An Economic Evaluation Framework for Government-Funded Home Adaptation Schemes: A Quantitative Approach



Abstract
:1. Introduction
- (i)
- How can we better measure the efficiency of these funding schemes?
- (ii)
- How can we improve the efficiency of these funding schemes?
2. Materials and Methods
2.1. Design
2.2. Methods
- Efficiency: if the inputs are minimized;
- Effectiveness: if the outcomes are maximized;
- Equality: if recipients have equal opportunities;
- Ethics: if ethical issues are handled properly.
2.3. Analysis
- Quantifiability—the indicators must be measurable using some quantitative metric.
- Commensurability—the indicators must be used across all ILA schemes.
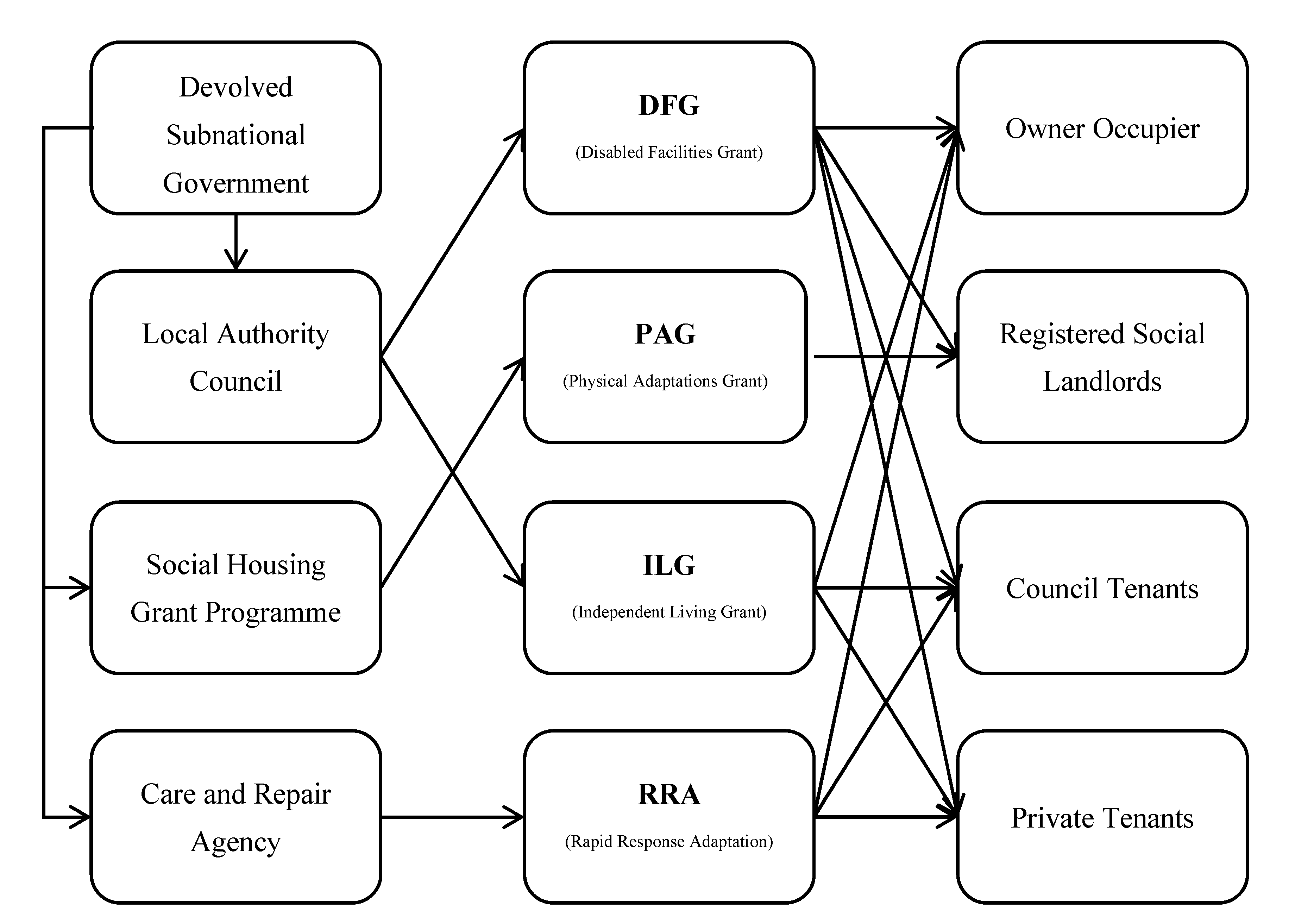
- which type of adaptation is provided (details described in Appendix A);
- which ILA scheme it belongs to (e.g., DFG, PAG);
- which delivery method is used;
- which structure is used;
- other relevant factors related to the provision.
- aggregate characteristics including economic development, institutional environment and other region-specific factors;
- individual characteristics including age, gender, race, disability type, family, etc.
2.4. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
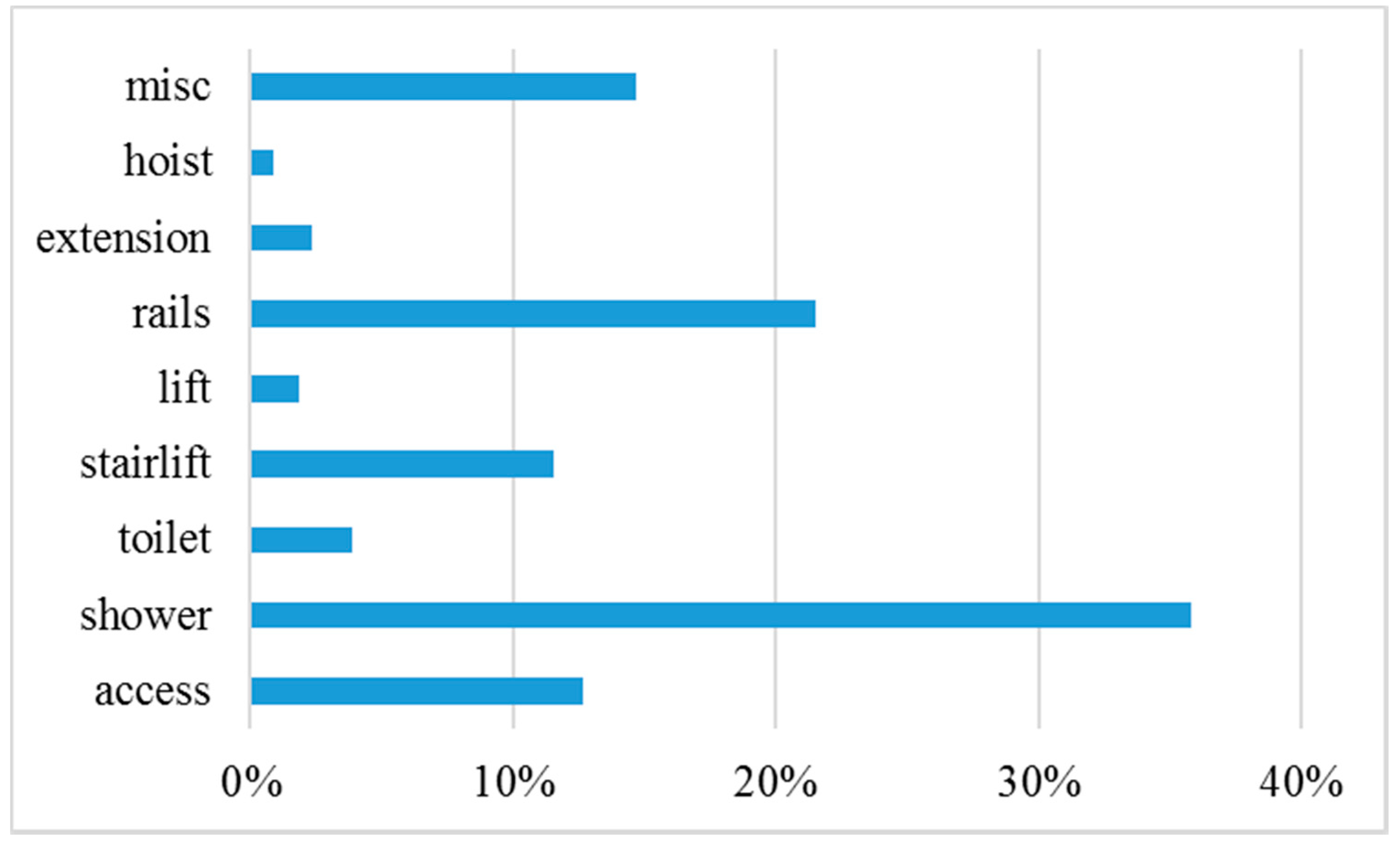
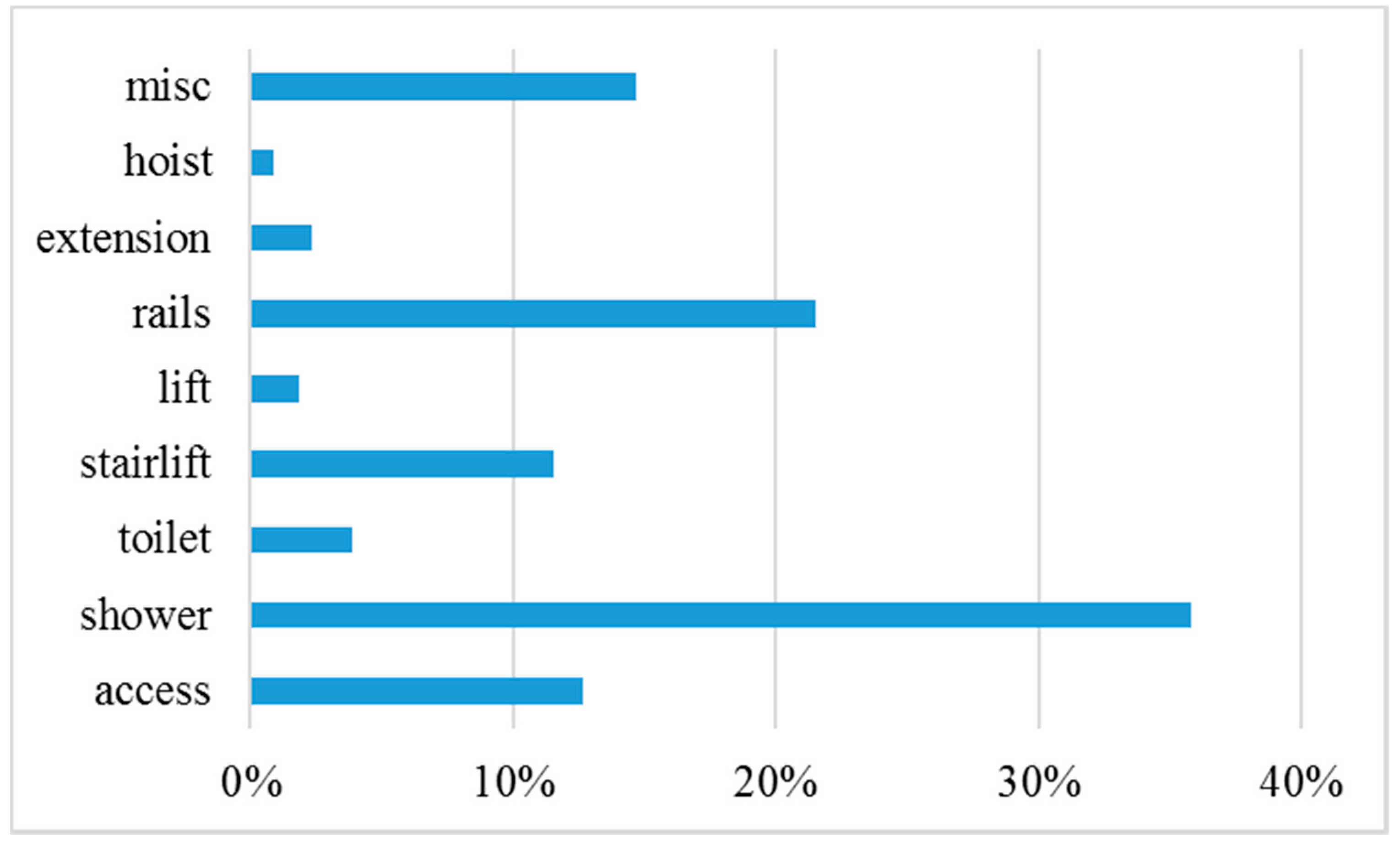
- “Access” refers to access adaptations such as ramps, gates, paths, the creation of steps and so forth.
- “Shower” refers to major adaptations related to the shower (thus excluding trivial things such as fixing shower doors). These are mostly composed of level access showers.
- “Toilet” refers to toilet adaptations, such as the installation of ground floor toilets and clos-o-mats.
- “Stairlift” refers to stair lifts, whilst other types of lifts are recorded more generally under lift.
- “Lift” simply refers to lifts for general use.
- “Rails” simply refers to grabrails, handrails and so forth.
- “Extension” refers to major extension work done to the residence. These are usually very high cost adaptations.
- “Hoist” refers to hoists, most commonly ceiling track hoists.
- “Misc” is an indicator of other adaptations works other than those listed. It is a binary variable indicating the presence of other adaptations or not.
References
- ONS. Disability in England and Wales, 2011 and Comparison with 2001. 2013. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/disability/articles/disabilityinenglandandwales/2013-01-30 (accessed on 17 September 2020).
- WHO. Disability and Health. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 17 September 2020).
- ONS. Living Longer. 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/livinglongerhowourpopulationischangingandwhyitmatters/2018-08-13 (accessed on 17 September 2020).
- Kendrick, D.; Kumar, A.; Carpenter, H.; Zijlstra, G.; Skelton, D.; Cook, J.; Stevens, Z.; Belcher, C.; Haworth, D.; Gawler, S.J.; et al. Exercise for Reducing Fear of Falling in Older People Living in the Community. Cochrane Database Syst. Rev. 2014, 11, CD009848. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, M.; Maiana, M.; Rafael, T.; Cláudia, F.; Maia, H.; Almeida, L.; Filho, J.; Pinto, E. External Validation of the Recurrent Falls Risk Scale in Community-Dwelling Stroke Individuals. J. Stroke Cerebrovasc. Dis. 2020, 29, 1049–1085. [Google Scholar]
- Xu, T.; Clemson, L.; O’Loughlin, K.; Lannin, N.; Dean, C.; Koh, G. Risk Factors for Falls in Community Stroke Survivors: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 563–573. [Google Scholar] [CrossRef]
- Wahl, H.W.; Fange, A.; Oswald, F.; Gitlin, L.N.; Iwarsson, S. The Home Environment and Disability-Related Outcomes in Aging Individuals: What Is the Empirical Evidence? Gerontologist 2009, 49, 355–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsson, G.; Nilsson, M.; Ekstam, L.; Chiatti, C.; Fange, A. Falls and Fear of Falling Among Persons Who Receive Housing Adaptations—Results From a Quasi-Experimental Study in Sweden. Healthcare 2017, 5, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewart, I.; Harty, C. Provision of Disability Adaptations to the Home: Analysis of Household Survey Data. Hous. Stud. 2015, 30, 901–923. [Google Scholar] [CrossRef]
- Kutty, N. Demand for Home Modifications: A Household Production Function Approach. Appl. Econ. 2010, 31, 1273–1281. [Google Scholar] [CrossRef]
- Evans, S.; Waller, S.; Bray, J.; Atkinson, T. Making Homes More Dementia-Friendly through the Use of Aids and Adaptations. Healthcare 2019, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.M.; Edmonston, B. Living Alone Among Older Adults in Canada and the U.S. Healthcare 2019, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Petersson, I.; Lilja, M.; Hammel, J.; Kottorp, A. Impact of Home Modification Services on Ability in Everyday Life for People Ageing with Disabilities. J. Rehabil. Med. 2008, 40, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Uppal, S. Demand for Home Modifications/Specialized Features: The Case of Disabled. Appl. Econ. 2007, 37, 1991–1999. [Google Scholar] [CrossRef]
- Pynoos, J.; Nishita, C. The Cost and Financing of Home Modifications in the United States. J. Disabil. Policy Stud. 2003, 14, 69–73. [Google Scholar] [CrossRef]
- Lilja, M.; Mansson, I.; Jahlenius, L.; Sacco-Peterson, M. Disability Policy in Sweden: Policies Concerning Assistive Technology and Home Modification Services. J. Disabil. Policy Stud. 2003, 14, 130–135. [Google Scholar] [CrossRef]
- Stark, S.; Keglovits, M.; Arbesman, M.; Lieberman, D. Effect of Home Modification Interventions on the Participation of Community-Dwelling Adults with Health Conditions: A Systematic Review. Am. J. Occup. Ther. 2017, 71, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, S.; Heywood, F. The Structural Neglect of Disabled Housing Association Tenants in England: Politics, Economics and Discourse. Hous. Stud. 2015, 30, 770–791. [Google Scholar] [CrossRef]
- Zhou, W.; Oyegoke, A.S.; Sun, M. Service Planning and Delivery Outcomes of Home Adaptations for Ageing in the UK. J. Hous. Built Environ. 2019, 34, 365–383. [Google Scholar] [CrossRef] [Green Version]
- Jones, C. Review of Housing Adaptations Including Disabled Facilities Grants—Wales; Welsh Government: Cardiff, Wales, UK, 2005.
- Welsh Government. Homes for Wales: A White Paper for Better Lives and Communities; Welsh Government: Cardiff, Wales, UK, 2012.
- National Assembly for Wales Equality of Opportunity Committee. Still Waiting: Home Maintenance and Adaptations Services for Older People in Wales; National Assembly for Wales: Cardiff, Wales, UK, 2009. [Google Scholar]
- National Assembly for Wales. Inquiry into Home Adaptations; National Assembly for Wales: Cardiff, Wales, UK, 2013. [Google Scholar]
- Bachrach, P.; Baratz, M. Two Faces of Power. Am. Political Sci. Rev. 1962, 56, 947–952. [Google Scholar] [CrossRef]
- Cobb, R.; Elder, C. Participation in American Politics: The Dynamics of Agenda-Building; Allyn and Bacon: Boston, MA, USA, 1972. [Google Scholar]
- Lukes, S. Power: A Radical View; Macmillan: London, UK, 1974. [Google Scholar]
- Lukes, S. Power: A Radical View, 2nd ed.; Palgrave Macmillan: Basingstoke, UK, 2005. [Google Scholar]
- Heywood, F. The Health Outcomes of Housing Adaptations. Disabil. Soc. 2004, 19, 129–143. [Google Scholar] [CrossRef]
- Heywood, F. Adaptation: Altering the House to Restore the Home. Hous. Stud. 2005, 20, 531–547. [Google Scholar] [CrossRef]
- Morris, S.; Devlin, N.; Parkin, D.; Spencer, A. Economic Analysis in Health Care, 2nd ed.; John Wiley & Sons Ltd.: Chichester, UK, 2012. [Google Scholar]
- Dudzinski, C.; Erekson, O.; Ziegert, A. Estimating a Hedonic Translog Cost Function for the Home Health Care Industry. Appl. Econ. 1998, 30, 1259–1267. [Google Scholar] [CrossRef]
- Boström, L.; Chiatti, C.; Thordardottir, B.; Ekstam, L.; Fange, A. Health-Related Quality of Life among People Applying for Housing Adaptations: Associated Factors. Int. J. Environ. Res. Public Health 2018, 15, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Lau, G.; Yu, M.; Brown, T.; Locke, C. Clients’ Perspectives of the Effectiveness of Home Modification Recommendations by Occupational Therapists. Occup. Ther. Health Care 2018, 32, 230–250. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.; Cummings, L.; Sixsmith, A.; Sixsmith, J. Impacts of Home Modifications on Aging-in-Place. J. Hous. Elder. 2011, 25, 246–257. [Google Scholar] [CrossRef]
- Tural, E.; Lu, D.; Cole, D. Factors Predicting Older Adults’ Attitudes Toward and Intentions to Use Stair Mobility Assistive Designs at Home. Prev. Med. Rep. 2020, 18, 1010–1082. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.; Sculpher, M.; Claxton, K. Health Opportunity Costs: Assessing the Implications of Uncertainty Using Elicitation Methods with Experts. Med. Decis. Mak. 2020, 40, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Cookson, R.; Mirelman, A.; Griffin, S.; Asaria, M.; Dawkins, B.; Norheim, O.; Verguet, S.; Culyer, A. Using Cost-Effectiveness Analysis to Address Health Equity Concerns. Value Health 2017, 20, 206–212. [Google Scholar] [CrossRef] [Green Version]
- Chiatti, C.; Iwarsson, S. Evaluation of Housing Adaptation Interventions: Integrating the Economic Perspective into Occupational Therapy Practice. Scand. J. Occup. 2014, 21, 323–333. [Google Scholar] [CrossRef] [Green Version]
- Curtis, L.; Beecham, J. A Survey of Local Authorities and Home Improvement Agencies: Identifying the Hidden Costs of Providing a Home Adaptations Service. Br. J. Occup. 2018, 81, 633–640. [Google Scholar] [CrossRef] [Green Version]
- Bibbings, J.; Boniface, G.; Campbell, J.; Findlay, G.; Reeves-McAll, E.; Zhang, M.; Zhou, P. A Review of Independent Living Adaptations; Welsh Government: Cardiff, Wales, UK, 2015.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Performance | Variable | Mean | Std. Dev. | 25% | Median | 75% |
|---|---|---|---|---|---|---|
| Money Input (in £) | Grant | 3887 | 5712 | 209 | 2549 | 4514 |
| Time Input (in days) | Total days | 177 | 152 | 65 | 143 | 257 |
| contact−approval | 87 | 96 | 15 | 54 | 132 | |
| approval−finish | 56 | 75 | 10 | 30 | 70 | |
| Outcome | Satisfaction | 9.74 | 0.94 | 10 | 10 | 10 |
| Regressor | Log Money Cost (in £) | ||
|---|---|---|---|
| OLS | Huber−White | Robust Reg | |
| access | 0.560 *** | 0.560 ** | 0.643 *** |
| shower | 0.811 *** | 0.811 ** | 0.838 *** |
| lift | 0.718 *** | 0.718 | 0.783 *** |
| rails | −1.131 *** | −1.131 * | −1.306 *** |
| stairlift | 0.510 *** | 0.510 * | 0.471 *** |
| toilet | −0.018 | −0.018 | −0.004 |
| extension | 1.828 *** | 1.828 *** | 1.888 *** |
| hoist | 0.524 ** | 0.524 *** | 0.533 ** |
| misc | −0.833 *** | −0.833 | −1.144 *** |
| PAG | −1.734 *** | −1.734 *** | −1.480 *** |
| Cadwyn | −0.086 | −0.086 | 0.086 |
| Caerphilly | −0.706 *** | −0.706 *** | −0.676 *** |
| Glamorgan | 0.117 | 0.117 * | 0.095 |
| Merthyr | 0.000 | 0.000 | 0.000 |
| Newport | −0.389 *** | −0.389 *** | −0.401 *** |
| Neath & PT | 0.000 | 0.000 | 0.000 |
| Pembroke | −2.471 *** | −2.471 *** | −2.307 *** |
| Torfaen | 0.000 | 0.000 | 0.000 |
| constant | 8.111 *** | 8.111 *** | 8.069 *** |
| observations | 3670 | 3670 | 3670 |
| R2 | 0.658 | 0.658 | 0.705 |
| R2 adjusted | 0.656 | 0.656 | 0.703 |
| Regressor | Input | Outcome | |
|---|---|---|---|
| Money Cost | Time Cost | Satisfaction | |
| access | 0.717 *** | 0.202 *** | −0.244 |
| shower | 0.838 *** | 0.052 | −0.051 |
| lift | 0.775 *** | −0.135 | 0.000 |
| rails | −1.545 *** | −0.346 *** | 0.000 |
| stairlift | 0.441 *** | −0.005 | −0.137 |
| toilet | 0.140 * | 0.127 | 0.000 |
| extension | 2.066 *** | 1.243 *** | −0.18 |
| hoist | 0.553 *** | −0.012 | 0.000 |
| misc | −1.196 *** | 0.141 | 0.032 |
| PAGs | −0.952 *** | −1.203 *** | - |
| constant | 7.801 *** | 5.310 *** | 11.034 *** |
| money cost | - | - | −0.044 |
| time cost | - | - | −0.158 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, B.; Zhou, P. An Economic Evaluation Framework for Government-Funded Home Adaptation Schemes: A Quantitative Approach. Healthcare 2020, 8, 345. https://doi.org/10.3390/healthcare8030345
Zhang B, Zhou P. An Economic Evaluation Framework for Government-Funded Home Adaptation Schemes: A Quantitative Approach. Healthcare. 2020; 8(3):345. https://doi.org/10.3390/healthcare8030345
Chicago/Turabian StyleZhang, Bo, and Peng Zhou. 2020. "An Economic Evaluation Framework for Government-Funded Home Adaptation Schemes: A Quantitative Approach" Healthcare 8, no. 3: 345. https://doi.org/10.3390/healthcare8030345
APA StyleZhang, B., & Zhou, P. (2020). An Economic Evaluation Framework for Government-Funded Home Adaptation Schemes: A Quantitative Approach. Healthcare, 8(3), 345. https://doi.org/10.3390/healthcare8030345