A Lightweight Convolutional Neural Network Architecture Applied for Bone Metastasis Classification in Nuclear Medicine: A Case Study on Prostate Cancer Patients

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
- Decrease the number of free parameters.
- Achieve high classification accuracy with small datasets.
- Decrease the training time needed for convergence.
- Decrease the complexity of the network thus enabling its mobile application.
- Establish a future research direction that will extend the applicability of the method to other types of scintigraphy.
2. Materials and Methods
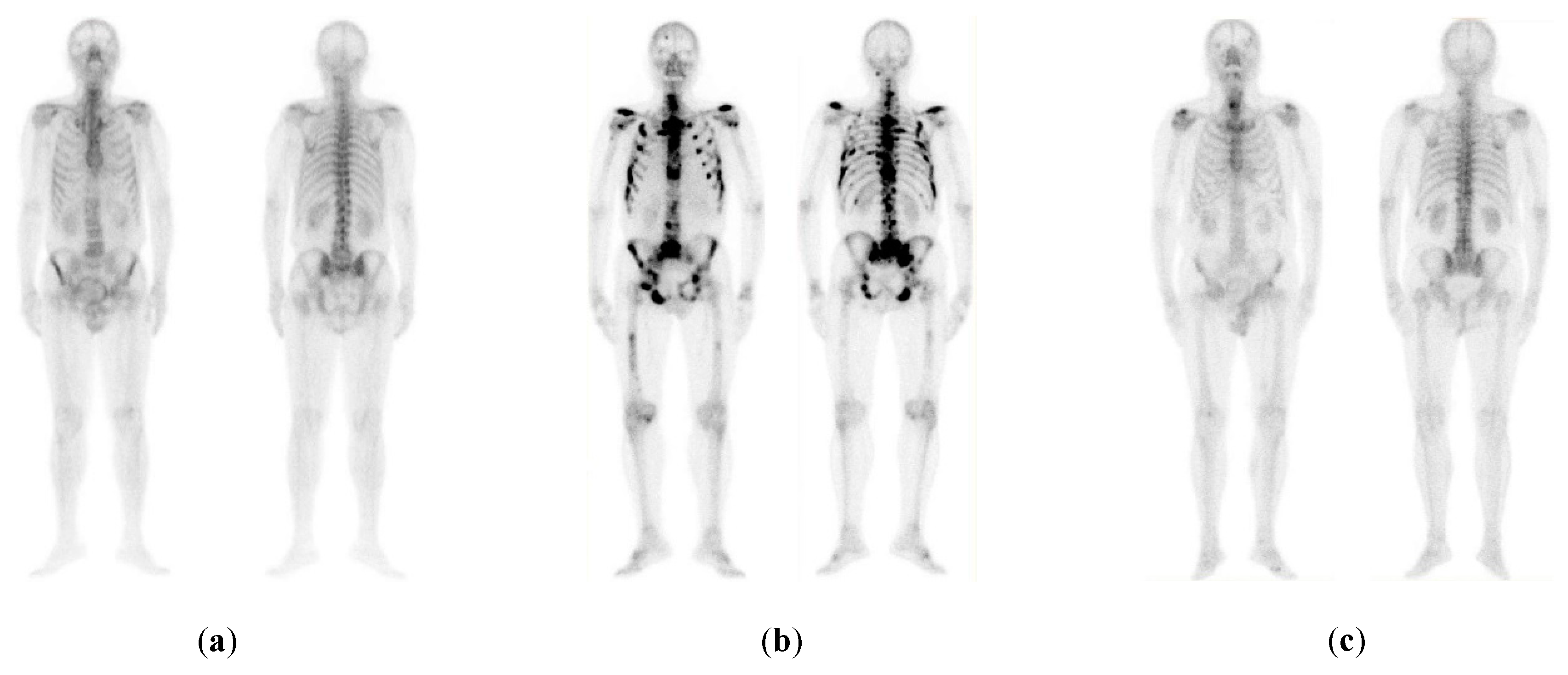
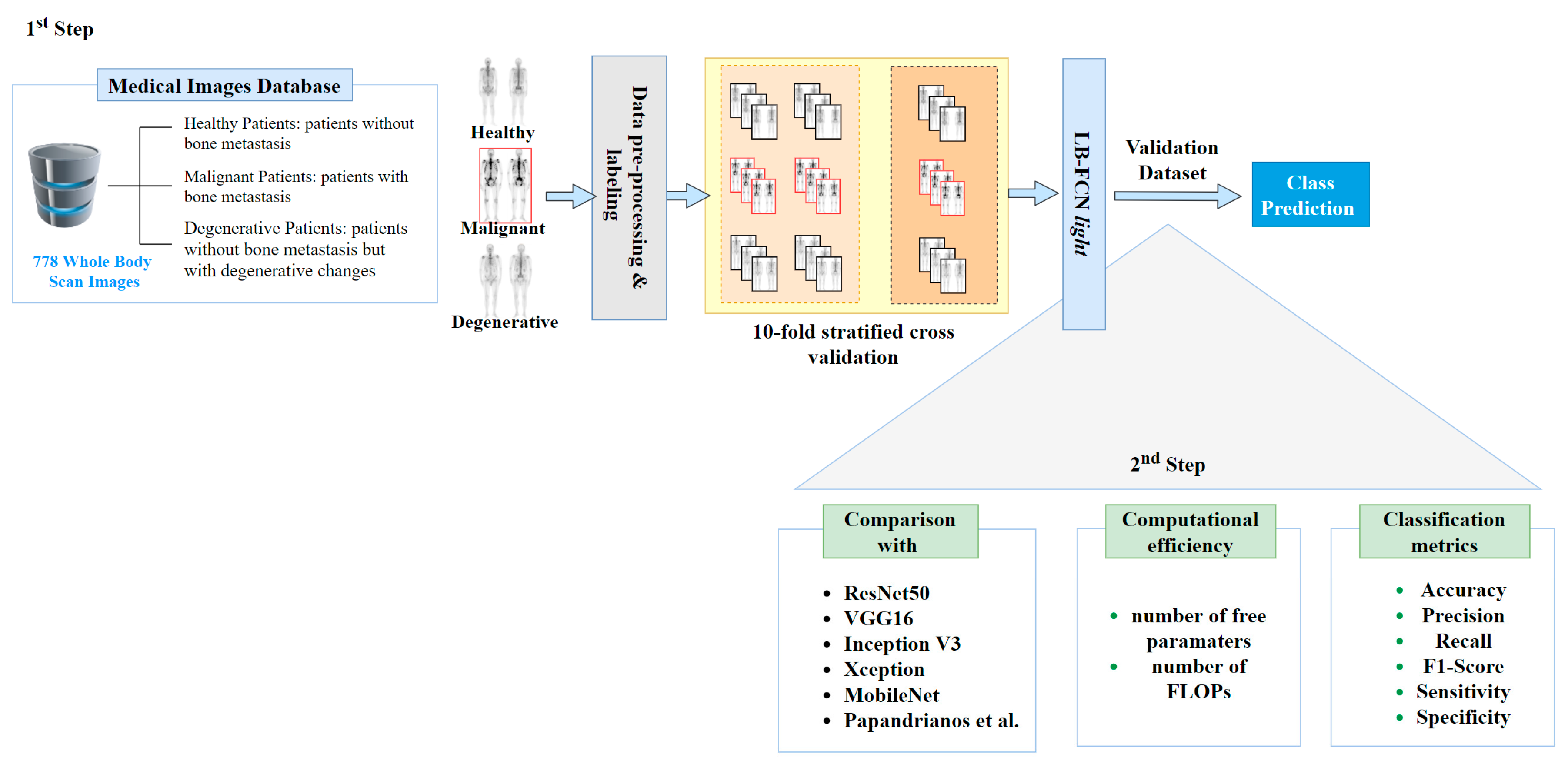
2.1. Dataset of Whole-Body Scan Images
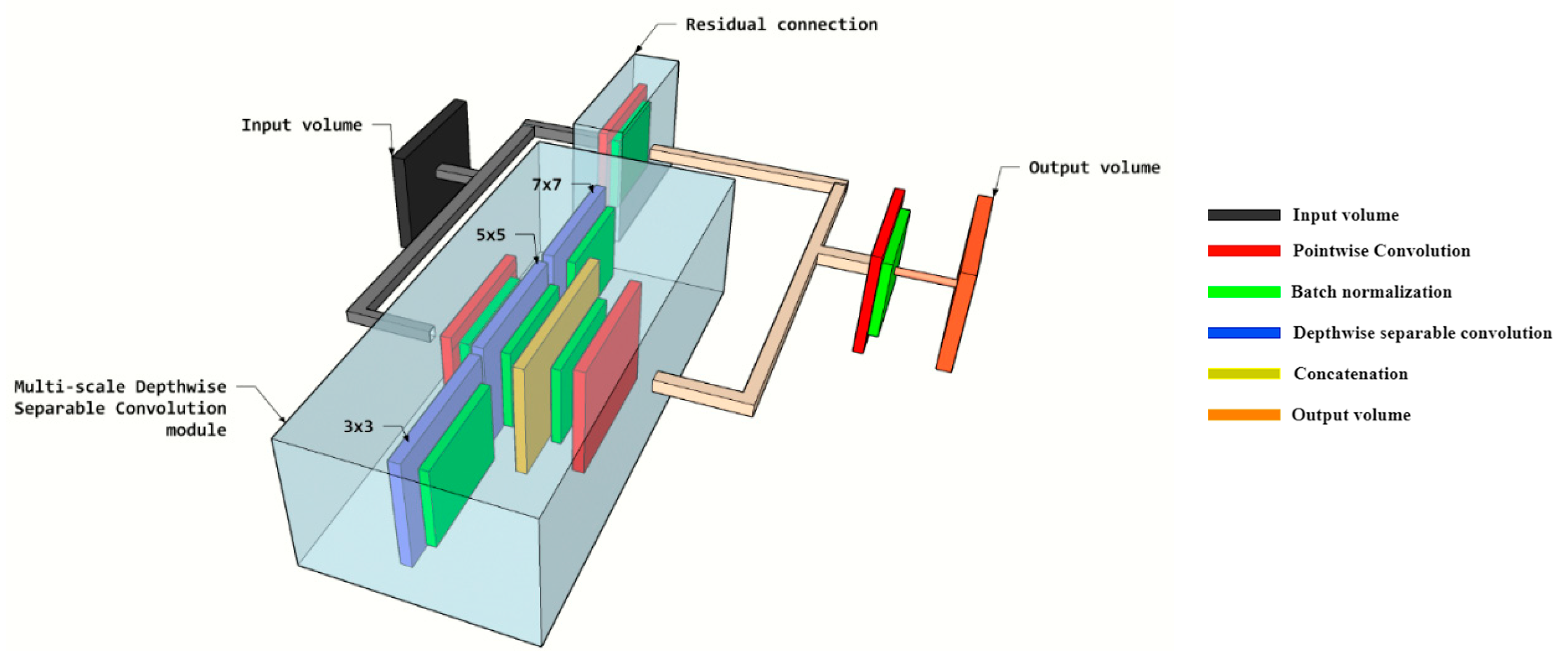
2.2. The Proposed Methodology
3. Results
4. Discussion
- A large annotated dataset of medical images is necessary to achieve strong generalization ability.
- Abnormalities in images can also be presented due to non-neoplastic diseases. This can lead to low specificity and high sensitivity.
- The use of deep learning in computer-aided diagnostic systems typically requires significant computational resources, limiting their use to powerful computers.
- Is capable of generalizing well, even when the availability of training images is limited, due to its multi-scale feature extraction process. This is important in applications where high classification performance is required with limited data. Such applications include computer-aided medical systems, where data availability is limited due to patient privacy legislation.
- Achieves a high overall classification performance outperforming the state-of-the-art approaches. Specifically, LB-FCN light achieved a 97.41% accuracy rate, which indicates that the proposed architecture can detect bone metastasis with almost three times lower error rate (2.59%) compared to the state-of-the-art approach [14].
- Has a significantly lower number of free parameters (0.3 × 106) and FLOPs (0.6 × 106) compared to conventional approaches enabling its use in embedded and mobile devices, such as tablets and portable diagnostic systems.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ibrahim, T.; Flamini, E.; Fabbri, L.; Serra, P.; Mercatali, L.; Ricci, R.; Sacanna, E.; Falasconi, M.C.; Casadei, R.; Galassi, R.; et al. Multidisciplinary approach to the treatment of bone metastases: Osteo-Oncology Center, a new organizational model. Tumori J. 2009, 95, 291–297. [Google Scholar] [CrossRef]
- Coleman, R. Metastatic bone disease: Clinical features, pathophysiology and treatment strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, Z.; Du, X.; He, L.; Chen, J.; Wang, W.; Sun, F.; Du, F.; Luo, Z.; Xue, Z.; et al. Clinical value of whole-body magnetic resonance diffusion weighted imaging on detection of malignant metastases. Chin. Med. Sci. J. 2009, 24, 112–116. [Google Scholar] [CrossRef]
- Wu, Q.; Yang, R.; Zhou, F.; Hu, Y. Comparison of whole-body MRI and skeletal scintigraphy for detection of bone metastatic tumors: A meta-analysis. Surg. Oncol. 2013, 22, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Bombardieri, E.; Aktolun, C.; Baum, R.P.; Bishof-Delaloye, A.; Buscombe, J.; Maffioli, L.S.; Moncayo, R.; Mortelmans, L.; Reske, S.N. Bone scintigraphy: Procedure guidelines for tumour imaging. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, B132–B139. [Google Scholar] [CrossRef] [PubMed]
- Ak, M.F. A Comparative Analysis of Breast Cancer Detection and Diagnosis Using Data Visualization and Machine Learning Applications. Healthcare 2020, 8, 111. [Google Scholar] [CrossRef]
- Yin, C.; Chen, Z. Developing Sustainable Classification of Diseases via Deep Learning and Semi-Supervised Learning. Healthcare 2020, 8, 291. [Google Scholar] [CrossRef]
- Yoo, H.; Han, S.; Chung, K. A Frequency Pattern Mining Model Based on Deep Neural Network for Real-Time Classification of Heart Conditions. Healthcare 2020, 8, 234. [Google Scholar] [CrossRef]
- Elfarra, F.-G.; Calin, M.A.; Parasca, S.V. Computer-aided detection of bone metastasis in bone scintigraphy images using parallelepiped classification method. Ann. Nucl. Med. 2019, 33, 866–874. [Google Scholar] [CrossRef]
- Pi, Y.; Zhao, Z.; Xiang, Y.; Li, Y.; Cai, H.; Yi, Z. Automated diagnosis of bone metastasis based on multi-view bone scans using attention-augmented deep neural networks. Med. Image Anal. 2020, 65, 101784. [Google Scholar] [CrossRef]
- Aslantas, A.; Dandil, E.; Saǧlam, S.; Çakiroǧlu, M. CADBOSS: A computer-aided diagnosis system for whole-body bone scintigraphy scans. J. Cancer Res. Ther. 2016, 12, 787. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Lu, H.; Kim, H.; Murakami, S.; Ueno, M.; Terasawa, T.; Aoki, T. Segmentation of Bone Metastasis in CT Images Based on Modified HED. In Proceedings of the 2019 19th International Conference on Control, Automation and Systems (ICCAS), Jeju, Korea, 15–18 October 2019; pp. 812–815. [Google Scholar]
- Papandrianos, N.; Papageorgiou, E.; Anagnostis, A.; Feleki, A. A Deep-Learning Approach for Diagnosis of Metastatic Breast Cancer in Bones from Whole-Body Scans. Appl. Sci. 2020, 10, 997. [Google Scholar] [CrossRef] [Green Version]
- Papandrianos, N.; Papageorgiou, E.; Anagnostis, A. Efficient Bone Metastasis Diagnosis in BoneScintigraphy Using a Fast Convolutional NeuralNetwork Architecture. Diagnostics 2020, 10, 532. [Google Scholar] [CrossRef] [PubMed]
- Papandrianos, N.; Papageorgiou, E.; Anagnostis, A.; Papageorgiou, K. Bone metastasis classification using whole body images from prostate cancer patients based on convolutional neural networks application. PLoS ONE 2020, 15, e0237213. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wen, X.; Lu, Y.; Yao, Y.; Zhao, H. Exploiting machine learning for predicting skeletal-related events in cancer patients with bone metastases. Oncotarget 2016, 7, 12612. [Google Scholar] [CrossRef]
- Pianou, N.K.; Stavrou, P.; Evangelia Vlontzou, M.; Phivi Rondogianni, M.; Demetrios, N.; Exarhos, M.; Datseris, I. More advantages in detecting bone and soft tissue metastases 18 from prostate cancer using F-PSMA PET/CT. Hell. J. Nucl. Med. 2019, 22, 6–9. [Google Scholar]
- Bradshaw, T.; Perk, T.; Chen, S.; Im, H.-J.; Cho, S.; Perlman, S.; Jeraj, R. Deep learning for classification of benign and malignant bone lesions in [F-18] NaF PET/CT images. J. Nucl. Med. 2018, 59, 327. [Google Scholar]
- Furuya, S.; Kawauchi, K.; Hirata, K.; Manabe, O.; Watanabe, S.; Kobayashi, K.; Ichikawa, S.; Katoh, C.; Shiga, T. A convolutional neural network-based system to detect malignant findings in FDG PET-CT examinations. J. Nucl. Med. 2019, 60, 1210. [Google Scholar]
- Perk, T.; Bradshaw, T.; Chen, S.; Im, H.; Cho, S.; Perlman, S.; Liu, G.; Jeraj, R. Automated classification of benign and malignant lesions in 18F-NaF PET/CT images using machine learning. Phys. Med. Biol. 2018, 63, 225019. [Google Scholar] [CrossRef] [Green Version]
- Springenberg, J.T.; Dosovitskiy, A.; Brox, T.; Riedmiller, M. Striving for simplicity: The all convolutional net. arXiv 2014, arXiv:1412.6806. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Hegenbart, S.; Uhl, A.; Vécsei, A.; Wimmer, G. Scale invariant texture descriptors for classifying celiac disease. Med. Image Anal. 2013, 17, 458–474. [Google Scholar] [CrossRef] [PubMed]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Diamantis, D.E.; Iakovidis, D.K.; Koulaouzidis, A. Look-behind fully convolutional neural network for computer-aided endoscopy. Biomed. Signal Process. Control 2019, 49, 192–201. [Google Scholar] [CrossRef]
- Weiner, G.M.; Jenicke, L.; Muller, V.; Bohuslavizki, K.H. Artifacts and non-osseous uptake in bone scintigraphy. Imaging reports of 20 cases. Radiol. Oncol. 2001, 35, 185–191. [Google Scholar]
- Ma, L.; Ma, C.; Liu, Y.; Wang, X. Thyroid diagnosis from SPECT images using convolutional neural network with optimization. Comput. Intell. Neurosci. 2019, 2019, 6212759. [Google Scholar] [CrossRef] [Green Version]
- Rybak, L.; Rosenthal, D. Radiological imaging for the diagnosis of bone metastases. QJ Nucl. Med. 2001, 45, 53–64. [Google Scholar]
- Eustace, S.; Tello, R.; DeCarvalho, V.; Carey, J.; Wroblicka, J.; Melhem, E.; Yucel, E. A comparison of whole-body turboSTIR MR imaging and planar 99mTc-methylene diphosphonate scintigraphy in the examination of patients with suspected skeletal metastases. Am. J. Roentgenol. 1997, 169, 1655–1661. [Google Scholar] [CrossRef]
- Mettler, F.A.; Guiberteau, M.J. Essentials of Nuclear Medicine and Molecular Imaging E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2018. [Google Scholar]
- Ziessman, H.A.; O’Malley, J.; Thrall, J. Requisites in radiology. Nuclear Medicine: The Requisites, 3rd ed.; Mosby Elsevier: Philadelphia, PA, USA, 2006. [Google Scholar]
- Gosfield, E.; Alavi, A.; Kneeland, B. Comparison of radionuclide bone scans and magnetic resonance imaging in detecting spinal metastases. J. Nucl. Med. 1993, 34, 2191. [Google Scholar]
- Diamantis, D.E.; Koutsiou, D.-C.C.; Iakovidis, D.K. Staircase Detection Using a Lightweight Look-Behind Fully Convolutional Neural Network. In Engineering Applications of Neural Networks, Proceedings of the International Conference on Engineering Applications of Neural Networks, Crete, Greece, 24–26 May 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 522–532. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. In 25th International Conference on Neural Information Processing Systems; ACM: Lake Tahoe, NV, USA, 2012; pp. 1097–1105. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Balayla, J. Prevalence Threshold and the Geometry of Screening Curves. arXiv 2020, arXiv:2006.00398. [Google Scholar] [CrossRef]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2020. [Google Scholar] [CrossRef]
- Prokopijevi, M.; Stanci, A.; Vasiljevi, J.; Stojkovi, Ž.; Dimi, G.; Sopta, J.; Risti, D.; Nagamalai, D. Neural Network based classification of bone metastasis by primary cacinoma. arXiv 2018, arXiv:1810.05725. [Google Scholar]
- Belcher, L. Convolutional Neural Networks for Classification of Prostate Cancer Metastases Using Bone Scan Images. Master’s Thesis, Physics and Astronomy, Department of Astronomy and Theoretical Physics, Lund University, Lund, Sweden, 2017. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. Tensorflow: A system for large-scale machine learning. In Proceedings of the OSDI, Savannah, GA, USA, 2–4 November 2016; Volume 16, pp. 265–283. [Google Scholar]
- Zhao, Z.; Pi, Y.; Jiang, L.; Xiang, Y.; Wei, J.; Yang, P.; Zhang, W.; Zhong, X.; Zhou, K.; Li, Y.; et al. Deep Neural Network Based Artificial Intelligence Assisted Diagnosis of Bone Scintigraphy for Cancer Bone Metastasis. Cancer Biol. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Network | Characteristics |
|---|---|
| ResNet50 [22] | pixel size , batch size = , dropout = , global average pooling, dense nodes , epochs = |
| VGG16 [35] | pixel size , batch size = , dropout = , flatten, dense nodes , epochs = |
| MobileNet [39] | pixel size , batch size = , dropout = , global average pooling, epochs = |
| InceptionV3 [36] | pixel size , batch size = , dropout = , global average pooling, dense nodes = , epochs = |
| Xception [37] | pixel size , batch size = , dropout = , flatten, dense nodes = , epochs = |
| Papadrianos et al. [14] | pixel size , batch size = 32, dropout = 0.2, dense nodes =, epochs = |
| LB-FCN light [33] | pixel size , batch size = 32, global average pooling, epochs = |
| Network | Precision | Recall | F1-Score | Sensitivity | Specificity |
|---|---|---|---|---|---|
| ResNet50 [22] | 0.994 | 0.777 | 0.866 | 0.825 | 0.997 |
| VGG16 [35] | 0.952 | 0.844 | 0.896 | 0.855 | 0.988 |
| MobileNet [39] | 0.890 | 0.990 | 0.936 | 0.857 | 0.960 |
| InceptionV3 [36] | 0.884 | 0.958 | 0.916 | 0.959 | 0.947 |
| Xception [37] | 0.958 | 0.908 | 0.931 | 0.913 | 0.988 |
| Papadrianos et al. [14] | 0.950 | 0.938 | 0.942 | 0.938 | 0.978 |
| LB-FCN light [33] | 0.972 | 0.978 | 0.975 | 0.978 | 0.992 |
| Network | Precision | Recall | F1-Score | Sensitivity | Specificity |
|---|---|---|---|---|---|
| ResNet50 [22] | 0.904 | 0.972 | 0.934 | 0.971 | 0.921 |
| VGG16 [35] | 0.952 | 0.950 | 0.952 | 0.949 | 0.960 |
| MobileNet [39] | 0.946 | 0.941 | 0.944 | 0.940 | 0.952 |
| InceptionV3 [36] | 0.902 | 0.922 | 0.911 | 0.920 | 0.909 |
| Xception [37] | 0.964 | 0.932 | 0.946 | 0.937 | 0.909 |
| Papadrianos et al. [14] | 0.948 | 0.928 | 0.938 | 0.927 | 0.960 |
| LB-FCN light [33] | 0.979 | 0.979 | 0.979 | 0.978 | 0.984 |
| Network | Precision | Recall | F1-Score | Sensitivity | Specificity |
|---|---|---|---|---|---|
| ResNet50 [22] | 0.830 | 0.882 | 0.846 | 0.881 | 0.902 |
| VGG16 [35] | 0.836 | 0.914 | 0.872 | 0.913 | 0.917 |
| MobileNet [39] | 0.938 | 0.856 | 0.888 | 0.857 | 0.960 |
| InceptionV3 [36] | 0.848 | 0.754 | 0.786 | 0.755 | 0.937 |
| Xception [37] | 0.820 | 0.936 | 0.904 | 0.934 | 0.925 |
| Papadrianos et al. [14] | 0.862 | 0.894 | 0.874 | 0.894 | 0.933 |
| LB-FCN light [33] | 0.970 | 0.967 | 0.968 | 0.967 | 0.984 |
| ResNet50 [22] | VGG16 [35] | MobileNet [39] | InceptionV3 [36] | Xception [37] | Papandrianos et al. [14] | LB-FCN light [33] | |
|---|---|---|---|---|---|---|---|
| Accuracy | 90.74% | 90.83% | 91.02% | 88.96% | 91.54% | 91.61% | 97.41% |
| FLOPs (×106) | Trainable Free Parameters (×106) | |
|---|---|---|
| ResNet50 [22] | 47.0 | 23.5 |
| VGG16 [35] | 268.5 | 134.2 |
| MobileNet [39] | 6.4 | 3.2 |
| InceptionV3 [36] | 43.5 | 21.8 |
| Xception [37] | 41.6 | 20.8 |
| Papadrianos et al. [14] | 13.1 | 6.5 |
| LB-FCN light [33] | 0.6 | 0.3 |
| Studies | Year | ML Method | Classification Problem | Results |
|---|---|---|---|---|
| [10] | 2020 | Deep CNNs | 2 classes: absence or presence of bone metastasis | accuracy of 89.00%, F1-score of 0.893, and Sensitivity of 92.00% |
| [14] | 2020 | CNN | 2 classes: BS metastasis in prostate patient or not 3 classes: (a) benign, (b) malignant and (c) degenerative | overall classification accuracy 91.61% ± 2.46% accuracy regarding normal, malignant and degenerative changes: 91.3%, 94.7% and 88.6% |
| [15] | 2020 | CNN | 2 classes: BS metastasis in prostate patient or not | 97.38% classification testing accuracy and 95.8% average sensitivity |
| [9] | 2019 | Parallelepiped algorithm | 2 classes: absence or presence of bone metastasis | 87.58 ± 2.25% classification accuracy and 0.8367 ± 0.0252 κ coefficient |
| [12] | 2019 | Modified Fully CNN | Segmentation of the BS area | 69.2% intersection over union rate and 79.8% true positive rate |
| [13] | 2019 | CNN | 2 classes: metastasis of breast cancer or not | classification accuracy of 92.50%, 95% sensitivity |
| [11] | 2016 | CADBOSS (ANNs) | 2 classes: absence or presence of bone metastasis | 92.30% accuracy, 94% sensitivity and 86.67% specificity |
| [16] | 2016 | LR, DT and SVM | 2 classes: absence or presence of bone metastasis | LR, DT, and SVM classification accuracy was 79.2%, 85.8% and 88.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ntakolia, C.; Diamantis, D.E.; Papandrianos, N.; Moustakidis, S.; Papageorgiou, E.I. A Lightweight Convolutional Neural Network Architecture Applied for Bone Metastasis Classification in Nuclear Medicine: A Case Study on Prostate Cancer Patients. Healthcare 2020, 8, 493. https://doi.org/10.3390/healthcare8040493
Ntakolia C, Diamantis DE, Papandrianos N, Moustakidis S, Papageorgiou EI. A Lightweight Convolutional Neural Network Architecture Applied for Bone Metastasis Classification in Nuclear Medicine: A Case Study on Prostate Cancer Patients. Healthcare. 2020; 8(4):493. https://doi.org/10.3390/healthcare8040493
Chicago/Turabian StyleNtakolia, Charis, Dimitrios E. Diamantis, Nikolaos Papandrianos, Serafeim Moustakidis, and Elpiniki I. Papageorgiou. 2020. "A Lightweight Convolutional Neural Network Architecture Applied for Bone Metastasis Classification in Nuclear Medicine: A Case Study on Prostate Cancer Patients" Healthcare 8, no. 4: 493. https://doi.org/10.3390/healthcare8040493
APA StyleNtakolia, C., Diamantis, D. E., Papandrianos, N., Moustakidis, S., & Papageorgiou, E. I. (2020). A Lightweight Convolutional Neural Network Architecture Applied for Bone Metastasis Classification in Nuclear Medicine: A Case Study on Prostate Cancer Patients. Healthcare, 8(4), 493. https://doi.org/10.3390/healthcare8040493