3.1. Health Expenditure
The analysis of the monetary value of public health expenditure “in” the municipalities showed that human resource expenditure increased from the year 2008 to the year 2015 in all regions and in almost all population strata of the country, constant Brazil (BRL) prices of 2015. The term “in” represents municipal expenditure made from all sources of available health resources—federal, state, and own resources managed by the city [
15]. The South, Midwest, and Northeast regions stood out the most, growing above 50% on average, considering the exchange rates of 2008 (USD 0.5450) and 2015 (USD 0.3001). In the South, the effect was basically due to the increase in spending in all cities, but especially in those with a population between 20 and 50 thousand inhabitants. The Northeast region followed the same pattern but with one difference: the cities between 500 thousand and 1 million were those responsible for increasing personnel expenditures. In cities above 1 million inhabitants, there was a 20% drop in expenses under this heading (
Table 5).
It is important to note that Brazil has 5570 cities, clustered in 26 states plus one Federal District, which are grouped within five geoeconomic regions—North, Northeast, Midwest, Southeast, and South. The Brazilian geoeconomical regions are North (No), which groups the states of Acre (AC), Amapá (AP), Amazonas (AM), Pará (PA), Rondônia (RO), Roraima (RR), and Tocantins (TO); Northeast (NoE), with Alagoas (AL), Bahia (BA), Ceará (CE), Maranhão (MA), Paraíba (PB), Pernambuco (PE), Piauí (PI), Rio Grande do Norte (RN), and Sergipe (SE) states; Midwest (MiW), with the Federal District (DF) and the states of Goiás (GO), Mato Grosso (MT), and Mato Grosso do Sul (MS); Southeast (SoE), with Espírito Santo (ES), Minas Gerais (MG), Rio de Janeiro (RJ) and São Paulo (SP); and South (So), which includes the states of Paraná (PR), Santa Catarina (SC) and Rio Grande do Sul (RS). The North and Northeast regions of Brazil are historically poor regions and have always had low levels of public health services. Southeast and South are rich regions with considerable levels of service offer. The Midwest is a relatively new region, where occupation effectively started in 1950.
Public investment was lower in relation to human resources; this is due to the particularities of the health sector [
16]. The production of services is labor intensive, and its operation consumes a good part (in Brazil, on average, 70% [
17] of the establishment’s resources [
18]. It grew in all regions, except in the Southeast with a 30% drop. The low investment inversion occurs mainly in the 24 largest cities that make up the medium-large stratum and two larger cities within the large group, Campinas (SP state, SoE region) and Curitiba (capital, PR state, therefore, So region) (
Table 6).
Despite their population size, medium-large cities show considerable year-to-year fluctuations in their investment expenditures. Some of the highlights are the cities of Sorocaba (SP, SoE), João Pessoa (capital, PB, NoE), and Duque de Caxias (RJ, SoE), which together drastically reduced their investments, with the former dropping from the millions to the thousands. The cities of Ananindeua (PA, No), Uberlândia (MG, SoE), Ribeirão Preto (SP, SoE), Santo André (SP, SoE), and Campo Grande (capital, MS, MiW) also presented considerable decrease. These variations suggest a certain structural constraint to the continuous and consistent expansion of expenditures, where a large part of these municipalities is still sensitive to federal transfers. This is different in the cases of Campinas (SP, SoE) and Curitiba (PR, So), both cities with a population of more than 1 million inhabitants, which are cities with some stability in their own resources but which show a fall in expenditure.
Despite this, some cities increased investment spending, with the expansion of network service. In the medium-large stratum, the cities of Cuiabá (capital, MG, MiW) and Teresina (capital, PI, NoE) and the large cities of Belém (capital, PA, No), Rio de Janeiro (capital, RJ, SoE), and Porto Alegre (capital, RS, So) doubled their expenditure.
The analysis of the health blocks indicates that there was an increase in primary health care spending in all regions of the country. The Southeast, South, and Midwest regions increased more than half of their expenditures. Cities with less than 20,000 inhabitants and large cities were responsible for this increase; the variation of these groups reached 43% and 165%, respectively (
Table 7).
Medium- and high-complexity care contracted in almost all regions, except in the Southeast, an effect caused, in part, by cities with less than 20 thousand inhabitants that do not have such a service. However, others consistently increased their average expenditures, especially in cities with a population between 50 thousand and 500 thousand inhabitants. (
Table 8).
In this analysis, two types of increase in public health coverage were observed. One linked to the benefits of investment growth in the same direction as medium- and high-complexity care, and another with a rather negative profile, in which investments fell alongside an increase in medium- and high-complexity care spending, suggesting unplanned commercialization of public services.
The Northeast and Midwest regions were the areas where the greatest increase in spending was observed, specifically in the medium-large and large city strata, where investment increased by the same amount as medium- and high-complexity care spending. On the contrary, the Southeast region was the prime location for the expansion of the medium- and high-complexity care with steep drops in investment, especially in the small-middle city strata. The Southeast region was the only one to grow above 50% of the average municipal expenses in medium- and high-complexity care, going from BRL 13 million to BRL 21 million.
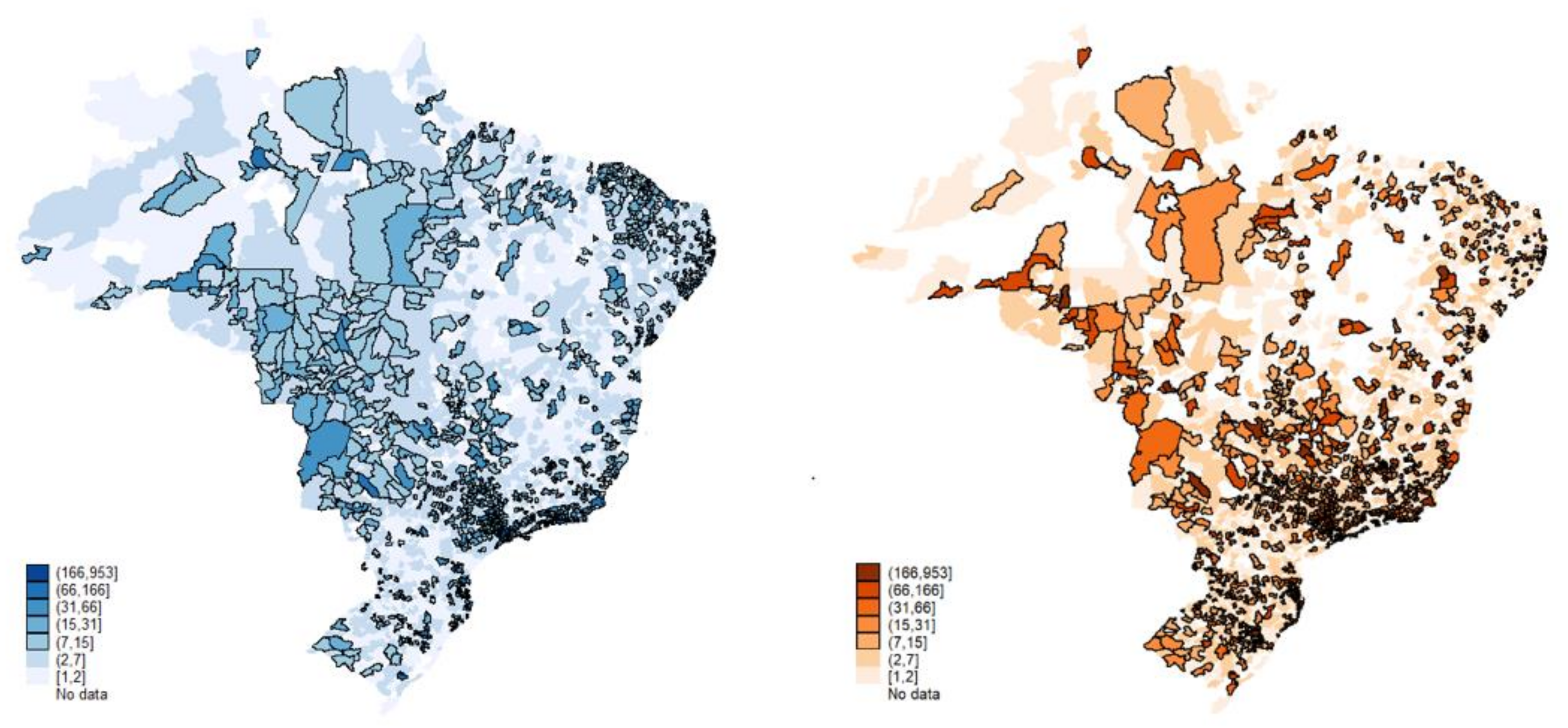
However, the expansion of public spending was largely permitted by the growth of the economy in the period between 2006 and 2014 and the increase of fund-to-fund transfers by the federal government. This has reduced some disparities in the distribution of resources. The years analyzed were marked by the growth of public spending, mainly in primary care and consistently in the strata for medium-/high-complexity care. Without this, perhaps,
Figure 3 would present greater imbalances than those already evident.
3.2. Concentration and Imbalance
The public installed capacity in primary care grew by 8000 units across all regions, with the North and the South growing by 22% and 19%, respectively. Between 2008 and 2015, public supply surpassed the private network in absolute and relative terms, as seen in
Table 9. However, the change is more due to private reduction than an increase in public supply. Negative changes in the private sector averaged 50% in almost all regions, with the Midwest and South regional changes being more pronounced (57% and 55%, respectively). Across all primary care units, the participation of the private sector showed a strong exit trend, falling from 49 thousand to 23 thousand in the period.
In fact, the average number of public primary health care units per municipality increased in all regions of the country. The North and Northeast regions increased by 2 points (9.5–11.5 and 10.2–12.1, respectively), while the private sector registered a consistent average reduction of its establishments, falling from 21.9 to 12.
The data suggest that there has been great progress in the universalization of primary care by SUS. Regionalization expanded in the regions and municipalities identified by the service, especially in small towns (0 to 50 thousand inhabitants). There was also a gradual inclusion of medium-sized urban centers (100 thousand to 500 thousand inhabitants) and the maintenance in absolute terms of the network in large cities (over 1 million inhabitants) with the dispersal of the establishments (
Table 10).
The private sector shows considerable declines, both in absolute and average numbers of primary facilities in all regions and population strata. In almost all regions, falls were above 50%. The only exception was the North region, which already has a small number of primary care units (963 to 870 establishments), with a reduction of approximately 10%.
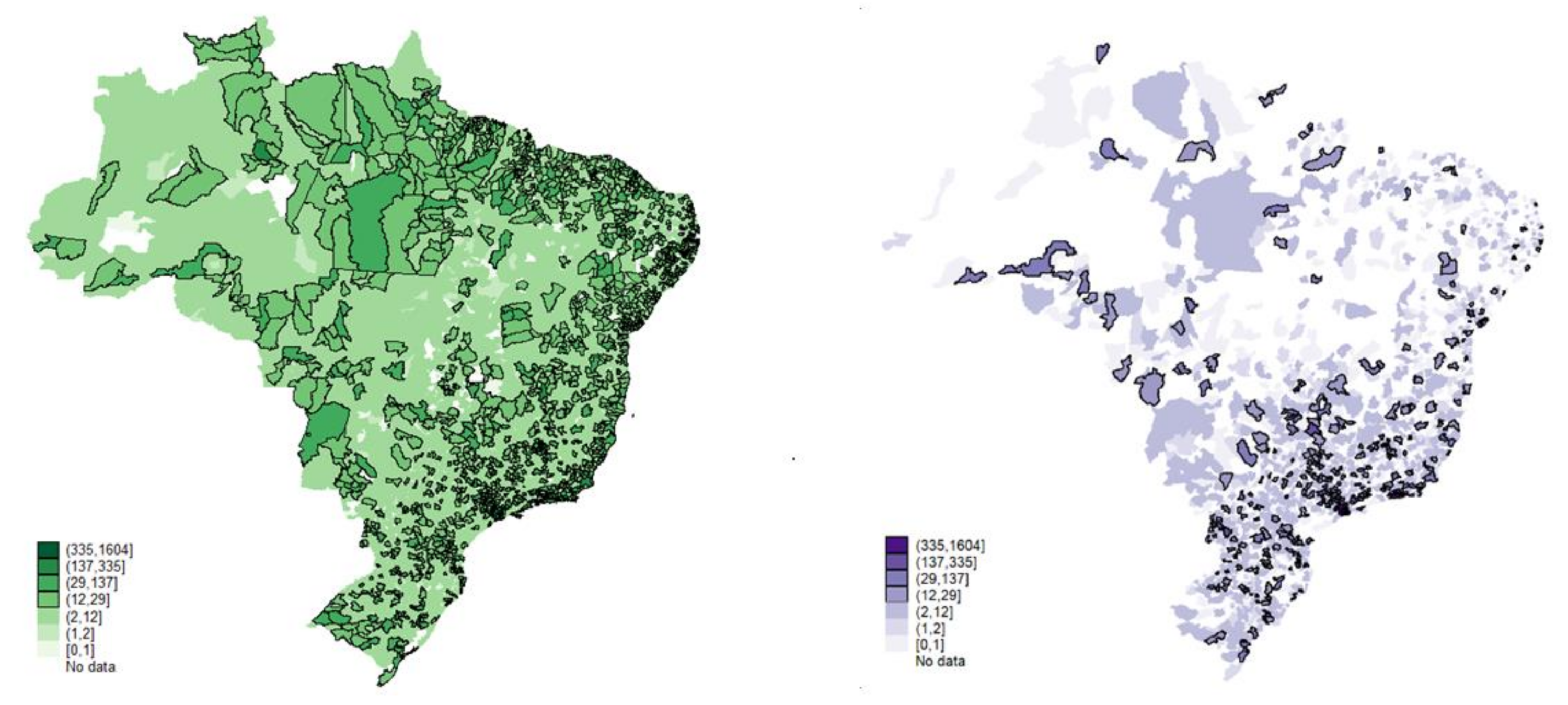
As a result,
Figure 4 shows that 70% of the municipalities (mostly cities with up to 20 thousand inhabitants) have, on average, six public primary health care establishments. The municipalities with up to 50 thousand inhabitants have, on average, 14 units, revealing a greater regional homogenization (the term “regional homogenization” refers to the regional disparity network offering service) of the public installed capacity in primary health care, with the geographic inequalities in health outcomes significantly reducing. The geographical visualization allows us to assert that for primary health care, there was, in fact, almost complete universalization of the installed capacity. The low level of voids in primary health care establishments across the country is a sign of this. There are few localities with public health care gaps.
The private sector, on the contrary, presents considerable geographic gaps. The sector has, on average, two primary establishments in the small towns and six in the municipalities with up to 50 thousand inhabitants. This is in the context of a sharp increase in private health insurance [
19].
The analysis of the evolution of medium-complexity health care in the period (2008–2015) reveals a consistent growth in the installed regional capacity, mainly in the form of emergency care units (UPAs).
Table 11 shows that there was an increase of more than 60% in public medium-complexity health care capacity in all regions. The South and North regions registered more significant expansions in the medium-complexity outpatient health care mode.
This increase in public medium-complexity health care facilities mainly took place in cities with less than 20 thousand inhabitants that expanded their installed capacity by 7696 units, and cities between 20,000 and 50,000 inhabitants, with 3674 new units (
Table 12).
In the medium-complexity hospital care mode, the Midwest region is the main highlight with a significant increase of 135% (M/hosp), followed by the Northeast and North regions with 58% and 53%, respectively. With respect to high-complexity care, public hospital establishments have strongly decreased their presence in almost all regions [
20]. The overall reduction in the high-complexity hospital care mode was 17% (H/hosp) in total. The Northeast and South regions had the highest contractions of 35% and 42%, respectively. The North region was the only one to generate growth of installed capacity in this period. Cities with 500,000 to 1 million inhabitants and those with more than 1 million inhabitants were responsible for reducing the number of high-complexity care hospitals, especially in the Southeast and Northeast regions.
Table 13 shows that the North region had the greatest expansion in the installed capacity of private units for medium-complexity outpatient care, approximately a 60% expansion, followed by the Midwest region with a 10% increase. Similar to the public sector, in absolute terms, small cities with less than 50 thousand inhabitants were the ones that collaborated most in the growth of private installed capacity for medium-complexity care (
Table 14).
The same is true in the high-complexity hospital sphere, which, during 2008–2015, also expanded in absolute and relative terms. The national average growth was 31% (80% in the North region and approximately 50% in the Midwest region). The elevated average of private establishments in almost all modalities in medium- and high-complexity care are the result of imbalances in the network. The analysis of the absolute values in the private sector according to population strata verifies that this expansion was highly concentrated in medium and large cities.
In large cities (above 1 million), the average of private medium-complexity outpatient facilities was eight times higher than the average of the public network (about 20 thousand more units). The network of private medium-complexity care hospitals (M/hosp) also grew in the period, although to a lesser degree to those of high complexity. The North and Midwest regions (36% and 29%, respectively) were the highlights. This expansion was concentrated in small (50,000 to 100,000 inhabitants) and medium-sized cities (100,000 to 500,000 inhabitants). As for high-complexity care (H/hosp), the expansion of the private network was even greater, especially in the North and Southeast regions, whose expansion reached 56% and 17%, respectively.
In summary, the public regionalization of medium-complexity outpatient facilities indicates that there has been decentralized growth in many of the country’s cities, except for the medium-large (500,000 to 1 million) and large (over 1 million) strata, thus covering previously undersupplied regions. The private sector expanded its installed capacity in all modes of medium- and high-complexity care, possibly in a move for higher profit margins.
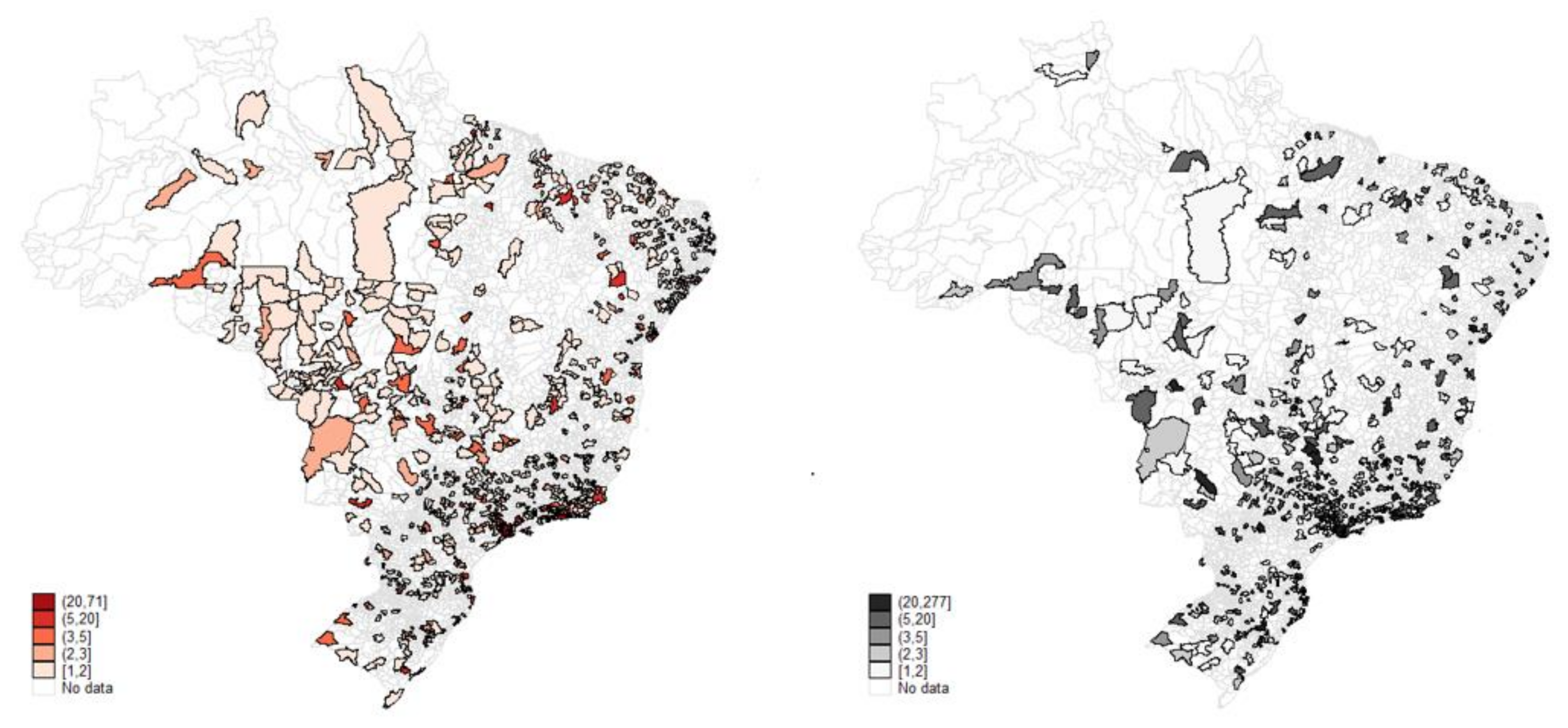
At first glance, the maps (
Figure 5 and
Figure 6) suggest that the two health care sectors appear to operate in the same localities with a slight reduction in private practice in some regions. However, it must be remembered that the private sector serves only 25% of the Brazilian population, while the public covers 75%. On average, the structures are almost equivalent regionally, with the greatest contrast in the high-complexity care mode, where the public covers most of the country’s territory.
3.3. Work in Health
During the analyzed period, SUS expanded human resources across Brazil. One of the constraints of this process was the Family Health Strategy (Estratégia Saúde da Família-ESF, in Portuguese) Program. Between 1998 and 2010, the ESF program grew rapidly from 4000 teams to over 31,600 and was able to expand coverage from 10.6 million to over 100 million registered people [
4].
The Family Health Strategy was inspired by the Community Health Agents Program (Programa de Agentes Comunitários de Saúde-PACS, in Portuguese), a community health initiative piloted in rural areas of Ceará during the 1980s. The Family Health Strategy (ESF) was initially developed in parallel with the PACS, gradually replacing it. It was designed to provide first-contact, comprehensive, and whole-person care coordinated with other health services, emphasizing care that takes place within the context of family and community. In the ESF, multiprofessional health teams (composed of a physician, a nurse, a nurse assistant, and four to six community health workers) are organized by geographic regions, with each team providing primary care to approximately 1,000 families (or about 3500 people) [
4].
Increased federal transfers and the expansion of private insurance also contributed to the expansion of health jobs. Public and private health sector job position offers increased in all regions and population strata, and the public occupational profile became more homogeneous between 2008 and 2015. The standard deviation of occupation for the four analyzed health worker groups in the public sector was almost 60% lower than in the private sector, where the North, Northeast, and South regions presented greater homogeneity. In both public and private segments, the growth in employment did not significantly alter the relative composition of the supply of physicians, nurses, nursing assistants, and technicians, but a larger difference can be observed between the number of nurses, nursing assistants, and technicians in the private sector, in a movement possibly caused by occupational substitution (
Table 15 and
Table 16).
Cities of 0 to 100 thousand inhabitants are largely responsible for the growth in all occupations. The increase in the number employed in the three groups of health professionals (n. assist/tech, nurse, and physician) working in the SUS (136 thousand) was much higher than in the private sphere (23 thousand).
Cities from 0 to 50 thousand inhabitants increased the absolute number of SUS physicians by about 31 thousand, while the private sector created only 539 new jobs. The largest absolute variation in the number of SUS physicians (35,000) was mainly concentrated in the medium-sized cities (100,000 to 500,000 inhabitants), while in the private sector, the expansion was concentrated in cities with more than 1 million inhabitants, with 30,000 more employed (
Table 17 and
Table 18).
In large cities, the increase in the number of SUS physicians, from 105 thousand to 124 thousand, was accompanied by a drop in the average number of these professionals per city, from 7.5 thousand to 6.5 thousand, suggesting an increase in the number of physicians but less geographically concentrated, thus improving geographical distribution. While in the private sector, the increase in the absolute number of occupations of physicians, from 84 thousand to 115 thousand, across the same stratum suggests a higher concentration of professionals, which increased from 6000 to 8200, that is, the public system is expanding supply in all regions of the country, especially in medium-sized cities, while the private sector is more concentrated in large cities.
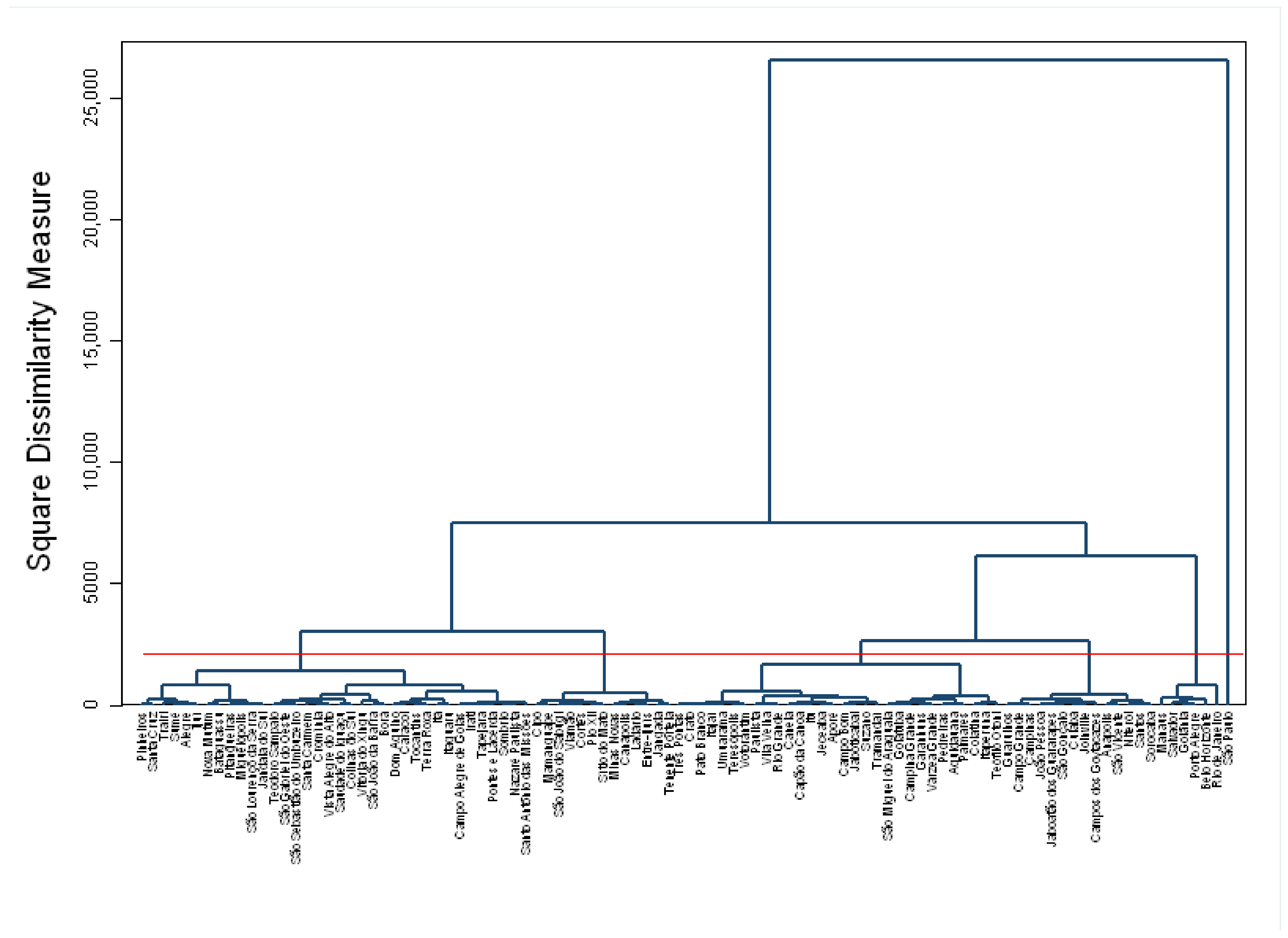
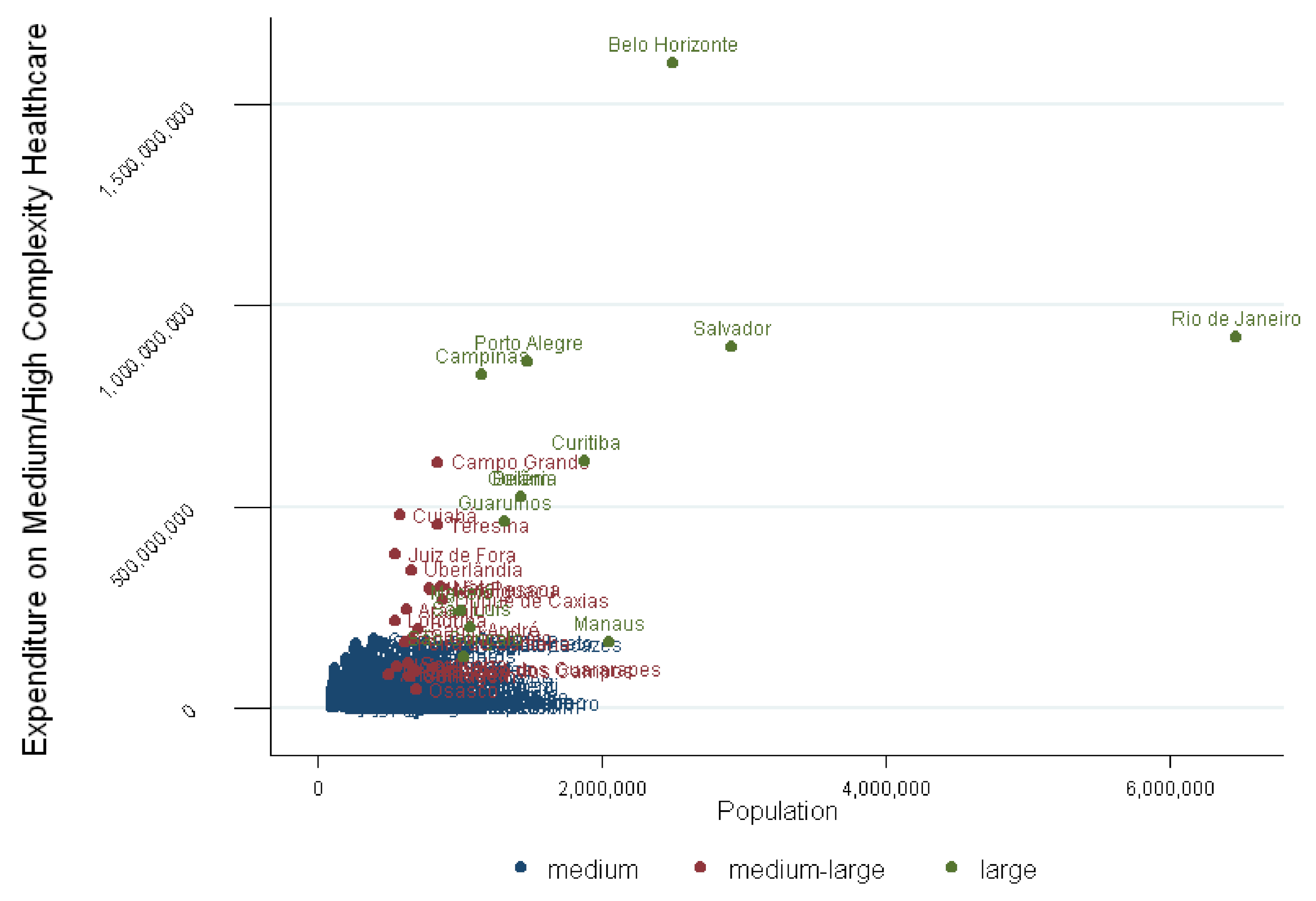
3.4. Cluster Analysis
The SUS clusters reveal a parallel with prevailing regional health theory, according to which the process of regionalization is still in its first steps and facing a serious persistence of gaps in medium- and high-complexity care, in addition to the concentration of full installed capacity in just a few cities. From cluster analysis, we found four groups (
Table 19,
Table 20,
Table 21 and
Table 22).
The concentration of installed capacity, which conditions and reflects the access flows to the health network, shows the Southeast region, excluding Espírito Santo, to be extremely dense, along with the cities of Belo Horizonte, São Paulo, and Rio de Janeiro. They invest almost twice the financial resources of the “central cities” cluster, 90% more than the “medium cities” cluster and 40% more than the “small cities” cluster.
The Southeast group’s average spending is BRL 1.5 billion, against BRL 124 million, BRL 31 million, and BRL 5 million in the “central cities”, “medium cities”, and “small towns” groups, respectively. Even with the clearly planned and rational objective of achieving economies of scale, the results indicate that a strong and persistent concentration of the network is still to be found in a small group of cities.
In quantitative terms, the average number of high-complexity outpatient clinics in Belo Horizonte (capital, MG, SoE), São Paulo (capital, SP, SoE), and Rio de Janeiro (capital, RJ, SoE) is four times higher than the central cities group. In this respect, the issue does not necessarily adhere to the logic of the system but rather is disproportionate, because as the technological density of the coverage decreases, the average number and the dispersal of services increases.
Almost every state in Brazil connects to the southeastern region, especially São Paulo, for access to the most complex care services. For myocardial revascularization, only the states of Ceará and Rio Grande do Sul are relatively autonomous. Flowing in the opposite direction and due to extreme isolation, the inhabitants of Rondônia travel to all regions of the country seeking treatment—the flows go from the State of Pará (No), through Rio Grande do Norte (NoE), Goiás (MiW) and São Paulo (SoE) and arrive as far away as Paraná (So) [
21].
Moreover, alongside the significant concentration of high-complexity care, the heterogeneity of SUS installed capacity is yet another point that needs to be improved. The k-means reveals that 3243 municipalities did not belong to any group at all, suggesting strong heterogeneity in the distribution of the SUS public offering capacity.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}