1. Introduction
Anxiety is one of the most concerning mental health problems across the world affecting various populations [
1], including adolescents. According to the global data, 6.5% of children and adolescents are suffering from anxiety disorders [
2]. Moreover, under the context of the COVID-19 pandemic, the pooled estimate obtained in the first year of the COVID-19 pandemic suggests that one in five youths was experiencing clinically elevated anxiety symptoms [
3]. Some studies even reported that the prevalence of anxiety symptoms reached more than 30% among adolescents during the COVID-19 pandemic [
4,
5]. Furthermore, anxiety disorders in adolescents can have long-term consequences on the quality of life and are often comorbid with other problems, such as depression, sleep disturbances, and attention-deficit/hyperactivity disorder [
6,
7,
8,
9]. Despite the fairly high prevalence and the psychosocial impairment that comes with anxiety disorders, the public generally has a relatively low understanding of symptoms, and anxiety disorders or symptoms often remain undetected and untreated [
10]. Therefore, it is crucial to have a suitable screening tool to help measure and identify anxiety among adolescents for subsequent treatment as early as possible. A suitable screening instrument should be well-validated, brief, easy to administer and score, able to be interpreted without extensive and professional training, feasible in practice, and free to use if possible.
The Generalized Anxiety Disorder-7 item (GAD-7) is a brief, self-report scale, which was originally developed to measure Generalized Anxiety Disorder, and was validated in primary care settings of the United States [
11]. Researchers have also extended the GAD-7 to screen for other anxiety disorders (e.g., Post-Traumatic Stress Disorder, Social Anxiety Disorder, and Panic Disorder) and found that the GAD-7 performed well for most of the anxiety disorders studied [
10,
12]. With the increasing demand for easy-to-use and effective anxiety scales in various countries, the GAD-7 has been translated into different languages (e.g., Chinese) over the two decades [
13,
14,
15,
16]. The GAD-7 has gradually become a widely used measurement tool in populations with different characteristics, especially adult populations, and showed satisfactory reliability and validity [
17,
18].
Although the GAD-7 has also been used for anxiety screening among adolescents, only a few studies have evaluated its measurement properties in adolescent samples. In a study on adolescents (average age = 16.85 years) in Ghana, the GAD-7 showed adequate internal consistency, a unidimensional structure, and criterion validity [
19]. In a recent study using survey data from 111,171 Finnish adolescents aged 14–18 years, the GAD-7 demonstrated good psychometric properties, including good internal consistency, a unidimensional factor structure, and criterion validity [
20]. In another recent study on young Americans aged 14–26 years with substance use disorders, the GAD-7 also showed excellent internal consistency and construct validity [
21]. However, to the best of our knowledge, there are no psychometric tests of the GAD-7 in Chinese adolescents. The GAD-7 has been translated to Chinese and validated in Chinese outpatients in a general hospital in 2010 [
22]. Since then, the GAD-7 has been validated in other Chinese adult samples in hospital settings [
15,
23,
24] and university students [
25,
26]. Given that adolescents may differently comprehend a questionnaire’s items in the same way as adults do, examining the psychometric properties of the GAD-7 in adolescents is essentially needed.
Additionally, substantial evidence has indicated that female adolescents are more likely to develop anxiety disorders than males [
5,
8,
27]. Prior research has also found that the prevalence of anxiety varies across different periods of adolescence, with more common anxiety symptoms observed in older adolescents [
5,
27]. However, to date, few studies have tested psychometric properties for the GAD-7 by sex and covered adolescents in early to late adolescence. Previous studies have shown that psychometric properties of the GAD-7 were similar across sex or age groups in Ghanian adolescents [
19], Finnish adolescents [
20], and Canadian youth [
28]. All these studies found that GAD-7 scores were higher in females and older adolescents. Nevertheless, the generalizability of these study results to other countries remains unknown, given that discrepancy in the perception of mental distress such as anxiety across cultures has been observed [
29,
30]. Therefore, sex- and age-stratified analyses are needed in examining the GAD-7 in Chinese adolescents.
Using a large sample of more than 60,000 Chinese adolescents, this study had the opportunity to examine the internal consistency, factor structure, and criterion validity of the GAD-7 by sex- and age-stratified analyses. As depression symptoms are frequently found to be comorbid with anxiety symptoms [
8,
31], we adopted depression scores assessed by the Patient Health Questionnaire-9 item (PHQ-9) as a criterion [
32] when examining the criterion validity of the GAD-7. Criterion validity refers to the degree to which two measures of constructs theoretically should be related, also known as convergent validity. The PHQ-9 was adopted to measure depression because it is an easy-to-use and widely used tool and has been proved to have satisfactory psychometric properties in the Chinese general population [
33], as well as Chinese adolescents [
34]. Existing literature has demonstrated that the GAD-7 was highly and positively correlated with the PHQ-9 in adolescents [
19,
20]. Specifically, we expected that the GAD-7 would present good internal consistency, a unidimensional structure, and a high and positive correlation with the PHQ-9 across sex and age groups. This study would provide evidence for whether the GAD-7 is optimal for measuring anxiety symptoms in Chinese adolescents of different sex and age groups.
4. Discussion
As mental health problems in adolescents have been a common public health issue [
3,
38], regular and simple screening tools for specific mental health problems, such as depression and anxiety disorders, are becoming increasingly needed. In this study, we gained convincing evidence that the GAD-7 is a reliable and valid self-reported measure with good psychometric properties in Chinese adolescents aged 10 to 17 years old. To our knowledge, this study is the first one to investigate the psychometric properties of the GAD-7 in Chinese adolescents, which adds evidence that the GAD-7 is a feasible screening tool to identify anxiety symptoms at the population level.
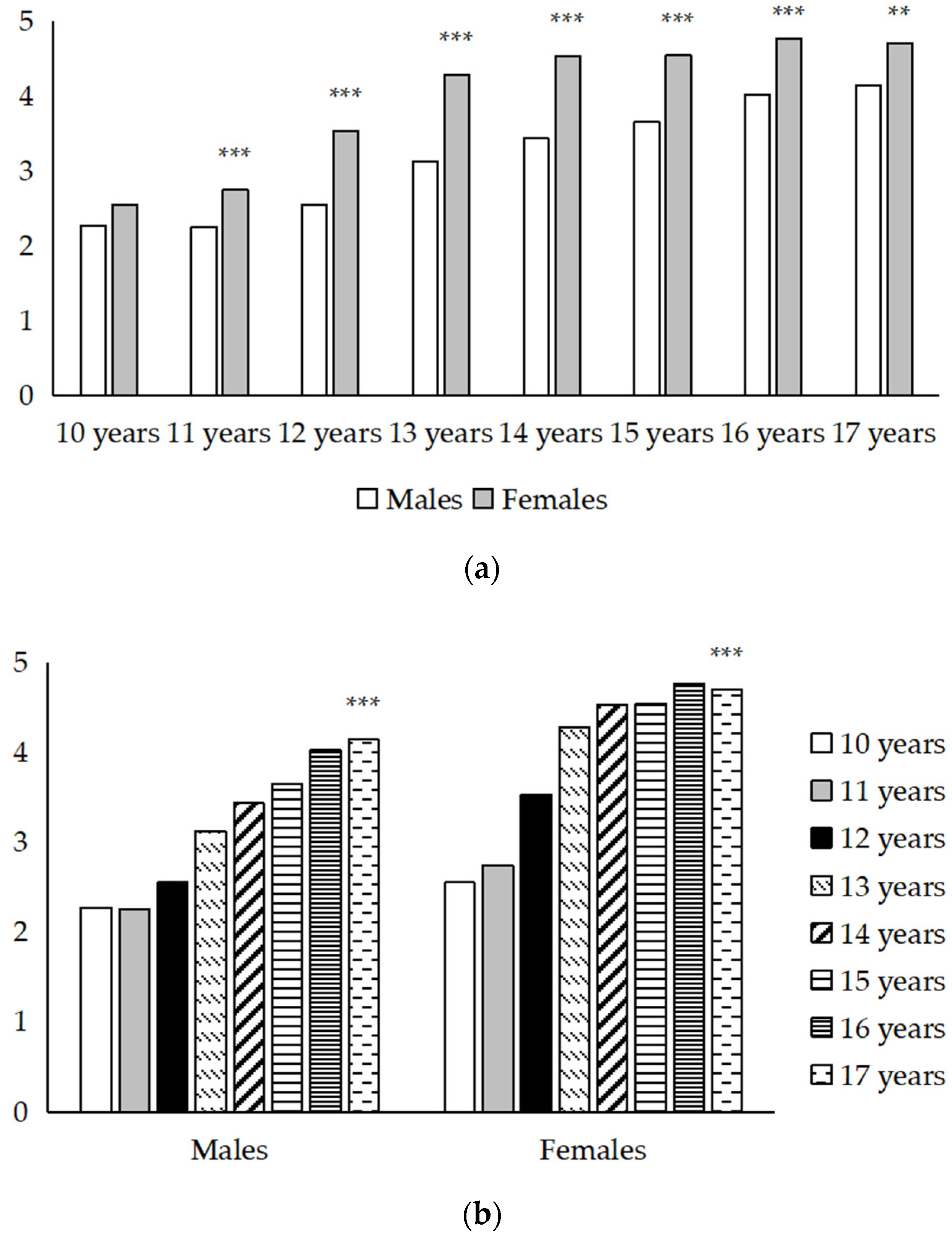
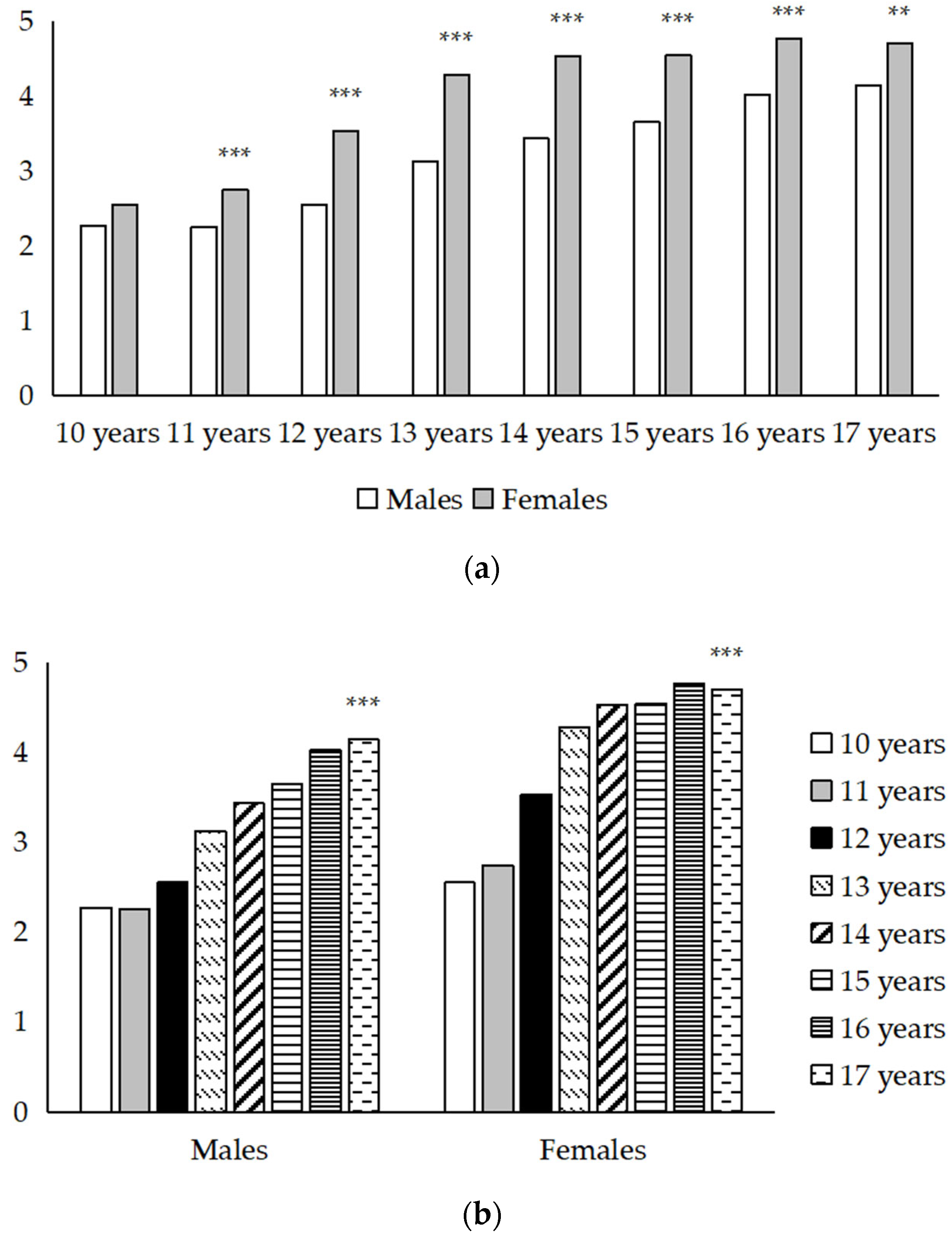
As expected, we apparently found sex and age differences in the GAD-7 scores. Specifically, the GAD-7 scores were higher in females than males, and the GAD-7 scores presented a significant increasing trend as age increased. A study examining the GAD-7 in Finnish adolescents also found that GAD-7 scores were the lowest in the youngest age group (14 years) and the highest in the oldest age group (18 years), although a linear association between the GAD total score and age was not supported in this Finnish study [
20]. The disparity of findings between our study and the Finnish study may be because our study covered a larger age range and, thus, was able to detect the linear trend of increased GAD-7 scores with age.
The Cronbach’s α coefficients of the GAD-7 in adolescents by sex and age ranged from 0.93–0.95, indicating excellent internal consistency. This research finding paralleled the early research in which the Cronbach’s alpha coefficients were at good to excellent levels in different populations [
20,
21,
23,
26,
39]. In our study, Cronbach’s α was at least 0.93 regardless of groups by sex and age; thus, excellent internal reliability of the GAD-7 was verified in Chinese adolescents as well.
The findings of the PCA in this study paralleled previous studies on the GAD-7 based on young adult samples [
26,
39,
40]. Specifically, the results for factor loadings revealed a unidimensional structure with strong loadings (all factor loadings values > 0.6). Furthermore, the results for CFA in sex- and age-specific subgroups were highly similar to those studies that reported good goodness-of-fit indices in the overall sample [
40,
41]. These research findings alongside prior studies indicate that the GAD-7 has good cultural adaptations in different populations. Of note, to our knowledge, our study is the first to investigate the goodness-of-fit of the GAD-7 in adolescents by sex- and age-specific subgroups, which provide persuasive evidence for the applicability of the GAD-7 in different young populations.
When looking at criterion validity, the GAD-7 and the PHQ-9 should be expectedly related, as anxiety and depression co-occur frequently. In this study, the GAD-7 and PHQ-9 scores presented strong correlations (all correlation coefficients in different subgroups > 0.7). Such a correlation between these two mental health problem measures supports some empirical research exploring the comorbidity between anxiety and depression symptoms (measured by the GAD-7 and PHQ-9). For example, increasing studies found that the symptoms of anxiety (measured by the GAD-7) and depression (measured by the PHQ-9) are intercorrelated and directly interacted [
42,
43,
44]. Moreover, researchers have found the GAD-7 performed well beyond measuring generalized anxiety disorder, but is also a useful measure in the mixed anxiety–depression sample [
12]. As criterion validity can also be viewed as an indicator to assess criterion validity, we can deem that the criterion validity of the GAD-7 is acceptable in Chinese adolescents.
This study has some strengths. To the authors’ knowledge, the current study is the first to investigate the psychometrics of the GAD-7 in an exclusively Chinese adolescent sample with a large sample size (n > 60,000). Further, we examined the reliability and validity of the GAD-7 in adolescents in sex- and age-specific subgroups, which provided robust evidence on the psychometric performance of applying GAD-7 in adolescents. This strength can help demonstrate the GAD-7 is a feasible instrument across different sexes and ages in young people.
However, a key limitation of the current study was that our study lacked diagnosis-specific criterion measures to assess the criterion validity of the GAD-7 since diagnostic interviews were not conducted in this study, and we only assessed the criterion validity by combining the PHQ-9. We noted that one study published in 2017 found that the specificity and sensitivity for detecting clinically significant anxiety symptoms were acceptable in adolescents with generalized anxiety disorder in Cincinnati [
45]. However, the study used a small sample size and all patients were evaluated at a single site, thus potentially limiting generalizability. Although clinical utility of the GAD-7 has been verified in adults [
12,
18,
23], more validation studies conducted in clinical adolescents are needed. Additionally, due to the lack of a diagnostic criterion, we failed to investigate the suitable cutoff of the GAD-7 in our sex- and age-specific groups. Therefore, further studies to include diagnosis-specific criterion measures and to determine the optimal cutoff point of the GAD-7 in adolescents are still warranted. Additionally, our study was based on the study samples from Shenzhen city, a southern city in mainland China. For this line, our research findings may not be generalizable to other adolescents from different countries or cultures.




{kind=link}