
The Role of a Physician-Staffed Helicopter in Emergency Care of Patients on Isolated Danish Islands


Abstract
:1. Background
2. Material and Methods
2.1. Study Design
2.2. Operational Setting
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afzali, M.; Hesselfeldt, R.; Steinmetz, J.; Thomsen, A.B.; Rasmussen, L.S. A helicopter emergency medical service may allow faster access to highly specialised care. Dan. Med. J. 2013, 60, 1. [Google Scholar]
- Andersen, M.S.; Johnsen, S.P.; Sørensen, J.N.; Jepsen, S.B.; Hansen, J.B.; Christensen, E.F. Implementing a Nationwide Criteria-Based Emergency Medical Dispatch System: A Register-Based Follow-up Study. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrew, E.; De Wit, A.; Meadley, B.; Cox, S.; Bernard, S.; Smith, K. Characteristics of Patients Transported by a Paramedic-staffed Helicopter Emergency Medical Service in Victoria, Australia. Prehospital Emerg. Care 2015, 19, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Langhelle, A.; Lossius, H.M.; Silfvast, T.; Björnsson, H.M.; Lippert, F.; Ersson, A.; Søreide, E. International EMS Systems: The Nordic countries. Resuscitation 2004, 61, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Hesselfeldt, R.; Pedersen, F.; Steinmetz, J.; Vestergaard, L.; Simonsen, L.; Jørgensen, E.; Clemmensen, P.; Rasmus, H. Implementation of a physician-staffed helicopter: Impact on time to primary PCI. EuroIntervention 2013, 9, 477–483. [Google Scholar] [CrossRef] [PubMed]
- The Regions Emergency Medical Helicopter Annual Report 2016. Available online: https://www.akutlaegehelikopter.dk/en/ (accessed on 1 September 2020).
- Population 1. January by Islands and Time, Statistics Denmark. Available online: https://www.statistikbanken.dk/statbank5a/selectvarval/saveselections.asp?MainTable=BEF4&PLanguage=1&TableStyle=&Buttons=&PXSId=2020101693738300223344BEF4&IQY=&TC=&ST=ST&rvar0=&rvar1=&rvar2=&rvar3=&rvar4=&rvar5=&rvar6=&rvar7=&rvar8=&rvar9=&rvar10=&rvar11= (accessed on 16 October 2020).
- Alstrup, K.; Møller, T.P.; Knudsen, L.; Hansen, T.M.; Petersen, J.A.K.; Rognås, L.; Barfod, C. Characteristics of Patients Treated by the Danish Helicopter Emergency Medical Service from 2014–2018: A Nationwide Population-Based Study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 102. [Google Scholar] [CrossRef] [PubMed]
- Kornhall, D.; Näslund, R.; Klingberg, C.; Schiborr, R.; Gellerfors, M. The mission characteristics of a newly implemented rural helicopter emergency medical service. BMC Emerg. Med. 2018, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurola, J.; Wangel, M.; Uusaro, A.; Ruokonen, E. Paramedic helicopter emergency service in rural Finland—Do benefits justify the cost? Acta Anaesthesiol. Scand. 2002, 46, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Alstrup, K.; Petersen, J.A.K.; Barfod, C.; Knudsen, L.; Rognås, L.; Møller, T.P. The Danish Helicopter Emergency Medical Service Database: High Quality Data with Great Potential. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The Injury Severity Score: A Method for Describing Patients with Multiple Injuries and Evaluating Emergency Care. J. Trauma 1974, 14, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Fjaeldstad, A.; Kirk, M.H.; Knudsen, L.; Bjerring, J.; Christensen, E.F. Physician-staffed emergency helicopter reduces transportation time from alarm call to highly specialized centre. Dan. Med. J. 2013, 60, 1–5. [Google Scholar]
- Funder, K.S.; Rasmussen, L.S.; Lohse, N.; Hesselfeldt, R.; Siersma, V.; Gyllenborg, J.; Wulffeld, S.; Hendriksen, O.M.; Lippert, F.K.; Steinmetz, J. The impact of a physician-staffed helicopter on outcome in patients admitted to a stroke unit: A prospective observational study. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funder, K.S.; Rasmussen, L.S.; Siersma, V.; Lohse, N.; Hesselfeldt, R.; Pedersen, F.; Hendriksen, O.M.; Steinmetz, J. Helicopter vs. ground transportation of patients bound for primary percutaneous coronary intervention. Acta Anaesthesiol. Scand. 2018, 62, 568–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Møller, T.P.; Kjærulff, T.M.; Viereck, S.; Østergaard, D.; Folke, F.; Ersbøll, A.K.; Lippert, F.K. The difficult medical emergency call: A register-based study of predictors and outcomes. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjertestop Uden for Hospital i Danmark 2016. Available online: https://genoplivning.dk/wp-content/uploads/2018/04/Dansk_Hjertestopregister2016.pdf (accessed on 17 September 2020).
- Walter, S.; Fassbender, K.; Easton, D.; Schwarz, M.; Gardiner, F.W.; Langenberg, F.; Dos Santos, A.; Bil, C.; Fox, K.; Bishop, L.; et al. Stroke care equity in rural and remote areas—Novel strategies. Vessel. Plus 2021, 27, 1–10. [Google Scholar] [CrossRef]
- Gardiner, F.W.; Bishop, L.; Dos Santos, A.; Sharma, P.; Easton, D.; Quinlan, F.; Churilov, L.; Schwarz, M.; Walter, S.; Fassbender, K.; et al. Aeromedical Retrieval for Stroke in Australia. Cerebrovasc. Dis. 2020, 49, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Lindskou, T.A.; Mikkelsen, S.; Christensen, E.F.; Hansen, P.A.; Jørgensen, G.; Hendriksen, O.M.; Kirkegaard, H.; Berlac, P.A.; Søvsø, M.B. The Danish prehospital emergency healthcare system and research possibilities. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Numbers (n) with % or 95% CI, Medians with IQR | PS-HEMS | Ambulance | Other |
|---|---|---|---|
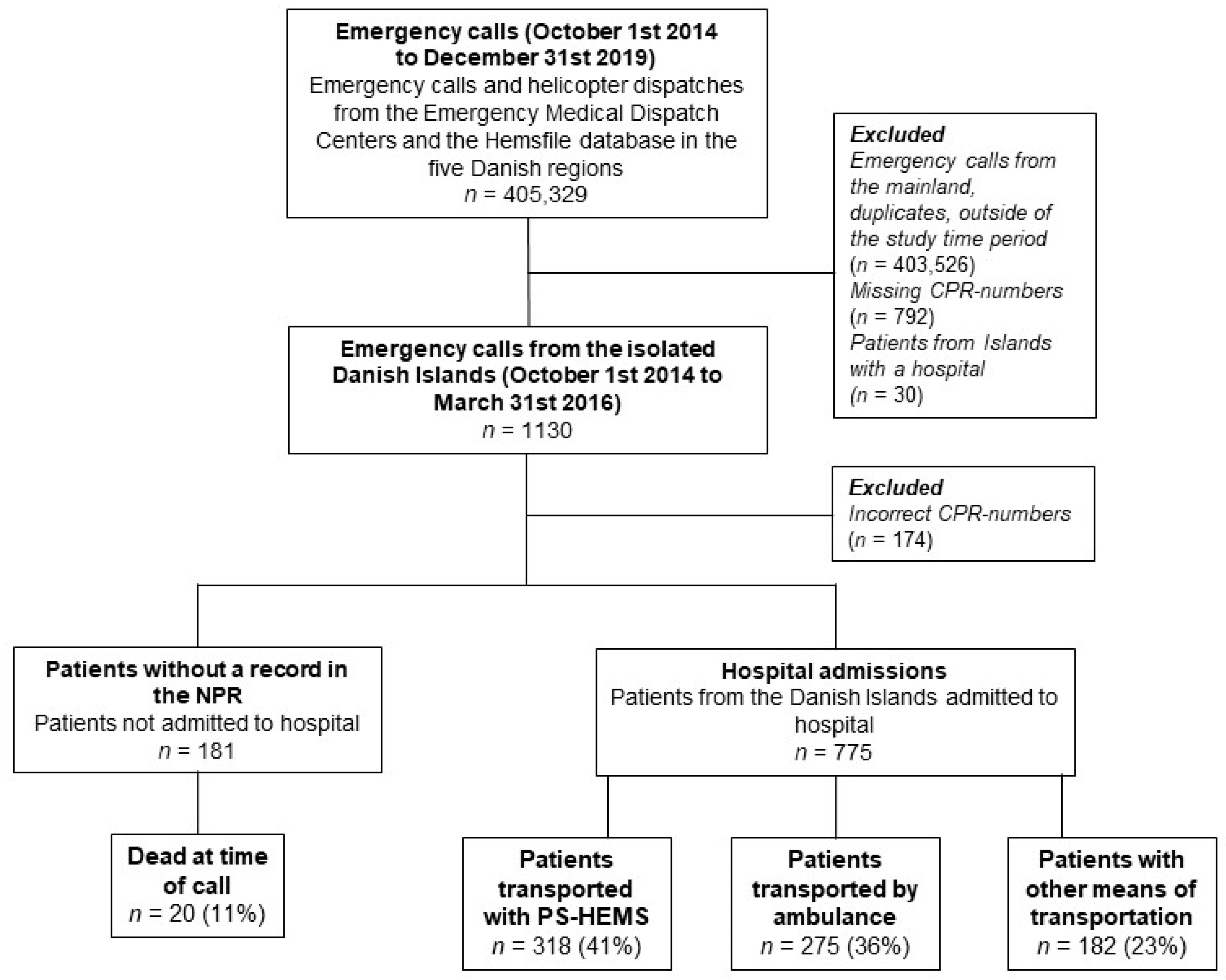
| Patient contacts, n (%) | 318 (41%) | 275 (36%) | 182 (23%) |
| Males, n (%) | 193 (61%) | 171 (62%) | 87 (48%) |
| Age, years, median (IQR) | 66 (52–74) | 66 (27–78) | 61 (41–75) |
| 30-day mortality, n (%, 95% CI) | 22 (6.9%, 95% CI: 4.4–10.3%) | 16 (5.8%, 95% CI: 3.4–9.3%) | 10 (5.5%, 95% CI: 2.7–9.9%) |
| 90-day mortality, n (%, 95% CI) | 31 (9.8%, 95% CI: 6.7–13.5%) | 23 (8.4%, 95% CI: 5.4–12.3%) | 14 (7.7%, 95% CI: 4.3–12.6%) |
| Time interval from emergency medical system dispatch to arrival at initial hospital, median in minutes (IQR) | 83 (66–104) | 90 (45–144) | 399 (196–665) |
| Diagnoses, n(%) | |||
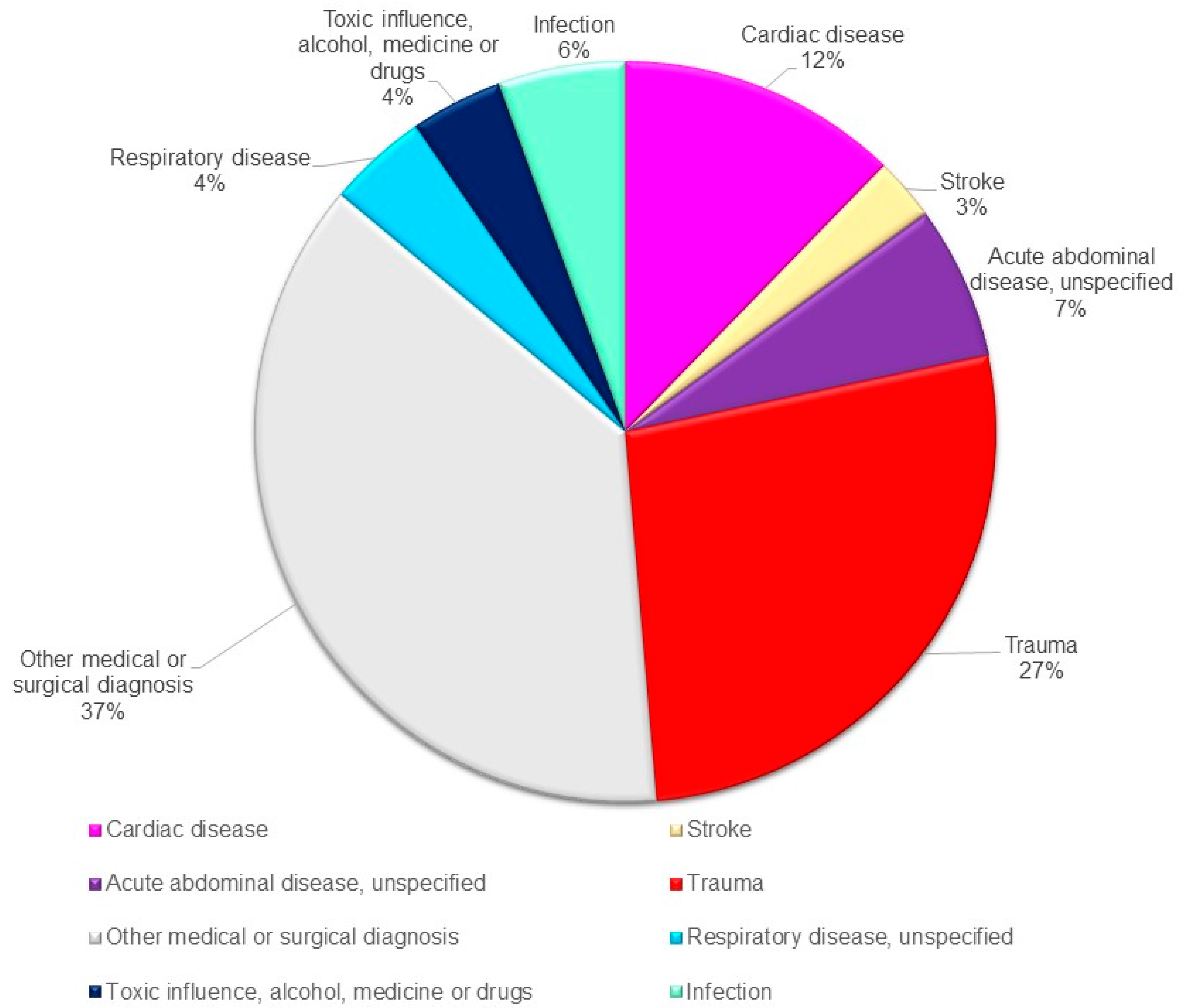
| Cardiac disease | 57 (18%) | 24 (9%) | 14 (8%) |
| CNS related conditions | 30 (9%) | 33 (11%) | 25 (14%) |
| Trauma | 70 (22%) | 86 (31%) | 53 (29%) |
| Acute abdominal disease, unspecified | 22 (7%) | 22 (8%) | 8 (4%) |
| Infection | 19 (6%) | 11 (4%) | 13 (7%) |
| Respiratory disease | 14 (4%) | 8 (3%) | 12 (7%) |
| Alcohol intoxication | 1 (0%) | 10 (4%) | 8 (4%) |
| Other medical diagnoses | 27 (8%) | 18 (7%) | 10 (5%) |
| Other, unspecified | 78 (25%) | 63 (23%) | 39 (21%) |
| Acute Cardiac Disease | Stroke | Trauma | ||||
|---|---|---|---|---|---|---|
| Patients, n (%) HEMS (N = 318) Ambulance and other (N = 457) | 95 57 (18%) 38 (8%) | p = 0.001 | 21 14 (4%) 7 (2%) | p = 0.02 | 209 70 (22%) 139 (30%) | p = 0.01 |
| Age, years, median (IQR) | 68 (57–75) | 72 (61–77) | 56 (25–71) | |||
| HEMS: time to admission, minutes (IQR) | 56 (30–94) | p = 0.6 | 78 (64–86) | p = 0.6 | 84 (75–109) | p = 0.4 |
| Ground ambulance: time to admission, minutes (IQR) | 50 (26–89) | 79 (56–80) | 82 (45–186) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrlin Jensen, A.; Sonne, A.; Rasmussen, L.S. The Role of a Physician-Staffed Helicopter in Emergency Care of Patients on Isolated Danish Islands. Healthcare 2021, 9, 1446. https://doi.org/10.3390/healthcare9111446
Herrlin Jensen A, Sonne A, Rasmussen LS. The Role of a Physician-Staffed Helicopter in Emergency Care of Patients on Isolated Danish Islands. Healthcare. 2021; 9(11):1446. https://doi.org/10.3390/healthcare9111446
Chicago/Turabian StyleHerrlin Jensen, Alice, Asger Sonne, and Lars S. Rasmussen. 2021. "The Role of a Physician-Staffed Helicopter in Emergency Care of Patients on Isolated Danish Islands" Healthcare 9, no. 11: 1446. https://doi.org/10.3390/healthcare9111446