
The Effects of Social Support and Morbidities on Self-Rated Health among Migrant Elderly Following Children to Jinan, China


Abstract
1. Introduction
2. Methods
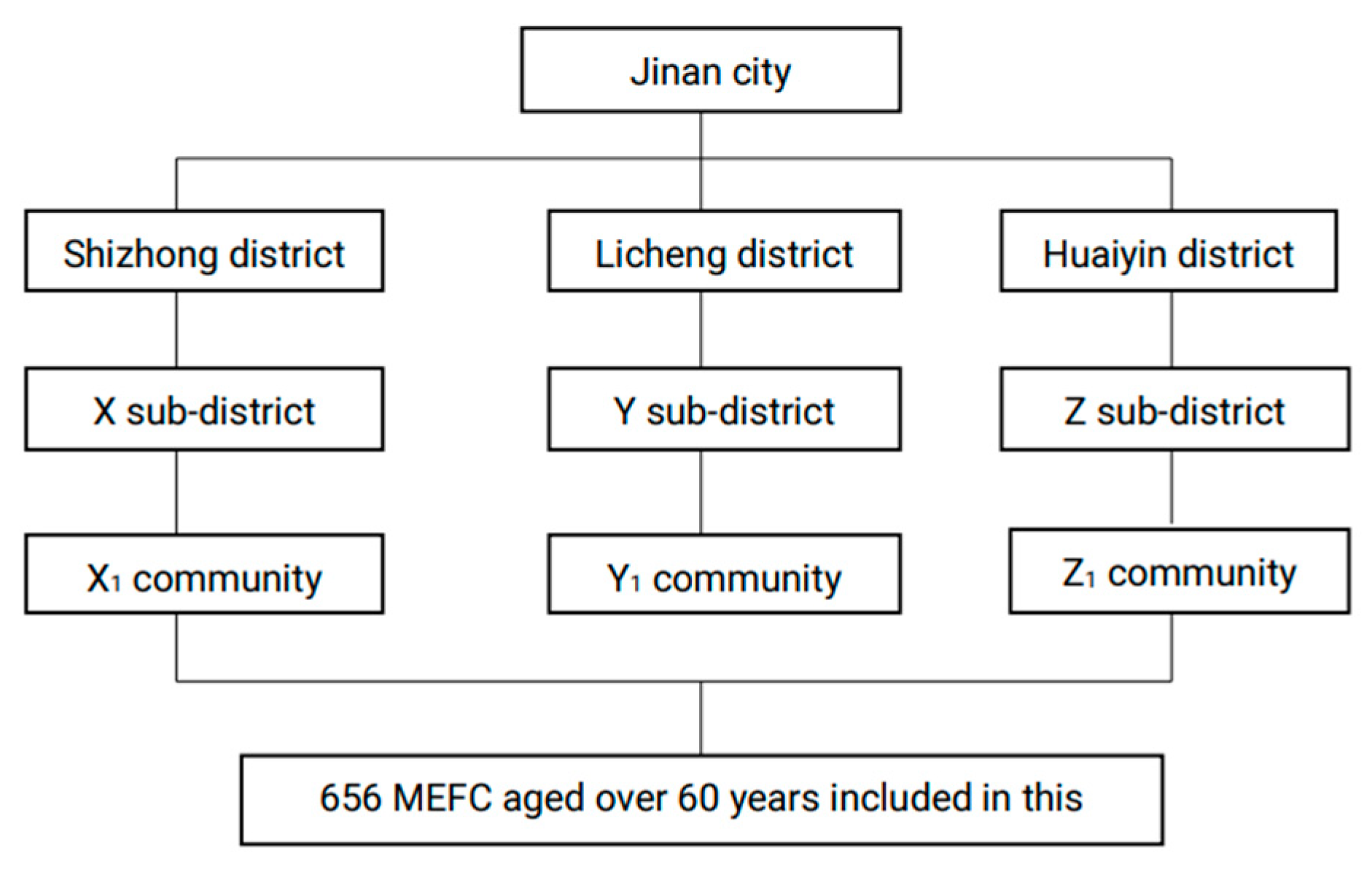
2.1. Data Collection and Research Subjects
2.2. Variables
2.2.1. Dependent Variable
2.2.2. Independent Variables
Sociodemographic Characteristics
Social Support
Morbidities
2.3. Analysis Approach
3. Results
3.1. The Demographic Characteristics
3.2. Social Support
3.3. Morbidities and Self-Rated Health
3.4. The Association between Social Support, Morbidities and Self-Rated Health
4. Discussion
4.1. Association between Demographic Characteristics and Self-Rated Health
4.2. Association between Morbidities and Self-Rated Health
4.3. Association between Social Support and Self-Rated Health
4.4. Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Bureau of Statistics of China (NBS). China Statistical Year Book 2020; China Statistics Press: Beijing, China, 2020.
- Lin, K.; Yin, P.; Loubere, N. Social Support and the ‘Left Behind’ Elderly in Rural China: A Case Study from Jiangxi Province. J. Community Health 2014, 39, 674–681. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission (NHC). Report on China’s Floating Population Development 2018; China Population Publishing House: Beijing, China, 2018. [Google Scholar]
- Wang, Q. Health of the Elderly Migration Population in China: Benefit from Individual and Local Socioeconomic Status? Int. J. Environ. Res. Public Health 2017, 14, 370. [Google Scholar] [CrossRef]
- Tang, D.; Wang, J. Basic Public Health Service Utilization by Internal Older Adult Migrants in China. Int. J. Environ. Res. Public Health 2021, 18, 270. [Google Scholar] [CrossRef]
- Lin, Y.; Chu, C.; Chen, Q.; Xiao, J.; Wan, C. Factors influencing utilization of primary health care by elderly internal migrants in China: The role of social contacts. BMC Public Health 2020, 20, 1054. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yin, H. A study on the social integration of the “Lao Piao tribe” from the perspective of social support networks: Taking Guangzhou as an example. Sci. Res. Aging 2016, 04, 53–64. [Google Scholar]
- Qi, Y.; Zhang, X. Research on the status and influencing factors of social support for the elderly in urban communities. Chin. Gen. Pract. 2016, 19, 3099–3102. [Google Scholar]
- Kong, F.; Kong, M.; Li, C.; Li, S.; Lv, J. Research progress of the elderly migrant following child at home and abroad. Chin. J. Gerontol. 2020, 40, 2443–2447. [Google Scholar]
- Wallston, B.S.; Pdagna, S.W.; DeVellis, B.M. Social support and physical health. J. Health Psychol. 1983, 2, 367–391. [Google Scholar] [CrossRef]
- Xiao, S. Social Support Scale: Theoretical Basis and Research Application. J. Clin. Psychiatry 1994, 4, 98–100. [Google Scholar]
- Li, M. A Review on the Social Adaptation of the Elderly. Sci. Res. Aging 2014, 2, 20–27. [Google Scholar]
- Schoenmakers, D.; Lamkaddem, M.; Suurmond, J. The Role of the Social Network in Access to Psychosocial Services for Migrant Elderly—A Qualitative Study. Int. J. Environ. Res. Public Health 2017, 14, 1215. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.; Becker, T.; McCrone, P.; Thornicroft, G. Social networks and mental health service utilization—A literature review. Int. J. Soc. Psychiatry 1998, 44, 248–266. [Google Scholar] [CrossRef] [PubMed]
- Jennings, E.A.; Ralston, M.; Schatz, E. Support in times of need: How depressive symptoms can impact receipt of social support among aging adults in rural South Africa. SSM Popul. Health 2020, 12, 100666. [Google Scholar] [CrossRef] [PubMed]
- Giang, L.T.; Nguyen, T.T.; Nguyen, N.T. Social Support and Self-Rated Health among Older Men and Women in Vietnam. JPA 2020, 13, 427–442. [Google Scholar]
- Amoah, P. The Relationship between Functional Health Literacy, Self-Rated Health, and Social Support between Younger and Older Adults in Ghana. Int. J. Environ. Res. Public Health 2019, 16, 3188. [Google Scholar] [CrossRef]
- Perruccio, A.V.; Katz, J.N.; Losina, E. Health burden in chronic disease: Comorbidity is associated with self-rated health more than medical comorbidity alone. J. Clin. Epidemiol. 2012, 65, 100–106. [Google Scholar] [CrossRef]
- Kaneva, M.; Gerry, C.J.; Baidin, V. The effect of chronic conditions and multi-morbidity on self-assessed health in Russia. Scand. J. Public Health 2018, 46, 886–896. [Google Scholar] [CrossRef]
- Zhu, L.; Zhu, G.; Meng, M.; Wu, X. Self-rated health status of Bengbu residents and its influencing factors. Chin. J. Dis. Control 2018, 22, 1173–1176. [Google Scholar]
- Wang, X.; Wang, L.; Wang, Z.; Qi, S.; Zhang, X.; Chen, Z.; Zhang, M. Status and influencing factors of self-rated health of elderly people in China. Chin. J. Prevent. Control Chronic Dis. 2019, 27, 406–411. [Google Scholar]
- Yi, D. Migrant elderly: A group in urgent need of social attention. J. Lanzhou IOE 2014, 30, 46–47. [Google Scholar]
- Duan, L. The Impact of Social Support on the Social Integration of Migrant Elderly; Northwest A & F University: Xianyang, China, 2018. [Google Scholar]
- Cui, L.; Li, H. Research on Social Support Network and Life Satisfaction of Urban Elderly. Psychol. Sci. 1997, 20, 123–126. [Google Scholar]
- Tong, X. Social Work Practice Research on Promoting Social Support for the Rural Elderly. Master’s Thesis, Yunnan University, Kunming, China, 2017. [Google Scholar]
- Jinan’s GDP Breaks Trillion! Shandong Adds “Promoters”. Available online: http://www.sd.chinanews.com.cn/2/2021/0126/77357.html (accessed on 11 February 2021).
- Administrative Division of Jinan City. Available online: http://www.jinan.gov.cn/col/col24699/index.html (accessed on 11 February 2021).
- Overview of Jinan City. Available online: http://www.jinan.gov.cn/col/col129/index.html (accessed on 11 February 2021).
- Jinan Has a Floating Population of More Than 2.9 Million, So It Is Advisable to Apply for Residence Permit. Available online: https://www.qlwb.com.cn/2019/0419/1419427.shtml (accessed on 11 February 2021).
- Long, C.; Han, J.; Yi, C. Does the Effect of Internet Use on Chinese Citizen’s Psychological Well-Being Differ Base on Their Hukou Category? Int. J. Environ. Res. Public Health 2020, 18, 6680. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wang, D.; Wang, Y. The Relationship between Parents and Mental Health of Chi Shiji Women from the Perspective of Social Support—Based on the Investigation in Qinba Mountain Area. J. Northwest Univ. (Philos. Soc. Sci.). 2021, 51, 76–84. [Google Scholar]
- Kim, Y.; Schneider, T.; Faß, E.; Lochbaum, M. Personal social capital and self-rated health among middle-aged and older adults: A cross-sectional study exploring the roles of leisure-time physical activity and socioeconomic status. BMC Public Health 2021, 21, 48. [Google Scholar] [CrossRef]
- Seo, J.; Choi, B.; Kim, S.; Lee, H.; Oh, D. The relationship between multiple chronic diseases and depressive symptoms among middle-aged and elderly populations: Results of a 2009 korean community health survey of 156,747 participants. BMC Public Health 2017, 17, 844. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Li, Z.; Luo, G.; Li, A.; Chen, P.; Huang, L. The prevalence of common chronic diseases and its correlation with body mass index in the elderly in Xuyong County. Chin. Prim. Health Care 2020, 34, 52–55. [Google Scholar]
- Kearns, K.; Dee, A.; Fitzgerald, A.P.; Doherty, E.; Perry, I.J. Chronic disease burden associated with overweight and obesity in Ireland: The effects of a small BMI reduction at population level. BMC Public Health 2014, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.; Bahk, J.; Yun, S.; Khang, Y. Income gaps in self-rated poor health and its association with life expectancy in 245 districts of Korea. Epidemiol. Health 2017, 39, e2017011. [Google Scholar] [CrossRef][Green Version]
- Song, F.; Kang, S. Dilemma and Path of Reconstruction of Old Communities under the Background of Population Aging. Hebei Acad. J. 2020, 40, 191–197. [Google Scholar]
- Zhang, X. Research on Aging Adaptation of Urban Old Community Based on the Behavioral and Psychological Characteristics of the Old. Master’s Thesis, Taiyuan University of Technology, Taiyuan, China, 2017. [Google Scholar]
- Chan, Y.; The, C.; Lim, K.; Lim, K.; Yeo, P.; Kee, C.; Omar, M.; Ahmad, N. Lifestyle, chronic diseases and self-rated health among Malaysian adults: Results from the 2011 National Health and Morbidity Survey (NHMS). BMC Public Health 2015, 15, 754. [Google Scholar] [CrossRef]
- Jiang, J.; Gao, X. Self-rated health status and its influencing factors of the elderly in rural Taizhou. J. Med. Soc. 2019, 32, 111–114. [Google Scholar]
- Chen, L.; Yao, Y. The effect of social support on the mental health of the elderly. Popul. Res. 2005, 4, 73–78. [Google Scholar]
- Wu, Y.; Han, X.; Qian, D.; Zhao, J. Quality of life of elderly chronic disease patients in rural areas of Jiangsu Province. J. Med. Soc. 2020, 33, 76–80. [Google Scholar]
- Zhou, M.; Sun, X.; Huang, L. Chronic disease and medical spending of Chinese elderly in rural region. Int. J. Qual. Health Care 2021, 33. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.E. Social Support and Health-Related Quality of Life Among Elderly Individuals Living Alone in South Korea: A Cross-Sectional Study. J. Nurs. Res. 2018, 26, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sangthong, R.; Ingviya, T.; Wan, C. Nothing Like Living with a Family: A Qualitative Study of Subjective Well-Being and its Determinants among Migrant and Local Elderly in Dongguan, China. Int. J. Environ. Res. Public Health 2019, 16, 4874. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Yeatts, D.E. Social support and life satisfaction among older adults in China: Family-based support versus community-based support. Int. J. Aging Hum. Dev. 2013, 77, 189–209. [Google Scholar] [CrossRef]
- Cheah, Y.K. An exploratory study on self-rated health status: The case of Penang, Malaysia. Malays. J. Econ. Stud. 2012, 49, 141–155. [Google Scholar]
- Cao, Z. Research on the Involvement of Group Work in the Social Communication Dilemma of the Elderly Migrant. Master’s Thesis, Nanjing Agricultural University, Nanjing, China, 2015. [Google Scholar]
- Li, M. The Emotional Needs and Social Support of the Elderly; China Population: Beijing, China, 2020. [Google Scholar]
- Ning, X.; Lai, Y.; Wu, C.; Huang, Z.; Mo, H.; Li, C.; Sun, Q. Physical health status and influencing factors of 60 to 69 years old people in Guangxi. Modern Prev. Med. 2020, 47, 2030–2034. [Google Scholar]
- Wang, Y. The Reconstruction of Old Residential Areas Should Focus on Solving the “Pain Points” of People’s Livelihood. Econ. Daily 2020, 03, 01. [Google Scholar]
- Wang, Z.; Zhang, Z.; Ma, Y.; Wan, Q. The mediating effect of income level on health literacy and self-rated health. Chin. J. Dis. Control Prev. 2020, 24, 1185–1189. [Google Scholar]


{kind=link}
| Variables | Total n(%) | Self-Rated Health Status | χ2/Kendall | p | |
|---|---|---|---|---|---|
| Good n(%) | Average or below n(%) | ||||
| Observations | 656(100) | 498(75.9) | 158(24.1) | ||
| Sex | 4.917 a | 0.027 | |||
| Female | 418(63.7) | 329(78.7) | 89(21.3) | ||
| Male | 238(36.3) | 169(71.0) | 69(29.0) | ||
| Age (years) | 0.032 b | 0.363 | |||
| 60–62 | 126(19.2) | 94(74.6) | 32(25.4) | ||
| 63–65 | 197(30.0) | 145(73.6) | 52(26.4) | ||
| 66–68 | 183(27.9) | 142(77.6) | 41(22.4) | ||
| 69–71 | 87(13.3) | 68(78.2) | 19(21.8) | ||
| 72–79 | 49(7.5) | 42(85.7) | 7(14.3) | ||
| 80– | 14(2.1) | 7(50) | 7(50) | ||
| BMI | 0.082 b | 0.019 | |||
| ≥28 | 74(11.3) | 67(90.5) | 7(9.5) | ||
| 24–27.9 | 300(45.7) | 225(75) | 75(25) | ||
| 18.5–23.9 | 259(39.5) | 188(72.6) | 71(27.4) | ||
| ≤18.4 | 23(3.5) | 18(78.3) | 5(21.7) | ||
| Monthly income | −0.109 b | 0.003 | |||
| CNY 0–100 (USD 0–15.5) | 152(23.2) | 121(79.6) | 31(20.4) | ||
| CNY 101–1000 (USD 15.6–154.5) | 194(29.6) | 159(82.0) | 35(18.0) | ||
| CNY 1001–2000 (USD 154.7–309.2) | 107(16.3) | 80(74.8) | 27(25.2) | ||
| CNY ≥2001 (≥USD 309.2) | 203(30.9) | 138(68.0) | 65(32.0) | ||
| Education | −0.045 b | 0.205 | |||
| Middle school and below | 340(51.8) | 268(78.8) | 72(21.2) | ||
| High school | 192(29.3) | 138(71.9) | 54(28.1) | ||
| Above high school | 124(18.9) | 92(74.2) | 32(25.8) | ||
| Employment | 10.892 a | 0.004 | |||
| Unemployed | 488(74.4) | 384(78.7) | 104(21.3) | ||
| Employed | 37(5.6) | 29(78.4) | 8(21.6) | ||
| Retired | 131(20.0) | 85(64.9) | 46(35.1) | ||
| Migration years | 786.244 b | 0.000 | |||
| 5 years and below | 355(54.1) | 266(74.9) | 89(25.1) | ||
| Above 5 years | 301(45.9) | 232(77.1) | 69(22.9) | ||
| Migration type | 0.281 a | 0.596 | |||
| Rural to urban | 556(84.8) | 420(75.5) | 136(24.5) | ||
| Urban to urban | 100(15.2) | 78(78) | 22(22) | ||
| Presence of an elevator | 103.577 a | 0.000 | |||
| Yes | 467(71.2) | 405(86.7) | 62(13.3) | ||
| No | 189(28.8) | 93(49.2) | 96(50.8) | ||
| Assessment of living condition | 36.761 a | 0.012 | |||
| Good | 523(79.7) | 403(77.1) | 120(22.9) | ||
| Poor | 133(20.3) | 95(71.4) | 38(28.6) | ||
| Variables | Total n(%) | Self-Rated Health Status | χ2/Kendall | p | |
|---|---|---|---|---|---|
| Good n(%) | Average or below n(%) | ||||
| Observations | 656 | 498(75.9) | 158(24.1) | ||
| Close friends | 26.354 a | 0.001 | |||
| None | 91(13.9) | 70(76.9) | 21(23.1) | ||
| 1–2 | 195(29.7) | 139(71.3) | 56(28.7) | ||
| 3–5 | 177(27.0) | 137(77.4) | 40(22.6) | ||
| 6–9 | 95(14.5) | 74(77.9) | 21(22.1) | ||
| ≥10 | 98(14.9) | 78(79.6) | 20(20.4) | ||
| One-year living style | 6.920 b | 0.040 | |||
| Alone | 6(0.9) | 2(33.3) | 4(66.7) | ||
| With strangers | 2(0.3) | 1(50) | 1(50) | ||
| With friends | 3(0.5) | 2(66.7) | 1(33.3) | ||
| With family | 645(98.3) | 493(76.4) | 152(23.6) | ||
| Relationship with neighbors | −0.100 a | 0.001 | |||
| Nodding acquaintance | 91(13.9) | 67(73.6) | 24(26.4) | ||
| Care a little | 116(17.7) | 81(69.8) | 35(30.2) | ||
| Some care | 155(23.6) | 113(72.9) | 42(27.1) | ||
| Most concern | 294(44.8) | 237(80.6) | 57(19.3) | ||
| Relationship with friends | −0.095 a | 0.003 | |||
| Nodding acquaintance | 67(10.2) | 48(71.6) | 19(28.4) | ||
| Care a little | 123(18.8) | 88(71.5) | 35(28.5) | ||
| Some care | 169(25.7) | 122(72.2) | 47(27.8) | ||
| Most concern | 297(45.3) | 240(80.8) | 57(19.2) | ||
| Couple support | 0.026 a | 0.456 | |||
| None | 60(9.1) | 45(75) | 15(25) | ||
| Few | 15(2.3) | 10(66.7) | 5(33.3) | ||
| General | 33(5.1) | 28(84.8) | 5(15.2) | ||
| Full | 548(83.5) | 415(75.7) | 133(24.3) | ||
| Parents support | 20.296 a | 0.161 | |||
| None | 540(82.3) | 410(75.9) | 130(24.1) | ||
| Few | 9(1.4) | 8(88.9) | 1(11.1) | ||
| General | 22(3.4) | 18(81.8) | 4(18.2) | ||
| Full | 85(12.9) | 62(72.9) | 23(27.1) | ||
| Children support | −0.048 a | 0.167 | |||
| None | 6(0.9) | 2(33.3) | 4(66.7) | ||
| Few | 19(2.9) | 15(78.9) | 4(21.1) | ||
| General | 44(6.7) | 31(70.5) | 13(29.5) | ||
| Full | 587(89.5) | 450(76.7) | 137(23.3) | ||
| Sibling support | −0.025 a | 0.445 | |||
| None | 93(14.2) | 70(75.3) | 23(24.7) | ||
| Few | 51(7.8) | 37(72.5) | 14(27.5) | ||
| General | 159(24.2) | 122(76.7) | 37(23.3) | ||
| Full | 353(53.8) | 269(76.2) | 84(23.8) | ||
| Other members support | −0.053 a | 0.099 | |||
| None | 158(24.1) | 116(73.4) | 42(26.6) | ||
| Few | 81(12.3) | 66(81.5) | 15(18.5) | ||
| General | 178(27.1) | 135(75.8) | 43(24.2) | ||
| Full | 239(36.4) | 181(75.7) | 58(24.3) | ||
| Crisis economic support | 3.370 b | 0.643 | |||
| Spouse | 22.522 b | 0.000 | |||
| Yes | 540(82.3) | 410(75.9) | 130(24.1) | ||
| No | 116(17.7) | 88(75.9) | 28(24.1%) | ||
| Other members | 9.135 b | 0.104 | |||
| Yes | 604(92.1) | 463(76.7) | 141(23.3) | ||
| No | 52(7.9) | 35(67.3) | 17(32.7) | ||
| Relative | 21.507 b | 0.001 | |||
| Yes | 351(53.5) | 264(75.2) | 87(24.8) | ||
| No | 305(46.5) | 234(76.7) | 71(23.3) | ||
| Crisis comfort support | |||||
| Spouse | 13.084 b | 0.023 | |||
| Yes | 543(82.8) | 410(75.5) | 133(24.5) | ||
| No | 113(17.2) | 88(77.9) | 25(22.1) | ||
| Other members | 7.991 b | 0.157 | |||
| Yes | 603(91.9) | 460(76.3) | 143(23.7) | ||
| No | 53(8.1) | 38(71.7) | 15(28.3) | ||
| Relative | 25.720 b | 0.000 | |||
| Yes | 344(52.4) | 255(74.1) | 89(25.9) | ||
| No | 312(47.6) | 243(77.9) | 69(22.1) | ||
| Ways to talk about troubles | 15.968 b | 0.384 | |||
| Never talk to anyone | 127(19.3) | 99(78) | 28(22) | ||
| Only tell close people | 174(26.5) | 122(70.1) | 52(29.9) | ||
| If friends ask | 120(18.4) | 91(75.8) | 29(24.2) | ||
| Take the initiative | 235(35.8) | 186(79.1) | 49(20.9) | ||
| How to ask for help | 0.020 a | 0.531 | |||
| Alone | 128(19.5) | 100(78.1) | 28(21.9) | ||
| Rarely ask for help | 132(20.1) | 104(78.8) | 28(21.2) | ||
| Sometimes ask for help | 123(18.8) | 89(72.4) | 34(27.6) | ||
| Often ask for help | 273(41.6) | 205(75.1) | 68(24.9) | ||
| Group activities | 17.571 a | 0.075 | |||
| Never attend | 474(72.3) | 360(75.9) | 114(24.1) | ||
| Sometimes attend | 118(17.9) | 86(72.9) | 32(27.1) | ||
| Often attend | 34(5.2) | 29(85.3) | 5(14.7) | ||
| Actively participate | 30(4.6) | 23(76.7) | 7(23.3) | ||
| SSRS | −0.080 a | 0.005 | |||
| ≤22 | 4(0.6) | 3(75) | 1(25) | ||
| ≥23 and ≤44 | 503(76.7) | 376(74.8) | 127(25.2) | ||
| ≥45 and ≤66 | 149(22.7) | 119(79.9) | 30(20.1) | ||
| Variables | Total n(%) | Self-Rated Health Status | χ2/Kendall | p | |
|---|---|---|---|---|---|
| Good n(%) | Average or below n(%) | ||||
| Observations | 656 | 498(75.9) | 158(24.1) | ||
| Total chronic diseases | 1.829 a | 0.836 | |||
| 0 | 383(58.4) | 290(75.7) | 93(24.3) | ||
| 1 | 187(28.5) | 142(75.9) | 45(24.1) | ||
| 2 | 56(8.5) | 42(75.0) | 14(25.0) | ||
| 3 | 18(2.7) | 13(72.2) | 5(27.8) | ||
| 4 | 9(1.4) | 8(88.9) | 1(11.1) | ||
| 5 | 3(0.5) | 3(100) | 0 | ||
| Heart disease | 0.008 b | 0.031 | |||
| Yes | 24(3.7) | 21(87.5) | 3(12.5) | ||
| No | 632(96.3) | 477(75.5) | 155(24.5) | ||
| Stroke | 11.238 b | 0.000 | |||
| Yes | 48(7.3) | 46(95.8) | 2(4.2) | ||
| No | 608(92.7) | 452(74.3) | 156(25.7) | ||
| Headache | 2.470 b | 0.081 | |||
| Yes | 32(4.9) | 28(87.5) | 4(12.5) | ||
| No | 624(95.1) | 470(75.3) | 154(24.7) | ||
| Back pain | 3.473 b | 0.038 | |||
| Yes | 82(12.5) | 69(84.1) | 13(15.9) | ||
| No | 574(87.5) | 429(74.7) | 145(25.3) | ||
| Leg pain | 3.355 b | 0.041 | |||
| Yes | 110(16.8) | 91(82.7) | 19(17.3) | ||
| No | 546(83.2) | 407(74.5) | 139(25.5) | ||
| Duration of chronic disease | 12.784 b | 0.012 | |||
| ≤5 years | 387(59.0) | 294(75.9) | 93(24.1) | ||
| 6–10 years | 66(10.1) | 54(81.8) | 12(18.2) | ||
| 11–19 years | 31(4.7) | 29(93.5) | 2(6.5) | ||
| ≥20 years | 172(26.2) | 121(70.3) | 51(29.7) | ||
| Degree of pain discomfort | −0.046 a | 0.207 | |||
| No pain | 536(81.7) | 403(75.2) | 133(24.8) | ||
| Have pain | 120(18.3) | 95(79.2) | 25(20.8) | ||
| Outpatient service attendance | 9.900 b | 0.002 | |||
| Yes | 166(25.3) | 141(84.9) | 25(15.1) | ||
| No | 490(74.7) | 357(72.9) | 133(27.1) | ||
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | OR | 95%CI | p | |
| Sex | |||||||||
| Female | 1.0 | 1.0 | 1.0 | ||||||
| Male | 1.426 | 0.936–2.174 | 0.099 | 0.793 | 0.507–1.241 | 0.310 | 0.760 | 0.474–1.219 | 0.255 |
| BMI | |||||||||
| ≥28 | 1.0 | 1.0 | 1.0 | ||||||
| 24–27.9 | 0.777 | 0.197–3.073 | 0.719 | 0.734 | 0.179–3.008 | 0.668 | 0.721 | 0.153–3.396 | 0.679 |
| 18.5–23.9 | 0.307 | 0.127–0.741 | 0.009 | 0.304 | 0.122–0.761 | 0.011 | 0.248 | 0.093–0.661 | 0.005 |
| ≤18.4 | 0.371 | 0.154–0.892 | 0.027 | 0.344 | 0.138–0.858 | 0.022 | 0.279 | 0.105–0.739 | 0.010 |
| Monthly income | |||||||||
| CNY 0–100 (USD 0–15.5) | 1.0 | 1.0 | 1.0 | ||||||
| CNY 101–1000 (USD 15.6–154.5) | 1.145 | 0.626–2.095 | 0.661 | 1.212 | 0.643–2.285 | 0.552 | 1.299 | 0.666–2.533 | 0.433 |
| CNY 1001–2000 (USD 154.7–309.2) | 1.827 | 1.036–3.221 | 0.037 | 1.786 | 0.981–3.251 | 0.058 | 1.954 | 1.049–3.641 | 0.035 |
| CNY ≥ 2001 (≥ USD 309.2) | 1.260 | 0.682–2.327 | 0.460 | 1.151 | 0.592–2.229 | 0.677 | 1.191 | 0.593–2.393 | 0.623 |
| Employment | |||||||||
| Unemployed | 1.0 | 1.0 | 1.0 | ||||||
| Employed | 1.587 | 0.631–3.991 | 0.326 | 1.481 | 0.561–3.910 | 0.428 | 1.359 | 0.494–3.742 | 0.553 |
| Retired | 0.768 | 0.446–1.321 | 0.340 | 0.769 | 0.432–1.367 | 0.371 | 0.868 | 0.473–1.592 | 0.647 |
| Migration years | |||||||||
| 5 years and below | 1.0 | 1.0 | 1.0 | ||||||
| Above 5 years | 0.730 | 0.483–1.104 | 0.136 | 0.817 | 0.526–1.269 | 0.368 | 0.792 | 0.496–1.266 | 0.330 |
| Presence of an elevator | |||||||||
| Yes | 1.0 | 1.0 | 1.0 | ||||||
| No | 7.023 | 4.614–10.690 | 0.000 | 18.296 | 9.836–34.033 | 0.000 | 20.982 | 10.772–40.869 | 0.000 |
| Assessment of living condition | |||||||||
| Good | 1.0 | 1.0 | 1.0 | ||||||
| Poor | 1.084 | 0.513–2.290 | 0.832 | 1.218 | 0.563–2.636 | 0.616 | 1.242 | 0.556–2.772 | 0.597 |
| Heart disease | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 0.181 | 0.035–0.942 | 0.042 | 0.164 | 0.032–0.849 | 0.031 | |||
| Stroke | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 0.187 | 0.042–0.833 | 0.028 | 0.236 | 0.045–1.252 | 0.040 | |||
| Headache | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 1.553 | 0.475–5.079 | 0.467 | 1.170 | 0.271–5.051 | 0.834 | |||
| Back pain | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 1.314 | 0.633–2.730 | 0.464 | 1.064 | 0.441–2.570 | 0.890 | |||
| Leg pain | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 1.399 | 0.759–2.581 | 0.282 | 0.991 | 0.468–2.097 | 0.980 | |||
| Duration of chronic disease | |||||||||
| No chronic disease | 1.0 | 1.0 | |||||||
| ≤5 years | 6.879 | 3.448–13.726 | 0.000 | 7.259 | 3.544–14.866 | 0.000 | |||
| 6–10 years | 4.459 | 1.903–10.445 | 0.001 | 5.320 | 2.129–13.297 | 0.000 | |||
| 11–19 years | 4.124 | 1.593–10.673 | 0.004 | 4.420 | 1.653–11.820 | 0.003 | |||
| ≥20 years | 35.185 | 6.511–190.137 | 0.000 | 39.055 | 6.789–224.660 | 0.000 | |||
| Outpatient service attendance | |||||||||
| Yes | 1.0 | 1.0 | |||||||
| No | 0.503 | 0.288–0.877 | 0.015 | 0.467 | 0.257–0.847 | 0.012 | |||
| Close friends | |||||||||
| None | 1.0 | ||||||||
| 1–2 | 0.535 | 0.207–1.380 | 0.196 | ||||||
| 3–5 | 0.806 | 0.382–1.703 | 0.573 | ||||||
| 6–9 | 0.717 | 0.335–1.537 | 0.393 | ||||||
| ≥10 | 0.542 | 0.229–1.281 | 0.163 | ||||||
| One-year living style | |||||||||
| Alone | 1.0 | ||||||||
| With strangers | 0.279 | 0.001–128.209 | 0.683 | ||||||
| With friends | 0.673 | 0.038–11.893 | 0.787 | ||||||
| With family | 0.033 | 0.002–0.449 | 0.010 | ||||||
| Relationship with neighbors | |||||||||
| Nodding acquaintance | 1.0 | ||||||||
| Care a little | 1.165 | 0.373–3.636 | 0.792 | ||||||
| Some care | 0.813 | 0.263–2.517 | 0.720 | ||||||
| Most concern | 0.751 | 0.275–2.056 | 0.578 | ||||||
| Relationship with friends | |||||||||
| Nodding acquaintance | 1.0 | ||||||||
| Care a little | 0.756 | 0.223–2.571 | 0.655 | ||||||
| Some care | 1.007 | 0.330–3.073 | 0.990 | ||||||
| Most concern | 0.705 | 0.270–1.841 | 0.476 | ||||||
| Spouse economic support | |||||||||
| Yes | 1.0 | ||||||||
| No | 0.765 | 0.223–2.629 | 0.671 | ||||||
| Relative economic support | |||||||||
| Yes | 1.0 | ||||||||
| No | 0.406 | 0.155–1.065 | 0.067 | ||||||
| Spouse comfort support | |||||||||
| Yes | 1.0 | ||||||||
| No | 1.352 | 0.383–4.777 | 0.640 | ||||||
| Relative comfort support | |||||||||
| Yes | 1.0 | ||||||||
| No | 2.399 | 0.921–6.250 | 0.073 | ||||||
| SSRS | |||||||||
| ≤22 | 1.0 | ||||||||
| ≥23 and ≤44 | 3.313 | 0.114–96.541 | 0.486 | ||||||
| ≥45 and ≤66 | 1.317 | 0.684–2.534 | 0.411 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, S.; Kong, F.; Li, S. The Effects of Social Support and Morbidities on Self-Rated Health among Migrant Elderly Following Children to Jinan, China. Healthcare 2021, 9, 686. https://doi.org/10.3390/healthcare9060686
Wei S, Kong F, Li S. The Effects of Social Support and Morbidities on Self-Rated Health among Migrant Elderly Following Children to Jinan, China. Healthcare. 2021; 9(6):686. https://doi.org/10.3390/healthcare9060686
Chicago/Turabian StyleWei, Suqing, Fanlei Kong, and Shixue Li. 2021. "The Effects of Social Support and Morbidities on Self-Rated Health among Migrant Elderly Following Children to Jinan, China" Healthcare 9, no. 6: 686. https://doi.org/10.3390/healthcare9060686
APA StyleWei, S., Kong, F., & Li, S. (2021). The Effects of Social Support and Morbidities on Self-Rated Health among Migrant Elderly Following Children to Jinan, China. Healthcare, 9(6), 686. https://doi.org/10.3390/healthcare9060686