
Psychometric Properties of the Health Literacy Scale Used in the Taiwan Longitudinal Study on Middle-Aged and Older People


Abstract
:1. Introduction
1.1. Introduction to the Available Health Literacy Scales
1.1.1. Objective Health Literacy Scales
1.1.2. Subjective Health Literacy Scales
1.1.3. Taiwan Health Literacy Scale
1.2. Research Questions and Purposes
2. Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. TLSA Health Literacy Scale
2.2.2. Instrumental Activities of Daily Living (IADL) Scale
2.2.3. Life Satisfaction Index
2.2.4. Self-Rated Health
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic Status and TLSA Health Literacy Scores of the Participants
3.2. Reliability
3.3. Validity
3.3.1. Criterion Validity
3.3.2. Construct Validity
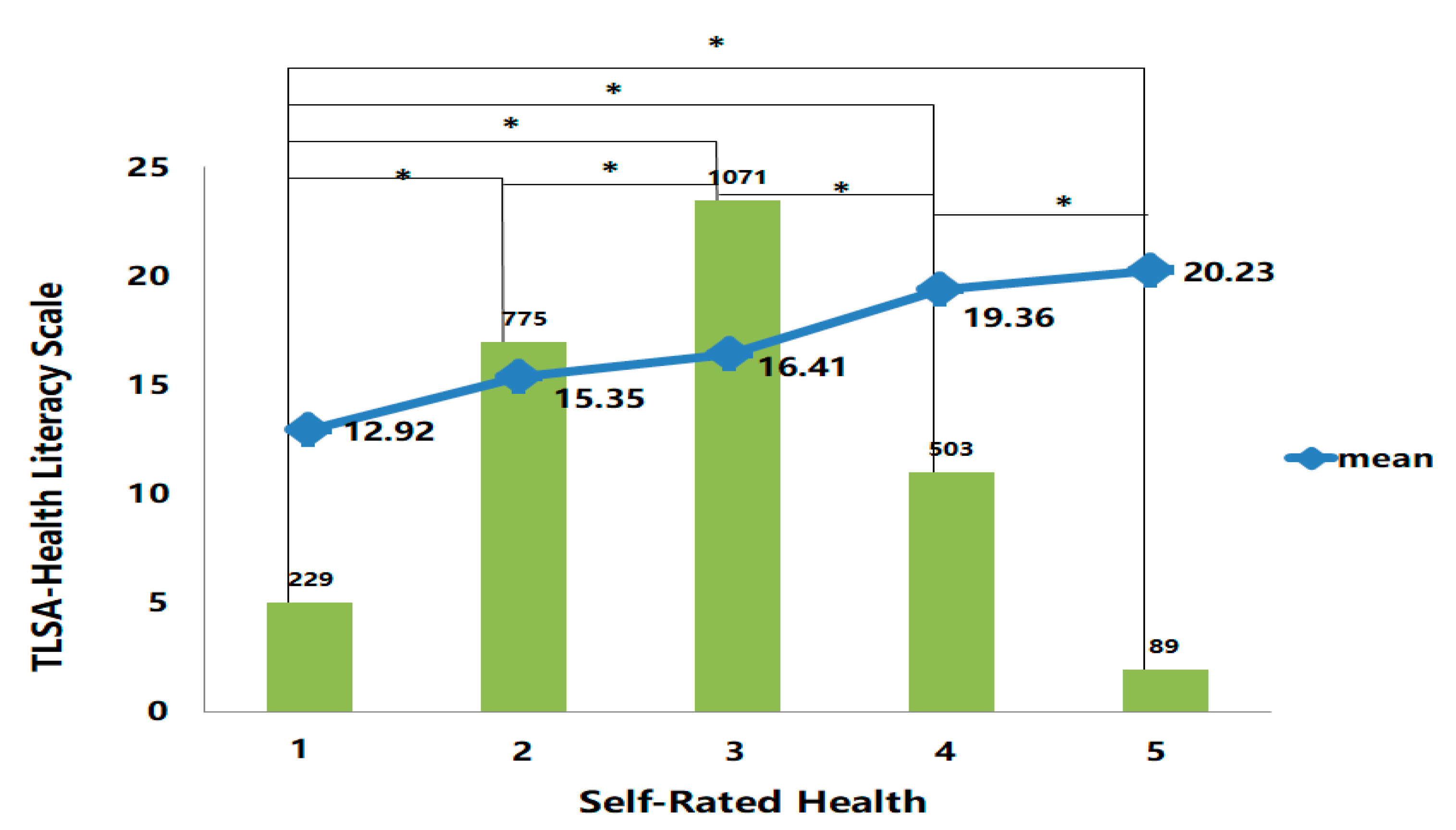
3.3.3. Known-Group Validity
4. Discussion
4.1. Participant Characteristics and the TLSA Health Literacy Scale
4.2. Reliability of the TLSA Health Literacy Scale
4.3. Validity of TLSA Health Literacy Scale
4.3.1. Criterion Validity
4.3.2. Construct Validity
4.3.3. Known-Group Validity
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- National Health Research Institutes Forum. The Determinates of Health Literacy and Related Health Outcomes Among Elders in Taiwan; National Health Research Institutes & Ministry of Health and Welfare: Taipei, Taiwan, 2019; pp. 1–195. [Google Scholar]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, T.C.; Long, S.W.; Jackson, R.H.; Mayeaux, E.; George, R.B.; Murphy, P.W.; Crouch, M.A. Rapid estimate of adult literacy in medicine: A shortened screening instrument. Fam. Med. 1993, 25, 391. [Google Scholar] [PubMed]
- Williams, M.V.; Parker, R.M.; Baker, D.W.; Parikh, N.S.; Pitkin, K.; Coates, W.C.; Nurss, J.R. Inadequate functional health literacy among patients at two public hospitals. JAMA 1995, 274, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.M.; Baker, D.W.; Williams, M.V.; Nurss, J.R. The test of functional health literacy in adults. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef]
- Baker, D.W.; Williams, M.V.; Parker, R.M.; Gazmararian, J.A.; Nurss, J. Development of a brief test to measure functional health literacy. Patient Educ. Couns. 1999, 38, 33–42. [Google Scholar] [CrossRef]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the european health literacy survey questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinn, D.; McCarthy, C. All aspects of health literacy scale (AAHLS): Developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ. Couns. 2013, 90, 247–253. [Google Scholar] [CrossRef]
- Dowse, R. The limitations of current health literacy measures for use in developing countries. J. Commun. Healthc. 2016, 9, 4–6. [Google Scholar] [CrossRef]
- Lin, C.W. Validation and implication for the Chinese version of the newest vital sign health literacy scale: A case study of pre-service early childhood teachers. J. Health Promot. Health Educ. Contents 2010, 34, 1–34. [Google Scholar]
- Duong, V.T.; Lin, I.-F.; Sorensen, K.; Pelikan, J.M.; Van den Broucke, S.; Lin, Y.-C.; Chang, P.W. Health literacy in Taiwan: A population-based study. Asia Pac. J. Public Health 2015, 27, 871–880. [Google Scholar] [CrossRef]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Mohamad, E.; Su, T.T. Measuring health literacy in Asia: Validation of the HLS-EU-Q47 survey tool in six Asian countries. J. Epidemiol. 2017, 27, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Su, C.L.; Chang, S.F.; Chen, R.C.; Pan, F.C.; Chen, C.H.; Liu, W.W. A preliminary study of Taiwan health literacy scale (THLS). Formos. J. Med. 2008, 12, 525–536. [Google Scholar]
- Tsai, T.I.; Lee, S.Y.D.; Tsai, Y.W.; Kuo, K.N. Development and validation of mandarin health literacy scale. J. Med. Educ. 2010, 14, 122–136. [Google Scholar]
- Wei, M.H.; Wang, Y.W.; Chang, M.C.; Hsieh, J.G. Development of mandarin multidimensional health literacy questionnaire (MMHLQ). Taiwan J. Public Health 2017, 36, 556–570. [Google Scholar]
- Pleasant, A.; McKinney, J. Coming to consensus on health literacy measurement: An online discussion and consensus-gauging process. Nurs. Outlook 2011, 59, 95–106. [Google Scholar] [CrossRef]
- Health Promotion Administration, Ministry of Health and Welfare. 2015 Taiwan longitudinal study on aging survey report. Taiwan Aging Study Ser. 2018, 13, 1–258. [Google Scholar]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Lee, K.-L.; Ou, Y.-L.; Chen, S.-H.; Weng, L.-J. The psychometric properties of a short form of the ces-d used in the taiwan longitudinal study on aging. J. Ment. Health 2009, 22, 383–410. [Google Scholar]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 16, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Do, B.N.; Nguyen, P.A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of health literacy and its associations with health-related behaviors, depression among the older people with and without suspected covid-19 symptoms: A multi-institutional study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.B.; Liu, L.; Li, Y.F.; Chen, Y.L. Relationship between health literacy, health-related behaviors and health status: A survey of elderly Chinese. Int. J. Environ. Res. Public Health 2015, 12, 9714–9725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protheroe, J.; Whittle, R.; Bartlam, B.; Estacio, E.V.; Clark, L.; Kurth, J. Health literacy, associated lifestyle and demographic factors in adult population of an English city: A cross-sectional survey. Health Expect. 2017, 20, 112–119. [Google Scholar] [CrossRef]
- Yang, Q.; Yu, S.; Wang, C.; Gu, G.; Yang, Z.; Liu, H.; Lin, L.; Qiao, Y.; Yu, L.; Feng, Q.; et al. Health literacy and its socio-demographic risk factors in Hebei: A cross-sectional survey. Medicine 2021, 100, e25975. [Google Scholar] [CrossRef]
- Thapa, S.; Nielsen, J.B. Association between health literacy, general psychological factors, and adherence to medical treatment among danes aged 50–80 years. BMC Geriatr. 2021, 21, 386. [Google Scholar] [CrossRef]
- Leist, A.K.; Bar-Haim, E.; Chauvel, L. Inequality of educational opportunity at time of schooling predicts cognitive functioning in later adulthood. SSM Popul. Health 2021, 15, 100837. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.D.; Arozullah, A.M.; Cho, Y.I.; Crittenden, K.; Vicencio, D. Health literacy, social support, and health status among older adults. Educ. Gerontol. 2009, 35, 191–201. [Google Scholar] [CrossRef]
- Vogt, D.; Schaeffer, D.; Messer, M.; Berens, E.-M.; Hurrelmann, K. Health literacy in old age: Results of a german cross-sectional study. Health Promot. Int. 2018, 33, 739–747. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Kivimaki, M.; Glymour, M.M.; Elbaz, A.; Berr, C.; Ebmeier, K.P.; Ferrie, J.E.; Dugravot, A. Timing of onset of cognitive decline: Results from Whitehall II prospective cohort study. Br. Med. J. 2012, 344, d7622. [Google Scholar] [CrossRef] [Green Version]
- Statsenko, Y.; Habuza, T.; Charykova, I.; Gorkom, K.N.; Zaki, N.; Almansoori, T.M.; Baylis, G.; Ljubisavljevic, M.; Belghali, M. Predicting age from behavioral test performance for screening early onset of cognitive decline. Front. Aging Neurosci. 2021, 13, 661514. [Google Scholar] [CrossRef] [PubMed]
- Eronen, J.; Paakkari, L.; Portegijs, E.; Saajanaho, M.; Rantanen, T. Assessment of health literacy among older Finns. Aging Clin. Exp. Res. 2019, 31, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Bozkurt, H.; Demirci, H. Health literacy among older persons in Turkey. Aging Male 2019, 22, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Uemura, K.; Yamada, M.; Okamoto, H. Effects of active learning on health literacy and behavior in older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2018, 66, 1721–1729. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.S.; Feinglass, J.; Thompson, J.; Baker, D.W. In search of ‘low health literacy’: Threshold vs. Gradient effect of literacy on health status and mortality. Soc. Sci. Med. 2010, 70, 1335–1341. [Google Scholar] [CrossRef]
- McDougall Jr, G.J.; Mackert, M.; Becker, H. Memory performance, health literacy, and instrumental activities of daily living of community residing older adults. Nurs. Res. 2012, 61, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancuso, J.M. Assessment and measurement of health literacy: An integrative review of the literature. Nurs. Health Sci. 2009, 11, 77–89. [Google Scholar] [CrossRef]
- Kaučič, B.M.; Ovsenik, M.; Filej, B. Is the holistic physical factor linked to life satisfaction in older age? Med. Pr. 2019, 70, 535–543. [Google Scholar] [CrossRef]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Baker, D.W.; Parker, R.M.; Williams, M.V.; Clark, W.S.; Nurss, J. The relationship of patient reading ability to self-reported health and use of health services. Am. J. Public Health 1997, 87, 1027–1030. [Google Scholar] [CrossRef] [Green Version]
- Suka, M.; Odajima, T.; Okamoto, M.; Sumitani, M.; Igarashi, A.; Ishikawa, H.; Kusama, M.; Yamamoto, M.; Nakayama, T.; Sugimori, H. Relationship between health literacy, health information access, health behavior, and health status in Japanese people. Patient Educ. Couns. 2015, 98, 660–668. [Google Scholar] [CrossRef]
- Murali, K.; Mullan, J.; Roodenrys, S.; Lonergan, M. Comparison of health literacy profile of patients with end-stage kidney disease on dialysis versus non-dialysis chronic kidney disease and the influencing factors: A cross-sectional study. BMJ Open 2020, 10, e041404. [Google Scholar] [CrossRef]
- Schillinger, D.; Grumbach, K.; Piette, J.; Wang, F.; Osmond, D.; Daher, C.; Palacios, J.; Sullivan, G.D.; Bindman, A.B. Association of health literacy with diabetes outcomes. JAMA 2002, 288, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Viera, A.; Crotty, K.; Holland, A.; Brasure, M.; Lohr, K.N.; Harden, E. Health literacy interventions and outcomes: An updated systematic review. Evid. Rep. Technol. Assess Full Rep. 2011, 199, 941. [Google Scholar]


{kind=link}
| Variable. | n | % | Total | HC | HP | DP | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |||
| Age | ||||||||||
| 50–64 | 584 | 21.90 | 13.73 | 4.69 | 1.27 | 0.52 | 1.95 | 0.88 | 1.40 | 0.60 |
| 65–85+ | 2083 | 78.10 | 17.26 | 6.61 | 1.78 | 0.87 | 2.36 | 1.00 | 1.54 | 0.70 |
| Gender | ||||||||||
| Male | 1302 | 48.80 | 15.44 | 5.87 | 1.48 | 0.71 | 2.18 | 0.96 | 1.50 | 0.70 |
| Female | 1365 | 51.20 | 17.49 | 6.73 | 1.85 | 0.90 | 2.35 | 1.01 | 1.51 | 0.66 |
| Education | ||||||||||
| Primary or junior high school | 2037 | 76.40 | 17.80 | 6.43 | 1.83 | 0.87 | 2.45 | 0.97 | 1.56 | 0.70 |
| High school or university and above | 630 | 23.60 | 12.25 | 4.08 | 1.16 | 0.41 | 1.66 | 0.76 | 1.32 | 0.58 |
| HL | 2667 | 100.00 | 16.49 | 6.40 | 1.67 | 0.83 | 2.26 | 0.99 | 1.51 | 0.68 |
| IADL | 2667 | 100.00 | 4.33 | 8.18 | - | - | - | - | - | - |
| Life Satisfaction Index | 2667 | 100.00 | 7.28 | 2.33 | - | - | - | - | - | - |
| Self-rated Health | 2667 | 100.00 | 2.89 | 1.01 | - | - | - | - | - | - |
| No. | Items | Factor Loading | ||
|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | ||
| Eigenvalue | 4.41 | 1.11 | 1.02 | |
| Variance % | 44.85 | 7.89 | 6.83 | |
| 2 | When you go to the doctor, can you understand the content or suggestions of the medical staff on the condition or medical treatment? | 0.92 | ||
| 1 | When you seek medical treatment, are you able to clearly express or explain your condition to the medical staff serving you? | 0.82 | ||
| 3 | Can you read the medication instructions on the medicine bag or understand the medication instructions given by the doctor? | 0.74 | ||
| 9 | When you are under pressure, do you know how to find a way to reduce it? | 0.79 | ||
| 8 | Did you know that you have to exercise 3 times a week, and each time it takes more than 30 min? | 0.74 | ||
| 5 | Can you understand the leaflets or explanatory materials given to you by the hospital on self-control or disease care? | 0.71 | ||
| 7 | Will you choose foods that are good for your health? | 0.58 | ||
| 6 | Do you usually follow the instructions given to you by the medical staff to control the condition yourself? | 0.86 | ||
| 4 | Will you follow the medication instructions (such as punctuality and dosage) given to you by your doctor? | 0.64 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, Y.-L.; Hsieh, C.-J.; Li, P.-S.; Liu, C.-Y. Psychometric Properties of the Health Literacy Scale Used in the Taiwan Longitudinal Study on Middle-Aged and Older People. Healthcare 2021, 9, 1391. https://doi.org/10.3390/healthcare9101391
Shih Y-L, Hsieh C-J, Li P-S, Liu C-Y. Psychometric Properties of the Health Literacy Scale Used in the Taiwan Longitudinal Study on Middle-Aged and Older People. Healthcare. 2021; 9(10):1391. https://doi.org/10.3390/healthcare9101391
Chicago/Turabian StyleShih, Ya-Ling, Chia-Jung Hsieh, Pei-Shan Li, and Chieh-Yu Liu. 2021. "Psychometric Properties of the Health Literacy Scale Used in the Taiwan Longitudinal Study on Middle-Aged and Older People" Healthcare 9, no. 10: 1391. https://doi.org/10.3390/healthcare9101391
APA StyleShih, Y.-L., Hsieh, C.-J., Li, P.-S., & Liu, C.-Y. (2021). Psychometric Properties of the Health Literacy Scale Used in the Taiwan Longitudinal Study on Middle-Aged and Older People. Healthcare, 9(10), 1391. https://doi.org/10.3390/healthcare9101391