Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review

 ,
,
Abstract
:1. Introduction
1.1. Rationale
“The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities.”
1.2. Telehealth and COVID-19
1.3. Objectives
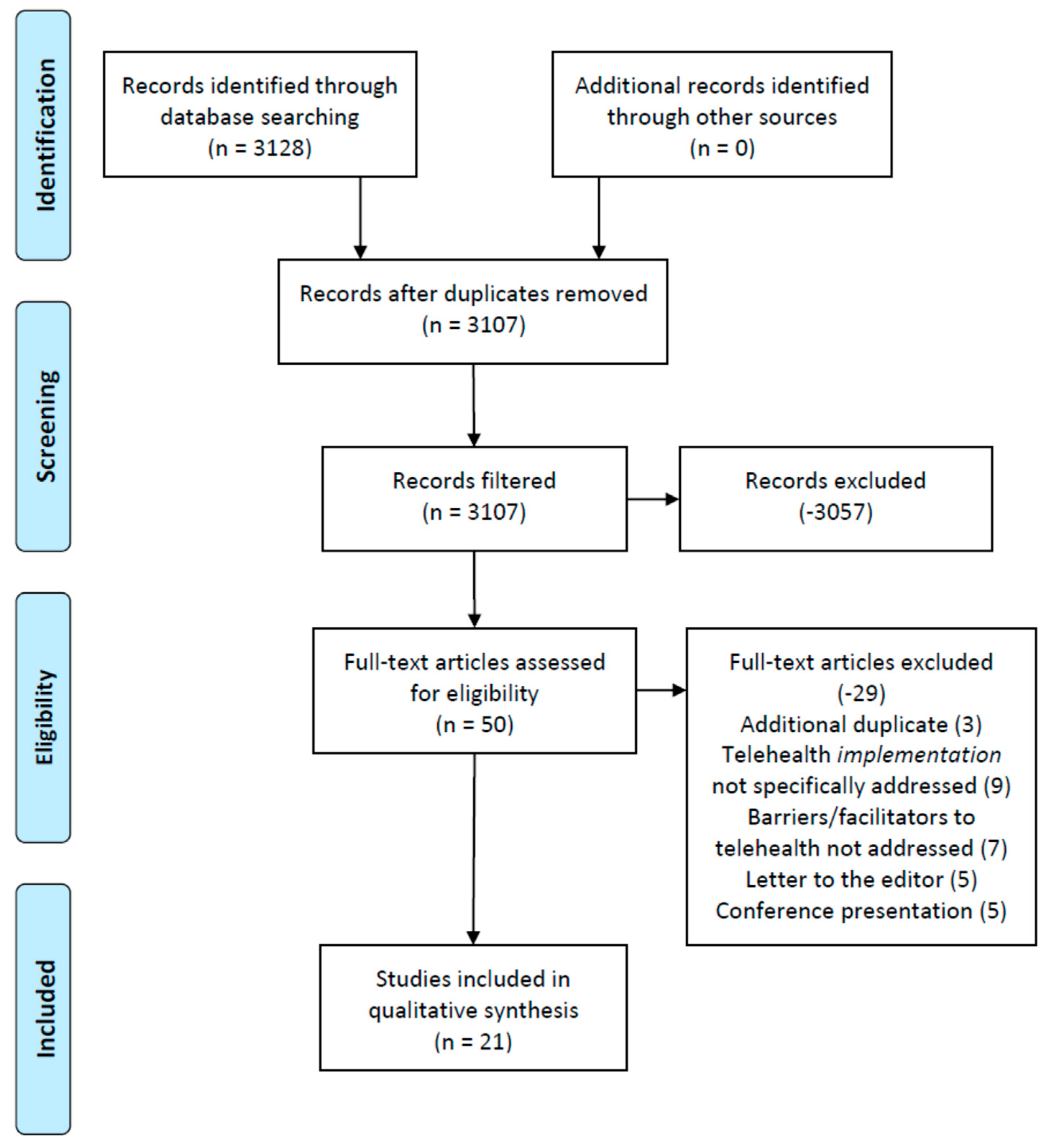
2. Methods
2.1. Overview
2.2. Inclusion Criteria
2.3. Exclusion Criteria
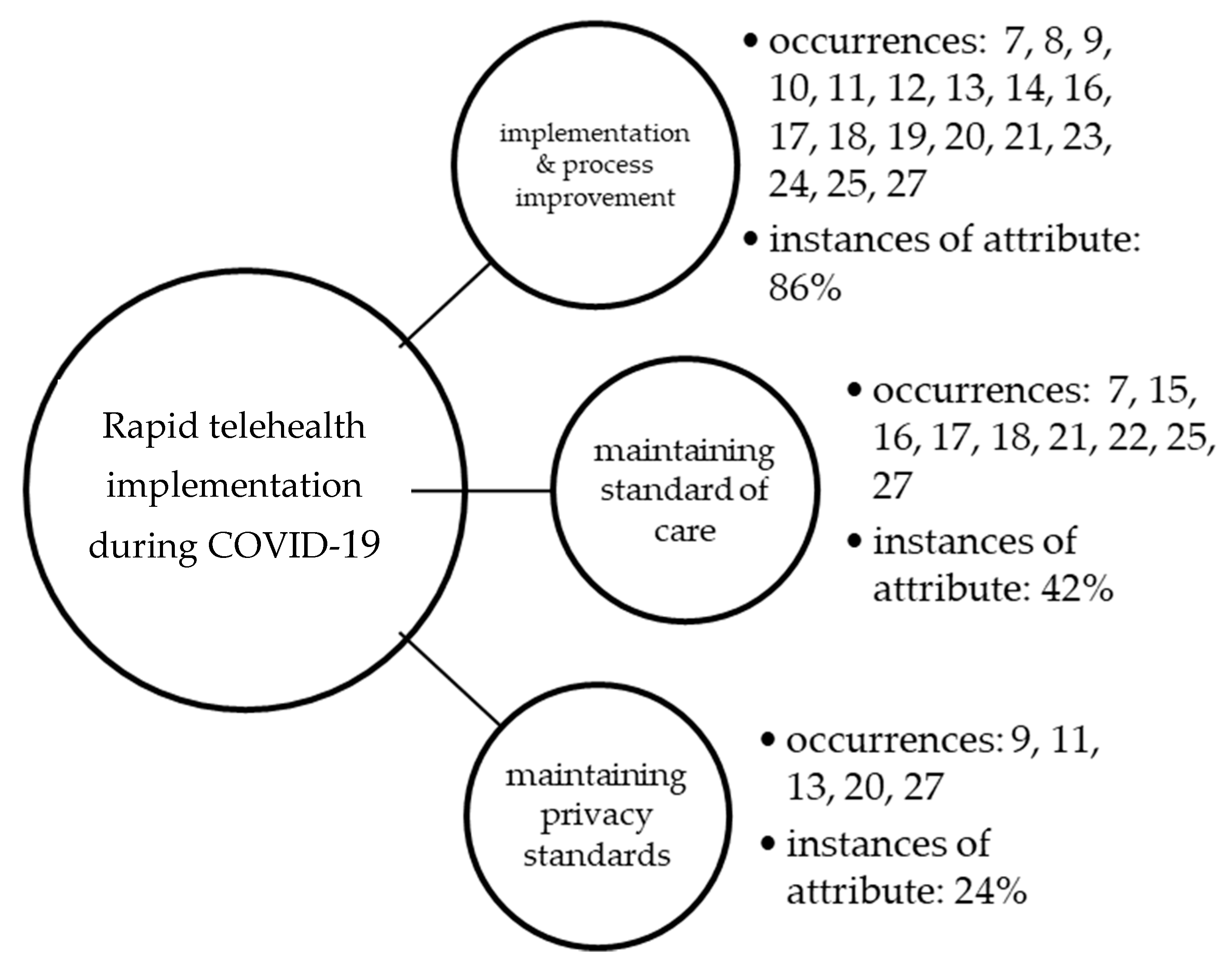
3. Results
4. Discussion
4.1. Implementation and Process Improvement
4.2. Maintaining the Standard of Care
4.3. Maintaining Privacy Standards
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/gho/goe/telehealth/en/ (accessed on 24 July 2020).
- Mahoney, M.F. Telehealth, Telemedicine, and Related Technologic Platforms: Current Practice and Response to the COVID-19 Pandemic. J. Wound Ostomy Cont. Nurs. 2020, 47, 439–444. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Family Physicians. What’s the Difference between Telemedicine and Telehealth? Available online: https://www.aafp.org/news/media-center/kits/telemedicine-and-telehealth.html (accessed on 24 November 2020).
- Centers for Disease Control and Prevention. Emergence of the COVID-19 Pandemic—United States, January–March 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6943a3.htm (accessed on 24 November 2020).
- Health and Human Services. Telehealth: Delivering Care Safely during COVID-19; Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.hhs.gov/coronavirus/telehealth/index.html (accessed on 24 July 2020).
- Imaging Technology News. Telehealth to Experience Massive Growth Due to COVID-19; Imaging Technology News: Park Ridge, NJ, USA, 2020; Available online: https://www.itnonline.com/content/telehealth-experience-massive-growth-due-covid-19 (accessed on 24 July 2020).
- Fisk, M.; Livingstone, A.; Pit, S. Telehealth in the Context of COVID-19: Changing Perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19264. [Google Scholar] [CrossRef] [PubMed]
- Drogin, E.Y. Forensic mental telehealth assessment (FMTA) in the context of COVID-19. Int. J. Law Psychiatry 2020, 71, 101595. [Google Scholar] [CrossRef] [PubMed]
- Green, B.N.; Pence, T.V.; Kwan, L.; Rokicki-Parashar, J. Rapid Deployment of Chiropractic Telehealth at 2 Worksite Health Centers in Response to the COVID-19 Pandemic: Observations from the Field. J. Manip. Physiol. Ther. 2020, 43, 404.e1–404.e10. [Google Scholar] [CrossRef]
- Keihanian, T.; Sharma, P.; Goyal, J.; Sussman, D.A.; Girotra, M. TeleHealth utilization in Gastroenterology (GI) clinics amid Coronavirus-19 (COVID-19) pandemic: Impact on clinical practice & GI training. Gastroenterology 2020, 159, 1598–1601. [Google Scholar]
- Carlson, J.; Goldstein, R. Using the Electronic Health Record to Conduct Adolescent Telehealth Visits in the Time of COVID-19. J. Adolesc. Health 2020, 67, 157–158. [Google Scholar] [CrossRef]
- Imperatori, C.; Dakanalis, A.; Farina, B.; Pallavicini, F.; Colmegna, F.; Mantovani, F.; Clerici, M. Global Storm of Stress-Related Psychopathological Symptoms: A Brief Overview on the Usefulness of Virtual Reality in Facing the Mental Health Impact of COVID-19. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 782–788. [Google Scholar] [CrossRef]
- Fang, J.; Liu, Y.T.; Lee, E.Y.; Yadav, K. Telehealth Solutions for In-hospital Communication with Patients under Isolation during COVID-19. West. J. Emerg. Med. 2020, 21, 801–806. [Google Scholar] [CrossRef]
- Wright, C.H.; Wright, J.; Shammassian, B. COVID-19: Launching neurosurgery into the era of telehealth in the United States. World Neurosurg. 2020, 140, 54–55. [Google Scholar] [CrossRef]
- Gould, C.E.; Hantke, N.C. Promoting Technology and Virtual Visits to Improve Older Adult Mental Health in the Face of COVID-19. Am. J. Geriatr. Psychiatry 2020, 28, 889–890. [Google Scholar] [CrossRef]
- Gao, Z.; Lee, J.E.; McDonough, D.J.; Albers, C. Virtual Reality Exercise as a Coping Strategy for Health and Wellness Promotion in Older Adults during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1986. [Google Scholar] [CrossRef] [PubMed]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.J.; Cohen, J.A.; Ba, M.B.; Levin, A.O.; Goyal, N.; Bs, T.L.; Chesney, M.A.; Shumay, D.M. “Soup cans, brooms, and Zoom”: Rapid conversion of a cancer survivorship program to telehealth during COVID-19. Psycho-Oncology 2020. [Google Scholar] [CrossRef]
- Hewitt, K.C.; Loring, D.W. Emory university telehealth neuropsychology development and implementation in response to the COVID-19 pandemic. Clin. Neuropsychol. 2020, 1–15. [Google Scholar] [CrossRef]
- Chowdhury, D.; Hope, K.D.; Arthur, L.C.; Weinberger, S.M.; Ronai, C.; Johnson, J.N.; Snyder, C.S. Telehealth for Pediatric Cardiology Practitioners in the Time of COVID-19. Pediatr. Cardiol. 2020, 1–11. [Google Scholar] [CrossRef]
- Burgess, C.; Miller, C.; Franz, A.; Abel, E.A.; Gyulai, L.; Osser, D.; Smith, E.G.; Connolly, S.L.; Krawczyk, L.; Bauer, M.; et al. Practical lessons learned for assessing and treating bipolar disorder via telehealth modalities during the COVID-19 pandemic. Bipolar Disord. 2020, 22, 556–557. [Google Scholar] [CrossRef]
- Fantz, C.R.; Rivers, M. COVID-19 Awakens a New Focus on Surge Capacity Blood Glucose Testing and the Critical Role of Telehealth in Self-Management. J. Diabetes Sci. Technol. 2020, 14, 733–734. [Google Scholar] [CrossRef]
- Gadzinski, A.J.; Andino, J.J.; Odisho, A.Y.; Watts, K.L.; Gore, J.L.; Ellimoottil, C. Telemedicine and eConsults for Hospitalized Patients During COVID-19. Urology 2020, 141, 12–14. [Google Scholar] [CrossRef]
- Shipchandler, T.Z.; Nesemeier, B.R.; Parker, N.P.; Vernon, D.; Campiti, V.J.; Anthony, B.P.; Alwani, M.M.; Illing, E.A.; Ting, J.Y. Telehealth Opportunities for the Otolaryngologist: A Silver Lining During the COVID-19 Pandemic. Otolaryngol. Neck Surg. 2020, 163, 112–113. [Google Scholar] [CrossRef]
- Hirko, K.A.; Kerver, J.M.; Ford, S.; Szafranski, C.; Beckett, J.; Kitchen, C.; Wendling, A.L. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. J. Am. Med. Inform. Assoc. 2020, 27, 1816–1818. [Google Scholar] [CrossRef]
- Baidal, J.A.W.; Chang, J.; Hulse, E.; Turetsky, R.; Parkinson, K.; Rausch, J.C. Zooming Toward a Telehealth Solution for Vulnerable Children with Obesity During Coronavirus Disease 2019. Obesity 2020, 28, 1184–1186. [Google Scholar] [CrossRef] [PubMed]
- Moring, J.C.; Dondanville, K.A.; Fina, B.A.; Hassija, C.; Chard, K.; Monson, C.; Losavio, S.T.; Wells, S.Y.; Morland, L.A.; Kaysen, D.; et al. Cognitive Processing Therapy for Posttraumatic Stress Disorder via Telehealth: Practical Considerations During the COVID-19 Pandemic. J. Trauma. Stress 2020, 33, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Levine, L.B.; Guidry, M. Telehealth and COVID-19. EP Magazine. 6 May 2020. Available online: https://www.mavenproject.org/press/2020/5/6/telehealth-and-covid-19 (accessed on 24 July 2020).
- Miller, J.J. Jumping Into Telehealth. Psychiatric Times. 18 June 2020. Available online: https://www.psychiatrictimes.com/view/jumping-into-telehealth (accessed on 19 July 2020).
- Kojima, N.; Klausner, J.D. Virtual House Calls: Telemedicine and Reforming the Health Care Delivery Model with Strategies Implemented in a Novel Coronavirus Pandemic. J. Gen. Intern. Med. 2020, 35, 2243. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Article Assignment | Reviewer 1 | Reviewer 2 | Reviewer 3 | Reviewer 4 | Reviewer 5 | Reviewer 6 |
|---|---|---|---|---|---|---|
| Articles 1–10 | X | X | X | |||
| Articles 11–20 | X | X | X | X | X | X |
| Articles 21–30 | X | X | X | X | X | X |
| Articles 31–40 | X | X | X | |||
| Articles 41–50 | X | X | X |
| Author(s) | Participant(s) | * JHNEBP Study Design | Telehealth Facilitator(s) | Telehealth Barrier(s) |
|---|---|---|---|---|
| Fisk et al. [7] | Australia, UK, and USA governments and health care agencies | 3 | Patient choice, cost, and convenience cited. Reduction in hospital admissions. Improvement in patient health literacy. | Further requirement to become integrated within health and social care service frameworks. Not viewed by patients as a 100% suitable replacement for in-person health care treatment. Technology concerns/barriers/bandwidth. |
| Drogin [8] | Mental health providers | 4 | Cites decrease in travel costs, and shorter eval turnaround time occasioned by more flexible scheduling. Increased validity of FMTA evaluations due to virtual setting/administration of exam. | Consideration to circumstances in which face-to-face interactions are eliminated by pandemic situations. Questionable communication ‘behind the scenes’ with patient during online exams are of concern. |
| Green et al. [9] | Chiropractic providers within a physical medicine practice | 4 | Communicate the availability of chiropractic specialty (virtual) care to neighboring providers ahead of time. Modify encounter to enable patient to demonstrate posture/etc in front of camera. | To implement video visits effectively and legally, one must consider several requirements (privacy, legal, others). Reviews several potential problems associated with video visit delivery, yet also associated solutions to assist others in implementing video-based care. |
| Keihanian et al. [10] | Gastroenterology group practice | 2 | Provider preference for webinar over phone visits/alternatives for higher acuity or less technology-inclined patents/visits. Private practice (versus academic centers) more apt and willing to support rapid implementation. | Provider half-days increased, while number of total visits decreased (patient throughput). Technical issues and patient preparedness for virtual visits cited. Lack of medical training (residents/fellows) once changed to virtual visits (supervision concerns). |
| Carlson et al. [11] | Academic pediatric center | 4 | Availability to pre-announce future available appointments helps with scheduling logistics. Ability to create an online patient portal with clinician/parent information separation for clinical reasons. Ability for increased patient (child) confidentiality exists due to increased access (availability to log-on without parent if necessary). | Access remains a concern when requiring children to make themselves available online via webcam. Patient confidentiality and parent authorization concerns. |
| Imperatori et al. [12] | Mental health organization | 3 | Psychopathological symptoms that increased during the pandemic may be addressed via virtual reality (VR) applications at an enhanced level. | Significant/clear guidelines for the correct use of this technology within mental health practice. Several technological and access issues related to the adoption of VR. |
| Fang et al. [13] | Academic medical center | 4 | Minimized PPE usage in the virtual environment. Respiratory isolated patients were not as big of a concern in the virtual environment. Enabled all patients who have been affected by hospital visitor restrictions to connect with their families. | Device cost, privacy, and security cited as provider concerns. Free apps and other software offer limited and/or varying opportunities (piecemeal). |
| Wright et al. [14] | Neurosurgery group practice | 4 | Multiple potential advantages of continuing to expand this model of health care delivery in specific neuroscience modality treatments. Alternative settings for telehealth include the permitted use of Google Hangouts, Facebook Messenger video chat, and Apple FaceTime. | Preparations must also be made for the unintended consequences of increased neurosurgery availability (many are listed). Cost and administrative challenges are a significant barrier to multistate telehealth licensure. Increased time per visit is a concern. |
| Gould et al. [15] | Gerontology | 4 | Increased access to care, even when compared to before the pandemic. Helps/assists (but does not completely resolve) social isolation and loneliness. | Sensory impairment accompanying aging and older adults of concern. Online/virtual movements, body language not interpreted the same, plus generational differences. Device ownership comes with an assumed competency of the technology and this is not always the case. |
| Gao et al. [16] | Gerontology/physical activity/recreational activity specialty | 4 | Efficacy and effectiveness of VR exercise in the promotion of favorable health outcomes among the older adults VR-based interventions are most effective in promoting improved health outcomes among older adults. Weight-loss management programs demonstrated some effectiveness (required further study/investigation). | Access to gaming systems cannot be assumed. Enhanced sessions can help with motivation (immersed treadmill video, etc) and also help with isolation concerns. |
| Wosik et al. [17] | Variety of health care organizations, undisclosed. | 3 | Health care encounters can be custom-tuned with telehealth applications for a better experience and patient outcomes. COVID-19 phases (isolation, initial hospital surge, and post-surge) also call for different telehealth application. | Phases of the pandemic will affect how to respond with telehealth, and this can become tricky and problematic if not tuned accordingly. Privacy noted as a serious concern. |
| Jhaveri et al. [18] | Hospital-based psych/oncology service line. | 4 | Participation surged as the program became instantly accessible to more survivors. Use of common household items became popular in exercises/etc in conjunction with webcams. | Group discussion included heightened risk and fear of falling ill, health-related vigilance, and risk associated with potential delays in surveillance or other survivorship care. Concerns regarding the requirement to initiate the program for survivorship reasons (no choice) and speed of implementation. Minimal screen-sharing (privacy, etc). |
| Hewitt et al. [19] | Academic neuropsychology clinic. | 4 | Troubleshooting manual created out of mock webinar testing enabled effective implementation results. Validated protocols can be highlighted to diminish the interoperative neuropsychological assertion in an adversarial environment. | Testing modifications (non-standard) had to occur to administer inventories to remote patients. Questionable state-level reimbursement based upon a) payer type and b) patient location (in or out-of-state). |
| Chowdhury et al. [20] | Pediatric cardiology medical practice. | 4 | Virtual health helps to increase physical distancing requirements with children. Provides a good/better view into the patient’s home environment, versus only being seen in the clinic/in-person. Decreased wait times for access to care assist providers with in-person triage encounters. | Adapted staffing and billing models are required for better/future telehealth visits. Still does not substitute for in-person procedures required (EKG, etc). Vital sign medical equipment is not always available in the patient’s home, much less pediatric sizes. |
| Burgess et al. [21] | Mental health: bipolar disorder treatment protocols | 4 | Telehealth possible, increased access if patient is available. More concerns and best-practices to control liability, versus facilitators beyond physical distancing protocols. | Certain aspects of speech, affect, and psychomotor agitation may require more effort when delivering virtual care compared to in-person care. Telephone connections feature significant lag, it may be difficult to interpret apparent interruptions or changes in voice. It is important to not assume; instead, assess for changes in functioning given novel outlets for various habits in the time of COVID-19. |
| Fantz et al. [22] | Diabetes self-management. | 4 | Use of ongoing/continuous glucose monitoring with technology assists with limited PPE during the pandemic. Self-management promotes physical distancing. Ongoing use of these self-management devices allow for a much larger data collection. | Putting a sharp focus on self-management will require more patient responsibility. Costs related to continuous monitoring. |
| Gadzinski et al. [23] | Hospital urology patients (routine and emergency) | 4 | eConsults allow for better inter-provider communication and overall access to information. Conserves PPE and limits COVID-19 exposures. Allows for a centralized workforce that is inter-connected online to support patient care. | Telehealth visits can include focused physical examination maneuvers using image- and audio capturing devices to assess the dermatologic, cardiac, and pulmonary systems. Strong focus on telehealth waivers and liability concerns. eConsults with other medical providers come with additional billing/documentation requirements. |
| Shipchandler et al. [24] | Otolaryngology medical practice | 4 | Improve upon current telehealth systems Improvement on access to care. Avoidance of ‘high risk’ settings. | Each visit is scheduled for 20 to 30 min employees who work remotely from home. Challenges to continue remote care beyond pandemic (routine care). |
| Hirko et al. [25] | Large rural health system. | 4 | Continued third-party reimbursement is promising to help continue increased access to medical providers (often more than before the pandemic). Rural locations virus prevalence is not to be taken lightly as surges expected to increase. | Issues in broadband access in rural settings, which limit the reach and effectiveness of telehealth initiatives, must be prioritized. Often rural patients endure financial challenges limiting technology access. |
| Woo et al. [26] | Pediatrics obesity clinic. | 4 | Contact hours (online) for pediatric and family weight-management counseling and other programs help control the disparities experienced during the pandemic. Rapid weight-management lifestyle changes forced into virtual visits continue to allow for such contact sessions with patients/family. | Privacy concerns for patients enrolled in weight-management programs. Access and cost of webinar equipment is an issue. Technology will only assist and not alleviate food insecurities and health disparities for patients in weight management programs. |
| Moring et al. [27] | Mental health/PTSD provider organizations. | 3 | Cognitive processing therapy was not compromised/lowered throughout telehealth visits. Keeping track of patient locations (addresses) during various telehealth visits helps with unanticipated medical emergencies. | Practitioners should attempt to use platforms that provide secure, encrypted videoconferencing technology. There is an limitation to a provider’s ability to address non-verbal (or even verbal) cues to intoxication and other issues virtually, versus in-person visits. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieneck, C.; Garvey, J.; Collins, C.; Graham, D.; Loving, C.; Pearson, R. Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review. Healthcare 2020, 8, 517. https://doi.org/10.3390/healthcare8040517
Lieneck C, Garvey J, Collins C, Graham D, Loving C, Pearson R. Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review. Healthcare. 2020; 8(4):517. https://doi.org/10.3390/healthcare8040517
Chicago/Turabian StyleLieneck, Cristian, Joseph Garvey, Courtney Collins, Danielle Graham, Corein Loving, and Raven Pearson. 2020. "Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review" Healthcare 8, no. 4: 517. https://doi.org/10.3390/healthcare8040517