
Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population


Abstract
:1. Introduction
2. Materials and Methods
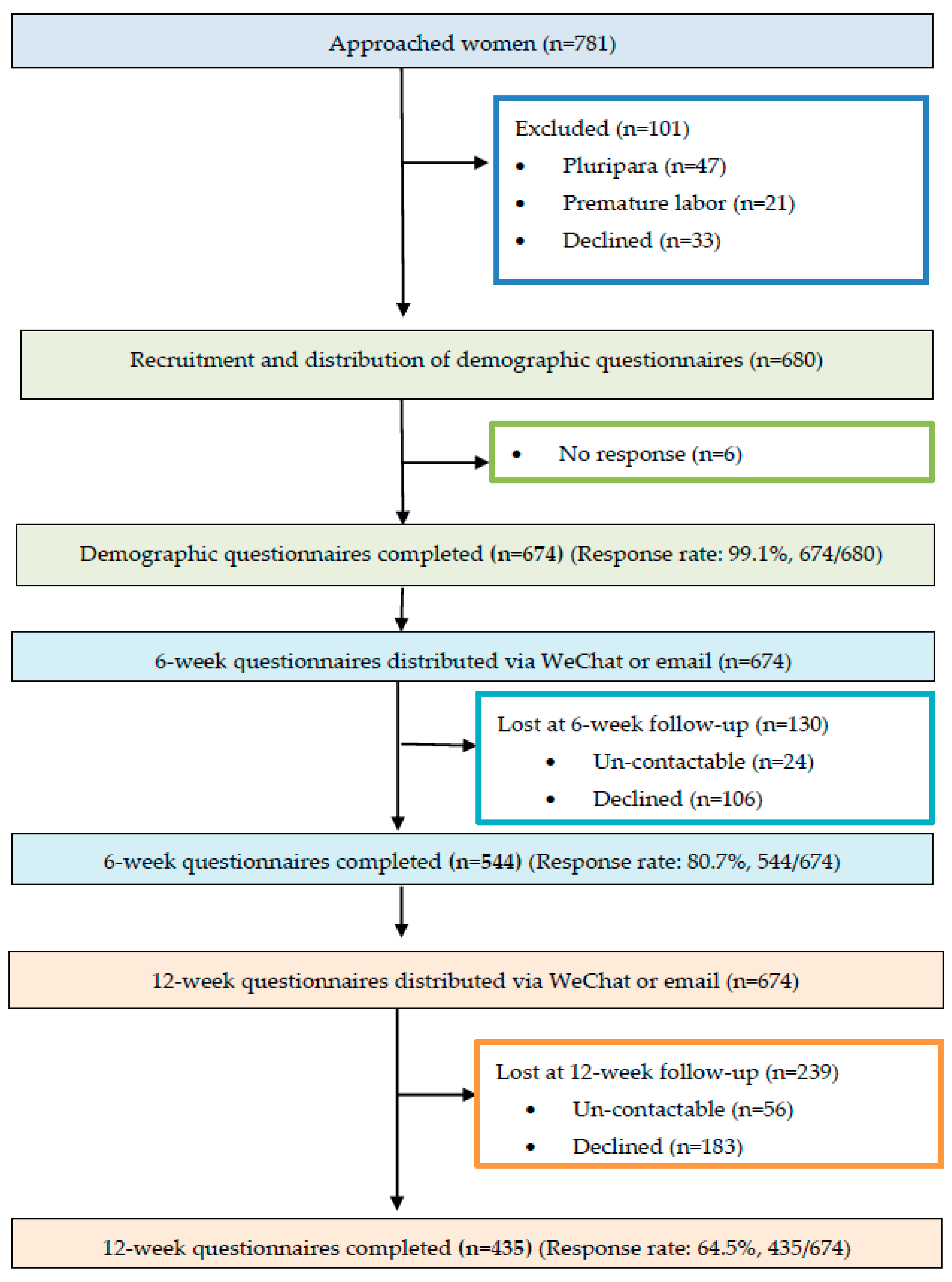
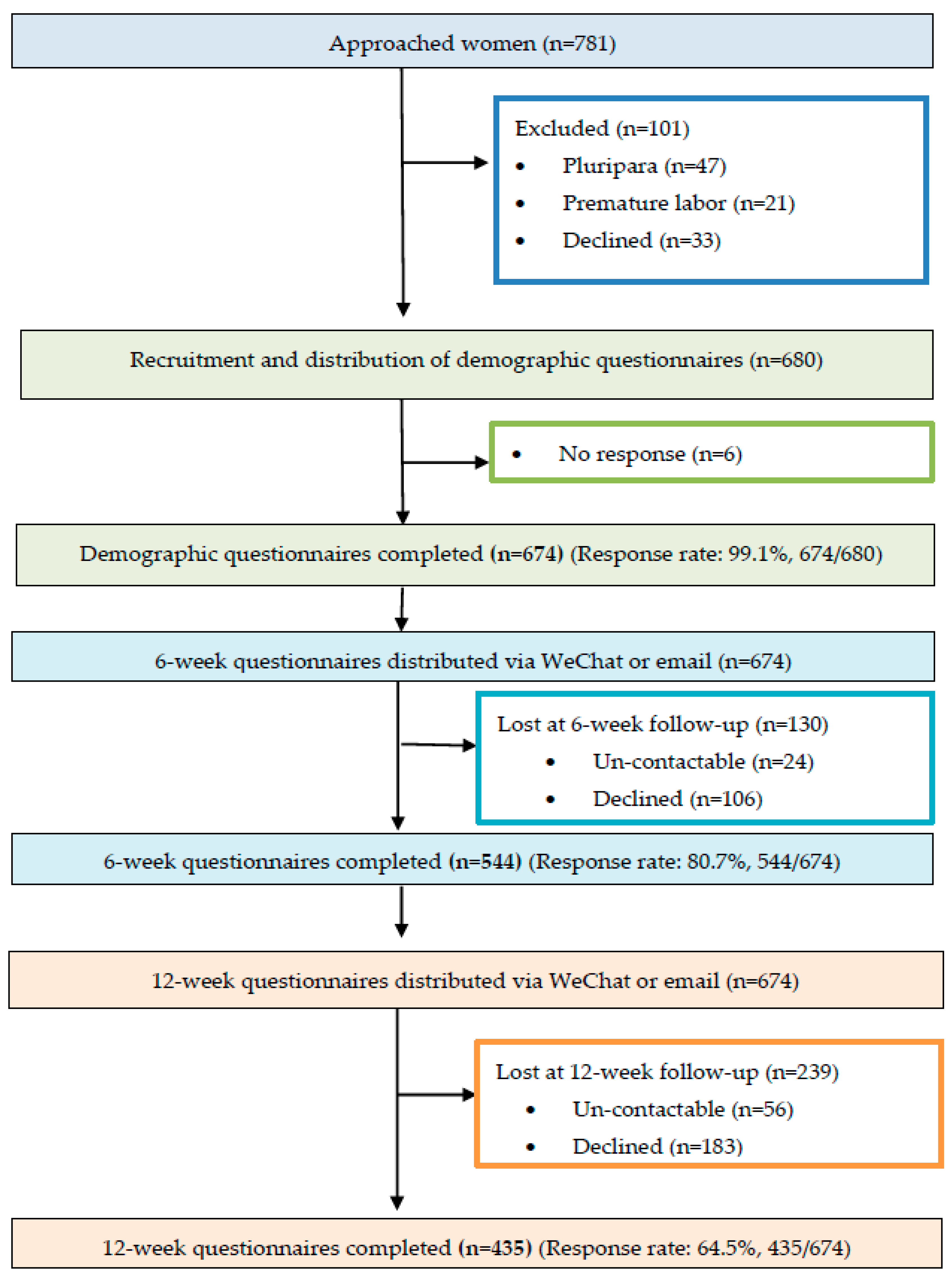
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Socio-Demographic Questionnaire
2.3.2. SICS
2.3.3. EPDS
2.3.4. PSSS
2.4. Data Analysis
3. Results
3.1. Participant Profile
3.2. MSE
3.2.1. The Mean Scores of SICS
3.2.2. Comparison of the Mean SICS Scores at 6 and 12 Weeks Postpartum
3.3. Postpartum Depression
3.3.1. Mean EPDS Scores
3.3.2. Comparison of the Mean EPDS Scores at the Two Time Points
3.4. Postnatal Social Support
3.4.1. The Mean PSSS Scores
3.4.2. Comparison of the Mean PSSS Scores at 6 and 12 Weeks Postpartum
4. Discussion
4.1. MSE
4.2. Postpartum Depression
4.3. Social Support
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhao, Y.J.; Kang, B.; Liu, Y.W.; Li, Y.C.; Shi, G.Q.; Shen, T.; Jiang, Y.; Zhang, M.; Zhou, M.G.; Wang, L.M.; et al. Health insurance coverage and its impact on medical cost: Observations from the floating population in China. PLoS ONE 2014, 9, e111555. [Google Scholar] [CrossRef] [PubMed]
- Davis, D. The emergence of a new urban China: Insider’s perspectives. Contemp. Soc. 2013, 42, 860–861. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Report on the Development of Chinese Floating Population in 2018. Available online: https://www.dyhzdl.cn/k/doc/c504711cbc23482fb4daa58da0116c175e0e1e73.html (accessed on 7 January 2021).
- Luo, Y.; Li, M.L. Research progress on the current situation of reproductive health knowledge-attitude-practice and its influencing factors of female floating population. Chin. J. Mod. Nurs. 2016, 22, 2499–2502. [Google Scholar]
- Zong, Z.H.; Huang, J.Y.; Sun, X.M.; Mao, J.S.; Shu, X.Y.; Hearst, N. Prenatal care among rural to urban migrant women in China. BMC Pregnancy Childb. 2018, 18, 301. [Google Scholar] [CrossRef]
- Luo, X.Q.; Gui, J.F. Analysis on the practice and cause factors of participation in medical insurance program for urban workers by migrants in cities. Popul. Dev. 2014, 6, 109. [Google Scholar]
- Cai, X.Z.; Yang, F.; Bian, Y. Gap analysis on hospitalized health service utilization in floating population covered by different medical insurances: Case study from Jiangsu Province, China. Int. Equity Health 2019, 18, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.H.; Wang, T.; Fu, J.X.; Chen, M.Z.; Meng., Y.T.; Luo., Y. Access to reproductive health services among the female floating population of childbearing age: A cross-sectional study in Changsha, China. BMC Health Serv. Res. 2019, 19, 54. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zhang, Y.; Li, X.; Ye, Z.; Huang, L.; Zhang, Y.; Zheng, X. Exploring maternal self-efficacy of first-time mothers among rural-to-urban floating women: A quantitative longitudinal study in China. Int. J. Environ. Res. Public Health 2021, 18, 2793. [Google Scholar] [CrossRef]
- Salonen, A.H.; Kaunonen, M.; Astedt-Kurki, P.; Järvenpää, A.L.; Isoaho, H.; Tarkka, M.T. Effectiveness of an internet-based intervention enhancing Finnish parents’ parenting satisfaction and parenting self-efficacy during the postnatal period. Midwifery 2011, 27, 832–841. [Google Scholar] [CrossRef]
- Law, K.H.; Dimmock, J.; Guelfi, K.J.; Jackson, B. Stress, depressive symptoms, and maternal self-efficacy in first-time mothers: Modelling and predicting change across the first six months of motherhood. Appl. Psychol. Health Well Being 2019, 11, 126–147. [Google Scholar] [CrossRef] [Green Version]
- Leahy-Warren, P.; McCarthy, G. Maternal parental self-efficacy in the postpartum period. Midwifery 2011, 27, 802–810. [Google Scholar] [CrossRef]
- Zheng, X.J.; Morrell, J.; Watts, K. An Exploration of Factors which Influence Maternal Self-Efficacy in Primiparous Women in China during the Initial Postnatal Period. Ph.D. Thesis, The University of Nottingham, Nottingham, UK, 2015. [Google Scholar]
- Zheng, X.J.; Morrell, J.; Watts, K. Changes in maternal self-efficacy, postnatal depression symptoms and social support among Chinese primiparous women during the initial postpartum period: A longitudinal study. Midwifery 2018, 62, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montigny, F.; Lacharite, C. Perceived parental self-efficacy: Concept analysis. J. Adv. Nurs. 2005, 49, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Li, X.W.; Liu, Y. Parent-Grandparent Coparenting Relationship, maternal parenting self-efficacy, and young children’s social competence in Chinese urban families. J. Child Fam. Stud. 2019, 28, 1145–1153. [Google Scholar] [CrossRef]
- Kohlhoff, J.; Barnett, B. Parenting self-efficacy: Links with maternal depression, infant behaviour and adult attachment. Early Hum. Dev. 2013, 89, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Leahy-Warren, P.; McCarthy, G.; Corcoran, P. First-time mothers: Social support, maternal parental self-efficacy and postnatal depression. J. Clin. Nurs. 2012, 21, 388–397. [Google Scholar] [CrossRef]
- Yap, D.F.F.; Nasir, N.; Tan, K.S.M.; Lau, L.H.S. Variables which predict maternal self-efficacy: A hierarchical linear regression analysis. J. Appl. Res. Intellect. Disabil. 2019, 32, 841–848. [Google Scholar] [CrossRef]
- Azmoude, E.; Jafarnejade, F.; Mazlom, S.R. The predictors for maternal self-efficacy in early parenthood. J. Midwifery. Reprod. Health 2015, 3, 368–376. [Google Scholar]
- Zheng, X.J.; Morrell, J.; Watts, K. A quantitative longitudinal study to explore factors which influence maternal self-efficacy among Chinese primiparous women during the initial postpartum period. Midwifery 2018, 59, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Daley, A.; Jolly, K.; MacArthur, C. The effectiveness of exercise in the management of post-natal depression: Systematic review and meta-analysis. Fam. Pract. 2009, 26, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.; Mello, M.C.D.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: A systematic review. Bull. World Health Organ. 2012, 90, 139–149. [Google Scholar] [CrossRef]
- Zhao, J.Z. The analysis of risk factors for postnatal depression and its nursing measurements. Chinese Gen. Pract. Nurs. 2012, 30, 2821–2822. [Google Scholar]
- Gao, L.L.; Chan, S.W.; Sun, K. Effects of an interpersonal-psychotherapy-oriented childbirth education program for Chinese first-time childbearing women at 3-month follow-up: Randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chan, S.W.; Chong, Y.S.; He, H.G. Predictors of maternal parental self-efficacy among primiparous women in the early postnatal period. Western. J. Nurs. Res. 2015, 37, 1604–1622. [Google Scholar] [CrossRef]
- Tietjen, A.M.; Bradley, C.F. Social support and maternal psychosocial adjustment during the transition to parenthood. Can. J. Behav. Sci. 1985, 17, 109–121. [Google Scholar] [CrossRef]
- House, J. Work, Stress and Social Support; Addison-Wesley Publishing Company: Reading, MA, USA, 1981. [Google Scholar]
- Zang, S.M.; Sheng, Y. Study on influencing factors of maternal self-efficacy in primiparous women. Chin. J. Mod. Nurs. 2010, 16, 2980–2982. [Google Scholar]
- Shorey, S.; Chan, S.W.; Chong, Y.S.; He, H.G. Maternal parental self-efficacy in newborn care and social support needs in Singapore: A correlational study. J. Clin. Nurs. 2014, 23, 2272–2283. [Google Scholar] [CrossRef] [PubMed]
- Prasopkittikun, T.; Tilokskulchai, F. Self-efficacy in Infant Care Scale: Revision and further. Nurs. Health Sci. 2010, 12, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh postnatal depression scale. Br. J. Psychiatry. 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Q.; Guo, X.J.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh postnatal depression scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zheng, X.X. The relationship between social support and postnatal depression of primiparous women. Chi. J. Nurs. 2001, 36, 731–733. [Google Scholar]
- Porter, C.H.; Hsu, H.C. First-time mothers ’perceptions of efficacy during the transition to motherhood: Links to infant temperament. J. Fam. Psychold. 2003, 17, 54–64. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control, 1st ed.; Freeman and Co.: New York, NY, USA, 1997. [Google Scholar]
- Fogel, A.; Nelson-Goens, G.C.; Hsu, H.; Shapiro, F.A. Do infant smiles reflect different positive emotions. Soc. Dev. 2000, 9, 497–520. [Google Scholar] [CrossRef]
- Haslam, D.M.; Pakenham, K.I.; Smith, A. Social support and postpartum depressive symptomatology, the mediating role of maternal self-efficacy. Infant. Ment. Health J. 2006, 27, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Hewitt, C.; Gilbody, S.; Brealey, S.M.; Paulden, M.; Palmer, S.; Mann, R.; Green, M.; Morrell, J.; Barkham, M.; Light, K.; et al. Methods to identify postnatal depression in primary care: An integrated evidence synthesis and value of information analysis. Health Technol. Assess. 2009, 13, 1–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthey, S. Calculating clinically significant change in postnatal depression studies using the Edinburgh postnatal depression scale. J. Affect. Disord. 2004, 78, 269–272. [Google Scholar] [CrossRef]
- China Research Center on Aging. A Compilation of Survey Data on the System of Elderly Support for the Elderly in China; Huangling Press: Beijing, China, 2012; Volume 132. [Google Scholar]
- Ngai, F.W.; Chan, S.W.C.; Ip, W.Y. The effects of a childbirth psychoeducation pro-gram on learned resourcefulness, maternal role competence and perinatal depression: A quasi-experiment. Int. J. Nurs. Stud. 2009, 46, 1298–1306. [Google Scholar] [CrossRef]
- Tarkka, M.T.; Paunonen, M. Social support provided by nurses to recent mothers on a maternity ward. J. Adv. Nurs. 1996, 23, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Jin, X.; Cheng, K.; Caine, E.; Lehman, R.; Xu, D. Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. Int. J. Environ. Res. Public Health 2020, 17, 8686. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| |
| |
|
| Variables | Mean (SD) | Frequency | Percentage (%) |
|---|---|---|---|
| Childbearing age | 25.82 (3.38) | ||
| Marital status | |||
| Married | 674 | 100 | |
| Divorced | 0 | 0 | |
| Single | 0 | 0 | |
| Monthly family income (RMB/Per person) | |||
| <3000 (USD < 420) | 151 | 22.4 | |
| 3001–5000 (USD 420–700) | 286 | 42.4 | |
| >5000 (USD > 700) | 237 | 35.2 | |
| Education | |||
| Middle school graduate or lower | 145 | 21.5 | |
| High school graduate | 347 | 51.5 | |
| University graduate or higher | 182 | 27 | |
| Employment | |||
| Professional | 31 | 4.6 | |
| Unskilled | 415 | 61.6 | |
| Skilled | 49 | 7.3 | |
| Unemployed | 179 | 26.6 | |
| Mode of childbirth | |||
| Natural childbirth | 417 | 61.4 | |
| Assisted childbirth | 119 | 17.5 | |
| C-section | 138 | 20.5 | |
| Baby gender | |||
| Boy | 392 | 58.2 | |
| Girl | 282 | 41.8 |
| Variable | Time Point | Mean (SD) | Minimum | Maximum |
|---|---|---|---|---|
| MSE score | ||||
| (0–100) | 6 weeks | 67.16 (14.35) | 37.17 | 98.91 |
| 12 weeks | 68.71 (15.00) | 37.39 | 99.57 | |
| Developmental Promotion | ||||
| (0–100) | 6 weeks | 73.32 (12.93) | 32.67 | 100.00 |
| 12 weeks | 75.88 (12.72) | 45.33 | 100.00 | |
| General Health Care | ||||
| (0–100) | 6 weeks | 49.19 (17.32) | 10.67 | 98.67 |
| 12 weeks | 53.13 (20.06) | 13.33 | 99.33 | |
| Safety | ||||
| (0–100) | 6 weeks | 84.26 (13.00) | 51.67 | 100.00 |
| 12 weeks | 83.79 (13.53) | 50.00 | 100.00 | |
| Diet | ||||
| (0–100) | 6 weeks | 74.70 (14.79) | 38.80 | 100.00 |
| 12 weeks | 71.60 (19.30) | 17.50 | 100.00 |
| Variable | Time Point | Mean (SD) | Paired Differences Mean (95% CI) | t Value | p Value |
|---|---|---|---|---|---|
| MSE score | |||||
| (0–100) | 6 weeks | 65.28 (14. 90) | 3.44 (2.79, 4.09) | 10.362 | <0.001 |
| 12 weeks | 68.71 (15.01) | ||||
| Developmental Promotion | 4.28 (3.54, 5.02) | 11.360 | <0.001 | ||
| 6 weeks | 71.59 (13.44) | ||||
| 12 weeks | 75.88 (12.72) | ||||
| General Health Care | 6.24 (5.12, 7.35) | 11.006 | <0.001 | ||
| 6 weeks | 46.89 (20.98) | ||||
| 12 weeks | 53.13 (20.06) | ||||
| Safety | 1.20 (0.40, 2.01) | 2.947 | 0.003 | ||
| 6 weeks | 82.58 (13.61) | ||||
| 12 weeks | 83.78 (13.53) | ||||
| Diet | 1.42 (0.58, 2.25) | 3.321 | 0.001 | ||
| 6 weeks | 71.60 (19.30) | ||||
| 12 weeks | 73.02 (15.53) |
| Variable | Time Point | Mean (SD) | Frequency | Percentage (%) |
|---|---|---|---|---|
| EPDS score | ||||
| 6 weeks | 11.19 (4.89) | |||
| 12 weeks | 11.18 (5.34) | |||
| EPDS scores of 10 or above | ||||
| 6 weeks | 296 | 54.4 | ||
| 12 weeks | 220 | 50.6 | ||
| EPDS scores of 13 or above | ||||
| 6 weeks | 218 | 40.1 | ||
| 12 weeks | 154 | 35.4 |
| EPDS | 6 Weeks | 12 Weeks | t/X2 Value | p Value |
|---|---|---|---|---|
| Mean (SD) a | 11. 95 (4.90) | 11.18 (5.35) | 5.536 | <0.001 |
| Threshold b N (%) | ||||
| ≥10 | 269 (61.8) | 220 (50.6) | __ | <0.001 |
| <10 | 166 (38.2) | 215 (49.4) | ||
| ≥13 | 208 (47.8) | 154 (35.4) | __ | 0.003 |
| <13 | 227 (52.2) | 281 (64.6) |
| Variable | Time Point | Mean (SD) | Minimum | Maximum |
|---|---|---|---|---|
| PSSS score | ||||
| (0–60) | 6 weeks | 37.04 (10.15) | 15 | 60 |
| 12 weeks | 38.68 (10.46) | 11 | 60 | |
| Emotional Support | ||||
| (0–20) | 6 weeks | 10.62 (2.67) | 4 | 15 |
| 12 weeks | 10.95 (2.61) | 4 | 15 | |
| Material support | ||||
| (0–20) | 6 weeks | 10.44 (3.22) | 2 | 15 |
| 12 weeks | 10.41 (3.02) | 2 | 15 | |
| Informational support | ||||
| (0–20) | 6 weeks | 7.02 (3.10) | 0 | 15 |
| 12 weeks | 7.79 (3.33) | 2 | 15 | |
| Evaluation of support | ||||
| (0–20) | 6 weeks | 8.96 (2.98) | 2 | 15 |
| 12 weeks | 9.53 (3.09) | 2 | 15 |
| Variable | Time Point | Mean (SD) | Paired Differences Mean (95%CI) | t Value | p Value |
|---|---|---|---|---|---|
| PSSS score | 2.72 (2.11, 3.33) | 8.774 | <0.001 | ||
| 6 weeks | 35.95 (10.36) | ||||
| 12 weeks | 38.68 (10.46) | ||||
| Emotional Support | 0.61 (0.39, 0.83) | 5.426 | <0.001 | ||
| 6 weeks | 10.34 (2.74) | ||||
| 12 weeks | 10.95 (2.61) | ||||
| Material support | 0.29 (0.06, 0.51) | 2.501 | 0.013 | ||
| 6 weeks | 10.12 (3.28) | ||||
| 12 weeks | 10.41 (3.02) | ||||
| Informational support | 0.85 (0.59, 1.10) | 6.565 | <0.001 | ||
| 6 weeks | 6.94 (3.21) | ||||
| 12 weeks | 7.79 (3.33) | ||||
| Evaluation of support | 0.98 (0.77, 1.20) | 8.980 | <0.001 | ||
| 6 weeks | 8.55 (2.99) | ||||
| 12 weeks | 9.53 (3.09) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, J.; Ye, Z.; Fang, Q.; Huang, L.; Zheng, X. Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population. Healthcare 2021, 9, 1516. https://doi.org/10.3390/healthcare9111516
Zhu J, Ye Z, Fang Q, Huang L, Zheng X. Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population. Healthcare. 2021; 9(11):1516. https://doi.org/10.3390/healthcare9111516
Chicago/Turabian StyleZhu, Jiemin, Ziwen Ye, Qiyu Fang, Lingling Huang, and Xujuan Zheng. 2021. "Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population" Healthcare 9, no. 11: 1516. https://doi.org/10.3390/healthcare9111516
APA StyleZhu, J., Ye, Z., Fang, Q., Huang, L., & Zheng, X. (2021). Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population. Healthcare, 9(11), 1516. https://doi.org/10.3390/healthcare9111516