
HIV Infection: Time from Diagnosis to Initiation of Antiretroviral Therapy in Portugal, a Multicentric Study

 , ,
, , 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Quantitative Approach
2.1.1. Participants
2.1.2. Study Procedures
2.1.3. Variables/Indicators
2.1.4. Statistical Analysis
2.2. Qualitative Approach
2.2.1. Sampling Strategy and Participants’ Characteristics
2.2.2. Context, Methods, and Instruments of Data Collection
2.2.3. Data Analysis
2.3. Ethical Issues
3. Results
3.1. Patients on ART in 2017 and 2018
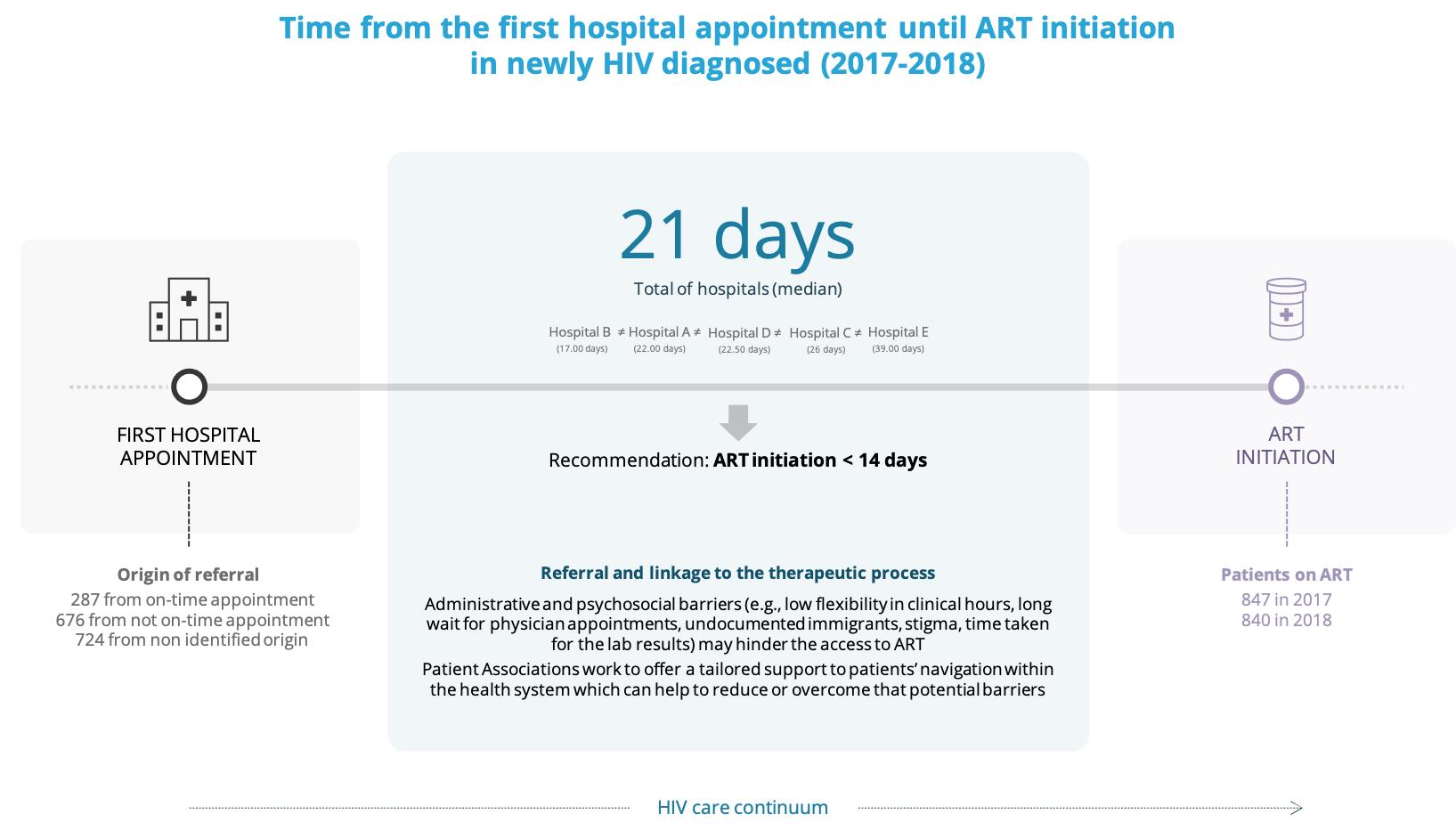
3.2. Time from the First Hospital Appointment to ART Initiation among Newly HIV Diagnosed
3.3. HIV Care Continuum: From a Community-Based Positive HIV Test to ART Initiation
“We have different kind of issues, first geographic disparities, everything changes depending on the geographical area.”(Patient association [PA] 2)
“From community-based testing, referral (to HIV care) has always been done informally, it’s done by email and through physicians with whom we work closely, or via telephone for urgent cases. Now one of our units had begun testing the referral system used by primary health care units, called on time appointment.”(PA3)
“We have a referral protocol, that with some hospitals is agreed informally, and we have a clinical point person, who immediately schedules the appointment.”(PA2)
“We always follow the procedure of delivering the referral form by hand. But when it´s an urgent case we contact the department director via telephone.”(PA1)
“We can follow up and support each person who test positive to HIV in our community services, through referral to the first appointment. we have workers who personally navigate individuals through the hospital setting for the first appointment (…) because our hospitals are not easy to navigate, especially for immigrants (…).”(PA3)
“But the process of navigating facilities for the first medical hospital visit is not easy (…), and this is one of our goals, to guide people through hospital facilities in the beginning of their HIV care pathway (…) and fortunately, for most of them, we aren´t needed anymore.”(PA1)
“As expected, the interim period of one month will cause suffering for some who are waiting for HIV confirmatory results. (…) They may come to believe they will be the exception, (the test proves they aren´t infected with HIV), one month post confirmatory results is too long (…). When needed, our professionals work to engage with and keep close contact with each person along that interim period, to help coping with anxiety.”(PA1)
“Along the implementation of routine HIV testing services, one of our first tasks was to navigate each hospital facilities and routes as an anonymous user. (…) once done became obvious that previous experience was critical before sharing information on accessibility with patients, along with scheduling their first appointment.”(PA2)
“It´s the physician with who we work closely that reports us missed first appointments, and we most often try to reach the person to offer a rescheduling. We look for the reasons for not attending and try to reschedule more accordingly to their availability. (…) Our role is to favor at most health care access and suit it best to each person’s life.”(PA3)
3.3.1. Barriers to a Reduction in the Time between Referral and ART Initiation
“Barriers (…) are easily seen and of importance in the immigrant population.”(PA3)
“In their hierarchy social issues become first than health (…).”(PA1)
(…) Affected populations are different. If we focus on people facing economically deprived situations or facing cognitive impairment deficits, they ask us for support to navigate the system and first-visit escort or transport to the HIV care and treatment facility. But if we talk about primary infections, mainly involving men who have sex with men, who demonstrate better knowledge about the infection, they value more support via telephone, message exchange, social networks.”(PA2)
“(…) We look for the reasons and try to understand, and sometimes is a matter of basic issues, as being unable to afford a bus ticket. To give you an example, a person can wait for more than an hour for the appointment, and some are unable to get that time off work. One of the persons, that we support, reported that he had to leave as he was risking being discharged from work. And for the physician he missed the appointment because he didn´t wait. We can bring the patient perspective to the physician and conciliate to reschedule and benefit from the tolerance between both sides.”(PA2)
3.3.2. Good Practices to Reinforce Care Continuity between HIV Diagnosis and ART Initiation
“(…) And we started working together. I see that as the main reason that led us to accomplish these extraordinary results. The opening of doors in hospitals to work closely with patients’ associations offered an opportunity to listen to each other, brought awareness for some of the barriers faced, and how we could find solutions.”(PA2)
“We try and invest our efforts to guarantee that we give an appointment date for a physician´s visit to each person testing reactive to HIV on the moment of their HIV test. Obviously that´s not a practice reachable with all hospitals. (…) To our knowledge that´s the best practice, even to avoid drop-outs, firming an appointment date after an HIV testing reactive, and assuring readiness to it, as a way of offering some comfort to that person.”(PA2)
“Well, this is an overly sensitive matter, test and treat early, before having some of the lab test results, (…). When we began to offer a post confirmatory test in our community-based testing services, we proposed to one referenced hospital for HIV care, the possibility of having a responsive scheduling that accommodates next-day appointments, making early treatment happen. Because, in fact, this is a recommendation whether from the WHO or from the ECDC (…).”(PA3)
We have a fast-track procedure (…), for suspected cases that are in the so-called acute phase, and we have managed to referral some, not as many as we would like. (…) This has been a reality for a small number of cases (…).”(PA3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hammer, S.M.; Squires, K.E.; Hughes, M.D.; Grimes, J.M.; Demeter, L.M.; Currier, J.S.; Eron, J.J.; Feinberg, J.E.; Balfour, H.H.; Deyton, L.R.; et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. N. Engl. J. Med. 1997, 337, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Palella, F.J.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining morbidity and mortality among patients with advanced human Immunodeficiency Virus Infection. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Andrade, H.B.; Shinotsuka, C.R.; Da Silva, I.R.F.; Donini, C.S.; Li, H.Y.; de Carvalho, F.B.; Alvarenga Americano do Brasil, P.E.; Bozza, F.A.; Japiassu, A.M. Highly active antiretroviral therapy for critically ill HIV patients: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186968. [Google Scholar] [CrossRef]
- Kitahata, M.M.; Gange, S.J.; Abraham, A.G.; Merriman, B.; Saag, M.S.; Justice, A.C.; Hogg, R.S.; Deeks, S.G.; Eron, J.J.; Brooks, J.T.; et al. Effect of early versus deferred antiretroviral therapy for HIV on survival. N. Engl. J. Med. 2009, 360, 1815–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.-C.; Cooper, D.A.; Fätkenheuer, G.; Llibre, J.M.; et al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef] [Green Version]
- Temprano ANRS 12136 Study Group A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N. Engl. J. Med. 2015, 373, 808–822. [CrossRef] [PubMed] [Green Version]
- Samji, H.; Cescon, A.; Hogg, R.S.; Modur, S.P.; Althoff, K.N.; Buchacz, K.; Burchell, A.N.; Cohen, M.; Gebo, K.A.; Gill, M.J.; et al. Closing the gap: Increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS ONE 2013, 8, e81355. [Google Scholar] [CrossRef] [PubMed]
- Lohse, N.; Obel, N. Update of survival for persons with HIV infection in Denmark. Ann. Intern. Med. 2016, 165, 749–750. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.S.; et al. Prevention of HIV-1 infection with early antiretroviral therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Verma, A.; Kashyap, M.; Gautam, P. ART in prevention of mother-to-child transmission of HIV. J. Obstet. Gynecol. India 2020, 70, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Gardner, E.M.; McLees, M.P.; Steiner, J.F.; del Rio, C.; Burman, W.J. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin. Infect. Dis. 2011, 52, 793–800. [Google Scholar] [CrossRef]
- Boyd, M.A.; Boffito, M.; Castagna, A.; Estrada, V. Rapid initiation of antiretroviral therapy at HIV diagnosis: Definition, process, knowledge gaps. HIV Med. 2019, 20, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilcher, C.D.; Ospina-Norvell, C.; Dasgupta, A.; Jones, D.; Hartogensis, W.; Torres, S.; Calderon, F.; Demicco, E.; Geng, E.; Gandhi, M.; et al. The effect of same-day observed initiation of antiretroviral therapy on HIV viral load and treatment outcomes in a US public health setting. J. Acquir. Immune Defic. Syndr. 2017, 74, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Koenig, S.P.; Dorvil, N.; Dévieux, J.G.; Hedt-Gauthier, B.L.; Riviere, C.; Faustin, M.; Lavoile, K.; Perodin, C.; Apollon, A.; Duverger, L.; et al. Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: A randomized unblinded trial. PLoS Med. 2017, 14. [Google Scholar] [CrossRef]
- Ford, N.; Migone, C.; Calmy, A.; Kerschberger, B.; Kanters, S.; Nsanzimana, S.; Mills, E.J.; Meintjes, G.; Vitoria, M.; Doherty, M.; et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS 2018, 32, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Mendez-Lopez, A.; McKee, M.; Stuckler, D.; Granich, R.; Gupta, S.; Noori, T.; Semenza, J.C. Population uptake and effectiveness of test-and-treat antiretroviral therapy guidelines for preventing the global spread of HIV: An ecological cross-national analysis. HIV Med. 2019, 20, 501–512. [Google Scholar] [CrossRef]
- Ford, N.; Vitoria, M.; Doherty, M. Providing antiretroviral therapy to all who are HIV positive: The clinical, public health and programmatic benefits of Treat All. J. Int. AIDS Soc. 2018, 21, e25078. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines for Managing Advanced HIV Disease and Rapid Initiation of Antiretroviral Therapy; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Medland, N.A.; Chow, E.P.F.; McMahon, J.H.; Elliott, J.H.; Hoy, J.F.; Fairley, C.K. Time from HIV diagnosis to commencement of antiretroviral therapy as an indicator to supplement the HIV cascade: Dramatic fall from 2011 to 2015. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Behav. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90: An Ambitious Treatment Target to Help End the AIDS Epidemic; UNAIDS: Geneva, Switzerland, 2014. [Google Scholar]
- Ministério da Saúde. Diário da República n.o 228/2015, 1o Suplemento, Série II de 2015-11-20, Despacho n.o 13447-C/2015; Ministério da Saúde: Lisboa, Portugal, 2015.
- Programa Nacional para a Infeção VIH e SIDA. Infeção VIH e SIDA: Desafios e Estratégias; Ministério da Saúde: Lisboa, Portugal, 2018. [Google Scholar]
- Njuguna, I.N.; Cranmer, L.M.; Otieno, V.O.; Mugo, C.; Okinyi, H.M.; Benki-Nugent, S.; Richardson, B.; Stern, J.; Maleche-Obimbo, E.; Wamalwa, D.C.; et al. Urgent versus post-stabilisation antiretroviral treatment in hospitalised HIV-infected children in Kenya (PUSH): A randomised controlled trial. Lancet HIV 2018, 5, e12–e22. [Google Scholar] [CrossRef]
- Grant, P.M.; Zolopa, A.R. When to start ART in the setting of acute AIDS-related opportunistic infections: The time is now! Curr. HIV/AIDS Rep. 2012, 9, 251–258. [Google Scholar] [CrossRef]
- Zolopa, A.R.; Andersen, J.; Komarow, L.; Sanne, I.; Sanchez, A.; Hogg, E.; Suckow, C.; Powderly, W. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: A multicenter randomized strategy trial. PLoS ONE 2009, 4, e5575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guidelines on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Ministério da Saúde. Diário da República, 1.a série—N.o 44—4 de Março de 2013, Portaria n.o 95/2013 de 4 de Março; Ministério da Saúde: Lisboa, Portugal, 2013.
- Administração Central do Sistema de Saúde Profissionais. Profissionais Utilizadores do CTH: Perguntas Frequentes. 2013. Available online: https://www2.acss.min-saude.pt/Portals/0/CTH%20FAQ%20Profissionais.pdf (accessed on 2 June 2021).
- Diniz, A.; Vieira, A.; Santos, D.; Maltez, F.; Oliveira, J.; Mansinho, K.; Serrão, R.; Sarmento e Castro, R.; Branco, T. Rede Nacional Hospitalar de Referenciação para a Infeção por VIH (RNHR HIV); Ministério da Saúde: Lisboa, Portugal, 2015.
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- World Medical Association WMA. Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects; WMA: Ferney-Voltaire, France, 2013. [Google Scholar]
- D’Arminio Monforte, A.; Tavelli, A.; Cozzi-Lepri, A.; Castagna, A.; Passerini, S.; Francisci, D.; Saracino, A.; Maggiolo, F.; Lapadula, G.; Girardi, E.; et al. Virological response and retention in care according to time of starting ART in Italy: Data from the Icona Foundation Study cohort. J. Antimicrob. Chemother. 2020, 75, 681–689. [Google Scholar] [CrossRef]
- Levy, J.A. Caution: Should we be treating HIV infection early? Lancet 1998, 352, 982–983. [Google Scholar] [CrossRef]
- Grinsztejn, B.; Hosseinipour, M.C.; Ribaudo, H.J.; Swindells, S.; Eron, J.; Chen, Y.Q.; Wang, L.; Ou, S.S.; Anderson, M.; McCauley, M.; et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: Results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect. Dis. 2014, 14, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Fox, J.; White, P.J.; Macdonald, N.; Weber, J.; McClure, M.; Fidler, S.; Ward, H. Reductions in HIV transmission risk behaviour following diagnosis of primary HIV infection: A cohort of high-risk men who have sex with men. HIV Med. 2009, 10, 432–438. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Continuum of HIV Care: Monitoring Implementation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia: 2018 Progress Report; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2018. [Google Scholar]
- Lesko, C.R.; Sampson, L.A.; Miller, W.C.; Clymore, J.; Leone, P.A.; Swygard, H.; Powers, K.A. Measuring the HIV care continuum using public health surveillance data in the United States. J. Acquir. Immune Defic. Syndr. 2015, 70, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Genberg, B.L.; Lee, Y.; Rogers, W.H.; Wilson, I.B. Four types of barriers to adherence of antiretroviral therapy are associated with decreased adherence over time. AIDS Behav. 2015, 19, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Croome, N.; Ahluwalia, M.; Hughes, L.D.; Abas, M. Patient-reported barriers and facilitators to antiretroviral adherence in sub-Saharan Africa. AIDS 2017, 31, 995–1007. [Google Scholar] [CrossRef] [Green Version]
- Wasti, S.P.; Simkhada, P.; Randall, J.; Freeman, J.V.; van Teijlingen, E. Barriers to and facilitators of antiretroviral therapy adherence in Nepal: A qualitative study. J. Health Popul. Nutr. 2012, 30, 410–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kebaabetswe, P.; Manyake, K.; Kadima, E.; Auletta-Young, C.; Chakalisa, U.; Sekoto, T.; Dintwa, O.M.; Mmalane, M.; Makhema, J.; Lebelonyane, R.; et al. Barriers and facilitators to linkage to care and ART initiation in the setting of high ART coverage in Botswana. AIDS Care 2020, 32, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Moges, N.A.; Adesina, O.A.; Okunlola, M.A.; Berhane, Y. Barriers and facilitators of same-day antiretroviral therapy initiation among people newly diagnosed with hiv in Ethiopia: Qualitative study using the transtheoretical model of behavioral change. J. Multidiscip. Healthc. 2020, 13, 1801–1815. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Dimension | Sub-Dimension |
|---|---|
| 1. Referral and health system navigation | Detailing the experience and practice of navigation between a positive HIV test and ART initiation in Portugal. Identifying procedures variability and time intervals between care referral, linkage to care, and ART initiation |
| 2. Access to referral services and access to care | Exploring the main facilitators, challenges, and barriers to accessing referral services, starting medical care, and ART initiation |
| 3. Good practices | Collecting good practice examples at national and international levels with possible impacts on the path between referral, diagnosis, and ART initiation |
| Total n | Hospital A n (%) | Hospital B n (%) | Hospital C n (%) | Hospital D n (%) | Hospital E n (%) | |
|---|---|---|---|---|---|---|
| Gender | - | - | ||||
| Male | 804 | 614 (77.2) | 139 (77.7) | 51 (61.4) | ||
| Female | 253 | 181 (22.8) | 40 (22.3) | 32 (38.6) | ||
| Age c | - | - | ||||
| <15 years | 12 | 11 (1.4) | 1 (0.6) | 0 (0.0) | ||
| 15–19 years | 8 | 4 (0.5) | 3 (1.7) | 1 (1.2) | ||
| 20–29 years | 261 | 202 (25.4) | 48 (26.8) | 11 (13.3) | ||
| 30–39 years | 315 | 249 (31.3) | 45 (25.1) | 21 (25.3) | ||
| 40–49 years | 248 | 198 (24.9) | 26 (14.5) | 24 (28.9) | ||
| 50–59 years | 137 | 87 (10.9) | 34 (19.0) | 16 (19.3) | ||
| >59 years | 76 | 44 (5.5) | 22 (12.3) | 10 (12.0) | ||
| Mean (± SD) | 39 (±12.98) | 38 (±12.41) | - | 41 (±15.00) | - | 44 (±12.29) |
| Minimum | 1 | 1 | 1 | 19 | ||
| Maximum | 83 | 83 | 83 | 79 | ||
| Origin of referral | ||||||
| On-time appointment | 287 | 121 (15.2) | 67 (11.1) | 92 (51.4) | 0 (0.0) | 7 (24.1) |
| Not on-time appointment d | 676 | 402 (50.6) | 84 (14.0) | 85 (47.5) | 83 (100.0) | 22 (75.9) |
| Not available | 724 | 272 (34.2) | 450 (74.9) | 2 (1.1) | 0 (0.0) | 0 (0.0) |
| Total n (%) | Hospital A n (%) | Hospital B n (%) | Hospital C n (%) | Hospital D n (%) | Hospital E n (%) | |
|---|---|---|---|---|---|---|
| 2017 | 847 (50.2) | 410 (51.6) | 290 (48.3) | 92 (51.4) | 42 (50.6) | 13 (44.8) |
| 2018 | 840 (49.8) | 385 (48.4) | 311 (51.7) | 87 (48.6) | 41 (49.4) | 16 (55.2) |
| Total N = 1687 | Hospital A n = 795 | Hospital B n = 601 | Hospital C a n = 179 | Hospital D n = 83 | Hospital E n = 29 | |
|---|---|---|---|---|---|---|
| Mean (95%CI) | 60.60 (52.51–68.69) | 83.96 (69.47–98.44) | 35.45 (28.36–42.54) | 71.06 (60.06–82.05 | 29.82 (20.12–39.53) | 71.96 (36.02–107.91) |
| Quartile 25 | 0.00 | 0.00 | 0.00 | 0.00 | 14.00 | 28.00 |
| Median | 21.00 | 22.00 | 17.00 | 26.00 | 22.50 | 39.00 |
| Quartile 75 | 40.00 | 49.00 | 34.00 | 46.25 | 30.00 | 82.50 |
| IQR | 40 | 49 | 34 | 46 | 16 | 55 |
| % of HIV patients with ART initiation < 14 days | 38.0% b | 36.6% | 43.9% | 5.7% | 15.7% | 17.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolau, V.; Cortes, R.; Lopes, M.; Virgolino, A.; Santos, O.; Martins, A.; Faria, N.; Reis, A.P.; Santos, C.; Maltez, F.; et al. HIV Infection: Time from Diagnosis to Initiation of Antiretroviral Therapy in Portugal, a Multicentric Study. Healthcare 2021, 9, 797. https://doi.org/10.3390/healthcare9070797
Nicolau V, Cortes R, Lopes M, Virgolino A, Santos O, Martins A, Faria N, Reis AP, Santos C, Maltez F, et al. HIV Infection: Time from Diagnosis to Initiation of Antiretroviral Therapy in Portugal, a Multicentric Study. Healthcare. 2021; 9(7):797. https://doi.org/10.3390/healthcare9070797
Chicago/Turabian StyleNicolau, Vanessa, Rui Cortes, Maria Lopes, Ana Virgolino, Osvaldo Santos, António Martins, Nancy Faria, Ana Paula Reis, Catarina Santos, Fernando Maltez, and et al. 2021. "HIV Infection: Time from Diagnosis to Initiation of Antiretroviral Therapy in Portugal, a Multicentric Study" Healthcare 9, no. 7: 797. https://doi.org/10.3390/healthcare9070797