
Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lipski, M.; Tomaszewska, I.M.; Lipska, W.; Lis, G.J.; Tomaszewski, K.A. The mandible and its foramen: Anatomy, anthropology, embryology and resulting clinical implications. Folia Morphol. 2013, 72, 285–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eramo, S.; De Carolis, C.; Pagano, S. Johann Baptist Spix and the “Lingula Mandibularis”. J. Hist. Dent. 2014, 62, 116–121. [Google Scholar]
- Hsu, K.J.; Tseng, Y.C.; Liang, S.W.; Hsiao, S.Y.; Chen, C.M. Dimension and Location of the Mandibular Lingula: Comparisons of Gender and Skeletal Patterns Using Cone-Beam Computed Tomography. Biomed Res. Int. 2020, 2020, 2571534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monnazzi, M.S.; Passeri, L.A.; Gabrielli, M.F.R.; Bolini, P.D.A.; De Carvalho, W.R.S.; Da Costa Machado, H. Anatomic study of the mandibular foramen, lingula and antilingula in dry mandibles, and its statistical relationship between the true lingula and the antilingula. Int. J. Oral Maxillofac. Surg. 2012, 41, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Kositbowornchai, S.; Siritapetawee, M.; Damrongrungruang, T.; Khongkankong, W.; Chatrchaiwiwatana, S.; Khamanarong, K.; Chanthaooplee, T. Shape of the lingula and its localization by panoramic radiograph versus dry mandibular measurement. Surg. Radiol. Anat. 2007, 29, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Sekerci, A.E.; Cantekin, K.; Aydinbelge, M. Cone beam computed tomographic analysis of the shape, height, and location of the mandibular lingula in a population of children. Biomed Res. Int. 2013, 2013, 825453. [Google Scholar] [CrossRef]
- Chen, H.S.; Chen, Y.S.; Lin, I.L.; Chen, C.F. Antilingula as a Surgical Reference Point for Vertical Ramus Osteotomy. Biomed. Res. Int. 2021, 2021, 5585297. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Bianchi, S.; Continenza, M.A.; Macchiarelli, G. Frequency and anatomical features of the mandibular lingual foramina: Systematic review and meta-analysis. Surg. Radiol. Anat. 2017, 39, 1349–1357. [Google Scholar] [CrossRef]
- Keetley, A.; Moles, D.R. A clinical audit into the success rate of inferior alveolar nerve block analgesia in general dental practice. Prim. Dent. Care 2001, 8, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.; Reader, A.; Drum, M.; Nusstein, J.; Beck, M. Comparison of the Anesthetic Efficacy of the Conventional Inferior Alveolar, Gow-Gates, and Vazirani-Akinosi Techniques. J. Endod. 2008, 34, 1306–1311. [Google Scholar] [CrossRef] [PubMed]
- Cvetko, E. Bilateral anomalous high position of the mandibular foramen: A case report. Surg. Radiol. Anat. 2014, 36, 613–616. [Google Scholar] [CrossRef]
- Blanton, P.L.; Jeske, A.H. Avoiding complications in local anesthesia induction: Anatomical considerations. J. Am. Dent. Assoc. 2003, 134, 888–893. [Google Scholar] [CrossRef] [Green Version]
- Soon-Seop, W.; Jung-Yeon, C.; Won-Hee, P.; Im-Hag, Y.; Young-Soo, L.; Kwang-Sup, S. A Study of mandibular anatomy for orthognathic suregery in Koreans. J. Korean Assoc. Oral Maxillofac. Surg. 2002, 28, 126–131. [Google Scholar]
- Alves, N.; Deana, N.F. Morphological study of the lingula in adult human mandibles of brazilians individuals and clinical implications. Biomed Res. Int. 2015, 2015, 873751. [Google Scholar] [CrossRef] [PubMed]
- Jansisyanont, P.; Apinhasmit, W.; Chompoopong, S. Shape, height, and location of the lingula for sagittal ramus osteotomy in thais. Clin. Anat. 2009, 22, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, N.H.; Unnikrishnan, S.; Ramachandra, J.A.; Arali, V. Evaluation of relative position of mandibular foramen in children as a reference for inferior alveolar nerve block using orthopantamograph. J. Clin. Diagnostic Res. 2017, 11, ZC71–ZC74. [Google Scholar] [CrossRef]
- Ezoddini Ardakani, F.; Bahrololoumi, Z.; Zangouie Booshehri, M.; Navab Azam, A.; Ayatollahi, F. The position of lingula as an index for inferior alveolar nerve block injection in 7-11-year-old children. J. Dent. Res. Dent. Clin. Dent. Prospects 2010, 4, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Loubele, M.; Guerrero, M.E.; Jacobs, R.; Suetens, P.; van Steenberghe, D. A comparison of jaw dimensional and quality assessments of bone characteristics with cone-beam CT, spiral tomography, and multi-slice spiral CT. Int. J. Oral Maxillofac. Implants 2007, 22, 446–454. [Google Scholar] [PubMed]
- Devlin, H.; Yuan, J. Object position and image magnification in dental panoramic radiography: A theoretical analysis. Dentomaxillofacial Radiol. 2013, 42, 29951683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupi, S.M.; Galinetto, P.; Cislaghi, M.; Rodriguez, Y.; Baena, A.; Scribante, A.; Rodriguez, Y.; Baena, R. Geometric distortion of panoramic reconstruction in third molar tilting assessments: A comprehensive evaluation. Dentomaxillofacial Radiol. 2018, 47, 20170467. [Google Scholar] [CrossRef]
- Rodriguez y Baena, R.; Beltrami, R.; Tagliabo, A.; Rizzo, S.; Lupi, S.M. Differences between panoramic and Cone Beam-CT in the surgical evaluation of lower third molars. J. Clin. Exp. Dent. 2017, 9, e259–e265. [Google Scholar] [CrossRef]
- Jun, S.H.; Kim, C.H.; Ahn, J.S.; Padwa, B.L.; Kwon, J.J. Anatomical differences in lower third molars visualized by 2D and 3D X-ray imaging: Clinical outcomes after extraction. Int. J. Oral Maxillofac. Surg. 2013, 42, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Jeon, T.-H.; Jun, S.-H.; Kwon, J.-J. Evaluation of mandibular lingula and foramen location using 3-dimensional mandible models reconstructed by cone-beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 30. [Google Scholar] [CrossRef] [Green Version]
- Akcay, H.; Kalabalık, F.; Tatar, B.; Ulu, M. Location of the mandibular lingula: Comparison of skeletal Class I and Class III patients in relation to ramus osteotomy using cone-beam computed tomography. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 504–508. [Google Scholar] [CrossRef]
- Ahn, B.S.; Oh, S.H.; Heo, C.K.; Kim, G.T.; Choi, Y.S.; Hwang, E.H. Cone-beam computed tomography of mandibular foramen and lingula for mandibular anesthesia. Imaging Sci. Dent. 2020, 50, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Senel, B.; Ozkan, A.; Altug, H.A. Morphological evaluation of the mandibular lingula using cone-beam computed tomography. Folia Morphol. 2015, 74, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Sekerci, A.E.; Sisman, Y. Cone-beam computed tomography analysis of the shape, height, and location of the mandibular lingula. Surg. Radiol. Anat. 2014, 36, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Aps, J.K.M.; Gazdeck, L.Y.; Nelson, T.; Slayton, R.L.; Scott, J.M. Assessment of the location of the mandibular lingula in pediatric patients using cone beam computed tomography images. J. Dent. Child. 2018, 85, 58–65. [Google Scholar]
- Moorrees, C.F.; Reed, R.B. Correlation among crown diameters of human teeth. Arch. Oral Biol. 1964, 9, 685–697. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautam, A.; Madan Sonal, G.; Madan, A.D.M. Failure of inferior alveolar nerve block: Exploring the alternatives. J. Am. Dent. Assoc. 2002, 133, 843–846. [Google Scholar]
- Yu, I.H.; Wong, Y.K. Evaluation of mandibular anatomy related to sagittal split ramus osteotomy using 3-dimensional computed tomography scan images. Int. J. Oral Maxillofac. Surg. 2008, 37, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Kanno, C.M.; De Oliveira, J.A.; Cannon, M.; Carvalho, A.A.F. The mandibular lingula’s position in children as a reference to inferior alveolar nerve block. J. Dent. Child. 2005, 72, 56–60. [Google Scholar]
- Tuli, A.; Choudhry, R.; Choudhry, S.; Raheja, S.; Agarwal, S. Variation in shape of the lingula in the adult human mandible. J. Anat. 2000, 197, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Sang-Wan, L.; Hwahae, J.; Youn-Kyoung, S.; Su-Kyung, J.; Shin-Young, K.; Manho, J.; Doo-Jin, P. A Morphometric Study on the Mandibular Foramen and the Lingula in Korean. Korean J. Phys. Anthropol. 2012, 25, 153–166. [Google Scholar]
- ArunKumar, G.; Chinagudi, M.; Patil, B.M.; Iqbal, S. The morphology and location of the Mandibular lingula in south Indian population using cone-beam computed tomography-a retro-sectional study. Int. J. Curr. Res. 2016, 8, 28466–28469. [Google Scholar]
- Jang, H.Y.; Han, S.J. Measurement of mandibular lingula location using cone-beam computed tomography and internal oblique ridge-guided inferior alveolar nerve block. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Sung, K.; Kim, J.; Lee, S.; Lee, Y.; Kim, J.; Byun, S.; Lee, J.; Lee, J.; Pang, K.; Kim, S.; et al. The study on the location of the mandibular lingula, the anatomical course of the mandibular canal, and the thickness of the buccal cortical bone in normal occlusion and skeletal Class III malocclusion patients. J. Dent. Implant. Res. 2013, 32, 25–32. [Google Scholar]
- Muto, T.; Shigeo, K.; Yamamoto, K.; Kawakami, J. Computed tomography morphology of the mandibular ramus in prognathism: Effect on the medial osteotomy of the sagittal split ramus osteotomy. J. Oral Maxillofac. Surg. 2003, 61, 89–93. [Google Scholar] [CrossRef]
- Müller, H.P.; Schaller, N.; Eger, T.; Heinecke, A. Thickness of masticatory mucosa. J. Clin. Periodontol. 2000, 27, 431–436. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
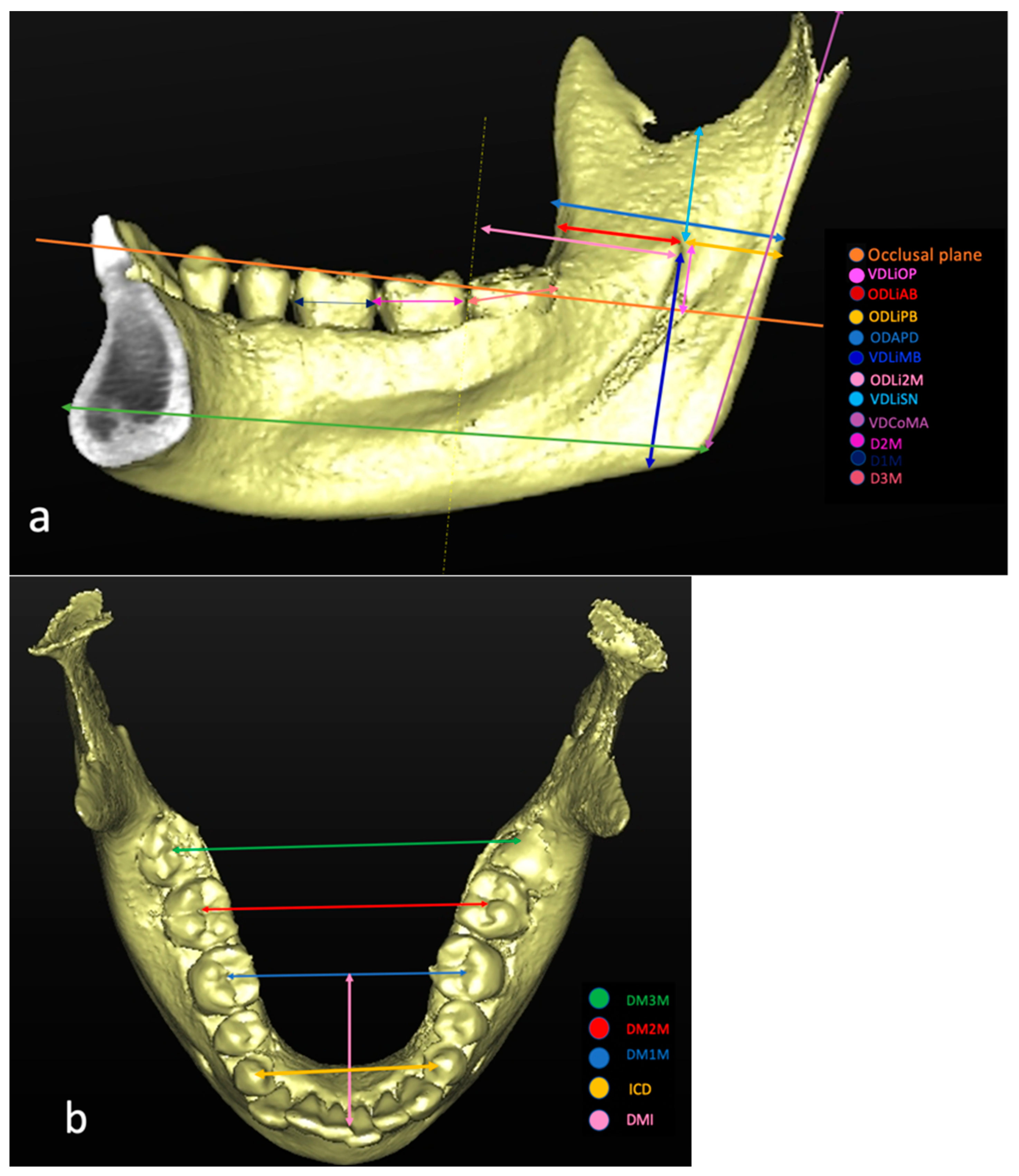
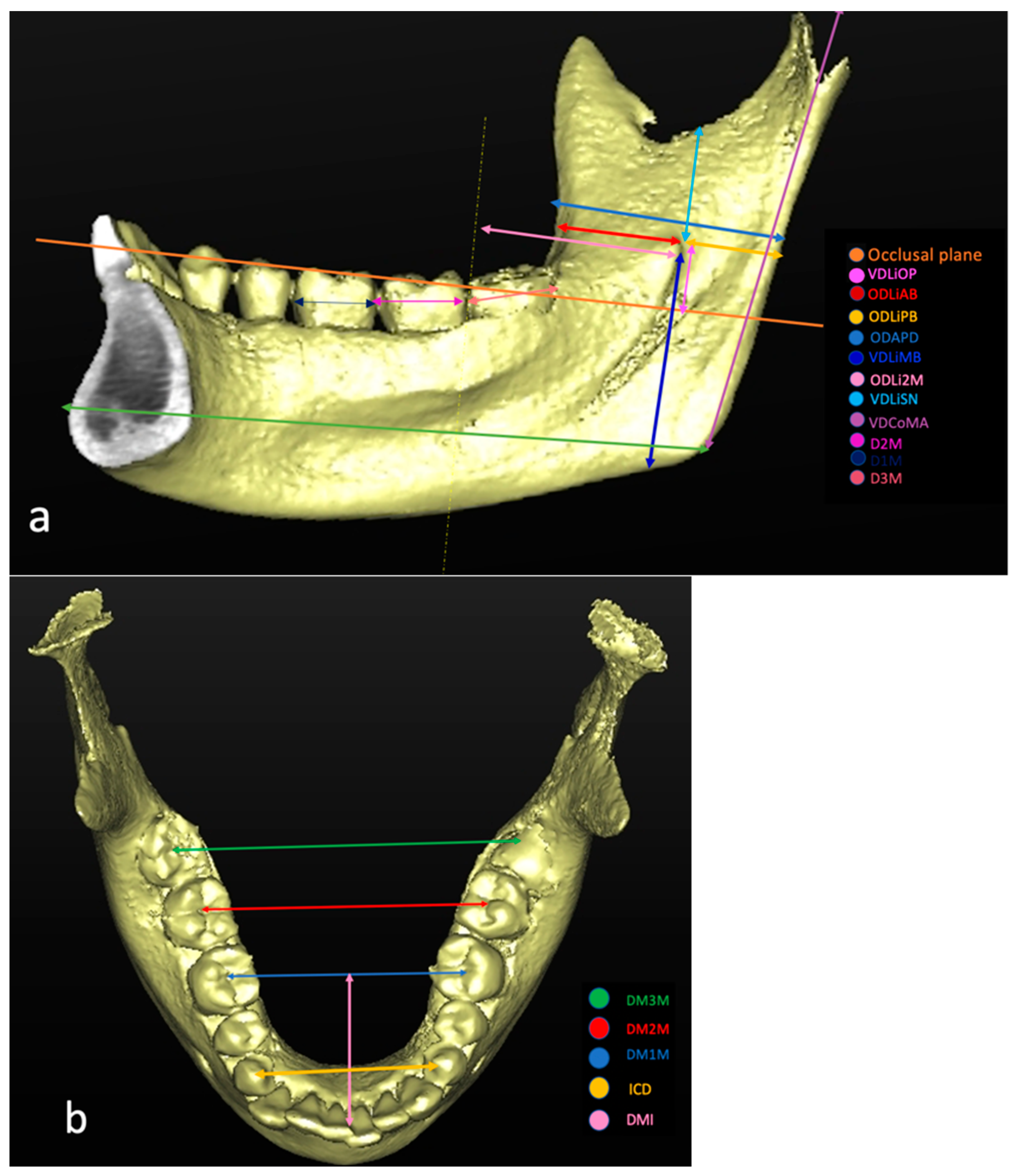
| Code | Definition | Description |
|---|---|---|
| VDLiOP | Distance of the Li from the OP | Measured on the coronal plane and perpendicular to the OP |
| ODLiAB | Distance of the Li from the anterior border of the mandible parallel to the OP | Measured on the axial plane passing through the ML and parallel to the OP |
| ODLiPB | Distance of the Li from the posterior border of the ramus | Measured on the axial plane passing through the ML and parallel to the OP |
| VDLiSN | Distance of the Li from the lower point of the sigmoid notch | Measured on the sagittal plane and perpendicular to the OP |
| VDLiMB | Distance of the Li from the mandibular base | Measured on the frontal plane passing through the Li and perpendicular to the OP |
| ODLi2M | Distance of the Li from the distal surface of the mandibular second molar tooth | Measured in the plane parallel to the OP passing through the Li, from the orthogonal projection of the most distal point of the crown to the Li |
| Code | Definition | Description |
|---|---|---|
| ODAPD | Anteroposterior diameter of the mandibular ramus | Measured on a plane passing at Li and parallel to the OP. |
| VDCoMA | Vertical distance between the condyle and mandibular angle | Measured on the sagittal plane as the distance from the highest point of the mandibular condyle to the gonion. |
| D1M | Mesial–distal diameter of the first mandibular molar | Measured on the sagittal plane as the largest dimension of the crown in the mesial distal direction, parallel to the occlusal surface of the tooth. |
| D2M | Mesial–distal diameter of the second mandibular molar | Measured on the sagittal plane as the largest dimension of the crown in the mesial distal direction, parallel to the occlusal surface of the tooth. |
| D3M | Mesial–distal diameter of the third mandibular molar | Measured on the sagittal plane as the largest dimension of the crown in the mesial distal direction, parallel to the occlusal surface of the tooth. |
| ICD | Intercanine distance | Measured on the frontal plane and parallel to the OP. |
| DM1M | Distance between the right first mandibular molars and the left ones | Measured on the frontal plane, using the central fossae of the molars as landmarks. |
| DM2M | Distance between the right second mandibular molars and the left ones | Measured on the frontal plane, using the central fossae of the molars as landmarks. |
| DM3M | Distance between the right third mandibular molars and the left ones | Measured on the frontal plane, using the central fossae of the molars as landmarks. |
| DMI | Anteroposterior distance between the intermolar line of the first molars and the midline | Measured on the axial plane as the space between the midline passing through the lower incisors and the intermolar line 36–46. |
| LMAN | The length of the mandibular body | Measured on the sagittal plane between the most-posterior point of the mandible and the pogonion. |
| Code | TOTAL (mm) | MALE (mm) | FEMALE (mm) | ICC |
|---|---|---|---|---|
| Age (years) | 34.93 ± 17.46 | 34.75 ± 18.68 | 35.07 ± 16.56 | |
| VDLiOP | 11.22 ± 4.27 | 11.77 ± 5.1 | 10.87 ± 3.61 | 0.99 (0.98–1.00) |
| ODLiAB | 16.96 ± 2.4 | 17.05 ± 2.7 | 16.9 ± 2.19 | 0.99 (0.97–1.00) |
| ODLiPB | 15.28 ± 2.1 | 16.04 ± 2.55 | 14.85 ± 1.65 | 0.98 (0.95–0.99) |
| ODAPD | 30.51 ± 3.12 | 31.16 ± 3.68 | 30.13 ± 2.69 | 0.99 (0.98–1.00) |
| VDLiMB | 31.2 ± 4.35 | 33.06 ± 4.4 | 30.05 ± 3.91 | 0.99 (0.98–1.00) |
| ODLi2M | 29.22 ± 3.98 | 30.59 ± 4.01 | 28.29 ± 3.71 | 0.99 (0.99–1.00) |
| VDLiSN | 13.87 ± 3.69 | 15.01 ± 3.76 | 13.34 ± 3.56 | 1 (1.00–1) |
| VDCoMA | 55.22 ± 6.58 | 61.58 ± 5.32 | 53.1 ± 5.63 | 0.99 (0.98–1.00) |
| D1M | 10.99 ± 0.7 | 11.13 ± 0.72 | 10.89 ± 0.68 | 1.00 (0.99–1.00) |
| D2M | 10.71 ± 0.9 | 10.85 ± 0.98 | 10.61 ± 0.85 | 0.88 (0.71–0.96) |
| D3M | 10.54 ± 1.04 | 10.54 ± 1.05 | 10.54 ± 1.05 | 0.98 (0.95–0.99) |
| ICD | 27.04 ± 3.16 | 28.02 ± 3.44 | 26.46 ± 2.84 | 0.80 (0.51–0.93) |
| DM1M | 42.18 ± 3.66 | 43.79 ± 3.22 | 41.02 ± 3.54 | 1.00 (0.99–1) |
| DM2M | 48.09 ± 3.42 | 49.59 ± 3.18 | 47.01 ± 3.2 | 0.94 0.87–0.98) |
| DM3M | 54.82 ± 4.95 | 54.98 ± 5.6 | 54.66 ± 4.46 | 0.98 (0.95–0.99) |
| DMLM | 27.97 ± 2.9 | 28.34 ± 3.34 | 27.67 ± 2.52 | 0.86 (0.66–0.95) |
| LMAN | 94.03 ± 5.74 | 97.28 ± 5.45 | 92.07 ± 5 | 0.99 (0.99–1.00) |
| Authors | Country | Study Design | Distance (mm) | |||||
|---|---|---|---|---|---|---|---|---|
| ODLiAB | ODLiPB | VDLiMB | VDLiSN | ODLi2M | ODAPD | |||
| Present study (2021) | Italy | CBCT | 16.96 ± 2.4 | 15.28 ± 2.1 | 31.2 ± 4.35 | 13.87 ± 3.69 | 29.22 ± 3.98 | 30.51 ± 3.12 |
| Sekerci et al. [6] (2013) | Turkey | CBCT | 13.3 ± 2.3 | 10.2 ± 1.6 | 23.1 ± 3.2 | 11.4 ± 2.5 | 24.7 ± 3.7 | |
| Sekerci and Sisman (2013) [27] | Turkey | CBCT | 16.77 ± 2.74 | 13.02 ± 2.31 | 26.05 ± 3.84 | 23.09 ± 3.67 | 29.45 ± 3.92 | |
| Senel et al. [26] (2015) | Turkey | CBCT | 18.5 ± 2.3 | 16.9 ± 3.5 | 38.3 ± 5.3 | 18.1 ± 3.6 | ||
| ArunKumar et al. [36] (2016) | South India | CBCT | 14.05 ± 6.68 | 12.91 ± 3.73 | 14.10 ± 4.74 | 11.4 ± 2.5 | 16.21 ± 4.85 | |
| Zhou et al. [23] (2017) | Korea | CBCT | 18.3 ± 2.3 | 17.6 ± 1.8 | 32.9 ± 3.05 | 15.6 ± 2.5 | 29.5 ± 3.05 | 33.05 ± 2.4 |
| Aps et al. [28] (2018) | America | CBCT | 18.12 ± 2.17 | 14.97 ± 1.86 | 27.38 ± 4.30 | 15.51 ± 2.36 | ||
| Akcay et al. [24] (2019) | Turkey | CBCT | 11.6 ± 1.67 | 16.2 ± 1.76 | 18.2 ± 2.8 | |||
| Jang et al. [37] (2019) | Korea | CBCT | 14.68 ± 1.44 | |||||
| Kun-Jung et al. [3] (2020) | Taiwan | CBCT | 19.21 ± 3.02 | 15.22 ± 2.02 | 31.20 ± 3.81 | 20.04 ± 3.16 | ||
| Soon-Seop et al. [13] (2002) | Korea | Dry Mandible | 16.13 ± 3.53 | 19.82 ± 5.11 | ||||
| Kositbowornchai et al. [5] (2007) | Thailand | OPT | 23.24 ± 3.82 | 17.83 ± 3.30 | ||||
| Kositbowornchai et al. [5] (2007) | Thailand | Dry Mandible | 20.7 ± 2.27 | 15.40 ± 1.90 | ||||
| Jansisyanont et al. [15] (2009) | Thailand | Dry Mandible | 20.6 ± 3.5 | 18.0 ± 2.6 | 16.6 ± 2.9 | 29.7 ± 4.4 | ||
| Monnazzi et al. [4] (2011) | Brazil | Dry Mandible | 16.5 ± 2.32 | 14.63 ± 2.13 | 27.09 ± 5.44 | 16.38 ± 2.59 | ||
| Alves et al. [14] (2015) | Brazil | Dry Mandible | 17.76 ± 2.69 | 15.28 ± 2.31 | 33.30 ± 4.14 | 17.29 ± 2.57 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupi, S.M.; Landini, J.; Olivieri, G.; Todaro, C.; Scribante, A.; Rodriguez y Baena, R. Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare 2021, 9, 1747. https://doi.org/10.3390/healthcare9121747
Lupi SM, Landini J, Olivieri G, Todaro C, Scribante A, Rodriguez y Baena R. Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare. 2021; 9(12):1747. https://doi.org/10.3390/healthcare9121747
Chicago/Turabian StyleLupi, Saturnino Marco, Jessica Landini, Giorgia Olivieri, Claudia Todaro, Andrea Scribante, and Ruggero Rodriguez y Baena. 2021. "Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT" Healthcare 9, no. 12: 1747. https://doi.org/10.3390/healthcare9121747
APA StyleLupi, S. M., Landini, J., Olivieri, G., Todaro, C., Scribante, A., & Rodriguez y Baena, R. (2021). Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare, 9(12), 1747. https://doi.org/10.3390/healthcare9121747