Association between Anticholinergic Burden and Constipation: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Search
2.3. Study Eligibility Criteria
2.3.1. Studies Inclusion Criteria
2.3.2. Exclusion Criteria
- The full text was not available.
- Constipation as a composite variable.
- Narrative reviews, letters to the editor, and conference summaries.
- Articles that measured only acute constipation.
- The association magnitude was not disclosed.
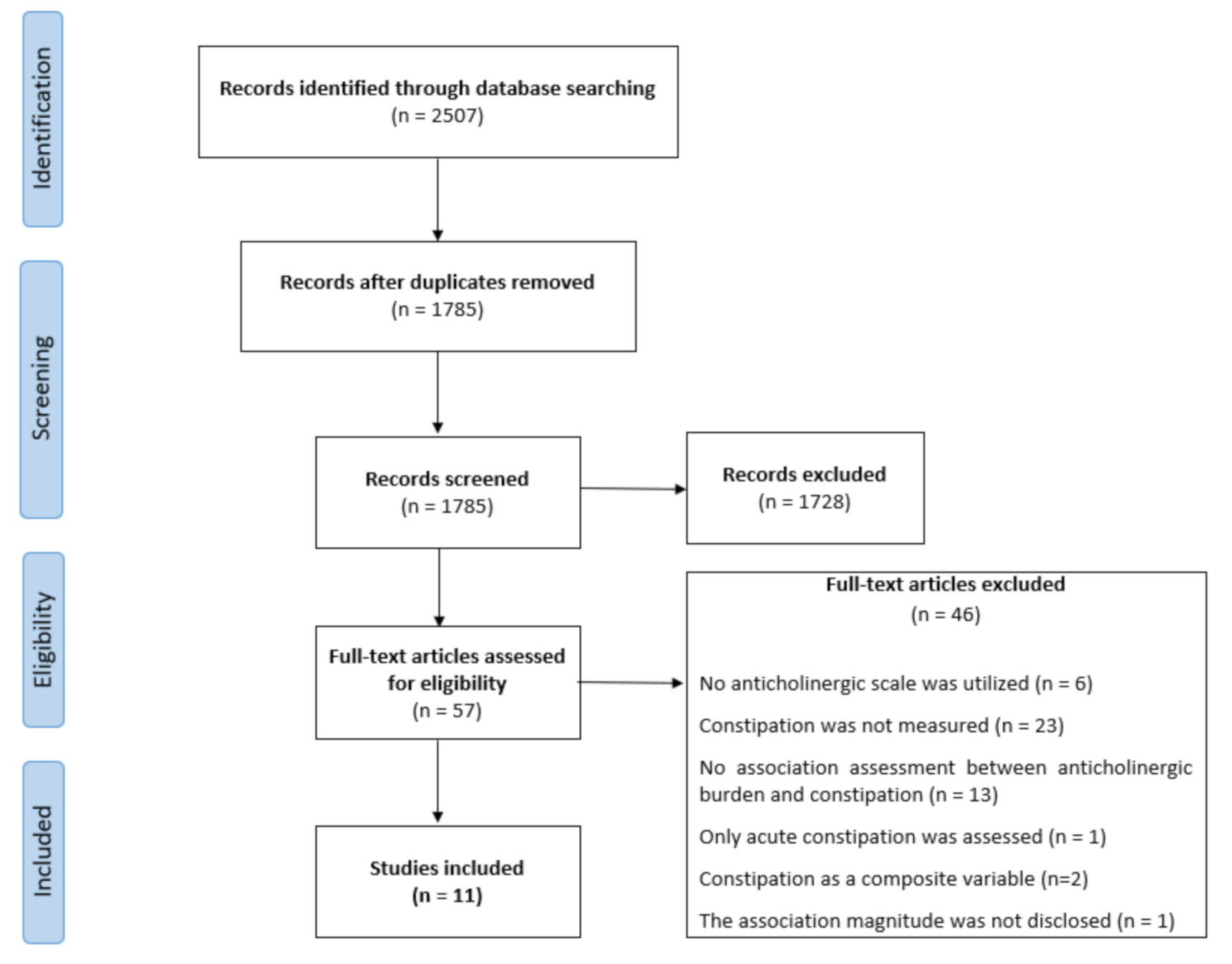
2.4. Study Selection
2.5. Assessment of Articles Quality
2.6. Data Collection
- Study characteristics: Study design (Interventional, observational, cross-sectional studies), country, the number of patients included, study duration.
- Patient characteristics: the setting of the population included (hospital, home-dwelling patients, nursing facilities inmates, community group homes, or patients from health insurance databases), average age or age limits for inclusion on each study, sex.
- Variables related to constipation: constipation diagnostic methods, number and percentage of patients diagnosed with constipation, patient’s physical activity, patient´s fluid and fiber intakes, polypharmacy rates, opioids use prevalence and patient´s diagnoses that may contribute to constipation: obstructive digestive diseases, mechanical causes of constipation, neurologic disorders such as Parkinson’s disease and multiple sclerosis, myogenic disorders, and enteric neuropathies.
- Anticholinergic activity data: number and percentage of patients treated with anticholinergic drugs and the anticholinergic scale used.
- Data about the association between constipation and anticholinergic burden: positive (significant data) or negative association (non-significant data) according to association measure (OR, p-value, RR, Hazard ratio, etc.), anticholinergic drugs that most frequently were associated with constipation.
3. Results
3.1. General Characteristics of the Included Studies
3.2. Constipation Prevalence and Anticholinergic Exposure
3.3. Alternative Causes of Constipation
3.4. Methods for Measuring Anticholinergic Burden
3.5. Association between Anticholinergic Burden and Constipation
3.6. Association Results by Anticholinergic Scale
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Fox, C.; Richardson, K.; Maidment, I.D.; Savva, G.M.; Matthews, F.E.; Smithard, D.; Brayne, C. Anticholinergic medication use and cognitive impairment in the older population: The medical research council cognitive function and ageing study. J. Am. Geriatr. Soc. 2011, 59, 1477–1483. [Google Scholar] [CrossRef]
- Tune, L.E. Anticholinergic effects of medication in elderly patients. J. Clin. Psychiatry 2001, 62 (Suppl. 21), 11–14. [Google Scholar]
- Ancelin, M.L.; Artero, S.; Portet, F.; Dupuy, A.M.; Touchon, J.; Ritchie, K. Non-degenerative mild cognitive impairment in elderly people and use of anticholinergic drugs: Longitudinal cohort study. BMJ 2006, 332, 455–459. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancelli, I.; Gigli, G.L.; Piani, A.; Zanchettin, B.; Janes, F.; Rinaldi, A.; Valente, M. Drugs with anticholinergic properties as a risk factor for cognitive impairment in elderly people: A population-based study. J. Clin. Psychopharmacol. 2008, 28, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Boustani, M.; Campbell, N.; Munger, S.; Maidment, I.; Fox, C. Impact of anticholinergics on the aging brain: A review and practical application. Aging Healt. 2008, 4, 311–320. [Google Scholar] [CrossRef]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Culp, K.R. The Anticholinergic Drug Scale as a measure of drug-related anticholinergic burden: Associations with serum anticholinergic activity. J. Clin. Pharm. 2006, 46, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Hilmer, S.N.; Mager, D.E.; Simonsick, E.M.; Cao, Y.; Ling, S.M.; Windham, B.G.; Abernethy, D.R. A Drug Burden Index to define the functional burden of medications in older people. Arch. Intern. Med. 2007, 167, 781–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalba-Moreno, A.M.; Alfaro-Lara, E.R.; Rodríguez-Pérez, A.; Báñez-Toro, D.; Sánchez-Fidalgo, S.; Pérez-Guerrero, M.C.; Nieto-Martín, M.D. Association Between Drug Burden Index and Functional and Cognitive Function in Patients with Multimorbidity. Curr. Pharm. Des. 2018, 24, 3384–3391. [Google Scholar] [CrossRef]
- Huang, K.; Chan, F.; Shih, H.; Lee, C. Relationship between potentially inappropriate anticholinergic drugs (PIADs) and adverse outcomes among elderly patients in Taiwan. J. Food Drug Anal. 2012, 20, 930–937. [Google Scholar]
- Salahudeen, M.S.; Duffull, S.B.; Nishtala, P.S. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: A systematic review. BMC Geriatr. 2015, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Peterson, G.M.; Bereznicki, L.R.; Salahudeen, M.S. Association between anticholinergic drug burden and mortality in older people: A systematic review. Eur J. Clin. Pharm. 2020, 76, 319–335. [Google Scholar] [CrossRef]
- Lembo, A.; Camilleri, M. Constipation. N. Engl. J. Med. 2003, 349, 1360–1368. [Google Scholar] [CrossRef]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Cusack, S.; Day, M.R.; Wills, T.; Coffey, A. Older people and laxative use: Comparison between community and long-term care settings. Br. J. Nurs. 2012, 21, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez, M.I.; Bercik, P. Epidemiology and burden of constipation. Can. J. Gastroenterol. 2011, 25 (Suppl. B), 11B–15B. [Google Scholar] [CrossRef]
- Forootan, M.; Bagheri, N.; Darvishi, M. constipation: A review of literature. Medicine 2018, 97, e10631. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, O. Study of constipation in a geriatric hospital, day hospital, old people’s home and at home. Aging 1991, 3, 161–170. [Google Scholar] [PubMed]
- O’Keefe, E.A.; Talley, N.J.; Zinsmeister, A.R.; Jacobsen, S.J. Bowel disorders impair functional status and quality of life in the elderly: A population-based study. J. Gerontol. 1995, 50, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Belsey, J.; Greenfield, S.; Candy, D.; Geraints, M. Systematic review: Impact of constipation on quality of life in adults and children. Aliment. Pharm. 2010, 31, 938–949. [Google Scholar] [CrossRef] [Green Version]
- Hunt, R.H.; Dhaliwal, S.; Tougas, G.; Pedro, C.; Labbe, J.F.; Paul, H.; Ennamorato, M. Prevalence, impact and attitudes toward lower gastrointestinal dysmotility and sensory symptoms and their treatment in Canada: A descriptive study. Can. J. Gastroenterol. 2007, 21, 31–37. [Google Scholar] [CrossRef]
- Chang, J.Y.; Locke, G.R., III; McNally, M.A.; Halder, S.L.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J. Impact of functional gastrointestinal disorders on survival in the community. Am. J. Gastroenterol. 2010, 105, 822–823. [Google Scholar] [CrossRef] [Green Version]
- Crowell, M.; Harries, L.A.; Lunsford, T.N.; Dibiase, J.K. Emerging drugs for constipation. Expert Opin. Emerg. Drugs 2009, 14, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Serrano Falcón, B.; Barceló López, M.; Mateos Muñoz, B.; Álvarez Sánchez, A.; Rey, E. Fecal impaction: A systematic review of its medical complications. BMC Geriatr. 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emmanuel, A.; Mattace-Raso, F.; Neri, M.C.; Petersen, K.U.; Rey, E.; Rogers, J. Constipation in older people: A consensus statement. Int J. Clin. Pract. 2017, 71, e12920. [Google Scholar] [CrossRef] [PubMed]
- Halawi, H.M.; Maasri, K.A.; Mourad, F.H.; Barada, K.A. Faecal impaction: In-hospital complications and their predictors in a retrospective study on 130 patients. Colorectal Dis. 2012, 14, 231–236. [Google Scholar] [CrossRef]
- Wrenn, K. Fecal impaction. N. Engl. J. Med. 1989, 321, 658–662. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 15 April 2021).
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Higgins, J.P. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Agar, M.; Currow, D.; Plummer, J.; Seidel, R.; Carnahan, R.; Abernethy, A.P. Changes in anticholinergic load from regular prescribed medications in palliative care as death approaches. Palliat. Med. 2009, 23, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Wawruch, M.; Macugova, A.; Kostkova, L.; Luha, J.; Dukat, A.; Murin, J.; Kuzelova, M. The use of medications with anticholinergic properties and risk factors for their use in hospitalised elderly patients. Pharmacoepidemiol. Drug Saf. 2012, 21, 170–176. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, M.; Maidment, I.D.; Bennett, K.; Peklar, J.; Mulryan, N.; McCallion, P.; Henman, M.C. Association of anticholinergic burden with adverse effects in older people with intellectual disabilities: An observational cross-sectional study. Br. J. Psychiatry 2016, 209, 504–510. [Google Scholar] [CrossRef] [Green Version]
- Allen, C.; Zarowitz, B.J.; O’Shea, T.; Datto, C.; Olufade, T. Clinical and Functional Characteristics of Nursing Facility Residents with Opioid-Induced Constipation. Consult. Pharm. 2017, 32, 285–298. [Google Scholar] [CrossRef] [PubMed]
- Briet, J.; Javelot, H.; Heitzmann, E.; Weiner, L.; Lameira, C.; D’Athis, P.; Vailleau, J.L. The anticholinergic impregnation scale: Towards the elaboration of a scale adapted to prescriptions in French psychiatric settings. Therapie 2017, 72, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Mayer, T.; Meid, A.D.; Saum, K.U.; Brenner, H.; Schöttker, B.; Seidling, H.M.; Haefeli, W.E. Comparison of Nine Instruments to Calculate Anticholinergic Load in a Large Cohort of Older Outpatients: Association with Cognitive and Functional Decline, Falls, and Use of Laxatives. Am. J. Geriatr. Psychiatry 2017, 25, 531–540. [Google Scholar] [CrossRef]
- De Vreese, L.P.; Mantesso, U.; De Bastiani, E.; Marangoni, A.; Weger, E.; Gomiero, T. Anticholinergic burden in adult and elderly people with intellectual disabilities: Results from an Italian multicenter cross-sectional study. PLoS ONE 2018, 13, e0205897. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, J.; Burke, É.; Mulryan, N.; O’Dwyer, C.; Donegan, C.; McCallion, P.; O’Dwyer, M. Drug burden index to define the burden of medicines in older adults with intellectual disabilities: An observational cross-sectional study. Br. J. Clin. Pharmacol. 2018, 84, 553–567. [Google Scholar] [CrossRef]
- Sevilla-Sánchez, D.; Molist-Brunet, N.; González-Bueno, J.; Solà-Bonada, N.; Espaulella-Panicot, J.; Codina-Jané, C. Prevalence, risk factors and adverse outcomes of anticholinergic burden in patients with advanced conditions at hospital admission. Geriatr. Gerontol. Int. 2018, 18, 1159–1165. [Google Scholar] [CrossRef]
- Hwang, S.; Jun, K.; Ah, Y.M.; Han, E.; Chung, J.E.; Lee, J.Y. Impact of anticholinergic burden on emergency department visits among older adults in Korea: A national population cohort study. Arch. Gerontol. Geriatr. 2019, 85, 103912. [Google Scholar] [CrossRef]
- Chew, M.L.; Mulsant, B.H.; Pollock, B.G.; Lehman, M.E.; Greenspan, A.; Mahmoud, R.A.; Gharabawi, G. Anticholinergic activity of 107 medications commonly used by older adults. J. Am. Geriatr. Soc. 2008, 56, 1333–1341. [Google Scholar] [CrossRef]
- Han, L.; Agostini, J.V.; Allore, H.G. Cumulative anticholinergic exposure is associated with poor memory and executive function in older men. J. Am. Geriatr. Soc. 2008, 56, 2203–2210. [Google Scholar] [CrossRef] [PubMed]
- Sittironnarit, G.; Ames, D.; Bush, A.I.; Faux, N.; Flicker, L.; Foster, J. AIBL Research Group. Effects of anticholinergic drugs on cognitive function in older Australians: Results from the AIBL study. Dement. Geriatr. Cogn. Disord. 2011, 31, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Dauphinot, V.; Faure, R.; Omrani, S.; Goutelle, S.; Bourguignon, L.; Krolak-Salmon, P.; Mouchoux, C. Exposure to anticholinergic and sedative drugs, risk of falls, and mortality: An elderly inpatient, multicenter cohort. J. Clin. Psychopharmacol. 2014, 34, 565–570. [Google Scholar] [CrossRef] [PubMed]
- WHO. ATC/DDD Index. 2019. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 15 July 2019).
- Cardwell, K.; Hughes, C.M.; Ryan, C. The Association Between Anticholinergic Medication Burden and Health Related Outcomes in the ‘‘Oldest Old”: A Systematic Review of the Literature. Drugs Aging 2015, 32, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Welsh, T.J.; van der Wardt, V.; Ojo, G.; Gordon, A.L.; Gladman, J.R.F. Anticholinergic Drug Burden Tools/Scales and Adverse Outcomes in Different Clinical Settings: A Systematic Review of Reviews. Drugs Aging 2018, 35, 523–538. [Google Scholar] [CrossRef]
- Andre, L.; Gallini, A.; Montastruc, F.; Montastruc, J.-L.; Piau, A.; Lapeyre-Mestre, M.; Gardette, V. Association between anticholinergic (atropinic) drug exposure and cognitive function in longitudinal studies among individuals over 50 years old: A systematic review. Eur. J. Clin. Pharmacol. 2019, 75, 1631–1644. [Google Scholar] [CrossRef]
- Dimidi, E.; Cox, C.; Grant, R.; Scott, S.M.; Whelan, K. Perceptions of Constipation Among the General Public and People With Constipation Differ Strikingly From Those of General and Specialist Doctors and the Rome IV Criteria. Am. J. Gastroenterol. 2019, 114, 1116–1129. [Google Scholar] [CrossRef]
- Suares, N.C.; Ford, A.C. Prevalence of, and risk factors for, idiopathic constipation in the community: Systematic review and metaanalysis. Am. J. Gastroenterol. 2011, 106, 1582–1591. [Google Scholar] [CrossRef]
- Lozano-Ortega, G.; Johnston, K.M.; Cheung, A.; Wagg, A.; Campbell, N.L.; Dmochowski, R.R.; Ng, D.B. A review of published anticholinergic scales and measures and their applicability in database analyses. Arch. Gerontol. Geriatr. 2020, 87, 103885. [Google Scholar] [CrossRef]
- Collamati, A.; Martone, A.M.; Poscia, A.; Brandi, V.; Celi, M.; Marzetti, E.; Landi, F. Anticholinergic drugs and negative outcomes in the older population: From biological plausibility to clinical evidence. Aging Clin. Exp. Res. 2016, 28, 25–35. [Google Scholar] [CrossRef]

{kind=link}
| Study Year | Study Design | Population Setting (N) | Country | Age (Y) | Patients (N) | Duration (M) |
|---|---|---|---|---|---|---|
| Agar M. 2009 | Post-hoc analysis of a randomized controlled trial | Home-dwelling: 89.0% (410) Nursing homes 6.5% (30) | Australia | 71 ± 12 † | 461 § | 24 |
| Wawruch M. 2011 | Retrospective cohort study | Hospital | Slovakia | 78 ± 7 † | 1636 | 24 |
| Kuang-Hua H.2012 | Retrospective cohort study | National Health Insurance database | Taiwan | >65 | 72,556 | 12 |
| Allen C. 2017 | Retrospective cohort study | Nursing homes | United States | >18 | 6556 | 24 |
| Hwang S. 2019 | Retrospective cohort study | National Health Insurance database | Korea | 75 ± 7 † | 118,750 | 3 |
| O’Dwyer M. 2016 | Cross-sectional study | Home-dwelling: 16.6% (122) Nursing homes: 83.4% (614) | Ireland | 54 ± 9 † | 736 | - |
| Briet J. 2017 | Cross-sectional study | Psychiatric facility | France | 50 ‡ | 7278 | - |
| Mayer T. 2017 | Cross-sectional study | Home-dwelling | Germany | 73 ± 6 † | 2761 | - |
| De Vreese L. P. 2018 | Cross-sectional study | Nursing homes 57.6% (159) Home-dwelling 42.4% (117) | Italy | 55 ± 8 † | 276 | - |
| O’Connell J. 2018 | Cross-sectional study | Nursing homes: 84.9% (574) Home-dwelling: 15.1% (102) | Ireland | >40 | 676 | - |
| Sevilla-Sánchez D. 2018 | Cross-sectional study | Hospital | Spain | 87 ± 5 † | 235 | - |
| Study Year | Patients (N) | Assessment Method for Constipation | Constipation Prevalence (N) | Anticholinergic Exposure (N) | Most Prescribed Drugs |
|---|---|---|---|---|---|
| Agar M. 2009 | 461 | Clinical assessment | No Data | No Data | Opioids |
| Wawruch M. 2011 | 1636 | Clinical assessment | 8.0% (131) | Admission: 10.5% (172) ‡ Discharge: 13.6% (223) ‡ | Opioids |
| Sevilla-Sánchez D. 2018 | 235 | Clinical assessment | 62.1% (146) | ADS: 93.6% (220) DBI: 82.1% (193) | No Data |
| O’Dwyer M. 2016 | 736 | Clinical assessment and laxative prescriptions | No Data | 70.1% (516) | Antipsychotics |
| Allen C. 2017 | 6556 | Clinical charts andlaxative prescriptions | 8.9% † | 73.4% (4811) | Opioids |
| Briet J. 2017 | 7278 | Laxative prescriptions | 48.2% (3509) | 97.2% (7077) | Antipsychotics |
| Mayer T. 2017 | 2761 | Laxative prescriptions | 1.5% (41) | 45.6% (1258) | No Data |
| De Vreese L. P. 2018 | 276 | Laxative prescriptions | 10.5% (29) | 35.5% (98) | Antipsychotics |
| Kuang-Hua H. 2012 | 72,556 | Laxative prescriptions | 7.9% (5742) | 75.7% (54,888) | No Data |
| O’Connell J. 2018 | 676 | Patient´s self-reports | 38.4% (257) | 78.6% (532) | Antiepileptics |
| Hwang S. 2019 | 118,750 | Diagnostic codes in emergency department visit claims | 0.5% (567) | 36.5% † | No Data |
| Study Year | Patient’s Groups Compared When Looking for a Correlation | Anticholinergic Scale | Association § | Association Magnitude § |
|---|---|---|---|---|
| Wawruch M. 2011 | Anticholinergic burden; 0 vs. >0 * | Anticholinergic Risk Scale † | + | OR: 1.91 (1.18–3.11) |
| Clinician-Rated Anticholinergic Scale † | ||||
| Kuang-Hua H. 2012 | Anticholinergic burden; 0 vs. >0 * | Anticholinergic Risk Scale | + | OR: 1.87 (1.72–2.03) |
| Hwang S. 2019 | Anticholinergic burden; 0 vs. ≥2 | Anticholinergic Risk Scale † | + | HR: 1.65 (1.35–2.02) |
| Mayer T. 2017 | Anticholinergic burden; 0 vs. >0 * | Anticholinergic Risk Scale | + | OR: 1.47 (p = 0.02) |
| Anticholinergic Burden Classification | + | OR: 1.58 (p < 0.001) | ||
| Cancelli’s Anticholinergic Burden Scale | + | OR: 1.58 (p < 0.001) | ||
| Chew’s list | + | OR: 1.57 (p = 0.002) | ||
| Anticholinergic Drug Scale | - | OR: 1.24 (p = 0.17) | ||
| Clinician-Rated Anticholinergic Scale | - | OR: 1.47 (p = 0.08) | ||
| Drug Burden Index | - | OR: 1.14 (p = 0.45) | ||
| Anticholinergic Loading scale | - | OR: 1.14 (p = 0.45) | ||
| Anticholinergic Cognitive Burden Scale | - | OR: 1.06 (p = 0.77) | ||
| ‘O’Dwyer M. 2016 | Anticholinergic burden; 0 vs. 1–4 vs. >5 | Anticholinergic Cognitive Burden Scale † | + | χ2: p < 0.001 |
| Allen C. 2017 | Patients with and without constipation | Anticholinergic Cognitive Burden Scale | + | χ2: p < 0.001 |
| De Vreese L. P. 2018 | Anticholinergic burden; 0 vs. >3 | Anticholinergic Cognitive Burden Scale | + | χ2: p = 0.003 |
| O’Connell J. 2018 | Anticholinergic burden; 0 vs. (0–1) ‡ | Drug Burden Index | - | OR: 1.28 (0.64–2.53) |
| Anticholinergic burden; 0 vs. ≥1 | - | OR: 1.68 (0.90–3.12) | ||
| Sevilla-Sánchez D. 2018 | Anticholinergic burden; 0 vs. >0 * | Drug Burden Index | + | χ2: p = 0.03 |
| Anticholinergic burden; 0 vs. 1–2 vs. >2 | - | χ2: p = 0.11 | ||
| Anticholinergic burden; 0 vs. >0 * | Anticholinergic Drug Scale | - | χ2: p = 0.46 | |
| Anticholinergic burden; < 3 vs. ≥3 | - | χ2: p = 0.92 | ||
| Agar M. 2009 | Anticholinergic burden; 0 vs. >0 | Clinician-Rated Anticholinergic Scale † | - | OR: 1.05 (0.98–1.12) |
| Briet J. 2017 | Anticholinergic burden; ≤5 vs.>5 | Anticholinergic impregnation scale | + | OR: 2.03 (1.81–2.28) |
| Anticholinergic Scale | Studies | Association Assessments | Association Present (+) | Association Absent (-) | ||
|---|---|---|---|---|---|---|
| Association Assessments | Patients Involved | Association Assessments | Patients Involved | |||
| Anticholinergic Risk Scale † | 4 | 4 | 4 | 195,703 | 0 | 0 |
| Anticholinergic Cognitive Burden Scale | 4 | 4 | 3 | 7568 | 1 | 2761 |
| Clinician-Rated Anticholinergic Scale † | 3 | 3 | 1 | 1636 | 2 | 3222 |
| Drug Burden Index | 3 | 5 | 1 | 235 | 4 | 4113 |
| Anticholinergic Drug Scale | 2 | 3 | 0 | 0 | 3 | 2555 |
| Anticholinergic impregnation scale | 1 | 1 | 1 | 7278 | 0 | 0 |
| Cancelli’s Anticholinergic Burden Scale | 1 | 1 | 1 | 2761 | 0 | 0 |
| Chew’s list | 1 | 1 | 1 | 2761 | 0 | 0 |
| Anticholinergic Burden Classification | 1 | 1 | 1 | 2761 | 0 | 0 |
| Anticholinergic Loading scale | 1 | 1 | 0 | 0 | 1 | 2761 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Ramallo, H.; Báez-Gutiérrez, N.; Prado-Mel, E.; Alfaro-Lara, E.R.; Santos-Ramos, B.; Sánchez-Fidalgo, S. Association between Anticholinergic Burden and Constipation: A Systematic Review. Healthcare 2021, 9, 581. https://doi.org/10.3390/healthcare9050581
Rodríguez-Ramallo H, Báez-Gutiérrez N, Prado-Mel E, Alfaro-Lara ER, Santos-Ramos B, Sánchez-Fidalgo S. Association between Anticholinergic Burden and Constipation: A Systematic Review. Healthcare. 2021; 9(5):581. https://doi.org/10.3390/healthcare9050581
Chicago/Turabian StyleRodríguez-Ramallo, Héctor, Nerea Báez-Gutiérrez, Elena Prado-Mel, Eva Rocío Alfaro-Lara, Bernardo Santos-Ramos, and Susana Sánchez-Fidalgo. 2021. "Association between Anticholinergic Burden and Constipation: A Systematic Review" Healthcare 9, no. 5: 581. https://doi.org/10.3390/healthcare9050581