Collerette, P. Why do people use information technology? A critical review of the Technology Acceptance Model. Inf. Manag. 2003, 40, 191–204. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A model of the antecedents of perceived ease of use: Development and test. Decis. Sci. 1996, 27, 451–481. [Google Scholar] [CrossRef]
- Dünnebeil, S.; Sunyaev, A.; Blohm, I.; Leimeister, J.; Krcmar, H. Determinants of physicians’ technology acceptance for e-health in ambulatory care. Int. J. Med. Inf. 2012, 81, 746–760. [Google Scholar] [CrossRef] [Green Version]
- Ilie, N.; Hickel, R. Investigations on mechanical behaviour of dental composites. Clin. Oral Investig. 2009, 13, 427. [Google Scholar] [CrossRef] [PubMed]
- Teo, H.T.S.; Lim, V.K.G.; Lai, R.Y.C. Intrinsic and extrinsic motivation in internet usage. Omega 27 1999, 25–37. [Google Scholar] [CrossRef]
- Johnson, M.P.; Zheng, K.; Padman, R. Modeling the longitudinality of user acceptance of technology with an evidence-adaptive clinical decision support system. Decis. Support. Syst. 2014, 57, 444–453. [Google Scholar] [CrossRef]
- Polančič, G.; Hericko, M.; Rozman, I. An empirical examination of application frameworks success based on Technology Acceptance Model. J. Syst. Softw. 2010, 83, 574–584. [Google Scholar] [CrossRef]
- Lishan, X.; Chiuan, Y.C.; Choolani, M.; Chuan, C.H. The perception and intention to adopt female-focused healthcare applications (Fha): A comparison between healthcare workers and non-healthcare workers. Int. J. Med. Inf. 2009, 78, 248–258. [Google Scholar] [CrossRef]
- Davis, F.; Bagozzi, R.; Warshaw, P. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Pan, P.-C.; Goldberg, D.P. A comparison of the validity of Ghq-12 and Chq-12 in Chinese primary care patients in Manchester. Psychol. Med. 1990, 20, 931–940. [Google Scholar] [CrossRef]
- Yang, Z.T.; Huang, L.; Wu, Z.Y. The application of Chinese health questionnaire for mental disorder screening in community settings in Mainland China. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua Liuxingbingxue Zazhi 2003, 24, 769–773. [Google Scholar]
- Kuo, S.-F.; Hou, W.-H.; Chang, C.C.; Liao, Y.-M.; Cheng, S.-Y.; Chou, Y.H.; Yeh, Y.-C.; Lin, Y.-K.; Chen, I.-H. Development and psychometric testing of the Chinese version of the resilience scale for Southeast Asian immigrant women who divorced in Taiwan. PLoS ONE 2019, 14, e0211451. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, P.D.; Hillier, V.F. A scaled version of the general health questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Furnham, A.; Cheng, H. Ghq score changes from teenage to young adulthood. J. Psychiatr. Res. 2019, 113, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Barquero, L.J.; Diez-Manrique, J.F.; Pena, C.; Quintanal, R.G.; Lopez, M.L. Two stage design in a community survey. Br. J. Psychiatr. 1986, 149, 88–97. [Google Scholar] [CrossRef]
- Burvill, W.P.; Knuiman, M.W. Which version of the general health questionnaire should be used in community studies? Aust. N. Z. J. Psychiatr. 1983, 17, 237–242. [Google Scholar] [CrossRef]
- Chong, M.-Y.; Wilkinson, G. Validation of 30-and 12-item versions of the Chinese health questionnaire (Chq) in patients admitted for general health screening. Psychol. Med. 1989, 19, 495–505. [Google Scholar] [CrossRef]
- Lung, F.-W.; Lee, F.-Y.; Shu, B.-C. The relationship between life adjustment and parental bonding in military personnel with adjustment disorder in Taiwan. Mil. Med. 2002, 167, 678–682. [Google Scholar]
- Chen, C.-C.; Wu, W.-C.; Chang, S.-S.; Chang, C.-B.; Yang, C.-T.J.; Su, H.-K.; Chan, D.-C.D. Common mental disorders in Taiwanese consumers of commercial low-dose computed tomography lung cancer screening: Comparison with a nationally representative sample. J. Formos. Med. Assoc. 2019. [Google Scholar] [CrossRef]
- Sheeran, P.; Abraham, C. The health belief model. Predict. Health Behav. 1996, 2, 29–80. [Google Scholar]
- Tang, C.P.; Ash, J.S.; Bates, D.W.; Overhage, M.J.; Sands, D.Z. Personal health records: Definitions, benefits, and strategies for overcoming barriers to adoption. J. Am. Med.Inf. Assoc. 2006, 13, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.D.; Schindler, P.S.; Sun, J. Business Research Methods; McGraw-Hill Irwin: New York, NY, USA, 2006; Volume 9. [Google Scholar]
- Chao, C.-M. Will economic integration between Mainland China and Taiwan lead to a congenial political culture? Asian Surv. 2003, 43, 280–304. [Google Scholar] [CrossRef]
- Thatcher, B.S.M.; Foster, W.; Zhu, L. B2b E-Commerce adoption decisions in Taiwan: The interaction of cultural and other institutional factors. Electron. Commer. Res. Appl. 2006, 5, 92–104. [Google Scholar] [CrossRef]
- Lampton, D.M. The Politics of Medicine in China: The Policy Process 1949–1977; Routledge: London, UK, 2019. [Google Scholar]
- Cheng, A.T.; Wu, J.T.; Chong, M.Y.; Williams, P. Internal consistency and factor structure of the Chinese health questionnaire. Acta Psychiatr. Scand. 1990, 82, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.S.; Tsang, H.Y.; Chang, M.Y.; Tang, T.C. Validation of the Chinese health questionnaire (Chq-12) in community elders. Kaohsiung J. Med. Sci. 2000, 16, 559–565. [Google Scholar]
- Wang, W.T.; Cheng, S.Y.; Huang, L.Y. Technology-Based Service Encounters Using Self-Service Technologies in the Healthcare Industry. Int. J. Human-Comp. Inter. 2013, 3, 139–155. [Google Scholar] [CrossRef]
- Bem, S.L. Gender schema theory: A cognitive account of sex typing. Psychol. Rev. 1981, 88, 354. [Google Scholar] [CrossRef]
- Berdie, D.R. Reassessing the value of high response rates to mail surveys. Mark. Res. 1989, 1, 52–64. [Google Scholar]
- Kim, J.; Park, H.A. Development of a health information technology acceptance model using consumers’ health behavior intention. J. Med. Internet Res. 2012, 14, e133. [Google Scholar] [CrossRef]
- Yun, E.K.; Park, H.A. Consumers’ disease information-seeking behaviour on the internet in Korea. J. Clin. Nurs. 2010, 19, 2860–2868. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Xue, L.; Yen, C.C.; Chang, L.; Chan, H.C.; Tai, B.C.; Tan, S.B.; Duh, H.B.L.; Choolani, M. An exploratory study of ageing women’s perception on access to health informatics via a mobile phone-based intervention. Int. J. Med. Inf. 2012, 81, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Srite, M. Culture as an explanation of technology acceptance differences: An empirical investigation of Chinese and us users. Australas. J.Inf. Syst. 2006, 14. [Google Scholar] [CrossRef]
- Javalgi, R.; Whipple, T.; McManamon, M.K.; Edick, V.L. Hospital image: A correspondence analysis approach. J. Health Care Mark. 1992, 12, 34–41. [Google Scholar]
- Kim, K.H.; Kim, K.S.; Kim, D.Y.; Kim, J.H.; Kang, S.H. Brand Equity in Hospital Marketing. J Bus Res. 2008, 1, 75–82. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Construct | Operational Definition | # of Items | Researches |
|---|---|---|---|
| Psychological health status | Employed the Chinese Health Questionnaire (CHQ-12) to measure nurses’ psychological health status | 12 | [58,59] |
| Technology sophistication | Having an active email account, the number of online activity, and online count (e.g., shopped or purchased something on an online auction, ordered medications, or managed prescriptions) were included to assess ability to use information | 6 | [6] |
| Hospital image | The sum of the beliefs, ideas, and impressions of patients and/or the general public with regard to a hospital, which were developed based on their past experience with the hospital | 4 | [60] |
| Perceived usefulness | The degree to which a nurse believes that the use of HMIS would enhance his or her health | 5 | [31,41] |
| Perceived ease of use | The degree to which a nurse believes that the use of HMIS would be free of effort | 4 | [31,41] |
| Subjective norm | The degree to which a nurse believes that people who are important to her/him thinks he/she should perform the behavior | 4 | [20,61] |
| HMIS usage intention | Nurses’ intention to use NHMIS | 3 | [21] |
| Demographic | Category | Taiwan (n = 142) | Northeast of China (n = 1422) | F-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PU | PEOU | SN | HI | TS | UI | PHS | ||||
| Gender | male | 2 | 17 | 0.196 | 0.839 | 0.465 | 0.315 | 1.191 | 0.749 | 1.193 |
| female | 140 | 1406 | ||||||||
| Education background | high school | 1 | 15 | 0.648 | 1.583 | 0.787 | 2.298 | 1.471 | 1.212. | 2.403 |
| college | 45 | 618 | ||||||||
| university | 74 | 782 | ||||||||
| graduate | 22 | 8 | ||||||||
| Marriage status | married | 88 | 776 | 2.190 | 0.588 | 2.100 | 2.431 * | 2.089 * | 1.755 | 0.010 |
| single | 54 | 647 | ||||||||
| Psychological health status | negative | 47 | 385 | 3.908 * n > p | 2.222 * n > p | 3.605 * n > p | 3.463 * n > p | 2.668 * n > p | 4.088 * n > p | 2.980 * n > p |
| positive | 95 | 1038 | ||||||||
| Variables | Cronbach’s Alpha |
|---|---|
| Perceived Ease of Use | 0.917 |
| Perceived Usefulness | 0.923 |
| Subjective Norm | 0.912 |
| Hospital Image | 0.920 |
| Technology Sophistication | 0.921 |
| NHMIS Usage Intention | 0.936 |
| Psychological health status | 0.771 |
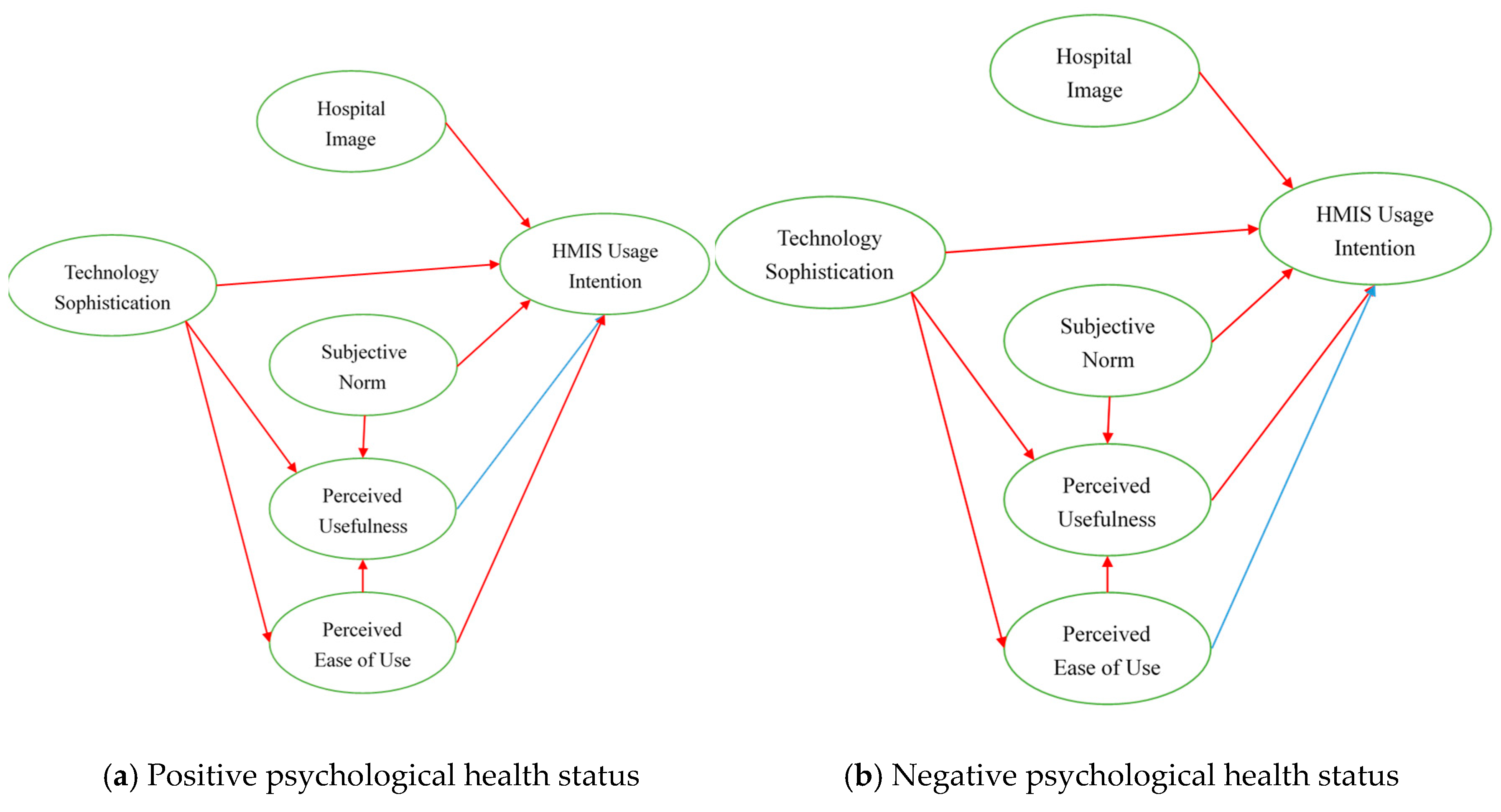
| Hypotheses | Full Sample (n = 1563) | Positive Psychological Health Status (n = 1146) | Negative Psychological Health Status (n = 417) |
|---|---|---|---|
| H1 | 0.28 * | 0.27 * | 0.29 * |
| H2 | 0.15 * | 0.11 * | 0.24 * |
| H3 | 0.60 * | 0.61 * | 0.54 * |
| H4 | 0.49 * | 0.50 * | 0.44 * |
| H5 | 0.37 * | 0.39 * | 0.35 * |
| H6 | 0.62 * | 0.68 * | 0.56 * |
| H7 | 0.10 * | 0.03 | 0.18 * |
| H8 | 0.30 * | 0.44 * | 0.30 * |
| H9 | 0.07 * | 0.16 * | −0.08 |
| R2 | 0.56 | 0.58 | 0.52 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, S.-J.; Tseng, H.-T. The Impact of the Moderating Effect of Psychological Health Status on Nurse Healthcare Management Information System Usage Intention. Healthcare 2020, 8, 28. https://doi.org/10.3390/healthcare8010028
Hsiao S-J, Tseng H-T. The Impact of the Moderating Effect of Psychological Health Status on Nurse Healthcare Management Information System Usage Intention. Healthcare. 2020; 8(1):28. https://doi.org/10.3390/healthcare8010028
Chicago/Turabian StyleHsiao, Shih-Jung, and Hsiao-Ting Tseng. 2020. "The Impact of the Moderating Effect of Psychological Health Status on Nurse Healthcare Management Information System Usage Intention" Healthcare 8, no. 1: 28. https://doi.org/10.3390/healthcare8010028