Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Head-Up Tilt Test with Cerebral Blood Flow and Stroke Volume Measurements
2.3. Cerebral Blood Flow Determination by Doppler Echographic Measurements
2.4. Stroke Volume Determination by Doppler Echocardiographic Measurements:
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
Patient Clinical and Echo Doppler Data
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine (IOM) (Ed.) Beyond Mayalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Van Campen, C. (L).M.C.; Verheugt, F.W.A.; Rowe, P.C.; Visser, F.C. Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: A quantitative, controlled study using Doppler echography. Clin. Neurophysiol. Pract. 2020, 5, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Van Campen, C. (L).M.C.; Verheugt, F.W.A.; Visser, F.C. Cerebral blood flow changes during tilt table testing in healthy volunteers, as assessed by Doppler imaging of the carotid and vertebral arteries. Clin. Neurophysiol. Pract. 2018, 3, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, R.S.; Grubb, B.P., II; Olshansky, B.; Shen, W.K.; Calkins, H.; Brignole, M.; Raj, S.R.; Krahn, A.D.; Morillo, C.A.; Stewart, J.M.; et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015, 12, e41–e63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, W.K.; Sheldon, R.S.; Benditt, D.G.; Cohen, M.I.; Forman, D.E.; Goldberger, Z.D.; Grubb, B.P.; Hamdan, M.H.; Krahn, A.D.; Link, M.S.; et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2017, 70, 620–663. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton. Neurosci. 2011, 161, 46–48. [Google Scholar] [CrossRef] [PubMed]
- Wyller, V.B.; Due, R.; Saul, J.P.; Amlie, J.P.; Thaulow, E. Usefulness of an abnormal cardiovascular response during low-grade head-up tilt-test for discriminating adolescents with chronic fatigue from healthy controls. Am. J. Cardiol. 2007, 99, 997–1001. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A.; International Chronic Fatigue Syndrome Study Group. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Van de Sande, M.I.; DE Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [Green Version]
- Van Campen, C.M.C.; Visser, F.C. The abnormal Cardiac Index and Stroke Volume Index changes during a normal Tilt Table Test in ME/CFS patients compared to healthy volunteers, are not related to deconditioning. J. Thromb. Circ. 2018. [Google Scholar] [CrossRef]
- Sato, K.; Ogoh, S.; Hirasawa, A.; Oue, A.; Sadamoto, T. The distribution of blood flow in the carotid and vertebral arteries during dynamic exercise in humans. J. Physiol. 2011, 589 Pt 11, 2847–2856. [Google Scholar] [CrossRef]
- Kusumoto, F.; Venet, T.; Schiller, N.B.; Sebastian, A.; Foster, E. Measurement of aortic blood flow by Doppler echocardiography: Temporal, technician, and reader variability in normal subjects and the application of generalizability theory in clinical research. J. Am. Soc. Echocardiogr. 1995, 8 Pt 1, 647–653. [Google Scholar] [CrossRef]
- Van Campen, C. (L).M.C.; Visser, F.C.; De Cock, C.C.; Vos, H.S.; Kamp, O.; Visser, C.A. Comparison of the haemodynamics of different pacing sites in patients undergoing resynchronisation treatment: Need for individualisation of lead localisation. Heart 2006, 92, 1795–1800. [Google Scholar] [CrossRef] [PubMed]
- Ostchega, Y.; Porter, K.S.; Hughes, J.; Dillon, C.F.; Nwankwo, T. Resting Pulse Rate Reference Data for Children, Adolescents, and Adults: United States, 1999–2008; National Health Stat Report; National Center for Health Statistics: Hyattsville, MD, USA, 2011; pp. 1–16. [Google Scholar]
- Schondorf, R.; Benoit, J.; Stein, R. Cerebral autoregulation in orthostatic intolerance. Ann. N. Y. Acad. Sci. 2001, 940, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Moya, A.; Sutton, R.; Ammirati, F.; Blanc, J.J.; Brignole, M.; Dahm, J.B.; Deharo, J.C.; Gajek, J.; Gjesdal, K.; Krahn, A.; et al. Guidelines: Guidelines for the diagnosis and management of syncope (version 2009): The Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur. Heart J. 2009, 30, 2631–2671. [Google Scholar]
- Haubrich, C.; Pies, K.; Dafotakis, M.; Block, F.; Kloetzsch, C.; Diehl, R.R. Transcranial Doppler monitoring in Parkinson’s disease: Cerebrovascular compensation of orthostatic hypotension. Ultrasound Med. Biol. 2010, 36, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Mankovsky, B.N.; Piolot, R.; Mankovsky, O.L.; Ziegler, D. Impairment of cerebral autoregulation in diabetic patients with cardiovascular autonomic neuropathy and orthostatic hypotension. Diabet. Med. 2003, 20, 119–126. [Google Scholar] [CrossRef]
- Purewal, T.S.; Watkins, P.J. Postural hypotension in diabetic autonomic neuropathy: A review. Diabet. Med. 1995, 12, 192–200. [Google Scholar] [CrossRef]
- Fuente Mora, C.; Palma, J.A.; Kaufmann, H.; Norcliffe-Kaufmann, L. Cerebral autoregulation and symptoms of orthostatic hypotension in familial dysautonomia. J. Cereb. Blood Flow Metab. 2017, 37, 2414–2422. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.M.; Jones, D.W.; Sinnott, A.; Brugniaux, J.V.; New, K.J.; Hodson, D.; Marley, C.J.; Smirl, J.D.; Ogoh, S.; Ainslie, P.N. Impaired cerebral haemodynamic function associated with chronic traumatic brain injury in professional boxers. Clin. Sci. (Lond.) 2013, 124, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Wong, B.J.; Sheriff, D.D. Role of splanchnic constriction in governing the hemodynamic responses to gravitational stress in conscious dogs. J. Appl. Physiol. 2011, 111, 40–47. [Google Scholar] [CrossRef]
- Deegan, B.M.; Sorond, F.A.; Galica, A.; Lipsitz, L.A.; O’Laighin, G.; Serrador, J.M. Elderly women regulate brain blood flow better than men do. Stroke 2011, 42, 1988–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razumovsky, A.Y.; DeBusk, K.; Calkins, H.; Snader, S.; Lucas, K.E.; Vyas, P.; Hanley, D.F.; Rowe, P.C. Cerebral and systemic hemodynamics changes during upright tilt in chronic fatigue syndrome. J. Neuroimaging 2003, 13, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Urbano, F.; Roux, F.; Schindler, J.; Mohsenin, V. Impaired cerebral autoregulation in obstructive sleep apnea. J. Appl. Physiol. 2008, 105, 1852–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treger, I.; Shafir, O.; Keren, O.; Ring, H. Cerebral blood flow velocity during postural changes on tilt table in stroke patients. Eur. Medicophys. 2005, 41, 293–296. [Google Scholar]
- Iwasaki, K.; Levine, B.D.; Zhang, R.; Zuckerman, J.H.; Pawelczyk, J.A.; Diedrich, A.; Ertl, A.; Cox, J.; Cooke, W.; Giller, C.; et al. Human cerebral autoregulation before, during and after spaceflight. J. Physiol. 2007, 579 Pt 3, 799–810. [Google Scholar] [CrossRef]
- Thomas, K.N.; Burgess, K.R.; Basnyat, R.; Lucas, S.J.; Cotter, J.D.; Fan, J.L.; Peebles, K.C.; Lucas, R.A.I.; Ainslie, P.N. Initial orthostatic hypotension at high altitude. High Alt. Med. Biol. 2010, 11, 163–167. [Google Scholar] [CrossRef]
- Van Beek, A.H.; Sijbesma, J.C.; Jansen, R.W.; Rikkert, M.G.; Claassen, J.A. Cortical oxygen supply during postural hypotension is further decreased in Alzheimer’s disease, but unrelated to cholinesterase-inhibitor use. J. Alzheimers Dis. 2010, 21, 519–526. [Google Scholar] [CrossRef]
- Lipsitz, L.A.; Mukai, S.; Hamner, J.; Gagnon, M.; Babikian, V. Dynamic regulation of middle cerebral artery blood flow velocity in aging and hypertension. Stroke 2000, 31, 1897–1903. [Google Scholar] [CrossRef] [Green Version]
- Low, P.A.; Novak, V.; Spies, J.M.; Novak, P.; Petty, G.W. Cerebrovascular regulation in the postural orthostatic tachycardia syndrome (POTS). Am. J. Med. Sci. 1999, 317, 124–133. [Google Scholar] [CrossRef]
- Morrison, S.A.; Ainslie, P.N.; Lucas, R.A.; Cheung, S.S.; Cotter, J.D. Compression garments do not alter cerebrovascular responses to orthostatic stress after mild passive heating. Scand. J. Med. Sci. Sports 2014, 24, 291–300. [Google Scholar] [CrossRef]
- Novak, P. Hypocapnic cerebral hypoperfusion: A biomarker of orthostatic intolerance. PLoS ONE 2018, 13, e0204419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, V.E.; Wight, V.L.; Brown, C.M.; Hainsworth, R. Vascular responses to orthostatic stress in patients with postural tachycardia syndrome (POTS), in patients with low orthostatic tolerance, and in asymptomatic controls. Clin. Auton. Res. 2000, 10, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, H.T.; Park, K.M.; Ha, S.Y.; Kim, S.E.; Shin, K.J.; Kim, S.E.; Jang, W.; Kim, J.S.; Youn, J.; et al. Orthostatic dizziness in Parkinson’s disease is attributed to cerebral hypoperfusion: A transcranial doppler study. J. Clin. Ultrasound 2017, 45, 337–342. [Google Scholar] [CrossRef]
- Shin, K.J.; Kim, S.E.; Park, K.M.; Park, J.; Ha, S.Y.; Kim, S.E.; Kwon, O.Y. Cerebral hemodynamics in orthostatic intolerance with normal head-up tilt test. Acta Neurol. Scand. 2016, 134, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Ocon, A.J.; Messer, Z.R.; Medow, M.S.; Stewart, J.M. Increasing orthostatic stress impairs neurocognitive functioning in chronic fatigue syndrome with postural tachycardia syndrome. Clin. Sci. (Lond.) 2012, 122, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Verbree, J.; Bronzwaer, A.S.; Ghariq, E.; Versluis, M.J.; Daemen, M.J.; Van Buchem, M.A.; Dahan, A.; Van Lieshout, J.J.; Van Osch, M.J.P. Assessment of middle cerebral artery diameter during hypocapnia and hypercapnia in humans using ultra-high-field MRI. J. Appl. Physiol. 2014, 117, 1084–1089. [Google Scholar] [CrossRef] [Green Version]
- Coverdale, N.S.; Gati, J.S.; Opalevych, O.; Perrotta, A.; Shoemaker, J.K. Cerebral blood flow velocity underestimates cerebral blood flow during modest hypercapnia and hypocapnia. J. Appl. Physiol. 2014, 117, 1090–1096. [Google Scholar] [CrossRef] [Green Version]
- Al-Khazraji, B.K.; Shoemaker, L.N.; Gati, J.S.; Szekeres, T.; Shoemaker, J.K. Reactivity of larger intracranial arteries using 7 T MRI in young adults. J. Cereb. Blood Flow Metab. 2019, 39, 1204–1214. [Google Scholar] [CrossRef]
- Immink, R.V.; Pott, F.C.; Secher, N.H.; Van Lieshout, J.J. Hyperventilation, cerebral perfusion, and syncope. J. Appl. Physiol. 2014, 116, 844–851. [Google Scholar] [CrossRef] [Green Version]
- Huisjes, R.; Bogdanova, A.; Van Solinge, W.W.; Schiffelers, R.M.; Kaestner, L.; Van Wijk, R. Squeezing for Life—Properties of Red Blood Cell Deformability. Front. Physiol. 2018, 9, 656. [Google Scholar] [CrossRef]
- Qiu, Y.; Myers, D.R.; Lam, W.A. The biophysics and mechanics of blood from a materials perspective. Nat. Rev. Mater. 2019, 4, 294–311. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hou, W.; Chui, J.; Han, R.; Gelb, A.W. Cardiac output and cerebral blood flow: The integrated regulation of brain perfusion in adult humans. Anesthesiology 2015, 123, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; De Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny Rose, A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Kardiol. Pol. 2018, 76, 1119–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschlbock, S.; Wenning, G.; Fanciulli, A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J. Neural. Transm. (Vienna) 2017, 124, 1567–1605. [Google Scholar] [CrossRef] [Green Version]
- Hainsworth, R.; Al-Shamma, Y.M. Cardiovascular responses to upright tilting in healthy subjects. Clin. Sci. (Lond.) 1988, 74, 17–22. [Google Scholar] [CrossRef]
- Cooper, V.L.; Hainsworth, R. Head-up sleeping improves orthostatic tolerance in patients with syncope. Clin. Auton. Res. 2008, 18, 318–324. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Supine | End of Study | p-Value | |
|---|---|---|---|
| Heart rate (bpm) | 83 (13) | 104 (23) | <0.0001 |
| Systolic blood pressure (mmHg) | 134 (11) | 138 (14) | 0.10 |
| Diastolic blood pressure (mmHg) | 80 (9) | 86 (9) | 0.0006 |
| End-tidal CO2 (mmHg) | 38 (3) | 29 (6) | <0.0001 |
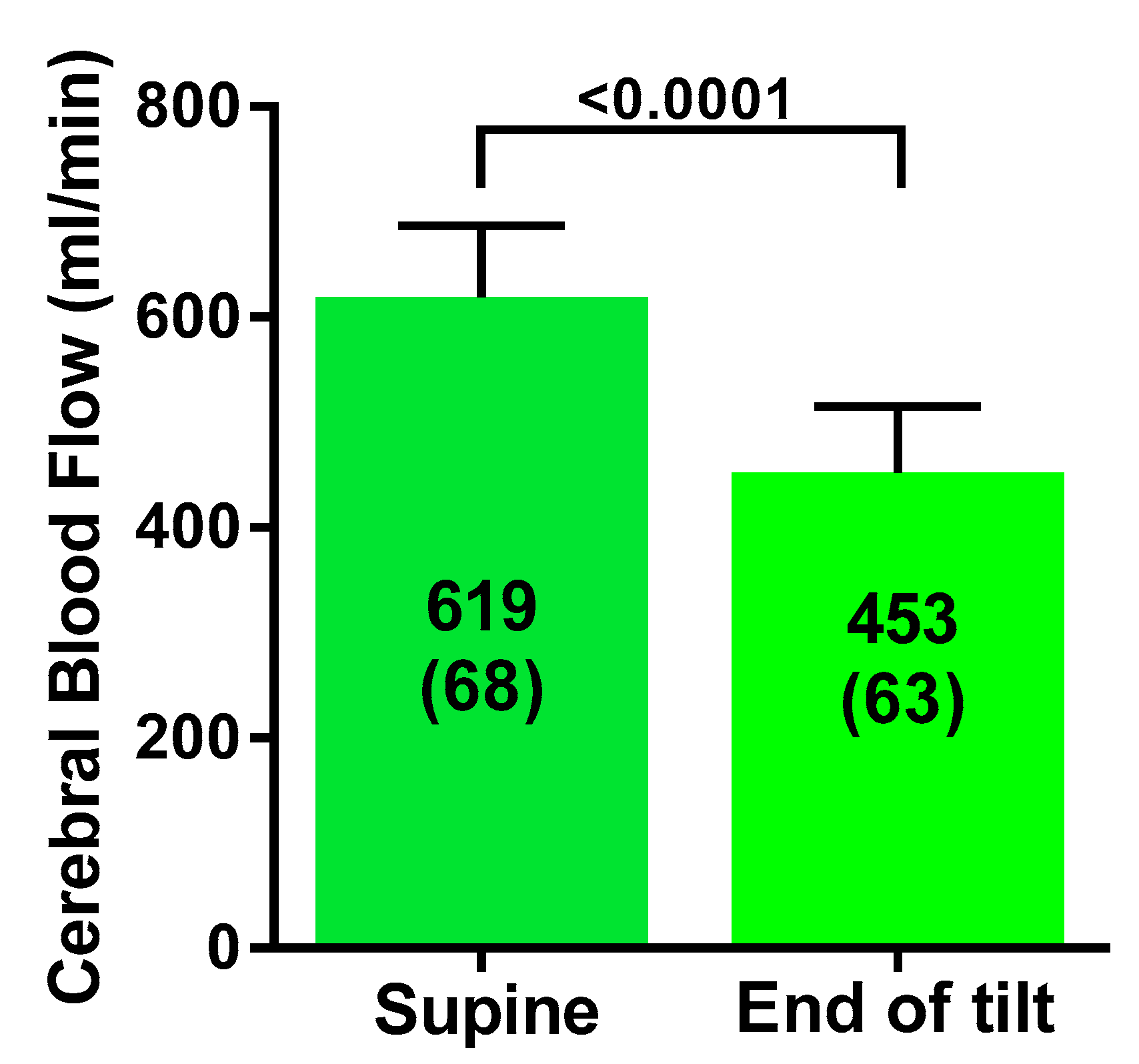
| Cerebral blood flow (mL/min) | 619 (68) | 453 (63) | <0.0001 |
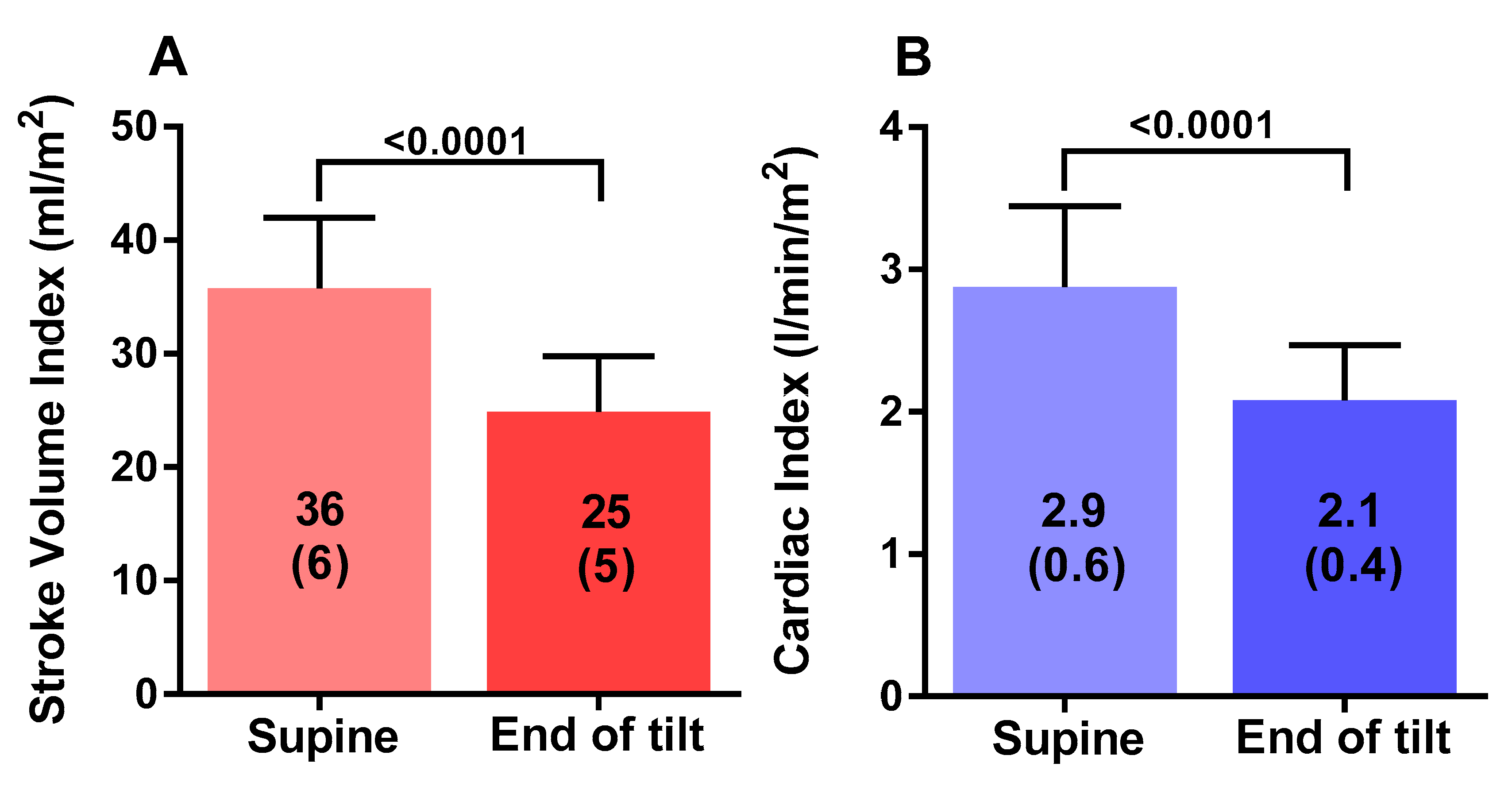
| Stroke volume index (mL/m2) | 36 (6) | 25 (5) | <0.0001 |
| Cardiac index (L/min/m2) | 2.9 (0.6) | 2.1 (0.4) | <0.0001 |
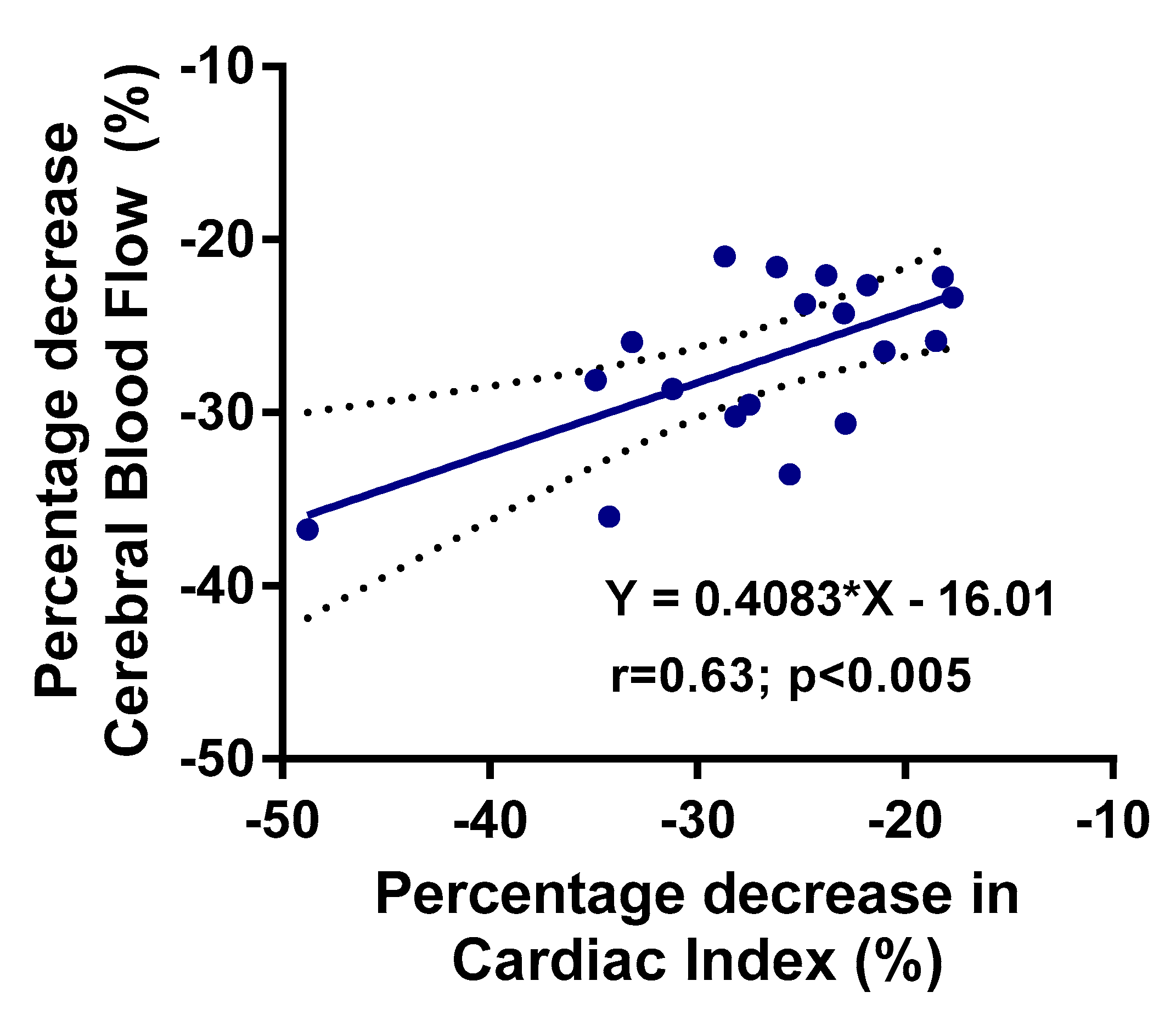
| Cerebral blood flow %change | −27 (5)% | ||
| Stroke volume index %change | −31 (8)% | ||
| Cardiac index %change | −27 (7)% | ||
| Group 1 Norm BPHR n = 15 | Group 2 POTS n = 4 | p-Value Group 1 vs. Group 2 | p-value Group 1 Supine vs. End Tilt | p-Value Group 2 Supine vs. End Tilt | |
|---|---|---|---|---|---|
| HR supine (bpm) | 80 (12) | 91 (10) | 0.14 | ||
| HR end-tilt (bpm) | 98 (21) | 126 (10) | 0.03 | 0.001 | 0.0002 |
| SBP supine (mmHg) | 135 (11) | 132 (7) | 0.63 | ||
| SBP end-tilt (mmHg) | 141 (13) | 126 (3) | 0.06 | 0.02 | 0.19 |
| DBP supine (mmHg) | 80 (10) | 80 (4) | 0.98 | ||
| DBP end-tilt (mmHg) | 87 (10) | 84 (3) | 0.57 | 0.002 | 0.05 |
| PetCO2 supine (mmHg) | 38 (3) | 38 (3) | 0.85 | ||
| PetCO2end-tilt (mmHg) | 30 (6) | 28 (6) | 0.57 | <0.0001 | 0.05 |
| CBF supine (mL/min) | 615 (71) | 632 (71) | 0.70 | ||
| CBF end-tilt (mL/min) | 452 (57) | 474 (67) | 0.54 | <0.0001 | <0.0001 |
| CBF end-tilt %change | −26 (5)% | −25 (2) | 0.69 | ||
| SVI supine (mL/m2) | 36 (5) | 36 (12) | 0.95 | ||
| SVI end-tilt (mL/m2) | 25 (4) | 23 (8) | 0.54 | <0.0001 | 0.01 |
| SVI end tilt %change | −30 (8)% | −35 (7)% | 0.27 | ||
| CI supine (L/min/m2) | 2.8 (0.5) | 3.2(0.8) | 0.17 | ||
| CI end tilt (L/min/m2) | 2.0 (0.3) | 2.4 (0.6) | 0.08 | <0.0001 | 0.01 |
| CI end tilt %change | −27 (8)% | −26 (6) | 0.72 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Campen, C.M.C.; Rowe, P.C.; Visser, F.C. Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing. Healthcare 2020, 8, 169. https://doi.org/10.3390/healthcare8020169
van Campen CMC, Rowe PC, Visser FC. Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing. Healthcare. 2020; 8(2):169. https://doi.org/10.3390/healthcare8020169
Chicago/Turabian Stylevan Campen, C (Linda) M.C., Peter C. Rowe, and Frans C. Visser. 2020. "Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing" Healthcare 8, no. 2: 169. https://doi.org/10.3390/healthcare8020169
APA Stylevan Campen, C. M. C., Rowe, P. C., & Visser, F. C. (2020). Cerebral Blood Flow Is Reduced in Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients During Mild Orthostatic Stress Testing: An Exploratory Study at 20 Degrees of Head-Up Tilt Testing. Healthcare, 8(2), 169. https://doi.org/10.3390/healthcare8020169