
Functional Settings of Hospital Outdoor Spaces and the Perceptions from Public and Hospital Occupant during COVID-19


Abstract
:
1. Introduction
2. Methods and Materials
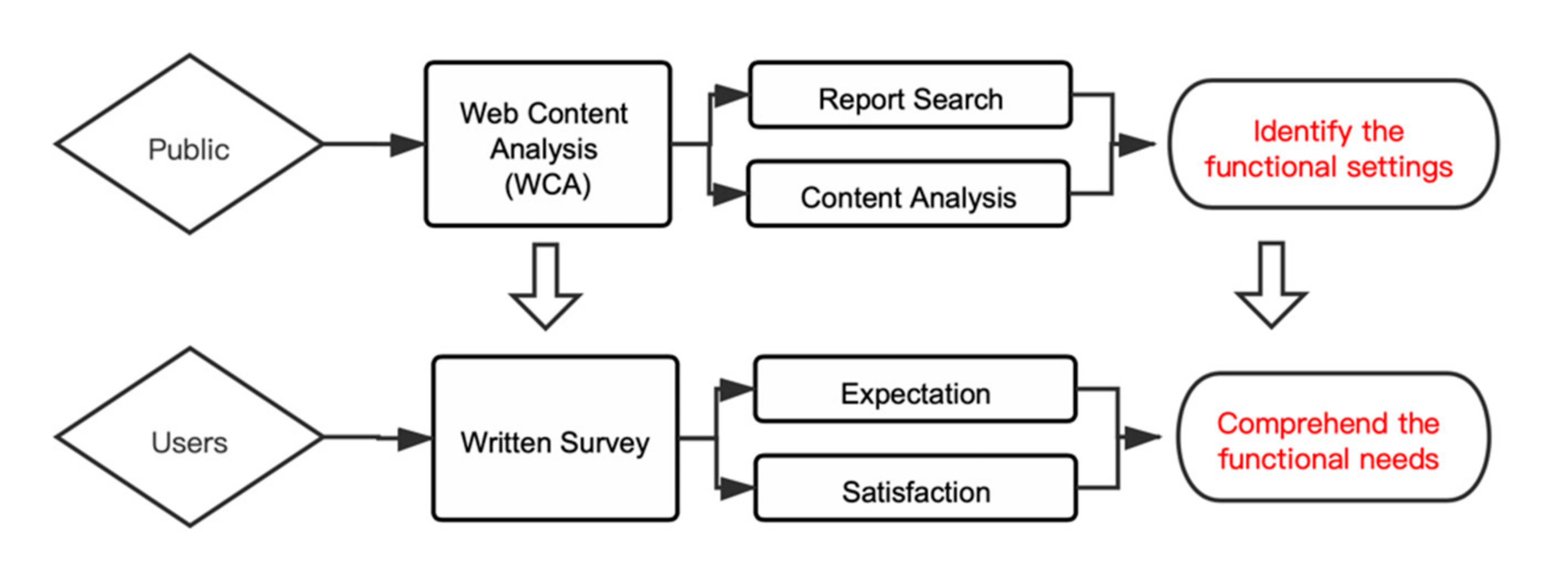
2.1. Instruments
2.1.1. Web Content Analysis
2.1.2. Web-Based Survey
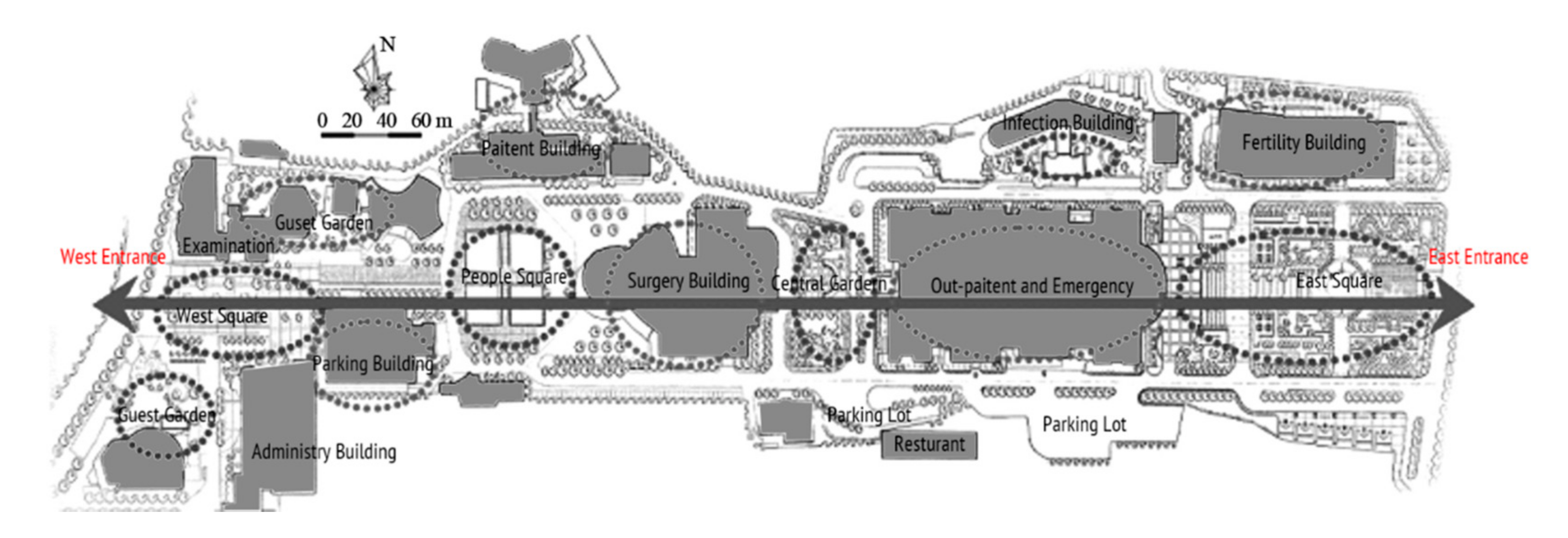
2.2. Data Source and Collection
2.3. Statistical Analysis
3. Results
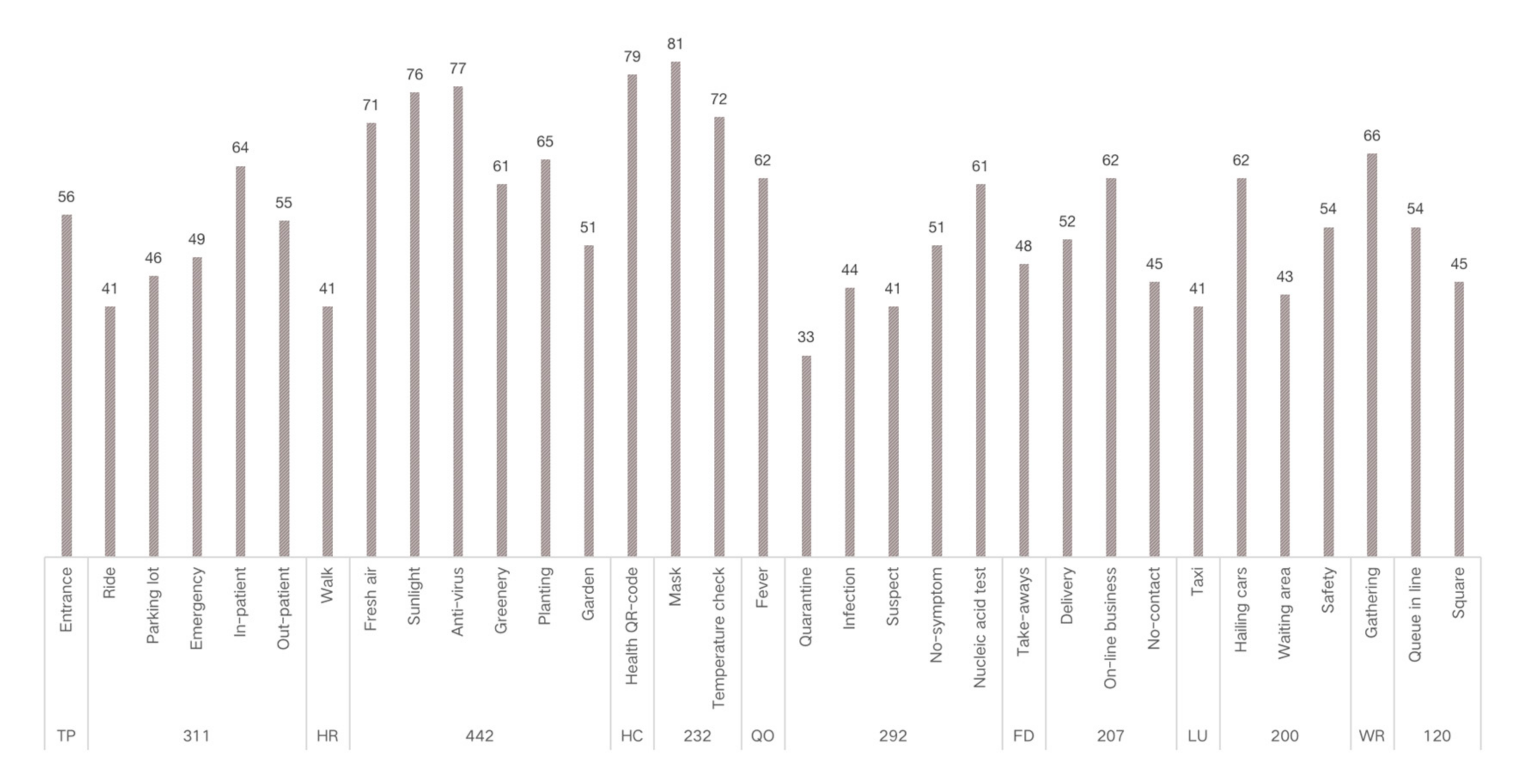
3.1. Functional Setting of Outdoor Space in the Hospital during COVID-19
3.2. Demographic Information
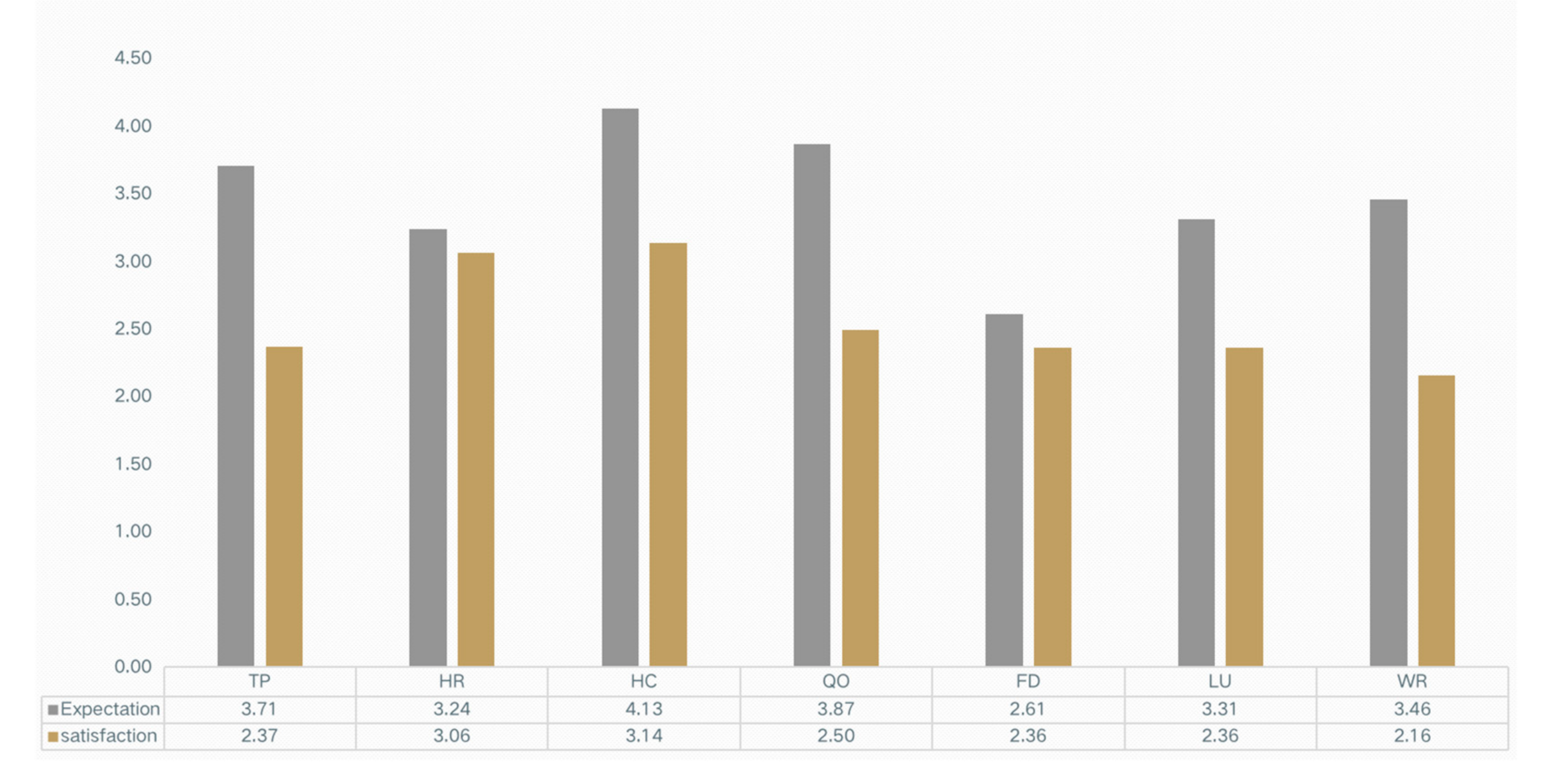
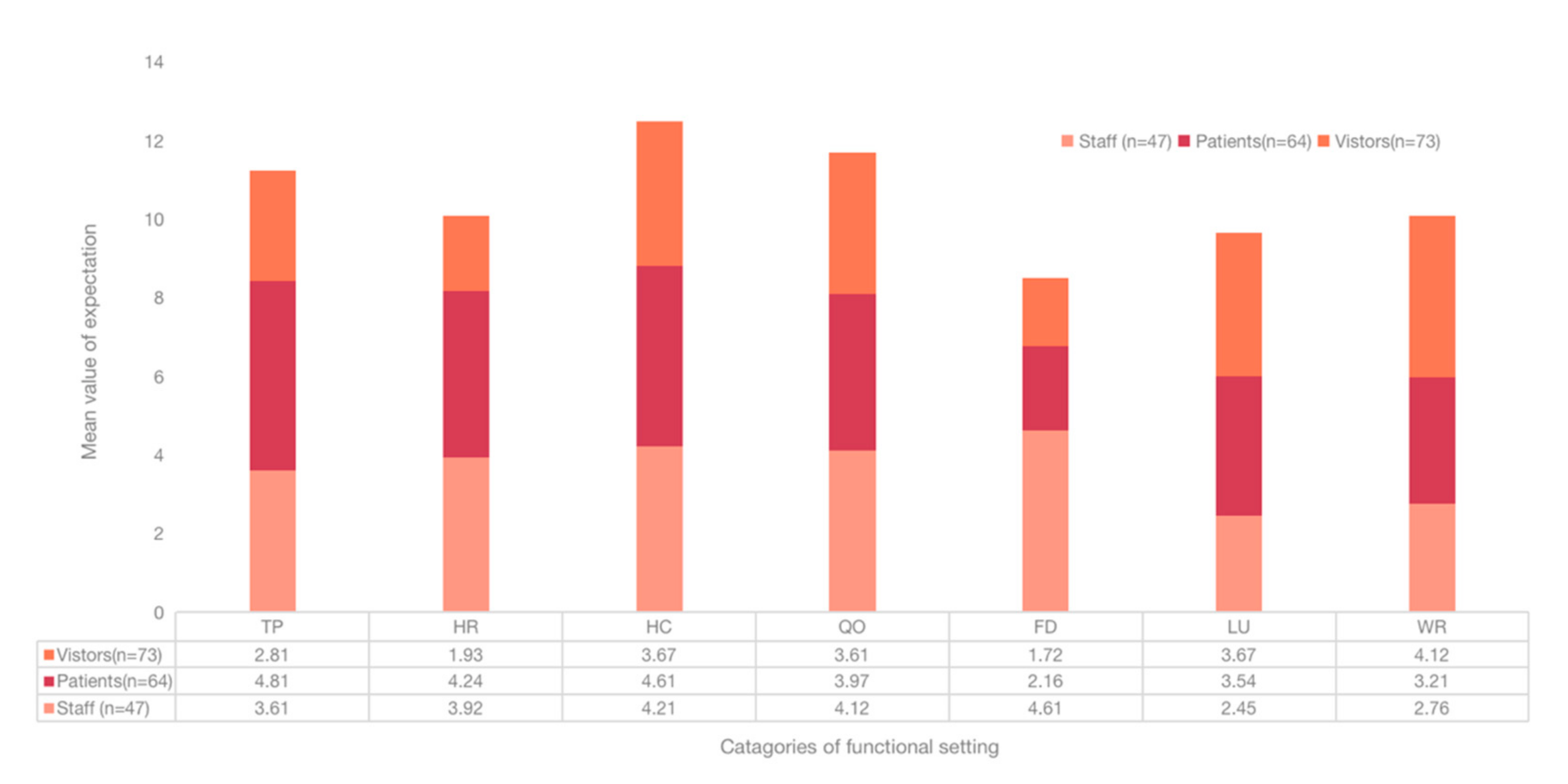
3.3. User Expectations of the Functional Settings of Outdoor Spaces
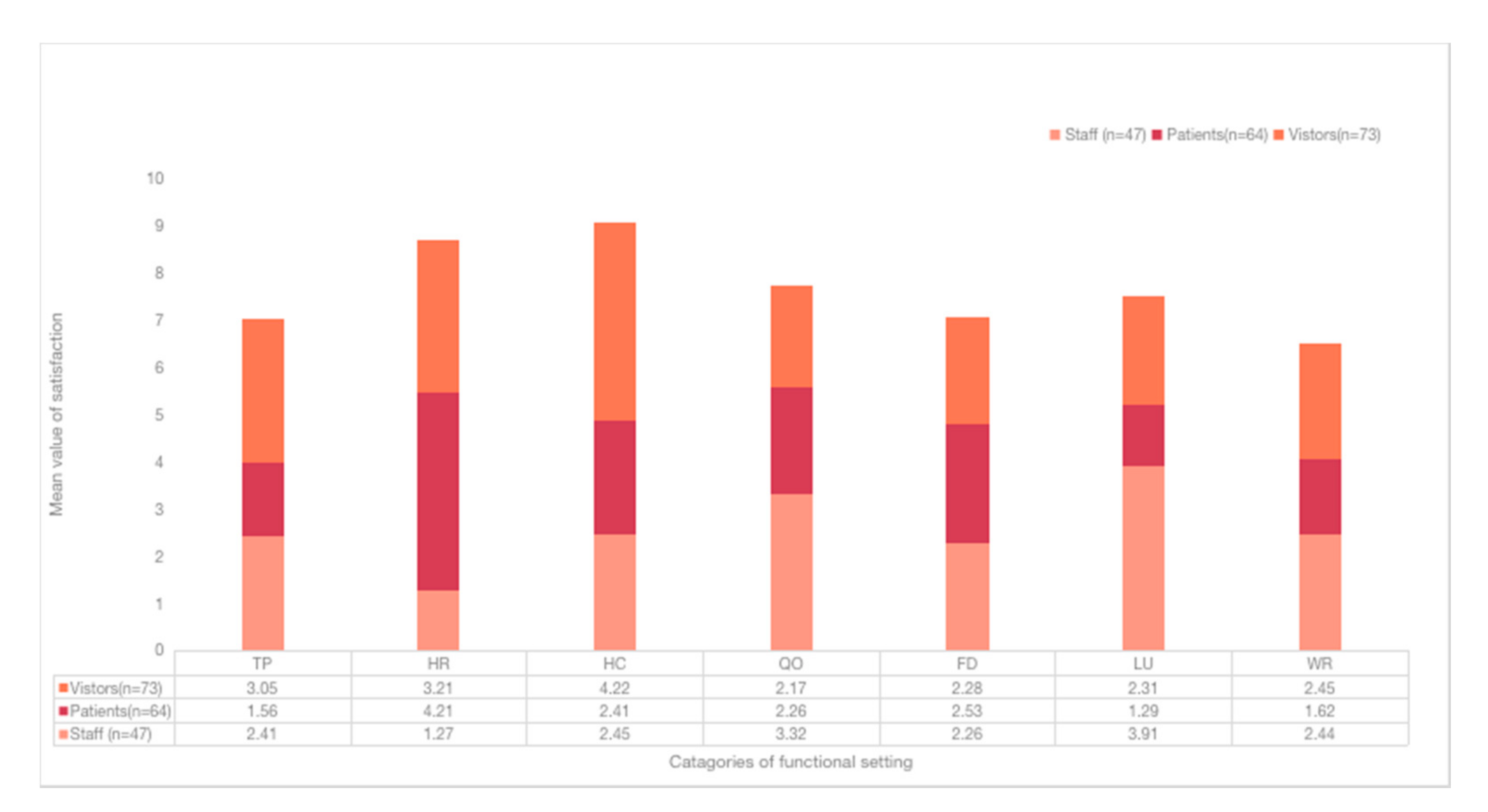
3.4. Satisfaction of the Functional Setting
4. Discussion
4.1. Influence of the Pandemic and Outdoor Space in the Hospital
4.2. Satisfaction with the Current Functional Setting of the Outdoor Space
4.3. What Are the Expected Functional Settings of an Outdoor Space?
4.4. The Role of Groups on the Respondents
4.5. Advice to the Practice
4.6. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Traffic Statistics of Three Selected Websites

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Global Rank | Chinese Rank | Gateway Site Rank | Daily Traffic | |
|---|---|---|---|---|
| People.com.cn | 626 | 22 | 6 | 2,478,214 |
| China.com.cn | 19,238 | 194 | 12 | 103,179 |
| Xinhuanet.com | 16 | 92 | 9 | 149,126,786 |
Appendix B. Questionnaire for Respondents’ Expectations and Satisfaction of the Functional Settings of the Outdoor Space at the Southwest Hospital
| Individual Information | |||||
|---|---|---|---|---|---|
| Role | Patient | Visitor | Staff | ||
| Age | |||||
| Gender | |||||
| Education Level | Junior college and below | Undergraduate | Master’s degree and above | ||
| Expectations on the seven functional settings of outdoor space at the hospital | |||||
| Instruction: how do you feel about the importance and necessity of the seven functional settings in the outdoor space, during and after COVID-19? Please rate from 1–5; 1 (not necessary or important), 5 (very necessary or important). | |||||
| 1 | 2 | 3 | 4 | 5 | |
| Health check (HC) | |||||
| Quarantine and observation (QO) | |||||
| Food and delivery (FD) | |||||
| Healing and restoration (HR) | |||||
| Transportation and parking (TP) | |||||
| Waiting and rest (WR) | |||||
| Load and unload (LU) | |||||
| Satisfaction on the seven functional settings of the outdoor space at the hospital | |||||
| Instruction: do you feel satisfied with the seven functional settings currently in the outdoor space, during and after COVID-19? Please rate from 1–5; 1 (not satisfied at all), 5 (very satisfied). | |||||
| 1 | 2 | 3 | 4 | 5 | |
| Health check (HC) | |||||
| Quarantine and observation (QO) | |||||
| Food and delivery (FD) | |||||
| Healing and restoration (HR) | |||||
| Transportation and parking (TP) | |||||
| Waiting and rest (WR) | |||||
| Load and unload (LU) | |||||
| Any recommendations and feedback regarding the current outdoor space. | |||||
References
- Megahed, N.A.; Ghoneim, E.M. Antivirus-built environment: Lessons learned from COVID-19 pandemic. Sustain. Cities Soc. 2020, 61, 102350. [Google Scholar] [CrossRef] [PubMed]
- Zimring, C.; Jacob, J.T.; Denham, M.E.; Kamerow, D.B.; Hall, K.K.; Cowan, D.Z.; Kasali, A.; Lenfestey, N.F.; Do, E.; Steinberg, J.P. The Role of Facility Design in Preventing the Transmission of Healthcare-Associated Infections: Background and Conceptual Framework. HERD: Health Environ. Res. Des. J. 2013, 7, 18–30. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.B.; Choi, Y.S.; Quan, X.; Joseph, A. A review of the research literature on evidence-based healthcare design. HERD: Health Environ. Res. Des. J. 2008, 1, 61–125. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.A. COVID-19 and the Need for More Accessible and Designed Hospital Outdoor Spaces in Developing Countries. HERD: Health Environ. Res. Des. J. 2021, 14, 368–372. [Google Scholar] [CrossRef]
- Capolongo, S.; Gola, M.; Brambilla, A.; Morganti, A.; Mosca, E.I.; Barach, P. COVID-19 and Healthcare Facilities: A Decalogue of Design Strategies for Resilient Hospitals. Acta Biomed. 2020, 91, 50–60. [Google Scholar] [CrossRef]
- Shu, L.; Ji, N.; Chen, X.; Feng, G. Ark of Life and Hope: The role of the Cabin Hospital in facing COVID-19. J. Hosp. Infect. 2020, 105, 351–352. [Google Scholar] [CrossRef]
- Sacchetto, D.; Raviolo, M.; Beltrando, C.; Tommasoni, N. COVID-19 surge capacity solutions: Our experience of converting a concert hall into a temporary hospital for mild and moderate COVID-19 patients. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef]
- Yuan, Y.; Qiu, T.; Wang, T.; Zhou, J.; Ma, Y.; Liu, X.; Deng, H. The application of Temporary Ark Hospitals in controlling COVID-19 spread: The experiences of one Temporary Ark Hospital, Wuhan, China. J. Med. Virol. 2020, 92, 2019–2026. [Google Scholar] [CrossRef]
- Gardens, H. Therapeutic Benefits and Design Recommendations; Cooper Marcus, C., Barnes, M., Eds.; Wiley: New York, NY, USA, 1999. [Google Scholar]
- Beaudry, A.; Laporte, G.; Melo, T.; Nickel, S. Dynamic transportation of patients in hospitals. OR Spectr. 2010, 32, 77–107. [Google Scholar] [CrossRef] [Green Version]
- Madureira, H.; Nunes, F.; Oliveira, J.V.; Madureira, T. Preferences for Urban Green Space Characteristics: A Comparative Study in Three Portuguese Cities. Environments 2018, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Roberts, G.L. Shades of green: The evolution of hospital sustainable design standards. Health Facil Manag. 2011, 24, 45–46. [Google Scholar]
- Lee, A.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Leigh, H. The Patient: Biological, Psychological, and Social Dimensions of Medical Practice; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Hartig, T.; van den Berg, A.E.; Hagerhall, C.M.; Tomalak, M.; Bauer, N.; Hansmann, R.; Ojala, A.; Syngollitou, E.; Carrus, G.; Van Herzele, A. Health benefits of nature experience: Psychological, social and cultural processes. In Forests, Trees and Human Health; Springer: Berlin, Germany, 2011; pp. 127–168. [Google Scholar]
- Ulrich, R.S.; Zhu, X. Medical complications of intra-hospital patient transports: Implications for architectural design and research. HERD: Health Environ. Res. Des. J. 2007, 1, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Nourmusavi Nasab, S.; Karimi Azeri, A.R.; Mirbazel, S. Ideal physical features of environmental design in children’s hospital: Using children’s perspectives. Facilities 2019, 38, 445–466. [Google Scholar] [CrossRef]
- Linebaugh, K.B. A Systematic Literature Review on Healing Environments in the Inpatient Health Care Setting; The University of Arizona: Tucson, AZ, USA, 2013. [Google Scholar]
- Ulrich, R.; Quan, X.; Joseph, A.; Chou D Hary, R.; Zimring, C. The Role of the Physical Environment in the Hospital of the 21st Century: A Once-in-a-Lifetime Opportunity; Center Health Design: Concord, CA, USA, 2004. [Google Scholar]
- Abdul Shukor, S.F.; Stigsdotter, U.K.; Nilsson, K. A Review of Design Recommendations for Outdoor Areas at Healthcare Facilities. J. Ther. Hortic. 2012, 22, 32–47. [Google Scholar]
- Peterson, K.H.J.; Muckey, E.J.C. Deployment and Operation of Outdoor Treatment Tents During the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef]
- Fang, D.P.; Pan, S.J.; Li, Z.S.; Yuan, T.; Jiang, B.R.; Gan, D.; Sheng, B.; Han, J.; Wang, T.; Liu, Z.M. Large-scale public venues as medical emergency sites in disasters: Lessons from COVID-19 and the use of Fangcang shelter hospitals in Wuhan, China. BMJ Glob. Health 2020, 5, 2059–7908. [Google Scholar] [CrossRef]
- Qian, H.; Miao, T.; Liu, L.; Zheng, X.; Luo, D.; Li, Y. Indoor transmission of SARS-CoV-2. Indoor Air 2021, 31, 639–645. [Google Scholar] [CrossRef]
- Crompton, J.L. Evolution of the “parks as lungs” metaphor: Is it still relevant? World Leis. J. 2017, 59, 1607–8055. [Google Scholar] [CrossRef]
- Naomi, A.S. Access to nature has always been important; with COVID-19, it is essential. HERD: Health Environ. Res. Des. J. 2020, 13, 242–244. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A.; Alyahya, S.A.; Alshehri, R.; Alqadi, K.; Alasmari, S. Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia. In Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2021; p. 854. [Google Scholar]
- Herring, S.C. Web content analysis: Expanding the paradigm. In International Handbook of Internet Research; Springer: Berlin/Heidelberg, Germany, 2009; pp. 233–249. [Google Scholar]
- Zeisel, J. Inquiry by Design: Environment/Behavior/Neuroscience in Architecture, Interiors, Landscape, and Planning; W.W. Nort. Co.: New York, NY, USA, 2006. [Google Scholar]
- McMillan, S.J. The Microscope and the Moving Target: The Challenge of Applying Content Analysis to the World Wide Web. Journal. Mass Commun. Q. 2000, 77, 80–98. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Rong, J.; Peng, L.; Yang, J.; Cong, G.; Fang, J. Analysis of Social Effects on Employment Promotion Policies for College Graduates Based on Data Mining for Online Use Review in China during the COVID-19 Pandemic. In Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2021; p. 846. [Google Scholar]
- Fu, Y.Q.; Wang, X.J.; Zheng, X.M. Study on Tourism Image Based on Web Text Analysis: Case of Gulangyu. Tour. Forum 2012, 5, 59–66. [Google Scholar]
- Chen, T.; Peng, L.; Yang, J.; Cong, G. Analysis of User Needs on Downloading Behavior of English Vocabulary APPs Based on Data Mining for Online Comments. Mathematics 2021, 9, 1341. [Google Scholar] [CrossRef]
- Karanikola, P.; Andrea, V.; Tampakis, S.; Tsolakidou, A. Indoor and Outdoor Design in Healthcare Environments: The Employees’ Views in the General University Hospital of Alexandroupolis, Greece. Environments 2020, 7, 61. [Google Scholar] [CrossRef]
- Harris, D.D.; Detke, L.A. The Role of Flooring as a Design Element Affecting Patient and Healthcare Worker Safety. HERD: Health Environ. Res. Des. J. 2013, 6, 95–119. [Google Scholar] [CrossRef] [PubMed]
- Eijkelenboom, A.; Bluyssen, P.M. Comfort and health of patients and staff, related to the physical environment of different departments in hospitals: A literature review. Intell. Build. Int. 2019, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Nejati, A.; Shepley, M.; Rodiek, S.; Lee, C.; Varni, J. Restorative Design Features for Hospital Staff Break Areas:A Multi-Method Study. HERD: Health Environ. Res. Des. J. 2016, 9, 16–35. [Google Scholar] [CrossRef]
- Chaudhury, H.; Mahmood, A.; Valente, M. The Effect of Environmental Design on Reducing Nursing Errors and Increasing Efficiency in Acute Care Settings A Review and Analysis of the Literature. Environ. Behav. 2009, 41, 755–786. [Google Scholar] [CrossRef]
- Kearney, A.R.; Winterbottom, D. Nearby nature and long-term care facility residents: Benefits and design recommendations. J. Hous. Elder. 2006, 19, 0276–3893. [Google Scholar] [CrossRef]
- Weerasuriya, R.; Henderson-Wilson, C.; Townsend, M. Accessing Green Spaces Within a Healthcare Setting: A Mixed Studies Review of Barriers and Facilitators. HERD: Health Environ. Res. Des. J. 2019, 12, 119–140. [Google Scholar] [CrossRef]
- Commission, F. PG Greenspace Design for Health and Well-Being; Forestry Commission: Edinburgh, UK, 2012. [Google Scholar]
- Pouso, S.; Borja, A.; Fleming, L.E.; Gomez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Lercher, P.; Browning, M.H.E.M.; Stoyanov, D.; Petrova, N.; Novakov, S.; Dimitrova, D.D. Does greenery experienced indoors and outdoors provide an escape and support mental health during the COVID-19 quarantine? Environ. Res. 2021, 196, 0013–9351. [Google Scholar] [CrossRef] [PubMed]
| Context | Architecture Setting | Study Body |
|---|---|---|
| Pandemic COVID-19 Virus | Hospital General hospital Infection disease hospital Temporary hospital | Outdoor space External environment Surrounding environment |
| Main Categories of Functional Settings | Sub-Categories of Functional Settings | Description | The Current Situations (Exampled at the Southwest Hospital) | Problems (Examples at the Southwest Hospital) |
|---|---|---|---|---|
| Health Check (HC) | Health QR-code Face mask Temperature check | To test body temperature, to check health QR code and nucleic acid test reports before entering the buildings. |  | Crowded with different flows. Not enough space. Causing chaos in the entrance and exit. |
| Quarantine and Observation (QO) | Fever Quarantine Infection Suspect Non-symptom Nucleic acid test | To accommodate suspected fever patients and provide temporary medications. |  | Difficult to find. Far from the main out-patient and emergency buildings. No shelters for the waiting crowds. |
| Food and Delivery (FD) | Take-away Delivery On-line business Touchless practice | To pick-up and drop-off deliveries and food. |  | No designated area for delivery and foods. Chaos by the delivery, mingling with other “flows”. Delivery blocks the entrance of the building. |
| Healing and Restoration (HR) | Walk Fresh air Sunlight Greenery Anti-virus | To provide places and resources for patients and staff to recover, relax, and rest. |  | Far from the in-patient and staff buildings. No covered corridor connecting to the building. No smoking prohibited and low environmental qualities. |
| Transportation and Parking (TP) | Entrance Ride Emergency Parking lot In-patient Garden | To provide places and space for transportation and flow. |  | Not enough parking lot space. Chaos of motor flow mingling with pedestrians. Weak connection between public transit and entrance. |
| Waiting and Rest (WR) | Gathering Waiting in queue Square Outpatient | To provide places and space for visitors and patients to rest, gather, and wait. |  | Not enough space for waiting crowds, but large water pool. No shelters in the waiting areas. No buffer zone between waiting area and roads. |
| Load and Unload (LU) | Taxi Hailing cars Waiting area Safety | To provide a place to load and unload people. |  | No designated area for loading and unloading. Chaos of flow, regarding taxis, hailing cars, private cars, and public transit. |
| Staff | Patients | Visitors | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | ||
| Age | <20 | 0 | 0.00% | 2 | 3.13% | 8 | 10.96% | 10 | 5.43% |
| 20–40 | 23 | 48.94% | 6 | 9.38% | 38 | 52.05% | 67 | 36.41% | |
| 40–60 | 20 | 42.55% | 17 | 26.56% | 25 | 34.25% | 62 | 33.70% | |
| >60 | 4 | 8.51% | 39 | 60.94% | 2 | 2.74% | 45 | 24.46% | |
| Gender | Male | 12 | 25.53% | 29 | 45.31% | 41 | 56.16% | 82 | 44.57% |
| Female | 35 | 74.47% | 35 | 54.69% | 32 | 43.84% | 102 | 55.43% | |
| Education | Junior college and below | 0 | 0.00% | 31 | 48.44% | 41 | 56.16% | 72 | 39.13% |
| Undergraduate | 17 | 36.17% | 28 | 43.75% | 29 | 39.73% | 74 | 40.22% | |
| Graduate and above | 30 | 63.83% | 5 | 7.81% | 3 | 4.11% | 38 | 20.65% |
| Variables | TP | HR | HC | QO | FD | LU | WR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T/F | p | T/F | p | T/F | p | T/F | p | T/F | p | T/F | p | T/F | p | ||
| Groups | Expectation | 0.237 | 0.813 | −0.946 | 0.346 | 0.066 | 0.936 | 1.712 | 0.636 | 21.53 | 0.000 | −3.282 | 0.002 | −2.731 | 0.007 |
| Satisfaction | 0.332 | 0.741 | 2.956 | 0.038 | 2.142 | 0.034 | 1.155 | 0.283 | −1.761 | 0.081 | 0.166 | 0.136 | −3.343 | 0.003 | |
| Age | Expectation | 0.215 | 0.832 | 2.679 | 0.021 | 0.069 | 0.945 | 1.921 | 0.165 | 0.472 | 0.639 | 0.084 | 0.892 | 0.021 | 1.839 |
| Satisfaction | 0.806 | 0.421 | −1.084 | 0.281 | 1.195 | 0.234 | 0.914 | 0.639 | 0.906 | 0.311 | 1.341 | 0.163 | 0.713 | 0.435 | |
| Gender | Expectation | 0.753 | 0.453 | −1.003 | 0.318 | 0.17 | 0.866 | 0.221 | 0.639 | 0.453 | 0.753 | 1.097 | 0.146 | 0.235 | 0.641 |
| Satisfaction | −1.896 | 0.071 | −0.295 | 0.769 | 0.554 | 0.581 | 4.714 | 0.095 | −2.196 | 0.051 | 0.754 | 0.482 | 0.199 | 0.889 | |
| Education | Expectation | −0.651 | 0.516 | 2.237 | 0.041 | 1.276 | 0.226 | 0.512 | 0.478 | 11.110 | 0.000 | 1.121 | 0.321 | 1.655 | 0.201 |
| Satisfaction | 1.539 | 0.219 | 1.245 | 0.297 | −1.266 | 0.208 | 0.137 | 0.718 | 9.480 | 0.009 | −1.415 | 0.178 | −2.062 | 0.041 |
| Indicators | Patients (Mean) | Visitors (Mean) | Staff (Mean) | Maximum | Minimum | Differences between Max and Min |
|---|---|---|---|---|---|---|
| TP | 3.61 | 4.81 | 2.81 | 4.81 | 2.81 | 2.00 |
| HR | 3.92 | 4.24 | 1.93 | 4.24 | 1.93 | 2.31 |
| HC | 4.21 | 4.61 | 3.67 | 4.61 | 4.21 | 0.40 |
| QO | 4.12 | 3.97 | 3.61 | 4.12 | 3.61 | 0.51 |
| FD | 4.61 | 2.16 | 1.72 | 4.61 | 1.72 | 2.89 |
| LU | 2.45 | 3.54 | 3.67 | 3.67 | 2.45 | 1.22 |
| WR | 2.76 | 3.21 | 4.12 | 4.12 | 2.76 | 1.36 |
| Indicators | Patients (Mean) | Visitors (Mean) | Staff (Mean) | Maximum | Minimum | Differences between Max and Min |
|---|---|---|---|---|---|---|
| TP | 2.41 | 1.56 | 3.05 | 3.05 | 1.56 | 1.49 |
| HR | 1.27 | 4.21 | 3.21 | 4.21 | 1.27 | 2.94 |
| HC | 2.45 | 2.41 | 4.22 | 4.22 | 2.41 | 1.81 |
| QO | 3.32 | 2.26 | 2.17 | 3.32 | 2.17 | 1.15 |
| FD | 2.26 | 2.53 | 2.28 | 2.53 | 2.26 | 0.27 |
| LU | 3.91 | 1.29 | 2.31 | 3.91 | 1.29 | 2.62 |
| WR | 2.44 | 1.62 | 2.45 | 2.45 | 1.62 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, M.; Adeney, M.; Long, H. Functional Settings of Hospital Outdoor Spaces and the Perceptions from Public and Hospital Occupant during COVID-19. Healthcare 2021, 9, 1534. https://doi.org/10.3390/healthcare9111534
Ma M, Adeney M, Long H. Functional Settings of Hospital Outdoor Spaces and the Perceptions from Public and Hospital Occupant during COVID-19. Healthcare. 2021; 9(11):1534. https://doi.org/10.3390/healthcare9111534
Chicago/Turabian StyleMa, Ming, Michael Adeney, and Hao Long. 2021. "Functional Settings of Hospital Outdoor Spaces and the Perceptions from Public and Hospital Occupant during COVID-19" Healthcare 9, no. 11: 1534. https://doi.org/10.3390/healthcare9111534
APA StyleMa, M., Adeney, M., & Long, H. (2021). Functional Settings of Hospital Outdoor Spaces and the Perceptions from Public and Hospital Occupant during COVID-19. Healthcare, 9(11), 1534. https://doi.org/10.3390/healthcare9111534