
Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review



Abstract
:1. Introduction
1.1. Scoping Review Research Question
1.2. Review Objective
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Extraction and Analysis
3. Results
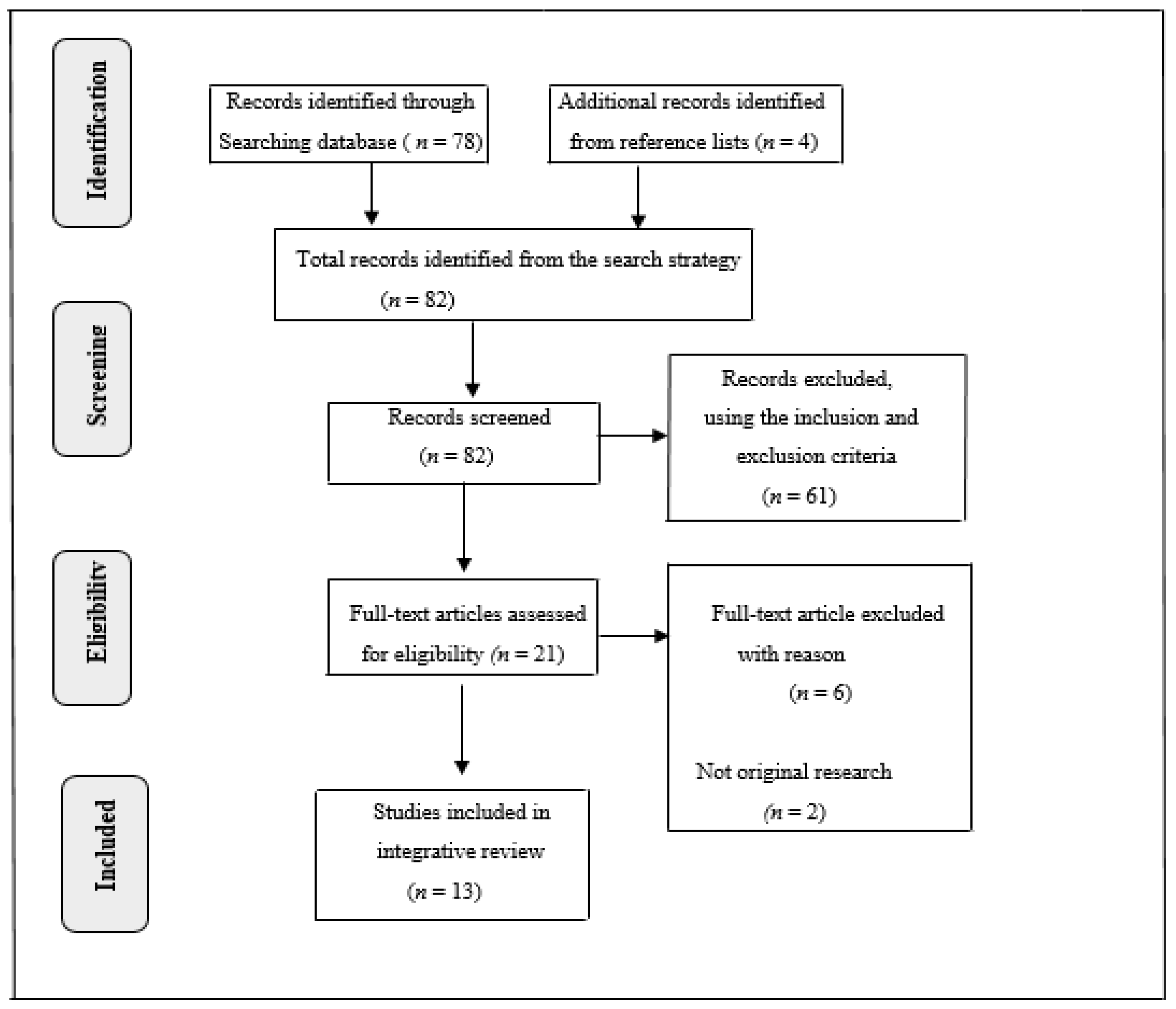
3.1. Search Outcome
3.2. Characteristics of Reviewed Articles
3.3. Themes Emerging from Studies Reviewed
3.3.1. Providers’ Knowledge
3.3.2. Providers’ Attitudes
3.3.3. Providers’ Practices
3.4. Barriers to Prenatal Physical Activity Counselling
4. Discussion
5. Limitations, Strengths and Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dipietro, L.; Evenson, K.R.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E. Benefits of physical activity during pregnancy and postpartum: An umbrella review. Med. Sci. Sports Exerc. 2019, 51, 1292–1302. [Google Scholar] [CrossRef]
- Ruchat, S.M.; Mottola, M.F.; Skow, R.J.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef]
- Harrison, A.L.; Taylor, N.F.; Shields, N.; Frawley, H.C. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. Physiotheraphy 2018, 64, 24–32. [Google Scholar] [CrossRef]
- Aune, D.; Schlesinger, S.; Henriksen, T.; Saugstad, O.; Tonstad, S. Physical activity and the risk of preterm birth: A systematic review and meta-analysis of epidemiological studies. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1816–1826. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Catov, J.M.; Parker, C.B.; Gibbs, B.B.; Bann, C.M.; Carper, B.; Silver, R.M.; Simhan, H.N.; Parry, S.; Chung, J.H.; Haas, D.M.; et al. Patterns of leisure-time physical activity across pregnancy and adverse pregnancy outcomes. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Thompson, E.L.; Vamos, C.A.; Daley, E.M. Physical activity during pregnancy and the role of theory in promoting positive behavior change: A systematic review. J. Sport Health Sci. 2017, 6, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Barakat, R.; Pelaez, M.; Lopez, C.; Montejo, R.; Coteron, J. Exercise during pregnancy reduces the rate of caesarean and instrumental deliveries: Results of a randomized controlled trial. J. Matern. Fetal Neonatal Med. 2012, 25, 2372–2376. [Google Scholar] [CrossRef] [Green Version]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; E Gray, C.; Barrowman, N.; Riske, L. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1376–1385. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Terrones, M.; Barakat, R.; Santacruz, B.; Fernandez-Buhigas, I.; Mottola, M.F. Physical exercise programme during pregnancy decreases perinatal depression risk: A randomised controlled trial. Br. J. Sports Med. 2018, 53, 348–353. [Google Scholar] [CrossRef]
- Cid, M.; González, M. Potential benefits of physical activity during pregnancy for the reduction of gestational diabetes prevalence and oxidative stress. Early Hum. Dev. 2016, 94, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.H.; Rothenberger, S.D.; Kline, C.E.; Okun, M.L. Exercise during Early Pregnancy is Associated with Greater Sleep Continuity. Behav. Sleep Med. 2018, 16, 482–493. [Google Scholar] [CrossRef]
- Nguyen, C.L.; Pham, N.M.; Lee, A.H.; Nguyen, P.T.H.; Chu, T.K.; Ha, A.V.V.; Duong, D.V.; Duong, T.H.; Binns, C.W. Physical activity during pregnancy is associated with a lower prevalence of gestational diabetes mellitus in Vietnam. Acta Diabetol. 2018, 55, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Sooknarine-Rajpatty, J.; Auyeung, A.B.; Doyle, F. A systematic review protocol of the barriers to both physical activity and obesity counselling in the secondary care setting as reported by healthcare providers. Int. J. Environ. Res. Public Health 2020, 17, 1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef] [PubMed]
- Gaston, A.; Cramp, A.; Prapavessis, H. Enhancing self-efficacy and exercise readiness in pregnant women. Psychol. Sport Exerc. 2012, 13, 550–557. [Google Scholar] [CrossRef]
- Moyer, C.; Reoyo, O.R.; May, L. The influence of prenatal exercise on offspring health: A review. Clin. Med. Insights Women’s Health 2016, 9, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.M.; Cooke, A.; Lavender, T. Maternal obesity is the new challenge; a qualitative study of health professionals’ views towards suitable care for pregnant women with a Body Mass Index (BMI) ≥ 30 kg/m2. BMC Pregnancy Childbirth 2012, 12, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, Z.; Bush, J.; Robson, S.J.; McParlin, C.; Rankin, J.; Bell, R. Physical activity in pregnancy: A qualitative study of the beliefs of overweight and obese pregnant women. BMC Pregnancy Childbirth 2010, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Goodrich, K.; Cregger, M.; Wilcox, S.; Liu, J. A qualitative study of factors affecting pregnancy weight gain in African American women. Matern. Child. Health J. 2013, 17, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Sui, Z.; Turnbull, D.; Dodd, J. Overweight and obese women’s perceptions about making healthy change during pregnancy: A mixed method study. Matern. Child Health J. 2013, 17, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.M.; Siega-Riz, A.M.; Evenson, K.R.; Moos, M.K.; Carrier, K.S. A qualitative study of women’s perceptions of provider advice about diet and physical activity during pregnancy. Patient Educ. Couns. 2013, 91, 372–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K.M.; Wilcox, S.; Liu, J.; Blair, S.N.; Pate, R.R. Pregnant women’s perceptions of weight gain, physical activity, and nutrition using Theory of Planned Behaviour constructs. J. Behav. Med. 2016, 39, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Leiferman, J.; Sinatra, E.; Huberty, J. Pregnant women’s perceptions of patient provider communication for health behaviour change during pregnancy. Open J. Obstet. Gynecol. 2014, 4, 672–684. [Google Scholar] [CrossRef] [Green Version]
- Santo, E.C.; Forbes, P.W.; Oken, E.; Belfort, M.B. Determinants of physical activity frequency and provider advice during pregnancy. BMC Pregnancy Childbirth 2017, 17, 286. [Google Scholar] [CrossRef] [Green Version]
- Vinturache, A.E.; Winn, A.; Tough, S.C. Recall of prenatal counselling among obese and overweight women from a Canadian population: A population based study. Matern. Child Health J. 2017, 21, 2092–2101. [Google Scholar] [CrossRef]
- Stengel, M.R.; Kraschnewski, J.L.; Hwang, S.W.; Kjerulff, K.H.; Chuang, C.H. “What my doctor didn’t tell me”: Examining health care provider advice to overweight and obese pregnant women on gestational weight gain and physical activity. Women’s Health Issues 2012, 22, e535–e540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emery, R.L.; Benno, M.T.; Salk, R.H.; Kolko, R.P.; Levine, M.D. Healthcare provider advice on gestational weight gain: Uncovering a need for more effective weight counselling. J. Obstet. Gynaecol. 2018, 38, 916–921. [Google Scholar] [CrossRef]
- Dalhaug, E.M.; Haakstad, L.A.H. What the health? Information sources and maternal lifestyle behaviors. Interact. J. Med. Res. 2019, 8, e10355. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.; Mcinerney, P.; Soares, C.B.; Khalil, H.; Parker, D. Chapter 11: Scoping reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Dieterich, R.; Demirci, J. Communication practices of healthcare professionals when caring for overweight/obese pregnant women: A scoping review. Patient Educ. Couns. 2020, 103, 1902–1912. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.W.; Broman, C.L.; Pivarnik, J.M. Exercise and pregnancy knowledge among healthcare providers. J. Women’s Health 2010, 19, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Leiferman, J.; Gutilla, M.; Paulson, J.; Pivarnik, J. Antenatal physical activity counselling among healthcare providers. Open J. Obstet. Gynecol. 2012, 2, 346–355. [Google Scholar] [CrossRef] [Green Version]
- May, L.E.; Suminski, R.R.; Linklater, E.R.; Jahnke, S.; Glaros, A.G. Exercise during pregnancy: The role of obstetric providers. J. Am. Osteopath. Assoc. 2013, 113, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Stotland, N.E.; Gilbert, P.; Bogetz, A.; Harper, C.C.; Abrams, B.; Gerbert, B. Preventing excessive weight gain in pregnancy: How do prenatal care providers approach counselling? J. Women’s Health 2010, 19, 807–814. [Google Scholar] [CrossRef] [PubMed]
- De Vivo, M.; Mills, H. “They turn to you first for everything”: Insights into midwives’ perspectives of providing physical activity advice and guidance to pregnant women. BMC Pregnancy Childbirth 2019, 19, 462. [Google Scholar] [CrossRef]
- Hopkinson, Y.; Hill, D.M.; Fellows, L.; Fryer, S. Midwives understanding of physical activity guidelines during pregnancy. Midwifery 2018, 59, 23–26. [Google Scholar] [CrossRef]
- McParlin, C.; Bell, R.; Robson, S.C.; Muirhead, C.R.; Araújo-Soares, V. What helps or hinders midwives to implement physical activity guidelines for obese pregnant women? A questionnaire survey using the Theoretical Domains Framework. Midwifery 2017, 49, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.D.; Oddie, B.; Constantinou, D. Exercise during pregnancy: Knowledge and beliefs of medical practitioners in South Africa: A survey study. BMC Pregnancy Childbirth 2015, 15, 245. [Google Scholar] [CrossRef] [Green Version]
- Malta, M.B.; Carvalhaes, M.D.; Takito, M.Y.; Tonete, V.L.P.; Aluísio, J.D.; Barros, A.J.D.; de Lima Parada, C.M.G.; D’Aquino Benício, M.H. Educational intervention regarding diet and physical activity for pregnant women: Changes in knowledge and practices among health professionals. BMC Pregnancy Childbirth 2016, 16, 175. [Google Scholar] [CrossRef] [Green Version]
- Haakstad, L.A.H.; Mjønerud, J.M.F.; Dalhaug, E.M. MAMMA MIA! Norwegian midwives’ practices and views about gestational weight gain, physical activity, and nutrition. Front. Psychol. 2020, 11, 1463. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, M.; Mogren, I.; Eurenius, E.; Edvardsson, K.; Persson, M. “An on-going individual adjustment”: A qualitative study of midwives’ experiences counselling pregnant women on physical activity in Sweden. BMC Pregnancy Childbirth 2014, 14, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issakainen, M.; Schwab, U.; Lamminpää, R. Qualitative study on public health nurses’ experience and assessment of nutritional and physical activity counselling of women with gestational diabetes. Eur. J. Midwifery 2020, 4, 37. [Google Scholar] [CrossRef]
- de Jersey, S.; Guthrie, T.; Tyler, J.; Ling, W.Y.; Powlesland, H.; Byrne, C.; New, K. A mixed method study evaluating the integration of pregnancy weight gain charts into antenatal care. Matern. Child Nutr. 2019, 15, e12750. [Google Scholar] [CrossRef]
- Lindsay, A.C.; Wallington, S.F.; Greaney, M.L.; Machado, M.M.T.; De Andrade, G.P. Patient–provider communication and counselling about gestational weight gain and physical activity: A qualitative study of the perceptions and experiences of Latinas pregnant with their first child. Int. J. Environ. Res. Public Health 2017, 14, 1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Obstetricians and Gynaecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynaecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Homepage. Available online: www.who.int (accessed on 29 March 2021).
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. No. 367-2019 Canadian Guideline for Physical Activity throughout Pregnancy. J. Obstet. Gynaecol. Can. 2018, 40, 1528–1537. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Arena, R.; Riebe, D.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; American College of Sports Medicine: Baltimore, MD, USA, 2014; ISBN 9781609136055. [Google Scholar]
- Alahmed, Z.; Lobelo, F. Correlates of physical activity counselling provided by physicians: A cross-sectional study in Eastern Province, Saudi Arabia. PLoS ONE 2019, 14, e0220396. [Google Scholar] [CrossRef]
- Kime, N.; Pringle, A.; Zwolinsky, S.; Vishnubala, D. How prepared are healthcare professionals for delivering physical activity guidance to those with diabetes? A formative evaluation. BMC Health Serv. Res. 2020, 20, 8. [Google Scholar] [CrossRef]
- Din, N.U.; Moore, G.F.; Murphy, S.; Wilkinson, C.; Williams, N.H. Health professionals’ perspectives on exercise referral and physical activity promotion in primary care: Findings from a process evaluation of the National Exercise Referral Scheme in Wales. Health Educ. J. 2015, 74, 743–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebert, E.T.; Caughy, M.O.; Shuval, K. Primary care providers’ perceptions of physical activity counselling in a clinical setting: A systematic review. Br. J. Sports Med. 2012, 46, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Willcox, J.C.; Campbell, K.J.; van der Pligt, P.; Hoban, E.; Pidd, D.; Wilkinson, S. Excess gestational weight gain: An exploration of midwives’ views and practice. BMC Pregnancy Childbirth 2012, 12, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, E.A.; Mottola, M.F.; Chambliss, H. Integrating exercise is medicine® into the care of pregnant women. Cur. Sports Med. Rep. 2013, 12, 245–247. [Google Scholar] [CrossRef]
- Sinclair, M.B.; Liddle, D.; Hill, A.; Stockdale, D.; Stockdale, M. Motivating pregnant women to eat healthily and engage in physical activity for weight management: An exploration of routine midwife instruction. Evid. Based Midwifery 2013, 11, 120–127. [Google Scholar]
- Aittasalo, M.; Raitanen, J.; Kinnunen, T.I.; Ojala, K.; Kolu, P.; Luoto, R. Is intensive counselling in maternity care feasible and effective in promoting physical activity among women at risk for gestational diabetes? Secondary analysis of a cluster randomized NELLI study in Finland. Int. J. Behav. Nutri. Phys. Act. 2012, 9, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, E.D.; Norris, S.A.; Draper, C.E.; Jones, R.A.; van Poppel, M.N.M.; Micklesfield, L.K. “Just because you’re pregnant, doesn’t mean you’re sick!” A qualitative study of beliefs regarding physical activity in black South African women. BMC Pregnancy Childbirth 2016, 16, 174. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Country | Study Design | Sample and Sampling | Outcome Measure(s) | Findings | Limitations |
|---|---|---|---|---|---|
| USA [23] | Qualitative study | 11 prenatal healthcare providers | Provider perceptions on physical activity counselling during prenatal care visits. | Most healthcare providers reported offering prenatal physical activity counselling during prenatal visit. Walking and swimming were the physical activities. recommended. Healthcare providers understood the benefits of prenatal physical activity counselling during pregnancy. Barriers to prenatal physical activity counselling included a lack of patient interest, lack of time, lack of training, and the low socioeconomic status of the patient. Providers were familiar with the ACOG guidelines. Advocated for further training on prenatal physical activity counselling. | Small sample size. Limited generalisability of findings. Self-reported information subject to recall and social desirability bias. |
| USA [34] | Cross-sectional descriptive study | Convenient sample of 93 healthcare providers. | Knowledge, beliefs, and practices of obstetric healthcare providers toward exercise during pregnancy. | Healthcare providers exhibited positive beliefs and attitudes about exercise during pregnancy. Providers recommended exercise to their pregnant patients (90%) and believed women with uncomplicated pregnancies can safely practice exercise (89%). Providers offered prenatal physical activity advice; however, the advice did not always align with the ACOG recommendations on prenatal physical activity because the providers were not familiar with the ACOG guidelines. | Non-randomisation of sample. Potential recall bias. Use of the ACOG guidelines. |
| USA [35] | Cross-sectional descriptive study | Convenient sample of 188 healthcare providers (91 obstetricians, 40 midwives, and 57 family medicine physicians) | Beliefs, attitudes, knowledge, self-efficacy and barriers. | Majority of the healthcare providers agreed that prenatal physical activity improves the general health of the mother and baby, and reduce excessive weight gain. They stressed the need for discussing physical activity with pregnant women; however, only about two-thirds did so with their patients. Over 40% providers were not confident with the physical activity information they had provided to women. Slightly over half of the healthcare providers offered in-office physical activity counselling, 90% accurately described the types of exercises generally considered safe for pregnant women, and 85% correctly identify the ACOG’s absolute contraindications to antenatal physical activity. Lack of time was a common barrier, and providers felt they received inadequate training. | Low response rate. Small sample from localised area. Potential recall bias. |
| USA [36] | Cross-sectional, retrospective study | 31 Obstetricians | Association between obstetric providers’ discussions about exercise and pregnant woman exercise behaviours. | Obstetric providers’ discussion of exercise associated with patient behaviour. Obstetric providers’ ages, private insurance, number of pregnant patients seen per month; pregnant patients with complications were not associated with exercise discussion with pregnant patients. | Small sample size. Recall bias due to self-report. |
| USA [37] | Qualitative study | Convenience sample of 52 obstetrician/gynaecologists, midwives and nurse practitioners. | Knowledge, attitudes, and practices of prenatal care providers regarding prenatal physical activity counselling. | Providers had no training on prenatal physical activity, but relied on their own personal experiences. Prenatal physical activity was not a priority. | Small sample size. Recall bias due to self-report. |
| United Kingdom [38] | Multiphase mixed methods | 10 randomly selected midwives | Roles, responsibilities, and barriers in providing physical activity advice and guidance to pregnant women; and any opportunities in changing pregnant women’s physical activity behaviour. | Midwives’ daily challenges affected their morale and ability to provide antenatal physical activity counselling. Midwives did not provide adequate information about prenatal physical activity. Less priority was accorded to physical activity. Barriers to prenatal physical activity advice and guidance included a lack of training, knowledge, confidence, time, and resources. Suggestions to address barriers included professional development and training, inter-professional collaboration, encouraging a support network, and challenging misconceptions about prenatal physical activity. | Small sample from localised area. |
| United Kingdom [39] | Descriptive online survey | 59 Midwives | Midwives understanding of the NICE physical activity guidelines, and the physical activity guidance provided to women during pregnancy. | Midwives had misplaced confidence in their knowledge of the NICE physical activity guidelines for pregnancy. The positive role of exercise and benefits to mother and baby were recognised by 24% of the midwives. The majority of midwives (91%) knew about the contraindications to exercise during pregnancy, and 59% felt confident answering questions about prenatal physical activity. | Small sample size. Participants skewed to those who felt confident in their knowledge about physical activity and pregnancy. Overestimation of the findings from the midwives based on prior information about the survey. |
| England [40] | Cross-sectional descriptive study | 192 Midwives | Barriers and facilitators associated with implementation of national guidelines for physical activity in obese pregnant woman. | Midwives perceived as not having the ability, proficiency or competency to implement, discuss and counsel women effectively on physical activity. Physical activity was not a priority. Midwives recognised their role to advise obese pregnant women about physical activity, but expressed concerns about the sensitive nature of the topic. Midwives advocated for routine prenatal physical counselling in clinical practice. | Poor response rate might result to error and bias. |
| South Africa [41] | Cross- sectional, descriptive study. | Convenience sample of 96 Medical Practitioners (MPs): General Practitioners (n = 58), Obstetricians/Gynaecologists (n = 33), other Specialists (n = 5). | Knowledge, attitudes and beliefs of South African MPs towards prenatal exercise. | Majority of the medical practitioners believed prenatal exercise is beneficial, but were unaware of the recommended exercise guidelines. They lacked accurate specifics about exercise prescription. Most MPs (94%) recommended moderate exercise during pregnancy. Few practitioners provided advice as well as individualised exercise prescription. Providers were not familiar with the ACOG guidelines for exercise during pregnancy. About 71% expressed a desire to attend a continuous professional development workshop on prenatal physical activity, if provided. | Low response rate. Response and selective bias. Exclusion of practitioners working in the public sector. |
| Brazil [42] | A controlled, non-randomized study | Doctors and nurses: Intervention group (22); Control group (20) | Effect of an educational intervention upon improving the knowledge and practices of health professionals concerning physical activity during pregnancy. | No difference in the knowledge scores between the control group and the intervention group. Compared to the control group, women in the intervention group were more likely to receive guidance regarding leisure-time walking. | Non randomisation of the sample in both groups. |
| Norway [43] | Cross-sectional descriptive study | 65 Midwives | Midwives’ practice and views about gestational weight gain and regular physical activity and nutrition. | Physical activity advice provided at least once throughout gestation. About 32.3% midwives based their advice on personal sport/exercise experience. | Small sample size. Recall bias due to self-report. |
| Sweden [44] | A qualitative study | Purposive sample of 41 midwives | Swedish midwives experience about prenatal physical activity counselling; and the facilitators and barriers during pregnancy. | Barriers to prenatal physical counselling included a lack of resources and cultural expectations of the women about physical activity during pregnancy. Midwives considered the topic as sensitive for some women, especially overweight and obese women. Individualised counselling approach applied. | |
| Finland [45] | Descriptive qualitative approach. | Convenience sample of 11 public health nurses. | Public health nurses’ experiences of physical activity counselling. | Level of knowledge and skills about physical activity counselling was inadequate. Barrier to prenatal physical activity included women’s attitudes towards exercise, lack of time, inadequate resources, and insufficient skills. Providers suggested fmulti-professional collaboration from different healthcare areas, such as physiotherapists, physical education instructors, and dieticians. They advocated further training in physical activity. | Small sample size. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okafor, U.B.; Goon, D.T. Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review. Healthcare 2021, 9, 609. https://doi.org/10.3390/healthcare9050609
Okafor UB, Goon DT. Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review. Healthcare. 2021; 9(5):609. https://doi.org/10.3390/healthcare9050609
Chicago/Turabian StyleOkafor, Uchenna Benedine, and Daniel Ter Goon. 2021. "Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review" Healthcare 9, no. 5: 609. https://doi.org/10.3390/healthcare9050609
APA StyleOkafor, U. B., & Goon, D. T. (2021). Physical Activity Advice and Counselling by Healthcare Providers: A Scoping Review. Healthcare, 9(5), 609. https://doi.org/10.3390/healthcare9050609