
Change Management and Digital Innovations in Hospitals of Five European Countries

 , , and
, , and
Abstract
1. Introduction
Setting the Scene of Change Management Analysis in Healthcare
2. Materials and Methods
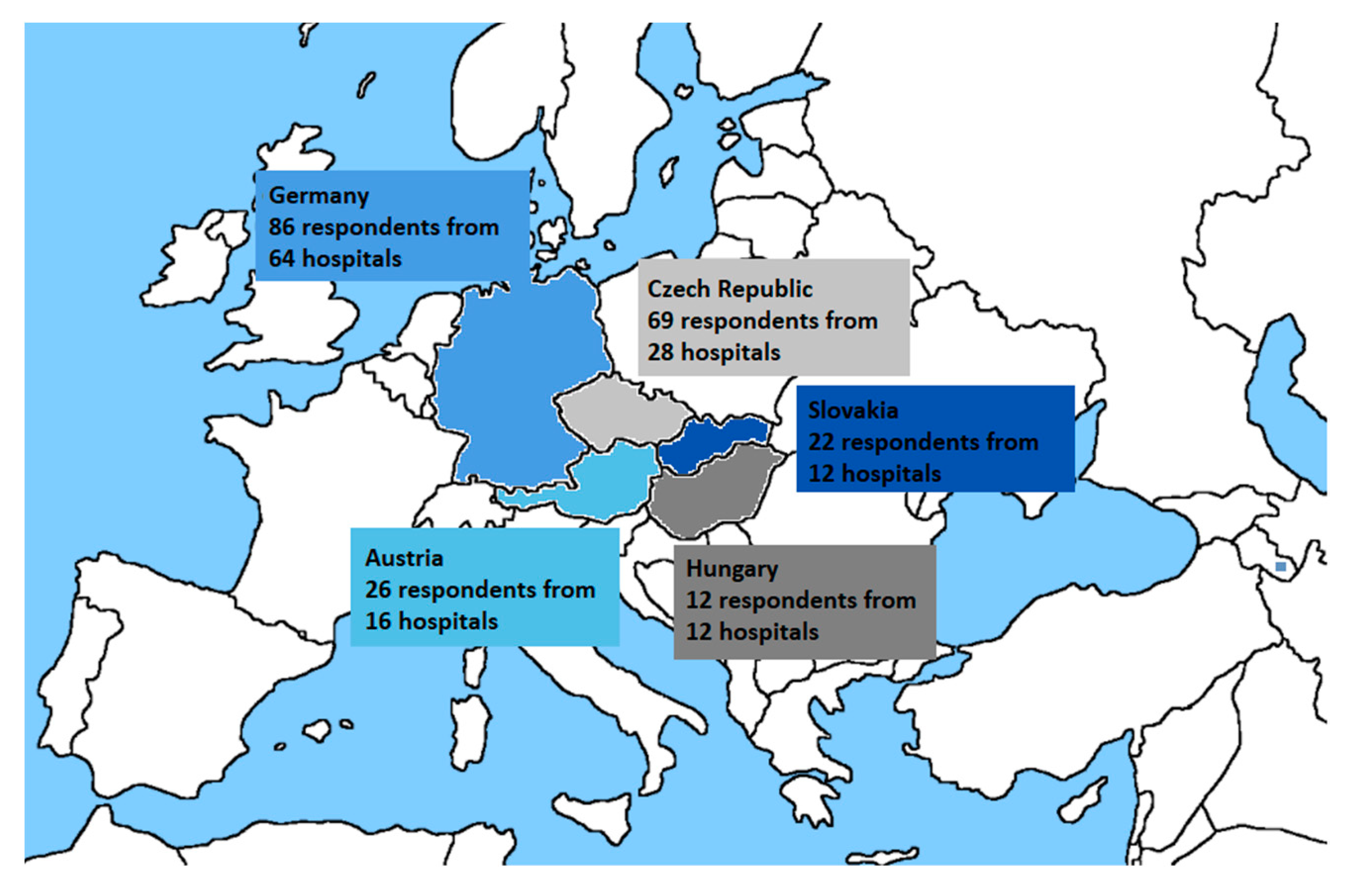
2.1. Questionnaire Survey
2.2. Systematic Review
3. Results
3.1. Questionnaire
3.1.1. Finding 1 (Research Question No. 1)
3.1.2. Finding 2 (Research Question No. 2)
3.1.3. Finding 3 (Research Question No. 3)
3.1.4. Finding 4 (Research Question No. 4)
3.1.5. Finding 5 (Research Question No. 5)
3.1.6. Finding 6 (Research Question No. 6)
3.2. Systematic Review
Finding 7 (Research Question No. 7)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nilsen, P.; Seing, I.; Ericsson, C.; Birken, S.A.; Schildmeijer, K. Characteristics of successful changes in health care organizations: An interview study with physicians, registered nurses and assistant nurses. BMC Health Serv. Res. 2020, 20, 147. [Google Scholar] [CrossRef]
- Moran, J.W.; Brightman, B.K. Leading organizational change. J. Workplace Learn. 2000, 12, 66–74. [Google Scholar] [CrossRef]
- Burnes, B. Emergent change and planned change-Competitors or allies? The case of XYZ construction. Int. J. Oper. Prod. Manag. 2004, 24, 886–902. [Google Scholar] [CrossRef]
- Lexa, F.J. Profiles in Leadership: What Does it Mean to Be a Great Leader. In Leadership Lessons for Health Care Providers, 1st ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 8–12. [Google Scholar]
- Lexa, F.J. Leading Change in an Organization. In Leadership Lessons for Health Care Providers, 1st ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 100–108. [Google Scholar]
- World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening. Available online: https://www.who.int/reproductivehealth/publications/digital-interventions-health-system-strengthening/en/ (accessed on 20 October 2021).
- Organization for Economic Co-Operation and Development (OECD). OECD Observatory of Public Sector Innovation. Available online: https://www.oecd.org/media/oecdorg/satellitesites/opsi/contents/files/SystemsApproachesDraft.pdf (accessed on 20 October 2021).
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Barry, S.; Dalton, R.; Eustace-Cook, J. Understanding Change in Complex Health Systems—A Review of the Literature on Change Management in Health and Social Care 2007–2017; Organisation Development and Design Services: Kells, Ireland, 2018. [Google Scholar]
- Birken, S.A.; Lee, S.Y.D.; Weiner, B.J.; Chin, M.H.; Chiu, M.; Schaefer, C.T. From strategy to action: How top managers’ support increases middle managers’ commitment to innovation implementation in health care organizations. Health Care Manag. Rev. 2015, 40, 159–168. [Google Scholar] [CrossRef]
- KPMG. Medical Devices 2030. Available online: https://assets.kpmg/content/dam/kpmg/xx/pdf/2017/12/medical-devices-2030.pdf (accessed on 20 October 2021).
- Deloitte. The Digital Era in the MedTech Industry. Available online: https://www2.deloitte.com/content/dam/Deloitte/us/Documents/process-and-operations/us-the-digital-era-in-the-medtech-industry.pdf (accessed on 20 October 2021).
- Ernst and Young. Pulse of the Industry: Medical Technology Report. 2020. Available online: https://assets.ey.com/content/dam/ey-sites/ey-com/en_gl/topics/health/ey-pulse-medical-technology-report.pdf (accessed on 20 October 2021).
- World Health Organization (WHO). Global Strategy on Digital Health 2020–2025. Available online: https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf (accessed on 20 October 2021).
- Labrique, A.B.; Vasudevan, L.; Kochi, E.; Fabricant, R.; Mehl, G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob. Health Sci. Pract. August 2013, 1, 160–171. [Google Scholar] [CrossRef]
- Small, A.; Gist, D.; Souza, D.; Dalton, J.; Magny-Normilus, C.; David, D. Using Kotter’s change model for implementing bedside handoff. J. Nurs. Care Qual. 2016, 31, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Kotter, J.P. Leading Change, With a New Preface by the Author, 1st ed.; Harvard Business Review Press: Boston, MA, USA, 2012. [Google Scholar]
- Maclean, D.F.W.; Vannet, N. Improving trauma imaging in Wales through Kotter’s theory of change. Clin. Radiol. 2016, 71, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Dolansky, M.A.; Hitch, J.A.; Piña, I.L.; Boxer, R.S. Improving Heart Failure Disease Management in Skilled Nursing Facilities: Lessons Learned. Clin. Nurs. Res. 2013, 22, 432–447. [Google Scholar] [CrossRef]
- Ellsbury, D.L.; Clark, R.H.; Ursprung, R.; Handler, D.L.; Dodd, E.D.; Spitzer, A.R. A multifaceted approach to improving outcomes in the NICU: The pediatrix 100 000 babies campaign. Pediatrics 2016, 137, e20150389. [Google Scholar] [CrossRef] [PubMed]
- Baloh, J.; Zhu, X.; Ward, M.M. Implementing team huddles in small rural hospitals: How does the Kotter model of change apply? J. Nurs. Manag. 2018, 26, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Lewin, K. Frontiers in Group Dynamics: Concept, Method and Reality in Social Science; Social Equilibria and Social Change. Hum. Relat. 1947, 1, 5–41. [Google Scholar] [CrossRef]
- Šuc, J.; Prokosch, H.U.; Ganslandt, T. Applicability of lewińs change management model in a hospital setting. Methods Inf. Med. 2009, 48, 419–428. [Google Scholar] [PubMed]
- Abd El-Shafy, I.; Zapke, J.; Sargeant, D.; Prince, J.M.; Christopherson, N.A.M. Decreased Pediatric Trauma Length of Stay and Improved Disposition with Implementation of Lewin’s Change Model. J. Trauma Nurs. 2019, 26, 84–88. [Google Scholar] [CrossRef]
- Shatpattananunt, B.; Petpichetchian, W.; Kitrungrote, L. Development of the Change Implementation Strategies Model Regarding Evidence-Based Chronic Wound Pain Management. Pac. Rim Int. J. Nurs. Res. 2015, 19, 359–372. [Google Scholar]
- Tetef, S. Successful Implementation of New Technology Using an Interdepartmental Collaborative Approach Recognizing an Opportunity for Growth in New Technology. J. PeriAnesthesia Nurs. 2017, 32, 225–230. [Google Scholar] [CrossRef]
- Welbourn, D.; Warwick, R.; Carnall, C.; Fathers, D. Leadership of Whole Systems; The King’s Fund: London, UK, 2012. [Google Scholar]
- Newell, K.; Corrigan, C.; Punshon, J.; Leary, A. Severe asthma: Emergency care patient driven solutions. Int. J. Health Care Qual. Assur. 2017, 30, 628–637. [Google Scholar] [CrossRef]
- Checkland, P. Achieving ‘desirable and feasible’ change: An application of soft systems methodology. J. Oper. Res. Soc. 1985, 36, 821–831. [Google Scholar]
- Emes, M.; Smith, S.; Ward, S.; Smith, A. Improving the patient discharge process: Implementing actions derived from a soft systems methodology study. Health Syst. 2019, 8, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Schneider, W.E. Why good management ideas fail: The neglected power of organizational culture. Strategy Leadersh. 2000, 28, 24–29. [Google Scholar] [CrossRef]
- Checkland, P.; Poulter, J. Systems Approaches to Managing Change: A Practical Guide; Springer: London, UK, 2010. [Google Scholar]
- Hřebíček, J. Modelování soft (měkkých) systémů. In 5. Letní Škola Matematické Biologie „Analýza Biologických a Klinických dat v Mezioborovém Pojetí; Masarykova univerzita v Brně: Brno, Czechia, 2009. [Google Scholar]
- Mukotekwa, C.; Carson, E. Improving the discharge planning process: A systems study. J. Res. Nurs. 2007, 12, 667–686. [Google Scholar] [CrossRef]
- Emes, M.; Smith, S.; Ward, S.; Smith, A.; Ming, T. Care and Flow: Using Soft Systems Methodology to understand tensions in the patient discharge process. Health Syst. 2017, 6, 260–278. [Google Scholar] [CrossRef]
- Deiters, W.; Burmann, A.; Meister, S. Strategies for digitalizing the hospital of the future. Urologe 2018, 57, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Bruthans, J. The past and current state of the Czech outpatient electronic prescription (eRecept). Int. J. Med. Inform. 2019, 123, 49–53. [Google Scholar] [CrossRef]
- Brice, S.; Almond, H. Health professional digital capabilities frameworks: A scoping review. J. Multidiscip. Healthc. 2020, 2, 1375–1390. [Google Scholar] [CrossRef]
- Shaw, B.; Chisholm, O. Creeping Through the Backdoor: Disruption in Medicine and Health. Front. Pharmacol. 2020, 11, 818. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health in the 21st Century; OECD: Paris, France, 2019. [Google Scholar]
- PROSCI. Communication Checklist for Achieving Change Management. Available online: https://www.prosci.com/resources/articles/change-managementcommunication-checklist (accessed on 18 August 2021).
- Ústav Zdravotnických Informací a Statistiky ČR. Interaktivní Prohlížeč dat-DRG Restart. Available online: https://drg.uzis.cz/index.php?pg=referencni-sit--mapovani-akutni-luzkove-121%20pece--interaktivni-prohlizecdat&studie=i&analyza=i.1&zz_type=&var1=pocet_luzek&var2=osa_b (accessed on 18 August 2021).
- German Hospital Directory. Available online: https://www.german-hospital-directory.com/app/search/maps (accessed on 18 August 2021).
- Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz. Available online: https://kliniksuche.at/suche/bundesland (accessed on 18 August 2021).
- Ministerstvo Zdravotníctva Slovenskej Republiky. Available online: https://www.health.gov.sk/?subjekty-hospodarskej-mobilizacie (accessed on 18 August 2021).
- Page, M.J.; Mckenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Ding, H.; Fatehi, F.; Maiorana, A.; Bashi, N.; Hu, W.; Edwards, I. Digital health for COPD care: The current state of play. J. Thorac. Dis. 2019, 11 (Suppl. 17), S2210–S2220. [Google Scholar] [CrossRef]
- Fatehi, F.; Wootton, R. Telemedicine, telehealth or e-health? A bibliometric analysis of the trends in the use of these terms. J. Telemed. Telecare 2012, 18, 460–464. [Google Scholar] [CrossRef]
- Meinert, E.; Van Velthoven, M.; Brindley, D.; Alturkistani, A.; Foley, K.; Rees, S.; Wells, G.; De Pennington, N. The internet of things in health care in Oxford: Protocol for proof-of-concept projects. J. Med. Internet Res. 2018, 7, e12077. [Google Scholar] [CrossRef]
- Olze, H.; Uecker, F.C.; Häubler, S.M.; Knopke, S.; Szczepek, A.J.; Gräbel, S. Hearing Implants in the Era of Digitization. Laryngo- Rhino- Otol. 2019, 98, S1–S24. [Google Scholar]
- Ferrante, G.; Licari, A.; Marseglia, G.L.; La Grutta, S. Digital health interventions in children with asthma. Clin. Exp. Allergy 2021, 51, 212–220. [Google Scholar] [CrossRef]
- Rose, K.J.; Petrut, C.; L’heveder, R.; De Sabata, S. IDF Europe’s position on mobile applications in diabetes. Diabetes Res. Clin. Pract. 2019, 149, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Kernebeck, S.; Busse, T.S.; Böttcher, M.D.; Weitz, J.; Ehlers, J.; Bork, U. Impact of mobile health and medical applications on clinical practice in gastroenterology. World J. Gastroenterol. 2020, 26, 4182–4197. [Google Scholar] [CrossRef] [PubMed]
- Wechkunanukul, K.; Parajuli, D.R.; Hamiduzzaman, M. Utilising digital health to improve medication-related quality of care for hypertensive patients: An integrative literature review. World J. Clin. Cases 2020, 8, 2266–2279. [Google Scholar] [CrossRef]
- Griauzde, D.; Kullgren, J.T.; Liestenfeltz, B.; Ansari, T.; Johnson, E.H.; Fedewa, A.; Saslow, L.R.; Richardson, C.; Heisler, M. A mobile phone-based program to promote healthy behaviors among adults with prediabetes who declined participation in free diabetes prevention programs: Mixed-methods pilot randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e11267. [Google Scholar] [CrossRef]
- Tripoliti, E.E.; Karanasiou, G.S.; Kalatzis, F.G.; Naka, K.K.; Fotiadis, D.I. The Evolution of mHealth Solutions for Heart Failure Management. In Heart Failure: From Research to Clinical Practice; Springer: New York, NY, USA, 2018; pp. 353–371. [Google Scholar]
- Wongvibulsin, S.; Martin, S.S.; Steinhubl, S.R.; Muse, E.D. Connected Health Technology for Cardiovascular Disease Prevention and Management. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 1–15. [Google Scholar] [CrossRef]
- Gopal, G.; Suter-Crazzolara, C.; Toldo, L.; Eberhardt, W. Digital transformation in healthcare-Architectures of present and future information technologies. Clin. Chem. Lab. Med. 2018, 57, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Seyhan, A.A.; Carini, C. Are innovation and new technologies in precision medicine paving a new era in patients centric care? J. Transl. Med. 2019, 17, 114. [Google Scholar] [CrossRef]
- Kataria, S.; Ravindran, V. Digital health: A new dimension in rheumatology patient care. Rheumatol. Int. 2018, 38, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Gessa, A.; Jiménez, A.; Sancha, P. Open innovation in digital healthcare: Users’ discrimination between certified and non-certified mhealth applications. J. Open Innov. Technol. Mark. Complex. 2020, 6, 1–20. [Google Scholar]
- Lo, C.; Yu, J.; Görges, M.; Matava, C. Anesthesia in the modern world of apps and technology: Implications and impact on wellness. Pediatric Anesth. 2021, 31, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Kouroubali, A.; Katehakis, D.G. The new European interoperability framework as a facilitator of digital transformation for citizen empowerment. J. Biomed. Inform. 2019, 94, 103166. [Google Scholar] [CrossRef]
- Scott, I.A.; Sullivan, C.; Staib, A. Going digital: A checklist in preparing for hospital-wide electronic medical record implementation and digital transformation. Aust. Health Rev. 2019, 43, 302–313. [Google Scholar] [CrossRef]
- Meinert, E.; Alturkistani, A.; Brindley, D.; Knight, P.; Wells, G.; De Pennington, N. The technological imperative for value-based health care. Br. J. Hosp. Med. 2018, 79, 328–332. [Google Scholar] [CrossRef]
- Faggini, M.; Cosimato, S.; Nota, F.D.; Nota, G. Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability 2019, 11, 165. [Google Scholar] [CrossRef]
- Hermes, S.; Riasanow, T.; Clemons, E.K.; Böhm, M.; Krcmar, H. The digital transformation of the healthcare industry: Exploring the rise of emerging platform ecosystems and their influence on the role of patients. Bus. Res. 2020, 13, 1033–1069. [Google Scholar] [CrossRef]
- Park, C.-W.; Seo, S.W.; Kang, N.; Ko, B.S.; Choi, B.W.; Park, C.M.; Chang, D.K.; Kim, H.; Kim, H.; Lee, H.; et al. Artificial Intelligence in Health Care: Current Applications and Issues. J. Korean Med. Sci. 2020, 35, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gehring, H.; Rackebrandt, K.; Imhoff, M. E-Health und die Realität–was sehen wir heute schon in der Klinik? Bundesgesundheitsblatt-Gesundh. -Gesundh. 2018, 61, 252–262. [Google Scholar] [CrossRef]
- Despotou, G.; Laleci Erturkmen, G.B.; Yuksel, M.; Sarigul, B.; Lindman, P.; Jaulent, M.C.; Bouaud, J.; Traore, L.; Lim Choi Keung, S.N.; De Manuel, E.; et al. Localisation, personalisation and delivery of best practice guidelines on an integrated care and cure cloud architecture: The C3-cloud approach to managing multimorbidity. Stud. Health Technol. Inform. 2020, 270, 623–627. [Google Scholar]
- Kobusinge, G. Managing as Designing: Transforming Digital Healthcare Interoperability. Proceedings of the 26th Americas Conference on Information Systems, AMCIS. 2020. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85097714752&partnerID=40&md5=f4e265b215fc68c6b6aec74633053412 (accessed on 29 August 2021).
- Kolasa, K.; Goettsch, W.; Petrova, G.; Berler, A. ‘Without data, you’re just another person with an opinion’. Expert Rev. Pharm. Outcomes Res. 2020, 20, 147–154. [Google Scholar] [CrossRef]
- Laleci Erturkmen, G.B.; Yuksel, M.; Sarigul, B.; Arvanitis, T.N.; Lindman, P.; Chen, R.; Zhao, L.; Sadou, E.; Bouaud, J.; Traore, L.; et al. A Collaborative Platform for Management of Chronic Diseases via Guideline-Driven Individualized Care Plans. Comput. Struct. Biotechnol. J. 2019, 17, 869–885. [Google Scholar] [CrossRef]
- Wang, S.Y.; Pershing, S.; Lee, A.Y. Big data requirements for artificial intelligence. Curr. Opin. Ophthalmol. 2020, 31, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Odisho, A.Y.; Lui, H.; Yerramsetty, R.; Bautista, F.; Gleason, N.; Martin, E.; Young, J.J.; Blum, M.; Neinstein, A.B. Design and development of Referrals Automation, a SMART on FHIR solution to improve patient access to specialty care. JAMIA Open 2020, 3, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Kourtis, L.C.; Regele, O.B.; Wright, J.M.; Jones, G.B. Digital biomarkers for Alzheimer’s disease: The mobile/wearable devices opportunity. NPJ Digit. Med. 2019, 2, 1–9. [Google Scholar] [CrossRef]
- Jin, X.; Liu, C.; Xu, T.; Su, L.; Zhang, X. Artificial intelligence biosensors: Challenges and prospects. Biosens. Bioelectron. 2020, 165, 112412. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, Y.; Cai, S.; Han, Z.; Liu, X.; Wang, F.; Cao, Y.; Wang, Z.; Li, H.; Chen, Y.; et al. Flexible Hybrid Electronics for Digital Healthcare. Adv. Mater. 2020, 32, 1902062. [Google Scholar] [CrossRef]
- Binder, A.F.; Handley, N.R.; Wilde, L.; Palmisiano, N.; Lopez, A.M. Treating Hematologic Malignancies During a Pandemic: Utilizing Telehealth and Digital Technology to Optimize Care. Front. Oncol. 2020, 10, 1183. [Google Scholar] [CrossRef]
- Noel, K.; Ellison, B. Inclusive innovation in telehealth. Digit. Med. 2020, 3, 1–3. [Google Scholar]
- Guy, M.; Koizia, L.; Kooner, A.; Cafferkey, J.; Ross, C.; Purkayastha, S.; Sivananthan, A.; Tanna, A.; Pratt, P.; Kinross, J. Use of the HoloLens2 mixed reality headset for protecting health care workers during the COVID-19 pandemic: Prospective, observational evaluation. J. Med. Internet Res. 2020, 22, e21486. [Google Scholar]
- Umoren, R.A.; Gray, M.M.; Handley, S.; Johnson, N.; Kunimura, C.; Mietzsch, U.; Billimoria, Z.; Lo, M.D. In-Hospital Telehealth Supports Care for Neonatal Patients in Strict Isolation. Am. J. Perinatol. 2020, 37, 857–860. [Google Scholar] [CrossRef]
- Raphael, B.P.; Schumann, C.; Garrity-Gentille, S.; Mcclelland, J.; Rosa, C.; Tascione, C.; Gallotto, M.; Takvorian-Bené, M.; Carey, A.N.; Mccarthy, P.; et al. Virtual Telemedicine Visits in Pediatric Home Parenteral Nutrition Patients: A Quality Improvement Initiative. Telemed. e-Health 2019, 25, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Ahad, A.; Tahir, M.; Sheikh, M.A.; Ahmed, K.I.; Mughees, A.; Numani, A. Technologies trend towards 5g network for smart health-care using iot: A review. Sensors 2020, 20, 4047. [Google Scholar] [CrossRef]
- Shayevitz, C.; Breitinger, S.; Lerario, M.P.; Mroczkowski, M.; Osuji, M.; Fleischut, P.; Khan, M.; Murray, J.; Wilner, P.; Sombrotto, L. Implementation of a Centralized Telepsychiatry Consult Service in a Multi-Hospital Metropolitan Health Care System: Challenges and Opportunities. Psychosomatics 2020, 62, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, L.R.; Hall, C.L.; Andrén, P.; Bethan Davies, E.; Kilgariff, J.; Kouzoupi, N.; Murphy, T.; Hollis, C. Therapist-supported online interventions for children and young people with tic disorders: Lessons learned from a randomized controlled trial and considerations for future practice. JMIR Ment. Health 2020, 7, e19600. [Google Scholar] [CrossRef]
- Mamyrbekova, S.; Nurgaliyeva, Z.; Saktapov, A.; Zholdasbekova, A.; Kudaibergenova, A. Medicine of the Future: Digital Technologies in Healthcare. E3S Web Conf. 2020, 159, 04036. [Google Scholar] [CrossRef]
- Dohan, M.S.; Califf, C.B.; Ghosh, K.; Tan, J. Digital transformation in healthcare: New value for a new movement. Health Policy Technol. 2020, 9, 177–178. [Google Scholar] [CrossRef]
- El Hayek, S.; Nofal, M.; Abdelrahman, D.; Adra, A.; Al Harthi, M.; Al Shamli, S.; Alnuaimi, N.; Bensid, L.; Cheaito, M.A.; Emberish, A.M.; et al. Telepsychiatry in the Arab World: A Viewpoint Before and During COVID-19. Neuropsychiatr. Dis. Treat. 2020, 16, 2805–2815. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Horsham, C.; Koh, U.; Gillespie, N.; Vagenas, D.; Loescher, L.J.; Curiel-Lewandrowski, C.; Hofmann-Wellenhof, R.; Peter Soyer, H. Evaluating healthcare practitioners’ views on store-and-forward teledermoscopy services for the diagnosis of skin cancer. Digit. Health 2019, 5, 2055207619828225. [Google Scholar] [CrossRef]
- Stephenson, D.; Alexander, R.; Aggarwal, V.; Badawy, R.; Bain, L.; Bhatnagar, R.; Bloem, B.R.; Boroojerdi, B.; Burton, J.; Cedarbaum, J.M.; et al. Precompetitive Consensus Building to Facilitate the Use of Digital Health Technologies to Support Parkinson Disease Drug Development through Regulatory Science. Digit. Biomark. 2020, 4, 28–49. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. A Showcase of Medical, Therapeutic and Pastime Uses of Virtual Reality (VR) and How (VR) Is Impacting the Dementia Sector. Adv. Exp. Med. Biol. 2019, 1156, 135–141. [Google Scholar]
- Bhavnani, S.P. Digital Health: Opportunities and Challenges to Develop the Next-Generation Technology-Enabled Models of Cardiovascular Care. Methodist DeBakey Cardiovasc. J. 2020, 16, 296–303. [Google Scholar] [CrossRef]
- Gruska, M.; Aigner, G.; Altenberger, J.; Burkart-Küttner, D.; Fiedler, L.; Gwechenberger, M.; Lercher, P.; Martinek, M.; Nürnberg, M.; Pölzl, G.; et al. Recommendations on the utilization of telemedicine in cardiology. Wien. Klin. Wochenschr. 2020, 132, 782–800. [Google Scholar] [CrossRef]
- Horgan, D.; Romao, M.; Morré, S.A.; Kalra, D. Artificial Intelligence: Power for Civilisation–and for Better Healthcare. Public Health Genom. 2019, 22, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Basset, M.; Chang, V.; Nabeeh, N.A. An intelligent framework using disruptive technologies for COVID-19 analysis. Technol. Forecast. Soc. Chang. 2021, 163, 120431. [Google Scholar] [CrossRef]
- Improta, G.; Luca, V.; Illario, M.; Triassi, M. Digital Innovation in Healthcare: A Device with A Method for Monitoring, Managing and Preventing the Risk of Chronic Polypathological Patients. Transl. Med. UniSa 2020, 21, 61–64. [Google Scholar]
- Pesapane, F.; Codari, M.; Sardanelli, F. Artificial intelligence in medical imaging: Threat or opportunity? Radiologists again at the forefront of innovation in medicine. Eur. Radiol. Exp. 2018, 2, 35. [Google Scholar] [CrossRef] [PubMed]
- Burnside, M.; Crocket, H.; Mayo, M.; Pickering, J.; Tappe, A.; De Bock, M. Do-It-Yourself Automated Insulin Delivery: A Leading Example of the Democratization of Medicine. J. Diabetes Sci. Technol. 2020, 14, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Coiera, E. The Price of Artificial Intelligence. Yearb. Med. Inform. 2019, 28, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Casey, D.; Joshi, I.; Zhu, J.; Cheng, F. Emergence of New Disease: How Can Artificial Intelligence Help? Trends Mol. Med. 2020, 26, 627–629. [Google Scholar] [CrossRef]
- Chehade, M.J.; Yadav, L.; Kopansky-Giles, D.; Merolli, M.; Palmer, E.; Jayatilaka, A.; Slater, H. Innovations to improve access to musculoskeletal care. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101559. [Google Scholar] [CrossRef]
- Lai, L.; Wittbold, K.A.; Dadabhoy, F.Z.; Sato, R.; Landman, A.B.; Schwamm, L.H.; He, S.; Patel, R.; Wei, N.; Zuccotti, G.; et al. Digital triage: Novel strategies for population health management in response to the COVID-19 pandemic. Healthcare 2020, 8, 100493. [Google Scholar] [CrossRef]
- Arora, A. Conceptualising artificial intelligence as a digital healthcare innovation: An introductory review. Med. Devices Evid. Res. 2020, 13, 223–230. [Google Scholar] [CrossRef]
- Bhavnani, S.P.; Sitapati, A.M. Virtual Care 2.0—a Vision for the Future of Data-Driven Technology-Enabled Healthcare. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 21. [Google Scholar] [CrossRef] [PubMed]
- Alami, H.; Lehoux, P.; Denis, J.L.; Motulsky, A.; Petitgand, C.; Savoldelli, M.; Rouquet, R.; Gagnon, M.P.; Roy, D.; Fortin, J.P. Organizational readiness for artificial intelligence in health care: Insights for decision-making and practice. J. Health Organ. Manag. 2020, 35, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Decary, M. Artificial intelligence in healthcare: An essential guide for health leaders. Healthc. Manag. Forum 2020, 33, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Suehling, M.; Flohr, T.; Comaniciu, D. Artificial Intelligence in Diagnostic Imaging: Status Quo, Challenges, and Future Opportunities. J. Thorac. Imaging 2020, 35 (Suppl. 1), S11–S16. [Google Scholar] [CrossRef]
- Siering, L.; Ludden, G.D.S.; Mader, A.; Van Rees, H. A Theoretical Framework and Conceptual Design for Engaging Children in Therapy at Home—The Design of a Wearable Breathing Trainer. J. Pers. Med. 2019, 9, 27. [Google Scholar] [CrossRef]
- Badawy, R.; Hameed, F.; Bataille, L.; Little, M.A.; Claes, K.; Saria, S.; Cedarbaum, J.M.; Stephenson, D.; Neville, J.; Maetzler, W.; et al. Metadata Concepts for Advancing the Use of Digital Health Technologies in Clinical Research. Digit. Biomark. 2019, 3, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Kooman, J.P.; Wieringa, F.P.; Han, M.; Chaudhuri, S.; Van Der Sande, F.M.; Usvyat, L.A.; Kotanko, P. Wearable health devices and personal area networks: Can they improve outcomes in haemodialysis patients? Nephrol. Dial. Transplant. 2020, 35 (Suppl. 2), II43–II50. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Corsini, E.M.; Jin, S.; Barbosa, G.R.; Kell, T.; Antonoff, M.H.; Antonoff, M.B. Advanced Data Analytics for Clinical Research Part I: What are the Tools? Innov. Technol. Tech. Cardiothorac. Vasc. Surg. 2020, 15, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Uslu, B.Ç.; Okay, E.; Dursun, E. Analysis of factors affecting IoT-based smart hospital design. J. Cloud Comput. 2020, 9, 67. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, J.; Glasziou, P.; Westbrook, J. The three numbers you need to know about healthcare: The 60–30–10 Challenge. BMC Med. 2020, 18, 102. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Papoutsi, C. Studying complexity in health services research: Desperately seeking an overdue paradigm shift. BMC Med. 2018, 16, 95. [Google Scholar] [CrossRef]
- Kraus, S.; Schiavone, F.; Pluzhnikova, A.; Invernizzi, A.C. Digital transformation in healthcare: Analyzing the current state-of-research. J. Bus. Res. 2021, 123, 557–567. [Google Scholar] [CrossRef]
- National Academies of Sciences Engineering and Medicine. Crossing the Global Quality Chasm: Improving Health Care Worldwide; The National Academies Press: Washington, DC, USA, 2018. [Google Scholar]
- Nielsen, P.; Nielsen, R.N.; Bamberger, S.G.; Stamhus, J.; Fonager, K.; Larsen, A.; Vinding, A.L.; Ryom, P.; Omland, O. Capabilities for innovation: The nordic model and employee participation. Nord. J. Work. Life Stud. 2012, 2, 85–115. [Google Scholar] [CrossRef][Green Version]
- Garmann-Johnsen, N.F.; Helmersen, M.; Eikebrokk, T.R. Digital Transformation in Healthcare: Enabling Employee Co-Creation through web 2.0. In Proceedings of the 26th Americas Conference on Information Systems 2018, Digital Disruption, AMCIS, New Orleans, LA, USA, 16 August 2018; Available online: https://www.researchgate.net/publication/328997843_Digital_Transformation_in_Healthcare_Enabling_Employee_Co-Creation_through_Web_20_Completed_Research (accessed on 31 August 2021).
- Hartvigsen, G.; Pedersen, S. Lessons Learned from 25 Years with Telemedicine in Northern Norway, 1st ed.; University Hospital of North Norway: Tromsø, Norway, 2015. [Google Scholar]
- Nonaka, I. Toward Middle-Up-Down Management: Accelerating Information Creation. MIT Sloan Manag. Rev. 1988, 20, 9–18. [Google Scholar]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J. Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef]
- Weiner, B.J.; Amick, H.; Lee, S.Y.D. Conceptualization and measurement of organizational readiness for change. A review of the literature in health services research and other fields. Med. Care Res. Rev. 2008, 65, 379–436. [Google Scholar] [CrossRef]
- Blease, C.; Kaptchuk, T.J.; Bernstein, M.H.; Mandl, K.D.; Halamka, J.D.; Desroches, C.M. Artificial intelligence and the future of primary care: Exploratory qualitative study of UK general practitioners’ views. J. Med. Internet Res. 2019, 21, e12802. [Google Scholar] [CrossRef] [PubMed]
- Sdělení Komise Evropskému Parlamentu, Radě, Evropskému Hospodářskému a Sociálnímu Výboru a Výboru Regionů. Available online: https://eur-lex.europa.eu/legal-content/CS/TXT/?uri=CELEX%3A52016AE3545 (accessed on 30 August 2021).
- Muffly, M.; Scheinker, D.; Muffly, T.; Singleton, M.; Agarwal, R.; Honkanen, A. Practice Characteristics of Board-certified Pediatric Anesthesiologists in the US: A Nationwide Survey. Cureus 2019, 11, e5745. [Google Scholar] [CrossRef] [PubMed]
- Faddis, A. The digital transformation of healthcare technology management. Biomed. Instrum. Technol. 2018, 52, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Elshaug, A.G.; Rosenthal, M.B.; Lavis, J.N.; Brownlee, S.; Schmidt, H.; Nagpal, S.; Littlejohns, P.; Srivastava, D.; Tunis, S.; Saini, V. Levers for addressing medical underuse and overuse: Achieving high-value health care. Lancet 2017, 390, 191–202. [Google Scholar] [CrossRef]
- Nolte, E.; World Health Organization. How Do We Ensure That Innovation in Health Service Delivery and Organization Is Implemented, Sustained and Spread? Available online: https://apps.who.int/iris/bitstream/handle/10665/331980/Policy-brief-3-1997-8073-2018-eng.pdf?sequence=5&isAllowed=y (accessed on 30 August 2021).
- Hansen, S.; Baroody, A.J. Electronic health records and the logics of care: Complementarity and conflict in the U.S. Healthcare system. Inf. Syst. Res. 2020, 31, 57–75. [Google Scholar] [CrossRef]
- Malhotra, N.K.; Kim, S.S.; Agarwal, J. Internet users’ information privacy concerns (IUIPC): The construct, the scale, and a causal model. Inf. Syst. Res. 2004, 15, 336–355. [Google Scholar] [CrossRef]
- Naidoo, R. Building a critical mass of users for digital healthcare promotion programs: A teaching case. J. Cases Inf. Technol. 2020, 22, 44–59. [Google Scholar] [CrossRef]
- Henke, N.; Ehrbeck, T.; Kibasi, T. Unlocking Productivity through Healthcare Delivery Innovations: Lessons from Entrepreneurs around the World; McKinsey & Company: Chicago, IL, USA, 2010. [Google Scholar]
- Britnell, M. Human: Solving the Global Workforce Crisis in Healthcare; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Greenhalgh, T.; Robert, G.; Macfarlane, F.; Bate, P.; Kyriakidou, O. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Q. 2004, 82, 581–629. [Google Scholar] [CrossRef]
- Frick, N.R.J.; Möllmann, H.L.; Mirbabaie, M.; Stieglitz, S. Driving Digital Transformation During a Pandemic: Case Study of Virtual Collaboration in a German Hospital. JMIR Med. Inform. 2021, 9, e25183. [Google Scholar] [CrossRef]
- Allard, J.; Dzwonczyk, R.; Yablok, D.; Block, F.E.; Mcdonald, J.S. Effect of automatic record keeping on vigilance and record keeping time. Br. J. Anaesth. 1995, 74, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Stol, I.S.; Ehrenfeld, J.M.; Epstein, R.H. Technology Diffusion of Anesthesia Information Management Systems into Academic Anesthesia Departments in the United States. Anesth. Analg. 2014, 118, 644–650. [Google Scholar] [CrossRef]
- Bruthans, J. Anesthesia Information Management Systems in the Czech Republic from the Perspective of Early Adopters. J. Med. Syst. 2020, 44, 70. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field | Lewin | Kotter | SSM |
|---|---|---|---|
| External expert | maybe | maybe | no |
| Pre-defined problem | yes | yes | no |
| Feedback | yes | yes | yes |
| Sociological approach | positivism | combination | interpretivism |
| Support tools | field theory, action research, group dynamics | “see-feel-change” | CATWOE, PQR, “root definitions” |
| Dismantling existing situation | in step 1 | in step 1 | during the process |
| Cyclical process (constant problem solving) | yes | yes | yes |
| Management/leading coalition | yes | yes | no |
| Recommended step sequence | yes | yes | steps overlap in reality |
| Building awareness why the change is necessary | yes | yes | not necessary, awareness arises spontaneously |
| Adaptability to changing environment | no | partly | yes |
| Suitable application | smaller changes | bigger changes | complex problems |
| CHM approach | top-down | top-down, partly bottom-up | combination of bottom-up and top-down |
| Question No. | Key Research Question |
|---|---|
| 1. | Do the majority of healthcare managers use CHM tools? |
| 2. | What specific CHM method do healthcare managers use the most? |
| 3. | What hospital actors are most involved in change implementation and management? |
| 4. | What changes (of what type) are currently most frequently being implemented in hospitals? |
| 5. | What is the target of the change implementation and what information do mangers provide to those involved in the change? |
| 6. | What do managers think about the implemented change? How do they judge the success/failure of a change? |
| 7. | What opportunities and threats can be identified in the context of digital innovations? |
| Country | Population 1 | Beds Per 100,000 Inhabitants (Rounded off) 2 | Number of Hospitals with 500+ Beds 3 | Number of Participating Hospitals |
|---|---|---|---|---|
| Czech Republic | 10,693,861 | 662 | 36 | 28 |
| Germany | 83,135,181 | 800 | 244 | 64 |
| Austria | 8,904,262 | 727 | 26 | 16 |
| Poland 3 | 37,941,122 | 654 | n/a | n/a |
| Hungary | 9,771,975 | 701 | 44 | 12 |
| Slovakia | 5,457,679 | 570 | 18 | 12 |
| In total | 368 | 132 |
| Web of Science | PubMed | Scopus | |
|---|---|---|---|
| Search terms | (((“trend”[Title] OR “evolution”[Title] OR “digital”)[Title]) AND ((“hospital”[Title] OR “healthcare”)[Title])) AND ((“transformation”[Topic] OR “innovation”)[Topic]) | (((“trend”[Title] OR “evolution”[Title] OR “digital”)[Title]) AND ((“hospital”[Title] OR “healthcare”)[Title])) AND ((“transformation”[Title/Abstract] OR “innovation”)[Title/Abstract]) | TITLE (“trend”OR “evolution” OR “digital”) AND Title (“hospital” OR “healthcare”) AND TitleABS (“transformation” OR “innovation”) |
| Time period | 2018–2020 | 2018–2020 (6 December 2020) | 2018–2021 (7 Mar 2021) |
| Languages | English, German | English, German | English, German |
| Document type | Papers, conferences, reviews, editorial material, early access | Papers, conferences, reviews, case studies, clinical trials, systematic literature review, randomized controlled trials | Papers, conferences, reviews |
| Question | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Does the study focus on the use of digital innovations in healthcare? | implementation or use of digital innovation as the main topic; digital innovation in any healthcare intervention with elements of e-Health, virtual reality, smart phones/portable devices, or telemedicine as part of its implementation; aimed at understanding why the innovation is being incorporated into healthcare activities | the main topic focuses on the creation of measures, checklists or other metrics that do not represent a healthcare digitisation intervention; merely a technical description of an innovation; studies focusing on safety, education, or ethical issues related to digital innovations |
| Does the study deal with the framework for a digital innovation implementation? | studies focusing on theoretical mathematical models or statistical models and simulations of | |
| Is the study rooted in the hospital environment? | hospital or clinic environment | other environments (e.g., pharmaceutical companies, medical device manufacturers) |
| Country | Number of Potential Respondents Contacted | Number of Answers | Return Rate |
|---|---|---|---|
| Czech Republic | 279 | 69 | 26% |
| Germany | 1389 | 86 | 7% |
| Austria | 293 | 26 | 10% |
| Slovakia | 78 | 22 | 30% |
| Hungary | 298 | 12 | 4% |
| Total | 2337 | 215 | 11% |
| Top Management | Whole Team (Leadership Coalition) | Middle Management | Quality Managers | Project Managers | HR Dept. | Outsourcing | Other | |
|---|---|---|---|---|---|---|---|---|
| Czech Republic | 70% | 32% | 19% | 33% | 9% | 6% | 1% | 6% |
| Germany | 46% | 71% | 40% | 27% | 31% | 6% | 2% | 1% |
| Austria | 35% | 77% | 31% | 15% | 12% | 4% | 4% | 4% |
| Slovakia | 65% | 17% | 0% | 26% | 4% | 0% | 0% | 9% |
| Hungary | 67% | 33% | 17% | 8% | 8% | 0% | 0% | 0% |
| % (average) | 48% | 51% | 27% | 26% | 17% | 5% | 2% | 4% |
| Absolute number | 104 | 110 | 57 | 56 | 37 | 10 | 4 | 8 |
| Technology | Opportunity | Threat |
|---|---|---|
| mHealth | Wide user basis of mobile phone users [49,50] Rapid growth in the number of applications supporting self-management [51,52,53] Applicable to a wide scope of diagnoses [47,53] Increased patient engagement during treatment [47,52,53,54,55] | Ethical and legal aspects [53,56,57,58] Limited evidence of outcomes and benefits (insufficient randomised controlled trials) [47,52,56,59,60] Low interoperability and integration with existing work procedures [56] Uncertainty concerning data reliability [47,56] Declining patient self-discipline over time [52] Absence of personal contact with physician [55] Non-certified applications, large number of applications [61,62] Level of physician acceptance of mobile health applications [62] |
| Electronic Health Record (EHR), Electronic Medical Record (EMR), Personal Health Record (PHR) | Access to information for all stakeholders [63,64,65,66,67] Benefits if combined with AI [58,65,68] Higher accuracy, legibility, reliability, and better information search functions [64,65,69,70] Risk management—reminders, warnings (allergies, patient history) [64,67,70] Less burden on treating medical staff [36,64] Reduction of cost related to poor documentation [64,65,69] | Violation of the interoperability condition [53,63,70,71] Problem with aligning operating standards with the current information exchange protocols for Big Data [72] Regulatory restraints [72,73,74] The risk of possible re-identification [74] Financial sustainability [75] |
| Digital biomarkers | Wide user base [76] Wide range of information [76] Better diagnostic and decision-making on interventions thanks to continual data collection [58,59] Developing flexible electronic materials for integrating chip technology [77,78] | Bad choice of monitored attributes [59] Problems with technology validation [59] |
| Telemedicine | Lower risk of disease transmission [79,80,81] Suitable for “social distancing” [82] Reduction in hospitalization cost [83,84] Comparable or better care than that of in-person consultations [79,83,85] Elimination of the feeling of isolation during hospitalization [79] Alleviation of resource scarcity (staff, geographical location) [84,86,87,88] Shorter waiting times [60,86] Applicable to numerous diagnoses (e.g., in psychiatry, dermatology, etc.) [60,89,90,91,92] | Limited applicability based on diagnosis [79,85] Unreliable Internet connection [79,85] Lack of training in the use of digital devices [60,79,93] Violation of interoperability between healthcare providers and healthcare systems [94] Discrimination of certain patient groups (e.g., people with particular handicaps) [80] Limited evidence of outcomes and benefits (insufficient randomised controlled trials) [60,80] |
| Artificial intelligence (AI) | Prediction of illness development [94,95,96,97,98] Improvements in treatment optimization and effectiveness [94,97,99,100] Evidence-based recommendations [60,98,101] Delegation of simple and repeating tasks to AI [96] Lower number of hospitalizations [95] Cost cutting [77,95,97] Less pressure on scarce HR in healthcare [102,103] Automatic recall and rescheduling of patients [98] Bigger potential of other digital innovations [68,104] Ability to process huge amounts of data [101] AI-biosensors (miniaturization, scalability, low power consumption, high sensitivity, multifunction, safety, non-toxicity, and degradation) [77] | Incompatible with older infrastructure [105] Lack of understanding of AI functionality [68,106] Inefficient use of AI in day-to-day workflows [107,108] Potential conflict between human ability to act autonomously and the complicated, allegedly infallible machine logic (known as automation bias [69,100] Legal and ethical issues [68,95,100,101,104] Physicians’ concern about AI (security, privacy, and confidentiality) [68,101] Missing multidisciplinary AI teams [98] |
| Wearable technologies | Wide user base [76,77,93] Better diagnostics and decision-making about interventions thanks to continual data collection [76,77,91,106,109] Source of objective data (measured in real-life conditions) [76,91,110] Reduction of “unnecessary” out-patient visits [94] 4P medicine (predictive, precise, preventative and personalized) [76,77,111] | Data smog [76,91] Standardization and validation issues with sensor placement [91] Energy consumption (limited battery capacity) [49,84] Different levels of digital literacy and/or aproach to technologies among patients [47,91] Declining patient self-discipline over time [91] Limited availability due to high production costs of some technologies [77] |
| Internet of Things (IoT) | Higher operational efficiency [49,112] Integration of data from various sources [49,112] Disease prevention and monitoring [49,113] Use of AI in analyses [49,65,113] | Loss of safe and stable communication with devices [84] Higher demands on network infrastructure [49] Unauthorised manipulation [49,112] There are currently no clear instructions for healthcare staff how to use IoT (e.g., in recommendations to patients concerning their use) [49] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hospodková, P.; Berežná, J.; Barták, M.; Rogalewicz, V.; Severová, L.; Svoboda, R. Change Management and Digital Innovations in Hospitals of Five European Countries. Healthcare 2021, 9, 1508. https://doi.org/10.3390/healthcare9111508
Hospodková P, Berežná J, Barták M, Rogalewicz V, Severová L, Svoboda R. Change Management and Digital Innovations in Hospitals of Five European Countries. Healthcare. 2021; 9(11):1508. https://doi.org/10.3390/healthcare9111508
Chicago/Turabian StyleHospodková, Petra, Jana Berežná, Miroslav Barták, Vladimír Rogalewicz, Lucie Severová, and Roman Svoboda. 2021. "Change Management and Digital Innovations in Hospitals of Five European Countries" Healthcare 9, no. 11: 1508. https://doi.org/10.3390/healthcare9111508
APA StyleHospodková, P., Berežná, J., Barták, M., Rogalewicz, V., Severová, L., & Svoboda, R. (2021). Change Management and Digital Innovations in Hospitals of Five European Countries. Healthcare, 9(11), 1508. https://doi.org/10.3390/healthcare9111508