Access to Information and Degree of Community Awareness of Preventive Health Measures in the Face of COVID-19 in Spain


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Item: “Under what circumstances do you think it is necessary to use a mask?”. Answer: “I do not think it is necessary as it does not fully protect”.
- Item: “Indicate what you usually wash your hands with”. Answer: “Only with water”.
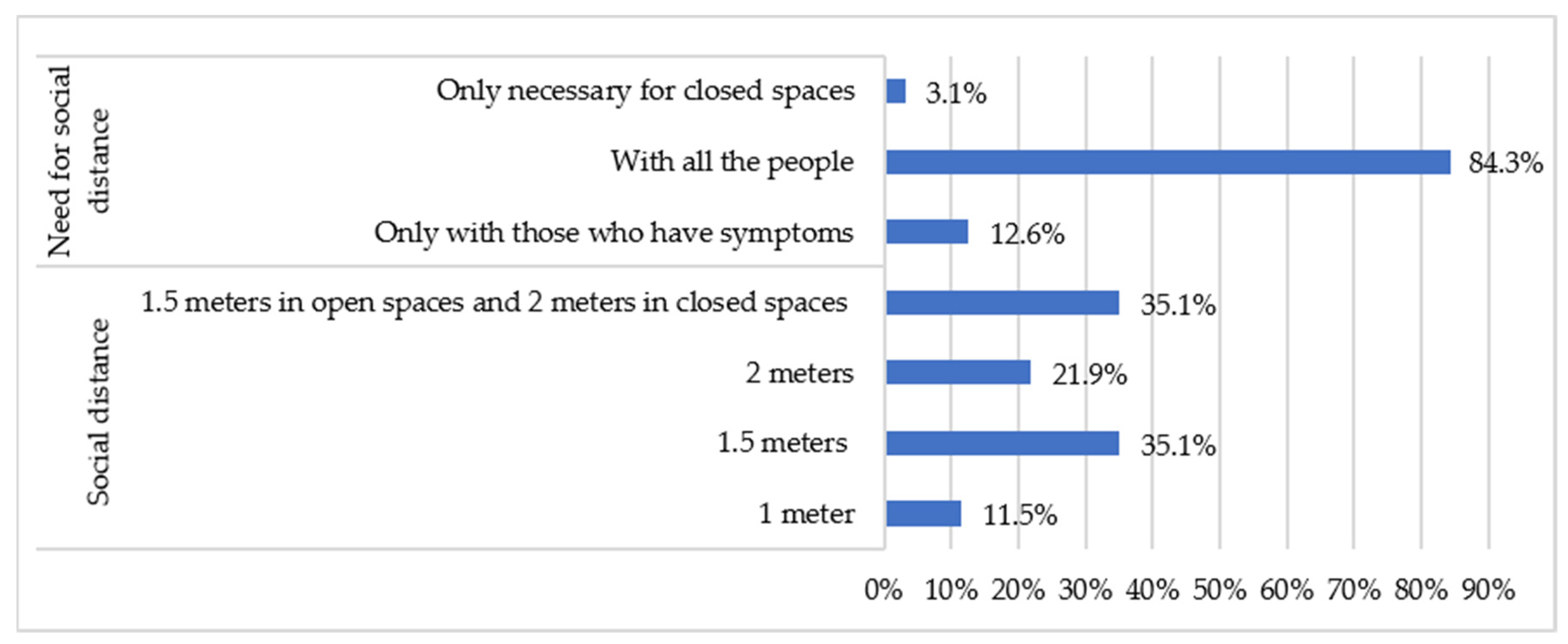
- Item: “When I go out, to work, to a shop or a place of leisure, etc., if I don’t wear a mask and there is no protective element (for example, a screen)”. Answers: I should keep physical distance only with those people who have symptoms/If I am in an outdoor space, the measure of physical distance is not necessary, it is only for closed spaces.
2.2. Data Collection Instruments
2.3. Procedure
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.W.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H.; et al. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef]
- Mondelli, M.U.; Colaneri, M.; Seminari, E.M.; Baldanti, F.; Bruno, R. Low risk of SARS-CoV-2 transmission by fomites in real-life conditions. Lancet Infect. Dis. 2020, 3099, 30678. [Google Scholar] [CrossRef]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef] [PubMed]
- Somsen, G.A.; Van Rijn, C.; Kooij, S.; Bem, R.A.; Bonn, D. Small droplet aerosols in poorly ventilated spaces and SARS-CoV-2 transmission. Lancet Respir. Med. 2020, 8, 658–659. [Google Scholar] [CrossRef]
- World Health Organization. Preguntas y Respuestas Sobre la Enfermedad por Coronavirus (COVID-19). 2020. Available online: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019/advice-for-public/q-a-coronaviruses (accessed on 12 April 2020).
- Ministerio de la Presidencia, Relaciones con las Cortes y Memoria Democrática. Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Boletín Oficial del Estado (BOE). 2020; pp. 25390–25400. Available online: https://www.boe.es/eli/es/rd/2020/03/14/463 (accessed on 9 September 2020).
- Ministerio de Sanidad, Consumo y Bienestar Social. Orden SND/422/2020, de 19 de Mayo, por la Que se Regulan las Condiciones Para el uso Obligatorio de Mascarilla Durante la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Boletín Oficial del Estado (BOE). 2020; pp. 33600–33602. Available online: https://www.boe.es/eli/es/o/2020/05/19/snd422 (accessed on 9 September 2020).
- Lau, J.T.F.; Tsui, H.; Lau, M.; Yang, X. SARS Transmission, Risk Factors, and Prevention in Hong Kong. Emerg. Infect. Dis. 2020, 10, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Low, J.G.H. Risk of respiratory infections in health care workers: Lessons on infection control emerge from the SARS outbreak. Southeast Asian J. Trop. Med. Public Health 2005, 36, 481–488. [Google Scholar] [PubMed]
- Davies, A.; Thompson, K.A.; Giri, K.; Kafatos, G.; Walker, J.; Bennett, A. Testing the efficacy of homemade masks: Would they protect in an influenza pandemic? Disaster Med. Public Health Prep. 2013, 7, 413–418. [Google Scholar] [CrossRef]
- Eikenberry, S.E.; Mancuso, M.; Iboi, E.; Phan, T.; Eikenberry, K.; Kuang, Y.; Kostelich, E.; Gumel, A.B. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infect. Dis. Model. 2020, 5, 293–308. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Consumo y Bienestar Social. Qué Debes Tener en Cuenta al Comprar una Mascarilla? 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/030520_GUIA_COMPRA_MASCARILLAS.pdf (accessed on 12 April 2020).
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Consumo y Bienestar Social. Uso Correcto de Mascarillas. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_uso_correcto_mascarillas.pdf (accessed on 12 April 2020).
- World Health Organization. Infection Prevention and Control. 2020. Available online: https://www.who.int/teams/integrated-health-services/infection-prevention-control (accessed on 12 April 2020).
- World Helath Organization. Material y Documentos Sobre la Higiene de Manos. 2020. Available online: https://www.who.int/gpsc/5may/tools/es/ (accessed on 9 September 2020).
- Ministerio de Sanidad, Consumo y Bienestar Social. Información Para la Ciudadanía. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/ciudadania.htm (accessed on 9 September 2020).
- Al-Hasan, A.; Yim, D.; Khuntia, J. Citizens’ Adherence to COVID-19 Mitigation Recommendations by the Government: A 3-Country Comparative Evaluation Using Web-Based Cross-Sectional Survey Data. J. Med. Internet Res. 2020, 22, e20634. Available online: https://www.jmir.org/2020/8/e20634/ (accessed on 1 January 2021). [CrossRef]
- Kwok, K.O.; Li, K.K.; Chan, H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, S.Y. Community Responses during Early Phase of COVID-19 Epidemic, Hong Kong. Emerg. Infect. Dis. 2020, 26, 1575–1579. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Mwamba, G.N.; Miema, J.M.; Umba, E.K.; Kangulu, I.B.; Ndala, D.B.; Mukendi, P.C.; Mutombo, D.K.; Kabasu, M.C.; Katala, M.K.; et al. Predictors of non-adherence to public health instructions during the covid-19 pandemic in the Democratic Republic of the Congo. J. Multidiscip. Healthc. 2020, 13, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.J.; Mesch, G.S. The adoption of preventive behaviors during the COVID-19 pandemic in China and Israel. Int. J. Environ. Res. Public Health 2020, 17, 7170. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Sarkar, T.; Khan, S.H.; Kamal, A.H.; Hasan, S.M.; Kabir, A.; Yeasmin, D.; Islam, M.A.; Chowdhury, K.I.; Anwar, K.S.; et al. COVID-19-Related infodemic and its impact on public health: A global social media analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Barari, S.; Caria, S.; Davola, A.; Falco, P.; Fetzer, T.; Fiorin, S.; Hensel, L.; Ivchenko, A.; Jachimowicz, J.; King, G.; et al. Evaluating COVID-19 Public Health Messaging in Italy: Self-Reported Compliance and Growing Mental Health Concerns. medRxiv 2020, 1–19. [Google Scholar] [CrossRef]
- Wang, J.; Pan, L.; Tang, S.; Ji, J.S.; Shi, X. Mask use during COVID-19: A risk adjusted strategy. Environ. Pollut. 2020, 266, 115099. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.; Wong, S.C.; Chuang, V.W.; So, S.Y.; Chen, J.H.; Sridhar, S.; To, K.K.; Chan, J.F.; Hung, I.F.; Ho, P.L.; et al. The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J. Infect. 2020, 81, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Dana, T.; Jungbauer, R.; Weeks, C.; McDonagh, M.S. Masks for prevention of respiratory virus infections, including SARS-CoV-2, in health care and community settings: A living rapid review. Ann. Intern. Med. 2020, 173, 542–555. [Google Scholar] [CrossRef]
- Bundgaard, H.; Bundgaard, J.S.; Raaschou-Pedersen, D.E.; von Buchwald, C.; Todsen, T.; Norsk, J.B.; Pries-Heje, M.M.; Vissing, C.R.; Nielsen, P.B.; Winsløw, U.C.; et al. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS-CoV-2 infection in Danish mask wearers: A randomized controlled trial. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Conselleria de Sanidad de la Xunta de Galicia. Resolución de 25 de junio de 2020, por el que se Introducen Determinadas Modificaciones en las Medidas de Prevención Previstas en el Acuerdo de 12 de junio de 2020, Sobre Medidas de Prevención Necesarias para Hacer Frente a la Crisis sanitaria Ocasionada. Diario Oficial de Galicia (DOG). 2020, pp. 25480–25493. Available online: https://www.xunta.gal/dog/Publicados/2020/20200627/AnuncioC3K1-250620-1_es.pdf (accessed on 12 April 2020).
- Consejería de Sanidad. Orden 1008/2020, de 18 de agosto, de la Consejería de Sanidad, por la que se Modifica la Orden 668/2020, de 19 de Junio de 2020, por la que se Establecen Medidas Preventivas Para Hacer frente A la Crisis Sanitaria Ocasionada por el COVID-19. Boletín Oficial de la Comunidad Madrid (BOCM). 2020, pp. 11–17. Available online: https://www.bocm.es/boletin/CM_Orden_BOCM/2020/08/19/BOCM-20200819-1.PDF (accessed on 12 April 2020).
- Nakamura, I.; Fujita, H.; Tsukimori, A.; Kobayashi, T.; Sato, A.; Fukushima, S.; Amano, K.; Abe, Y. Scenario-based simulation health care education for performance of hand hygiene. Am. J. Infect. Control 2019, 47, 144–148. [Google Scholar] [CrossRef]
- Shao, S.; Zhou, D.; He, R.; Li, J.; Zou, S.; Mallery, K.; Kumar, S.; Yang, S.; Hong, J. Risk assessment of airborne transmission of COVID-19 by asymptomatic individuals under different practical settings. J. Aerosol Sci. 2021, 151, 105661. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.; Liu, H.; Li, X.D.; Liu, H.R. Factors affecting infection control behaviors to prevent COVID-19: An online survey of nursing students in Anhui, China in March and April 2020. Med. Sci. Monit. 2020, 26, e925877-1. [Google Scholar] [CrossRef] [PubMed]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Moore, J.L.; Steege, L.M.; Koopman, R.J.; Belden, J.L.; Canfield, S.M.; Meadows, S.E.; Elliott, S.G.; Kim, M.S. Health information needs, sources, and barriers of primary care patients to achieve patient-centered care: A literature review. Health Inform. J. 2016, 22, 992–1016. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Block II. Access to Information on Preventive Measures | ||
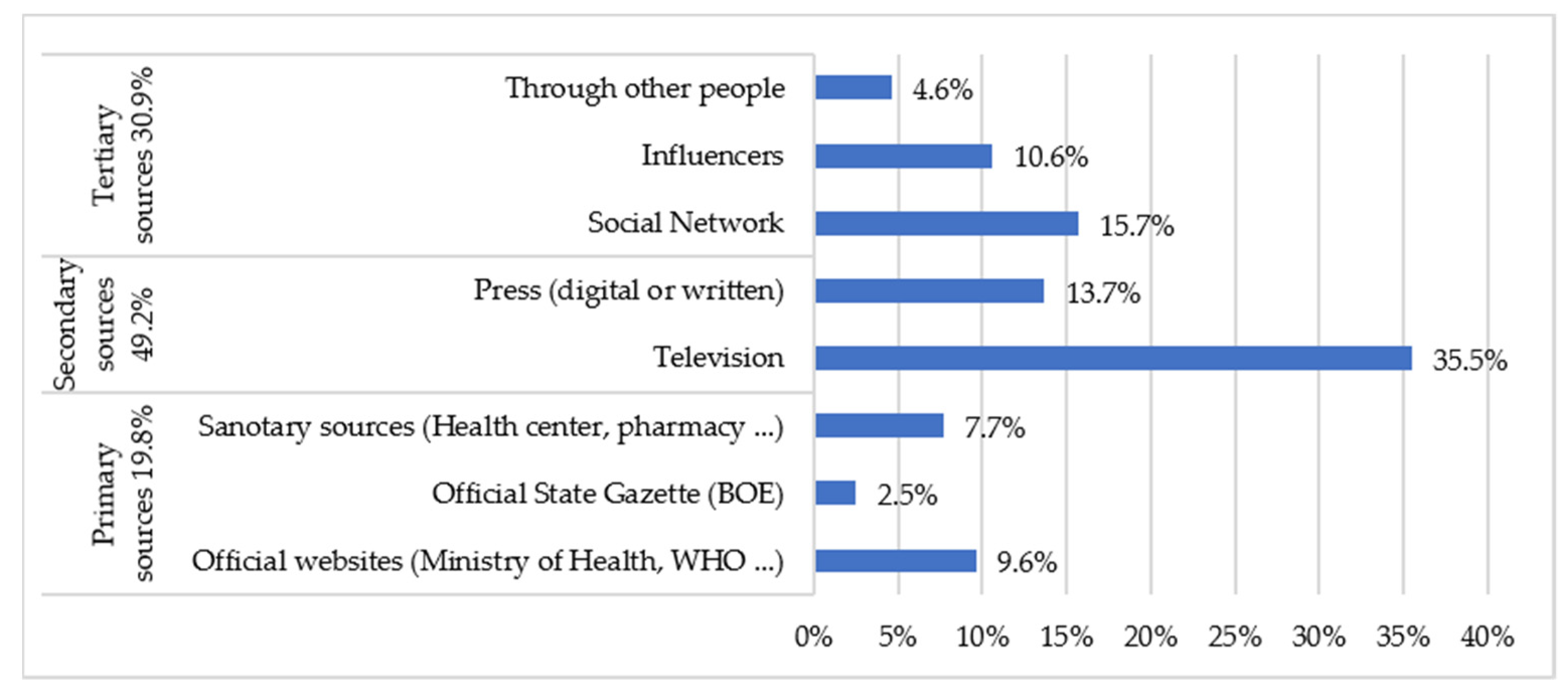
| By what means of communication have you received more information about the preventive measures established in the new normality (use of masks, hygiene measures, physical distance, etc.)? | Television press (digital or written). Social networks. Influencers. Through other people. Official websites (Ministry of Health, WHO, etc.). B.O.E. Sanitary (health center, pharmacy, etc.). | |
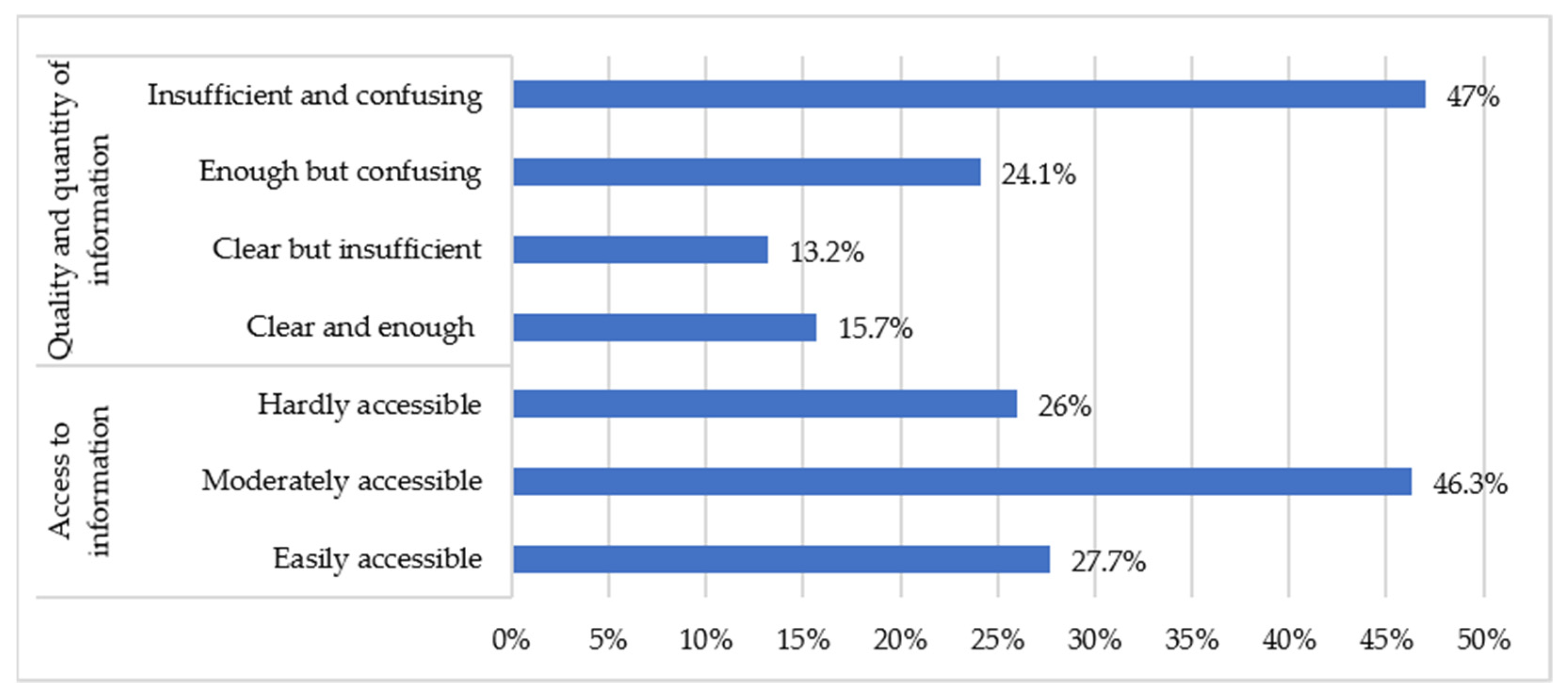
| How do you consider the information provided by the competent bodies in the field of health (Ministry of Health, Ministry of Health and Consumer Affairs, World Health Organization) on the preventive measures established in the new normality? | Clear and sufficient. Clear but insufficient. Sufficient but confusing. Insufficient and confusing. | |
| It considers that the information provided by the competent bodies in the field of health (Department of Health, Ministry of Health, World Health Organization) on preventive measures is: | Easily accessible. Moderately accessible. Difficult to access. | |
| Block III. Degree of Knowledge/Adoption of Preventive Measures | ||
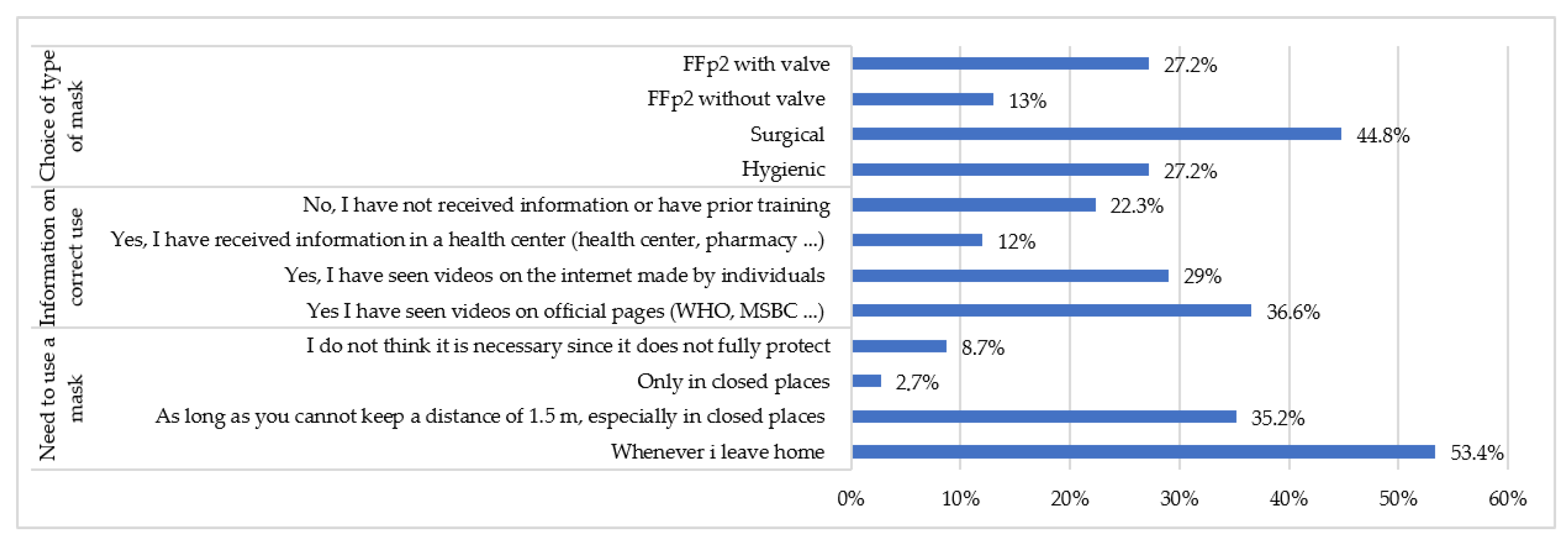
| Use of Masks | In what circumstances do you think it is necessary to use a mask? | Whenever you leave the house. Whenever you can’t keep a distance of 1.5 m, especially indoors. Only in closed places. I do not think it is necessary since it does not fully protect. |
| Have you been informed about the correct way to put on and take off your mask? | Yes, I have seen videos on the websites of official organizations (Department of Health, Ministry of Health, WHO, etc.). Yes, I have seen videos on the internet made by individuals. Yes, I have received information at a health center: hospital, primary care center, pharmacy. No, I have not received any information about it and I do not have any previous training. | |
| Which mask do you think a person without risk factors should wear to the supermarket? | Hygienic. Surgical. FFp2 with valve. FFp2 without valve. | |
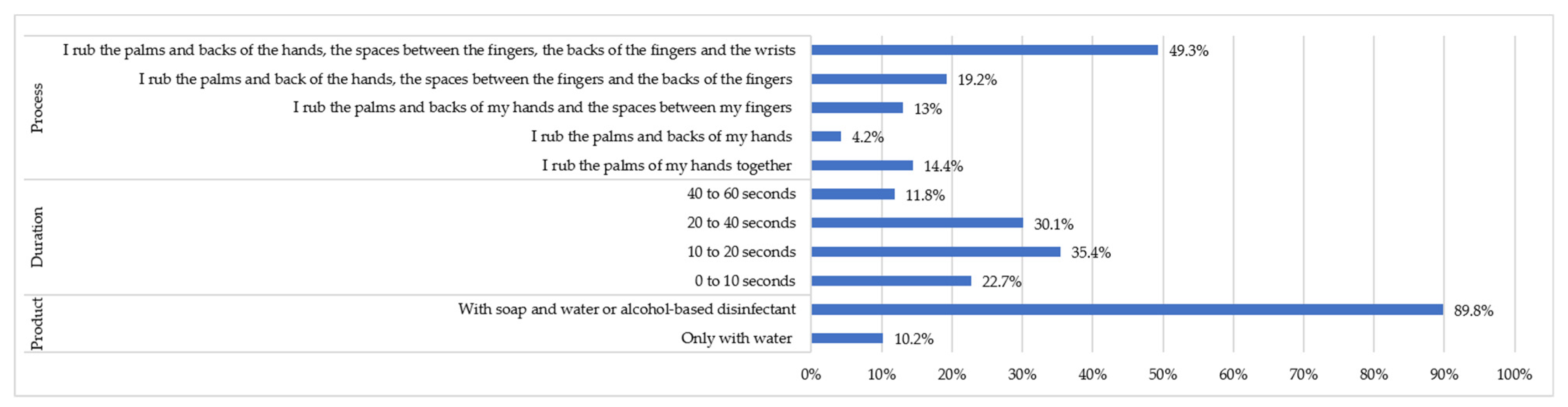
| Hand Washing | Indicate what you usually wash your hands with: | With water only. With soap and water or alcohol-based disinfectant. |
| How much time do you spend washing your hands? | From 0 to 10 s. From 10 to 20 s. From 20 to 40 s. From 40 to 60 s. | |
| Please indicate which of the following procedures best suits your regular hand washing: | I rub my palms together. I rub my palms and the backs of my hands. I rub the palms and backs of my hands and the spaces between my fingers. I rub the palms and backs of the hands, the spaces between the fingers and the backs of the fingers. I rub the palms and backs of the hands, the spaces between the fingers, the backs of the fingers and the wrists. | |
| Physical Distancing | The physical distance in the “new normal” to prevent the spread of COVID-19 is: | 1 m. 1.5 m. 2 m. 1.5 m in open spaces and 2 m in closed spaces. |
| When I go out, to work, to a shop or a place of leisure, etc., if I don’t wear a mask and there isn’t some kind of protective element (for example, a screen): | I should keep physical distance only from those people who have symptoms. I have to keep my physical distance from everyone. If I am in an open space, the measure of physical distance is not necessary, it is only for closed spaces. | |
| Socio-Demographics Variables | N (%) | |
|---|---|---|
| Sex | Men | 556 (30.7%) |
| Women | 1.255 (69.3%) | |
| Age | Young adults (18–35) | 489 (27%) |
| Mature adults (36–59) | 652 (36%) | |
| Seniors (≥60) | 670 (37%) | |
| Residence | Rural | 1.340 (74%) |
| Urban | 471 (26%) | |
| Educational level | None | 51 (2.8%) |
| Primary | 203 (11.2%) | |
| Secondary | 594 (32.8%) | |
| University | 963 (53.2%) | |
| Person or cohabiting person of risk | No | 770 (42.50%) |
| Yes | 1.041 (57.50%) | |
| Autonomous Region | Andalucía | 55 (3%) |
| Aragón | 76 (4.2%) | |
| Asturias | 53 (2.9%) | |
| Canarias | 83 (4.6%) | |
| Cantabria | 26 (1.4%) | |
| Castilla y León | 681 (37.6%) | |
| Castilla la Mancha | 47 (2.6%) | |
| Cataluña | 73 (4%) | |
| Extremadura | 60 (3.3%) | |
| Galicia | 60 (3.3%) | |
| Islas Baleares | 60 (3.3%) | |
| La Rioja | 56 (3.1%) | |
| Madrid | 282 (15.6%) | |
| Murcia | 54 (3%) | |
| Navarra | 45 (2.5%) | |
| The Basque Country | 64 (3.5%) | |
| Valencia | 36 (2%) | |
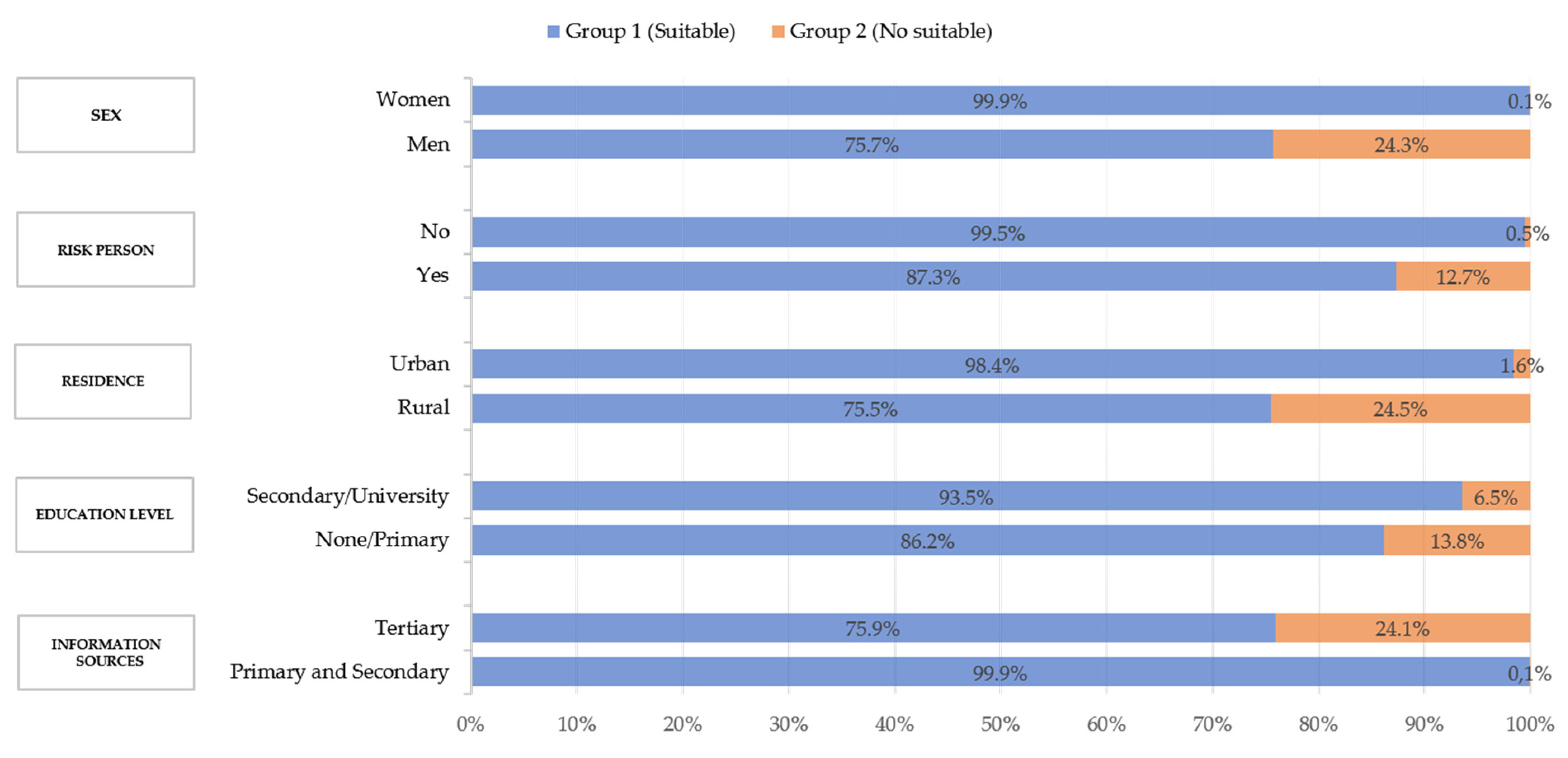
| Socio-Demographic Variables | Chi-Square 1 |
|---|---|
| Sex | 255.5 |
| Person or cohabiting person of risk | 304.1 |
| Residence | 310.5 |
| Educational level | 271.1 |
| Information sources | 290.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Velasco, L.; Liébana-Presa, C.; Abella-Santos, E.; Villar-Suárez, V.; Fernández-Gutiérrez, R.; Fernández-Martínez, E. Access to Information and Degree of Community Awareness of Preventive Health Measures in the Face of COVID-19 in Spain. Healthcare 2021, 9, 104. https://doi.org/10.3390/healthcare9020104
Gutiérrez-Velasco L, Liébana-Presa C, Abella-Santos E, Villar-Suárez V, Fernández-Gutiérrez R, Fernández-Martínez E. Access to Information and Degree of Community Awareness of Preventive Health Measures in the Face of COVID-19 in Spain. Healthcare. 2021; 9(2):104. https://doi.org/10.3390/healthcare9020104
Chicago/Turabian StyleGutiérrez-Velasco, Laura, Cristina Liébana-Presa, Elena Abella-Santos, Vega Villar-Suárez, Rocío Fernández-Gutiérrez, and Elena Fernández-Martínez. 2021. "Access to Information and Degree of Community Awareness of Preventive Health Measures in the Face of COVID-19 in Spain" Healthcare 9, no. 2: 104. https://doi.org/10.3390/healthcare9020104
APA StyleGutiérrez-Velasco, L., Liébana-Presa, C., Abella-Santos, E., Villar-Suárez, V., Fernández-Gutiérrez, R., & Fernández-Martínez, E. (2021). Access to Information and Degree of Community Awareness of Preventive Health Measures in the Face of COVID-19 in Spain. Healthcare, 9(2), 104. https://doi.org/10.3390/healthcare9020104