Does Educational Attainment Affect Residents’ Health?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
2.1.1. Research on Influencing Factors of Health
2.1.2. Research on the Relationship between Education and Health
2.2. Data, Variables and Methods
2.2.1. Data Source
2.2.2. Variable Design
Dependent Variables
Independent Variables
Control Variables
2.2.3. Methods
3. Results
3.1. The Relationship between Education Level and Health
3.2. Discussion on the Issue of Selection Bias
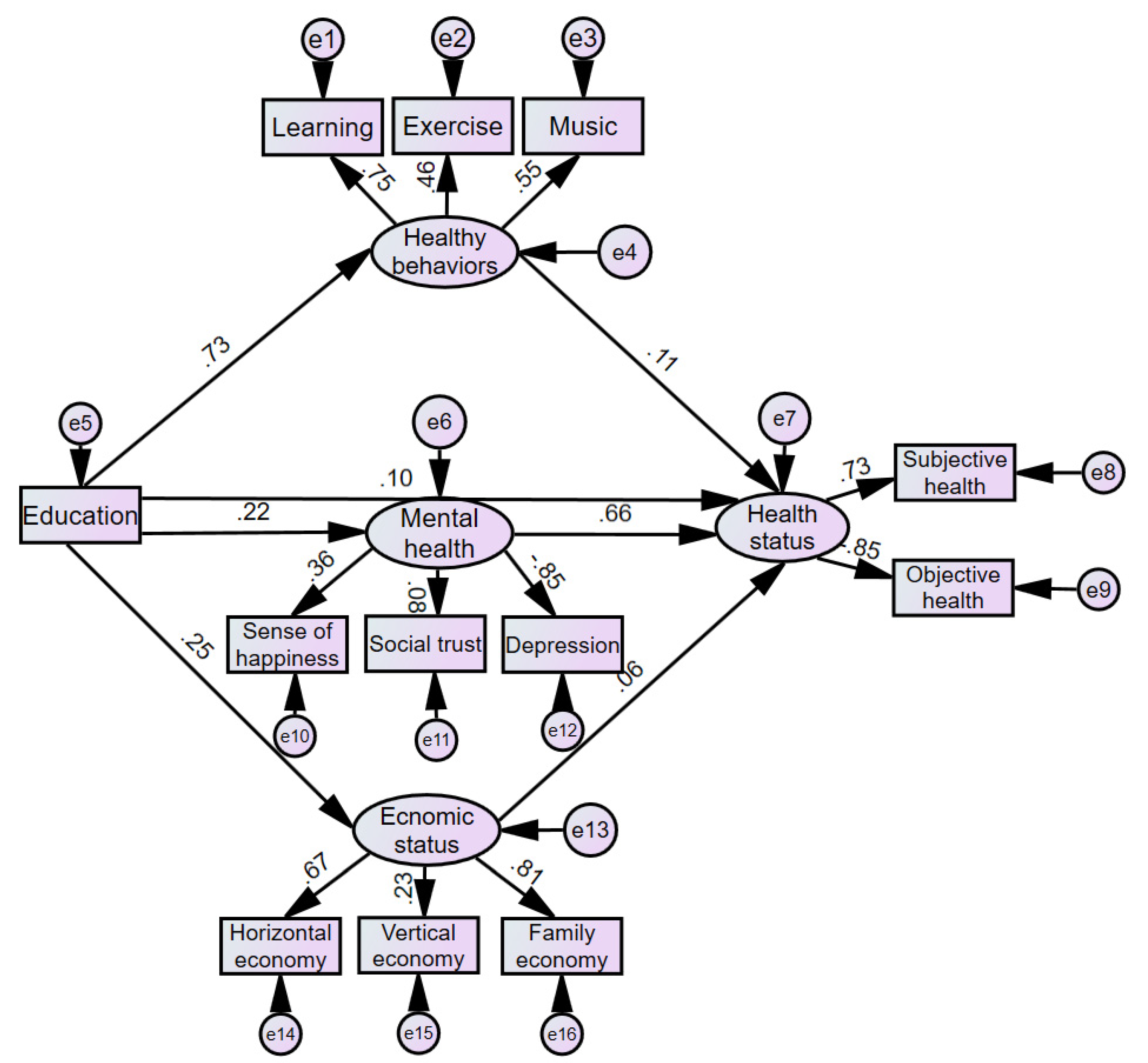
3.3. How Education Affects Health
3.4. Heterogeneity Analysis and Robustness Test
3.4.1. Heterogeneity Analysis of the Effect of Education on Health
Urban–Rural Differences in Education’s Effect on Health
Gender Differences in Education’s Effect on Health
Age Differences in Education’s Effect on Health
Regional Differences in Education’s Effect on Health
3.5. Robustness Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Akinkugbe, O.; Mohanoe, M. Public health expenditure as a determinant of health-status in Lesotho. Soc. Work Public Health 2009, 24, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Benzeval, M.; Judge, K.; Shouls, S. Understanding the Relationship between Income and Health: How Much can be Gleaned from Cross-Sectional Data. Soc. Policy Adm. 2001, 35, 376–396. [Google Scholar] [CrossRef]
- Ettner, S.L. New evidence on the relationship between income and health. J. Health Econ. 1996, 15, 67–68. [Google Scholar] [CrossRef]
- Folland, S. An economic model of social capital and health. Health Econ. Policy Law 2008, 3, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M. On the Concept of Health Capital and the Demand for Health. J. Polit. Econ. 1972, 80, 223–255. [Google Scholar] [CrossRef] [Green Version]
- Shindell, D.T.; Lee, Y.H.; Faluvegi, G. Climate and Health Impacts of US Emissions Reductions Consistent with 2 °C. Nat. Clim. Chang. 2016, 6, 503–507. [Google Scholar] [CrossRef]
- Yip, W.; Subramanian, S.V.; Mitchell, A.D.; Kawachi, I.; Lee, D.T.S.; Wang, J. Does Social Capital Enhance Health and Well-being? Evidence from Rural China. Soc. Sci. Med. 2007, 64, 35–49. [Google Scholar] [CrossRef]
- Côté-Sergent, A.; Raquel, F.; Erin, S. Comparing the education gradient in health deterioration among the elderly in six OECD countries. Health Policy 2020, 124, 326–335. [Google Scholar] [CrossRef]
- Opinions on the Implementation of Healthy China Strategy issued by the State Council. Available online: http://www.gov.cn/zhengce/content/2019-07/15/content_5409492.htm (accessed on 26 March 2020).
- Sepehri, A.; Simpson, W.; Sarma, S. The influence of health insurance on hospital admission and length of stay—The case of Vietnam. Soc. Sci. Med. 2006, 63, 1757–1770. [Google Scholar] [CrossRef]
- Preston, S.H. The changing relation between mortality and level of economic development. Popul. Stud. 1975, 29, 231–248. [Google Scholar] [CrossRef]
- Grossman, M. The Correlation between Health and Schooling; NBER Working Paper Series; National Bureau of Economic Research: Cambridge, MA, USA, 1973. [Google Scholar]
- Grossman, M. The Human Capital Model of the Demand for Health; NBER Working Paper Series; National Bureau of Economic Research: Cambridge, MA, USA, 1999. [Google Scholar]
- Lleras-Muney, A. The Relationship between Education and Adult Mortality in the United States. Rev. Econ. Stud. 2005, 72, 189–221. [Google Scholar]
- Kennedy, B.P.; Kawachi, I.; Glass, R.; Prothrow-Stith, D. Income Distribution, Socioeconomic Status, and Self Rate Health in the United States: Multilevel Analysis. Br. Med. J. 1998, 317, 917–921. [Google Scholar]
- Kennedy, B.P.; Kawachi, I.; Prothrow-Stith, D. Income distribution and mortality: Cross sectional ecological study of the Robin Hood index in the United States. Br. Med. J. 1996, 312, 1004–1007. [Google Scholar]
- Wilkinson, R.G. Income Distribution and Mortality: ‘A Natural Experiment’. Sociol. Health Illn. 1990, 12, 391–412. [Google Scholar]
- Wilkinson, R.G.; Kawachi, I.; Kennedy, B.P. Mortality, the Social Environment, Crime and Violence. Sociol. Health Illn. 1998, 20, 578–597. [Google Scholar]
- Pappas, G.; Queen, S.; Hadden, W.; Fisher, G. The Increasing Disparity in Mortality between Socioeconomic Groups in the United States, 1960 and 1986. N. Engl. J. Med. 1993, 329, 103–109. [Google Scholar]
- Bidani, B.; Ravallion, M. Decomposing social indicators using distributional data. J. Econom. 1997, 77, 125–139. [Google Scholar]
- Flegg, A.T. Inequality of Income, Illiteracy and Medical Care as Determinants of Infant Mortality in Underdeveloped Countries. Popul. Stud. 1982, 36, 441–458. [Google Scholar]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar]
- Lindstr, M.; Moghaddassi, M.; Merlo, J. Individual self-reported health, social participation and neighborhood: A multilevel analysis in Malmö, Sweden. Prev. Med. 2004, 39, 135–141. [Google Scholar]
- Franzini, L.; Spears, W. Contributions of social context to inequalities in years of life lost to heart disease in Texas, USA. Soc. Sci. Med. 2003, 57, 1847–1861. [Google Scholar] [CrossRef]
- Silles, M. The Causal Effect of Education on Health: Evidence from the United Kingdom. Econ. Educ. Rev. 2009, 28, 122–128. [Google Scholar] [CrossRef]
- Curry, G.D. The Impact of Educational Attainment on Black Women’s Obesity Rate in the United States. J. Racial Ethn. Health Disparit. 2020, 7, 345–354. [Google Scholar] [PubMed] [Green Version]
- Kye, B.; Arenas, E.; Teruel, G.; Rubalcava, L. Education, elderly health, and differential population aging in South Korea: A demographic approach. Demogr. Res. 2014, 30, 753–794. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.G.; Zhang, Y.; Shen, K. How does education affect people’s health? Evidence from the elderly in China. Econ. Q. 2014, 14, 305–330. [Google Scholar]
- Ye, X.M.; Liang, W.Y. Research on the effect mechanism of education on the health of the elderly in China—Evidence from CLHLS in 2011. Educ. Econ. 2017, 33, 68–76. [Google Scholar]
- Willis, R. Wage Determinants: A Survey and Reinterpretation of Human Capital Earnings Functions. Handb. Labor Econ. 1986, 1, 525–602. [Google Scholar]
- Moen, E.R. Education, Ranking, and Competition for Jobs. J. Labor Econ. 1999, 17, 694–723. [Google Scholar] [CrossRef]
- Goldman, D.P.; Smith, J.P. Can Patient Self-Management Help Explain the SES Health Gradient? Proc. Natl. Acad. Sci. USA 2002, 99, 10929–10934. [Google Scholar]
- Clark, D.; Royer, H. The Effect of Education on Adult Health and Mortality: Evidence from Britain. Am. Econ. Rev. 2013, 103, 2087–2120. [Google Scholar]
- Meghir, C.; Palme, M.; Simeonova, E. Education and mortality: Evidence from a social experiment. Am. Econ. J. Appl. Econ. 2018, 10, 234–256. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, S.V.; Subramanyam, M.A.; Selvaraj, S.; Kawachi, I. Are Self Reports of Health and Morbidities in Developing Countries Misleading? Evidence from India. Soc. Sci. Med. 2009, 68, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Shea, S.; Stein, D.A.; Basch, C.E.; Freudenheim, J.; Lantigua, R.; Maylahn, C.; Strogatz, D.S.; Novick, L. Independent Associations of Educational Attainment and Ethnicity with Behavioral Risk Factors for Cardiovascular Disease. Am. J. Epidemiol. 1991, 134, 567–582. [Google Scholar] [CrossRef]
- Hu, A.N. Can education make us healthier: A comparative analysis of urban and rural areas based on the 2010 China Comprehensive Social Survey. Soc. Sci. China 2015, 36, 64–82. [Google Scholar]
- Knight, J.; Gunatilaka, R. Great Expectations? The subjective well-being of rural-urban migrants in China. World Dev. 2010, 38, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Mirowsky, J.; Ross, C.E. Education, cumulative advantage, and health. Aging Int. 2005, 30, 27–62. [Google Scholar] [CrossRef]
- Currie, J.; Moretti, E. Mother’s Education and the Intergenerational Transmission of Human Capital: Evidence from College Openings. Q. J. Econ. 2003, 118, 1495–1532. [Google Scholar] [CrossRef]
- Case, A.; Lubotsky, D.; Paxson, C. Economic status and health in childhood: The origins of the gradient. Am. Econ. Rev. 2002, 92, 1308–1334. [Google Scholar] [CrossRef] [Green Version]
- Ryff, C.D.; Singer, B.H. Social environments and the genetics of aging: Advancing knowledge of protective health mechanisms. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, 12–23. [Google Scholar] [CrossRef]
- Cunha, F.; Heckman, J. The technology of skill formation. Am. Econ. Rev. 2007, 97, 31–47. [Google Scholar] [CrossRef] [Green Version]
- Perri, T.J. Health Status and Schooling Decisions of Young Men. Econ. Educ. Rev. 1984, 3, 207–213. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Wu, M.L. Structural Equation Model—Operation and Application of AMOS; Chongqing University Press: Chongqing, China, 2015. [Google Scholar]
- Kenkel, D.S. Health Behavior, Health Knowledge, and Schooling. J. Polit. Econ. 1991, 99, 287–305. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Gender and the Health Benefits of Education. Sociol. Q. 2010, 51, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.P. Family Internalization and Intergenerational Sharing of Care Responsibilities: The Effect of Parents Living Together on Female Labor Participation. Popul. Res. 2019, 43, 78–89. [Google Scholar]
- Cebula, R.J.; Coombs, C.K. Recent Evidence on Factors Influencing the Female Labor Force Participation Rate. J. Labor Res. 2008, 29, 272–284. [Google Scholar] [CrossRef]
- Fang, C.L. Botai Line—Important Function and Construction Conception of China’s Regional Development Equilibrium Line. Acta Geogr. Sin. 2020, 75, 2221–2225. [Google Scholar]
- Long, C.; Han, J.; Liu, Y. Has Rural-Urban Migration Promoted the Health of Chinese Migrant Workers? Int. J. Environ. Res. Public Health 2020, 17, 1218. [Google Scholar] [CrossRef] [Green Version]
- Bowles, S.; Gintis, H.; Osborne, M. The determinants of earnings: A behavioral approach. J. Econ. Lit. 2001, 39, 1137–1176. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variable Type | Variable Name | Sample Size | Mean | Standard Deviation | Min | Max |
|---|---|---|---|---|---|---|
| Dependent variable | Self-reported health | 8680 | 3.739 | 1.010 | 1 | 5 |
| Frequency of health effects on work | 8680 | 2.019 | 0.978 | 1 | 5 | |
| Independent variable | Respondent’s education level | 8680 | 3.253 | 1.451 | 1 | 7 |
| Control variable | Gender | 8680 | 0.478 | 0.500 | 0 | 1 |
| Age | 8680 | 55.254 | 21.207 | 22 | 115 | |
| Ethnicity | 8680 | 0.924 | 0.265 | 0 | 1 | |
| Political identity | 8680 | 0.109 | 0.311 | 0 | 1 | |
| Marital status | 8680 | 0.791 | 0.406 | 0 | 1 | |
| Father’s education level | 8680 | 2.719 | 1.788 | 1 | 9 | |
| Mother’s education level | 8680 | 2.174 | 1.578 | 1 | 9 | |
| Province dummy variable | 28 | 0 | 1 | |||
| Channel variable | Frequency of exercise | 8680 | 2.518 | 1.517 | 1 | 5 |
| Frequency of learning | 8680 | 2.035 | 1.095 | 1 | 5 | |
| Frequency of listening to music | 8680 | 2.503 | 1.481 | 1 | 5 | |
| Happiness | 8680 | 3.885 | 0.795 | 1 | 5 | |
| Frequency of depression | 8680 | 2.110 | 0.893 | 1 | 5 | |
| Social trust | 8680 | 3.470 | 0.959 | 1 | 5 | |
| Horizontal economic status | 8680 | 1.733 | 0.542 | 1 | 3 | |
| Vertical economic status | 8680 | 2.264 | 0.617 | 1 | 3 | |
| Family economic status | 8680 | 2.695 | 0.698 | 1 | 5 | |
| Variables | Health Evaluation | Frequency of Health Effects on Work | ||||
|---|---|---|---|---|---|---|
| Model1 | Model2 | Model3 | Model4 | Model5 | Model6 | |
| Education level | 0.184 *** | 0.133 *** | 0.102 *** | −0.128 *** | −0.127 *** | −0.096 *** |
| (0.007) | (0.008) | (0.010) | (0.005) | (0.008) | (0.010) | |
| Age | −0.008 *** | −0.007 *** | 0.008 *** | 0.007 *** | ||
| (0.001) | (0.001) | (0.001) | (0.001) | |||
| Ethnicity | −0.025 | −0.020 | −0.022 | −0.028 | ||
| (0.047) | (0.047) | (0.048) | (0.047) | |||
| Gender | 0.107 *** | 0.118 *** | −0.106 *** | −0.117 *** | ||
| (0.021) | (0.021) | (0.020) | (0.020) | |||
| Political identity | −0.043 | −0.033 | 0.044 | 0.035 | ||
| (0.034) | (0.034) | (0.034) | (0.034) | |||
| Marital status | −0.000 | 0.019 | −0.013 | −0.032 | ||
| (0.025) | (0.026) | (0.024) | (0.024) | |||
| Father’s education | 0.027 *** | −0.027 *** | ||||
| (0.008) | (0.008) | |||||
| Mother’s education | 0.033 *** | −0.031 *** | ||||
| (0.010) | (0.009) | |||||
| Province | Yes | Yes | Yes | Yes | Yes | Yes |
| Observations | 8680 | 8680 | 8680 | 8680 | 8680 | 8680 |
| R-squared | 0.101 | 0.129 | 0.133 | 0.102 | 0.128 | 0.133 |
| Dependent Variable | Matching Method | Average Treatment Effect | Standard Error | t-Test |
|---|---|---|---|---|
| K-nearest neighbor matching (K = 4) | 0.196 *** | 0.071 | 2.75 | |
| Self-Reported Health | Caliper matching (Cal = 0.05) | 0.220 *** | 0.056 | 3.97 |
| Nearest neighbor matching within caliper (K = 4 Cal = 0.05) | 0.196 *** | 0.071 | 2.75 | |
| Kernel matching Average value | 0.224 *** 0.209 | 0.056 | 3.99 | |
| The Frequency of Health Effects on Work | K-nearest neighbor matching (K = 4) | −0.201 *** | 0.069 | −2.90 |
| Caliper matching (Cal = 0.05) | −0.218 *** | 0.053 | −4.07 | |
| Nearest neighbor matching within caliper (K = 4 Cal = 0.05) | −0.201 *** | 0.069 | −2.90 | |
| Kernel matching Average value | −0.217 *** −0.209 | 0.054 | −4.01 |
| Variable | K-Nearest Neighbor Matching | Caliper Matching | Nearest Neighbor Matching within Caliper | Kernel Matching |
|---|---|---|---|---|
| Age | −75.5 (−5.3) | −75.5 (−11.2) | −75.5 (−5.3) | −75.5 (−10.8) |
| Political status | 38.1 (17.9) | 38.1 (17.4) | 38.1 (17.9) | 38.1 (17.1) |
| Gender | 28.0 (−5.5) | 28.0 (−0.9) | 28.0 (−5.5) | 28.0 (−1.1) |
| Ethnicity | 13.8 (−4.8) | 13.8 (−0.8) | 13.8 (−4.8) | 13.8 (−1.3) |
| Marital status | −16.6 (−18.5) | −16.6 (−19.8) | −16.6 (−18.5) | −16.6 (−19.6) |
| Father’s education | 109.8 (−4.4) | 109.8 (5.0) | 109.8 (−4.4) | 109.8 (4.2) |
| Mother’s education | 106.8 (−4.5) | 106.8 (7.9) | 106.8 (−4.5) | 106.8 (6.3) |
| Indicator Type | Index | Critical Value | Model Result | Whether the Results Meet Requirement |
|---|---|---|---|---|
| Absolute fit index | RMSEA | ≤0.08 | 0.067 | Yes |
| GFI | >0.9 | 0.963 | Yes | |
| AGFI | >0.9 | 0.940 | Yes | |
| Relative fit index | NFI | >0.9 | 0.911 | Yes |
| IFI | >0.9 | 0.913 | Yes | |
| CFI | >0.9 | 0.913 | Yes | |
| Simple fit index | PGFI | >0.5 | 0.593 | Yes |
| PNFI | >0.5 | 0.662 | Yes | |
| PCFI | >0.5 | 0.664 | Yes | |
| CMIN/DF | <2 | 39.722 | No |
| Paths between Variables | Estimation | C.R. | Standard Errors | |||||
|---|---|---|---|---|---|---|---|---|
| Unstandardized Coefficient | Standardized Coefficient | |||||||
| Health status | ← | Education | 0.050 | *** | 0.099 | *** | 5.042 | 0.010 |
| Economic status | ← | Education | 0.063 | *** | 0.253 | *** | 17.698 | 0.004 |
| Healthy behavior | ← | Education | 0.414 | *** | 0.729 | *** | 61.583 | 0.007 |
| Mental health | ← | Education | 0.042 | *** | 0.216 | *** | 13.932 | 0.003 |
| Health status | ← | Economic status | 0.114 | *** | 0.056 | *** | 4.599 | 0.025 |
| Health status | ← | Healthy behavior | 0.102 | *** | 0.114 | *** | 5.390 | 0.019 |
| Health status | ← | Mental health | 1.711 | *** | 0.656 | *** | 25.075 | 0.068 |
| Exercise | ← | Healthy behavior | 0.846 | *** | 0.459 | *** | 35.353 | 0.024 |
| Learning | ← | Healthy behavior | 1.000 | 0.751 | ||||
| Listening to music | ← | Healthy behavior | 0.988 | *** | 0.549 | *** | 41.155 | 0.024 |
| Social trust | ← | Mental health | 0.282 | *** | 0.083 | *** | 6.655 | 0.042 |
| Depression | ← | Mental health | −2.677 | *** | −0.847 | *** | −21.721 | 0.123 |
| Sense of happiness | ← | Mental health | 1.000 | 0.356 | ||||
| Horizontal economy | ← | Economic status | 1.000 | 0.668 | ||||
| Vertical economy | ← | Economic status | 0.392 | *** | 0.230 | *** | 17.775 | 0.022 |
| Family economy | ← | Economic status | 1.566 | *** | 0.812 | *** | 23.734 | 0.066 |
| Health evaluation | ← | Health status | 1.000 | 0.734 | ||||
| Work affected by health | ← | Health status | −1.117 | *** | −0.847 | *** | −53.611 | 0.021 |
| Variables | Self-Reported Health | The Frequency of Health Effects on Work | ||||
|---|---|---|---|---|---|---|
| Urban and Rural | Urban | Rural | Urban and Rural | Urban | Rural | |
| Education | 0.043 *** | 0.033 *** | 0.080 *** | −0.050 *** | −0.022 | −0.079 *** |
| (0.010) | (0.014) | (0.015) | (0.010) | (0.014) | (0.013) | |
| Individual variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Channel variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Province | Yes | Yes | Yes | Yes | Yes | Yes |
| Sample size | 8055 | 3282 | 4773 | 8055 | 3282 | 4773 |
| R-squared | 0.289 | 0.264 | 0.322 | 0.343 | 0.282 | 0.380 |
| Variables | Self-Reported Health | The Frequency of Health Effects on Work | ||||
|---|---|---|---|---|---|---|
| All | Female | Male | All | Female | Male | |
| Education | 0.047 *** | 0.056 *** | 0.032 ** | −0.053 *** | −0.055 *** | −0.048 *** |
| (0.010) | (0.013) | (0.014) | (0.009) | (0.013) | (0.013) | |
| Individual variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Channel variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Province | Yes | Yes | Yes | Yes | Yes | Yes |
| Sample size | 8680 | 4534 | 4146 | 8680 | 4534 | 4146 |
| R-squared | 0.287 | 0.313 | 0.259 | 0.342 | 0.376 | 0.306 |
| Variables | Self-Reported Health | The Frequency of Health Effects on Work | ||||
|---|---|---|---|---|---|---|
| ≤39 Years Old | 40–59 Years Old | ≥60 Years Old | ≤39 Years Old | 40–59 Years Old | ≥60 Years Old | |
| Education | −0.017 | 0.034 ** | 0.027 * | −0.011 | −0.049 *** | −0.045 *** |
| (0.017) | (0.017) | (0.016) | (0.014) | (0.016) | (0.016) | |
| Individual variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Channel variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Province | Yes | Yes | Yes | Yes | Yes | Yes |
| Sample size | 2090 | 3379 | 3211 | 2090 | 3379 | 3211 |
| R-squared | 0.197 | 0.273 | 0.259 | 0.215 | 0.329 | 0.334 |
| Variables | Self-Reported Health | The Frequency of Health Effects on Work | ||||
|---|---|---|---|---|---|---|
| Eastern Area | Central Area | Western Area | Eastern Area | Central Area | Western Area | |
| Education | 0.004 | 0.067 *** | 0.079 *** | −0.049 *** | −0.047 *** | −0.055 *** |
| (0.013) | (0.019) | (0.021) | (0.012) | (0.018) | (0.019) | |
| Individual variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Channel variables | Yes | Yes | Yes | Yes | Yes | Yes |
| Sample size | 4329 | 2255 | 2096 | 4329 | 2255 | 2096 |
| R-squared | 0.219 | 0.301 | 0.312 | 0.277 | 0.354 | 0.386 |
| Dependent Variables | Group 1 | Group 2 | Group 3 | Group 4 | ||||
|---|---|---|---|---|---|---|---|---|
| 1 vs. 2, 3, 4, 5 | 1, 2 vs. 3, 4, 5 | 1, 2, 3 vs. 4, 5 | 1, 2, 3, 4 vs. 5 | |||||
| Subjective Health | Objective Health | Subjective Health | Objective Health | Subjective Health | Objective Health | Subjective Health | Objective Health | |
| Education | 0.106 | −0.134 *** | 0.210 *** | −0.183 *** | 0.092 *** | −0.162 *** | −0.028 | −0.010 |
| (0.122) | (0.033) | (0.049) | (0.039) | (0.033) | (0.060) | (0.035) | (0.139) | |
| Age | −0.013 *** | 0.012 *** | −0.014 *** | 0.013 *** | −0.015 *** | 0.016 *** | −0.019 *** | 0.021 *** |
| (0.005) | (0.001) | (0.002) | (0.001) | (0.001) | (0.002) | (0.002) | (0.005) | |
| Gender | 0.235 | 0.054 | 0.012 | 0.137 | -0.118 | −0.077 | 0.178 * | −0.210 |
| (0.261) | (0.098) | (0.121) | (0.105) | (0.094) | (0.141) | (0.107) | (0.302) | |
| Ethnicity | 0.142 | −0.169 *** | 0.138 * | −0.212 *** | 0.231 *** | −0.106 | 0.137 ** | 0.214 |
| (0.173) | (0.052) | (0.071) | (0.058) | (0.051) | (0.087) | (0.055) | (0.204) | |
| Political identity | −0.488 | 0.034 | −0.250 * | 0.274 *** | −0.363 *** | 0.273 * | −0.025 | 0.208 |
| (0.308) | (0.085) | (0.132) | (0.100) | (0.087) | (0.159) | (0.091) | (0.376) | |
| Marital status | 0.033 | −0.018 | −0.096 | 0.104 | −0.052 | 0.280 ** | −0.145 ** | 0.133 |
| (0.205) | (0.066) | (0.090) | (0.075) | (0.065) | (0.114) | (0.069) | (0.262) | |
| Father’s education | 0.074 | −0.079 *** | 0.022 | −0.035 | −0.001 | 0.024 | 0.040 * | −0.031 |
| (0.072) | (0.021) | (0.031) | (0.025) | (0.021) | (0.036) | (0.022) | (0.090) | |
| Mother’s education | 0.025 | −0.048 ** | 0.109 *** | −0.088 *** | 0.068 *** | −0.198 *** | 0.008 | −0.339 ** |
| (0.081) | (0.023) | (0.039) | (0.030) | (0.025) | (0.050) | (0.024) | (0.142) | |
| Horizontal economic status | −0.082 | 0.060 | 0.214 *** | −0.117 * | 0.175 *** | −0.323 *** | −0.006 | −0.021 |
| (0.189) | (0.057) | (0.074) | (0.063) | (0.055) | (0.093) | (0.061) | (0.216) | |
| Vertical economic status | 0.321 ** | 0.019 | −0.070 | 0.012 | 0.096 ** | 0.104 | 0.071 | 0.082 |
| (0.125) | (0.043) | (0.056) | (0.047) | (0.042) | (0.068) | (0.045) | (0.144) | |
| Family economic status | 0.215 | 0.085 * | 0.211 *** | −0.129 ** | 0.220 *** | −0.198 *** | 0.137 *** | −0.168 |
| (0.143) | (0.045) | (0.059) | (0.051) | (0.044) | (0.074) | (0.048) | (0.160) | |
| Exercise | 0.056 | 0.023 | 0.004 | 0.004 | −0.042 ** | 0.006 | −0.028 | −0.083 |
| (0.063) | (0.019) | (0.025) | (0.021) | (0.018) | (0.031) | (0.020) | (0.071) | |
| Learning | 0.138 | 0.019 | 0.151 *** | −0.025 | 0.118 *** | −0.104 * | 0.077 ** | −0.135 |
| (0.107) | (0.029) | (0.044) | (0.036) | (0.030) | (0.055) | (0.031) | (0.123) | |
| Listening to music | −0.013 | −0.104 *** | 0.040 | −0.071 *** | 0.037 * | 0.006 | 0.050 ** | 0.049 |
| (0.067) | (0.020) | (0.028) | (0.024) | (0.020) | (0.036) | (0.021) | (0.079) | |
| Sense of happiness | 0.201 ** | −0.156 *** | 0.115 *** | −0.077 * | 0.189 *** | −0.009 | 0.385 *** | −0.219 ** |
| (0.091) | (0.038) | (0.044) | (0.040) | (0.036) | (0.053) | (0.043) | (0.103) | |
| Social trust | 0.119 | 0.064 ** | 0.080 ** | 0.038 | 0.020 | −0.013 | −0.056 * | 0.042 |
| (0.080) | (0.027) | (0.036) | (0.031) | (0.027) | (0.044) | (0.029) | (0.094) | |
| Depression | −1.299 *** | 1.144 *** | −1.024 *** | 1.493 *** | −0.839 *** | 1.477 *** | −0.699 *** | 1.440 *** |
| (0.094) | (0.036) | (0.041) | (0.042) | (0.032) | (0.055) | (0.037) | (0.110) | |
| N | 8680 | 8680 | 8680 | 8680 | 8680 | 8680 | 8680 | 8680 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, C.; Liu, P.; Yi, C. Does Educational Attainment Affect Residents’ Health? Healthcare 2020, 8, 364. https://doi.org/10.3390/healthcare8040364
Long C, Liu P, Yi C. Does Educational Attainment Affect Residents’ Health? Healthcare. 2020; 8(4):364. https://doi.org/10.3390/healthcare8040364
Chicago/Turabian StyleLong, Cuihong, Pei Liu, and Chengzhi Yi. 2020. "Does Educational Attainment Affect Residents’ Health?" Healthcare 8, no. 4: 364. https://doi.org/10.3390/healthcare8040364
APA StyleLong, C., Liu, P., & Yi, C. (2020). Does Educational Attainment Affect Residents’ Health? Healthcare, 8(4), 364. https://doi.org/10.3390/healthcare8040364