1. Introduction
Hospital readmissions have received substantial worldwide attention in recent years. According to a report, over 17% of patients were readmitted within 30 days of discharge [
1]. Hospital readmissions are often costly, representing USD 25 billion per year [
2]. However, approximately 75% of all readmissions can be prevented by appropriate post-discharge monitoring and management [
3]. A high readmission rate imposes a heavy financial burden on patients but is also regarded as a symbol of poor quality of medical services [
4,
5,
6].
To reduce readmissions and curb rising medical costs, there have been many payment systems, such as capitation, pay-for-performance, per diem prospective payment, and diagnostic-related groups, aiming at replacing the traditional fee-for-service (FFS) that has long been criticized for rewarding healthcare providers who spend more unnecessarily [
7,
8]. In 2013, the Centers for Medicare and Medicaid Services (CMS) initiated a new payment program called Bundled Payments for Care Improvement (BPCI) [
9]. BPCI requires hospital to define bundles of healthcare services associated with a specified disease. For example, bundles for joint replacement include advance payments, details of healthcare services during the episode, and plans for post-discharge monitoring [
10,
11]. Under the bundled payment (BP) system, the hospital will receive a lump sum for a whole episode of care, including index admissions and readmissions that occur over a specified warranty period, such as 90 days after discharge, regardless of the treatment details and the possible related complications [
12]. Here, BP is a reimbursement scheme with the implication of healthcare warranty, and the 90 days after discharge can be regarded as the warranty period. In addition to BP, there are other forms of payment such as ProvenCare and PROMETHEUS, which can be described as healthcare warranties [
13]. Under the healthcare warranty, if the actual healthcare costs are lower than the lump sum, the hospital will profit; otherwise, the hospital will suffer a financial loss [
14]. Therefore, the transformation of the payment mechanism from the traditional FFS to healthcare warranty has shifted the financial risk from the patient to the healthcare provider. Some scholars hold that healthcare warranty payments contribute to a higher quality of healthcare and keep treatment costs under control because patients would no longer pay for hospital readmissions when they occur [
9,
15]. Thus, providing a high level of treatment services to the patient during index admission may increase the profit margins by reducing the probability of readmissions under healthcare warranty payments [
16]. The healthcare warranty reimbursement scheme is currently applied to joint replacement surgery, cardiovascular care, cancer care, and treatment of chronic diseases such as diabetes and chronic obstructive pulmonary disease [
15,
17,
18,
19,
20,
21]. The practice has proven that healthcare warranties can be greatly beneficial for reducing costs, improving patient satisfaction, and enhancing the competitiveness of medical institutions. Numerous efforts have been made to improve healthcare performance, from strategic to operational levels. Strategic decisions involve capital investment, resource planning of healthcare services, etc. [
22,
23]. Healthcare operations management focuses on the decision making related to the execution of healthcare delivery processes, including healthcare resources scheduling, process optimization and control, disease management, etc. [
24,
25,
26]. Disease management comprises disease prediction and diagnosis, risk assessment, healthcare service strategy optimization, and disease monitoring [
27,
28,
29,
30]. In addition, research on healthcare cost control and management support systems in recent years has also created value in healthcare. For example, time-driven activity-based costing has been applied in healthcare and can help to efficiently modify cost processes and thereby contribute to cost control and efficiency improvement in healthcare delivery [
31]. Another example is a healthcare management system with blockchain-based electronic healthcare records against the background of data security and inefficiently management [
32]. This study is intended to provide an effective medical service decision-making model to enrich disease management research.
Jacobs et al. [
33] showed that many types of patients’ post-discharge care processes and readmission characteristics are similar. For example, when a cystectomy patient is discharged from hospital, a disease-monitoring plan consisting of periodic follow-up is made. After the patient is discharged, they will receive scheduled follow-up checkups, such as a timely general inspection, comprehensive inspection, phone call, and office visit. The purpose of follow-up is to detect whether the patient has developed illnesses or complications prior to patient readmission. Once a condition is detected by follow-up, measures such as drug interventions can prevent further development. Moreover, early intervention and prevention programs may save total treatment costs and improve service quality simultaneously. Previous literature shows that undertaking a series of disease-monitoring plans can significantly reduce readmission rates [
14,
34]. Based on our field research, the patient’s condition goes through several states of progression before readmission. As time passes, the patient may develop a readmission-causing condition (called an “illness” in this article). When the illness first develops, it will not trigger immediate readmission. However, if nothing is done to address this illness, the patient’s condition will worsen and eventually lead to readmission. We call the time lapse between a detectable illness and readmission the delay time. In this study, we developed an optimization model based on a delay time model from the reliability and machine maintenance literature to capture disease-monitoring dynamics. The delay-time model is widely applied to model engineering problems in machine maintenance and inspection; it assumes that a device’s life cycle has an increasing failure rate [
35,
36,
37]. The period that starts with the device showing signs of failure, and ending with the final failure, is called the delay time. In medical operations management, the delay-time model has been used to model disease progression. Fu et al. [
38] proposed a two-stage delayed diagnosis regression model for hepatitis screening based on a delay time model. Zhang et al. [
39] applied a delay time model to optimize postoperative monitoring plans for vascular surgery by minimizing the probability of failing to detect patency loss before readmission. Helm et al. [
40] developed mixed integer programming based on a delay time model to determine optimal follow-up schedules and allocate necessary resources. Liu et al. [
2] developed a delay time model to analyze the impact of quantity, effectiveness to detect conditions and a mix of different checkup methods on the optimal decision making of follow-up schedules.
Providing disease monitoring for patients implies additional costs for the hospital under the healthcare warranty, and these costs result from labor costs for medical staff, medical devices, and drugs during a predetermined warranty period. However, these interventions may lower the lump sum of healthcare warranties by reducing readmissions rates. The episodes of care can be divided into two consecutive periods: the hospitalization phase and the post-discharge phase. Healthcare providers need to develop a healthcare warranty policy that includes treatment decisions for the first phase and monitoring plans for the second phase. Treatment decisions affect the baseline readmission rate after discharge, and the follow-up monitoring strategy will also affect the readmission rate. Although a high number of treatment decisions incur higher medical costs, providing a high number of treatment options may reduce overall costs by reducing baseline readmission rates. Therefore, for cost control and profitability, joint optimization of hospital treatment decisions and monitoring strategies is of great significance for reducing patient readmissions and controlling the healthcare costs for a medical institution.
Previous studies and medical practices have demonstrated the potential of a healthcare warranty in terms of cost saving and quality improvement [
9,
14,
15]. However, some questions need to be further explored, which are also the motivation for this study. First, existing studies on disease-monitoring policies have aimed at maximizing the probability of detecting the patients’ health conditions but failed to consider the costs associated with follow-up and treatment. Sujan et al. [
41] pointed out that it is necessary for hospitals to establish a mechanism for managing explicitly the trade-off between risk reduction and cost. Second, the extant research does not use appropriate models to simulate the effect of disease monitoring on the patients’ readmission rates. The purpose of disease monitoring is to reduce the readmission rates by follow-up checkups of patients to detect the illness early and take intervention measures to remove it. Consequently, after an illness intervention, the progress of the disease is expected to be halted, and the readmission risk of the patient is expected to be reduced compared to that before the follow-up interventions, which may in turn influence the decisions made about a disease-monitoring policy. In addition, although healthcare warranties are beneficial for cost savings and medical quality assurance, the method behind designing effective healthcare warranty policies is poorly understood. Currently implemented healthcare warranty policies have been obtained empirically and subjectively without supporting quantitative analysis.
Our study is relevant to the research on developing the optimal follow-up policies based on the delay time model as mentioned above [
2,
39,
40]. Given that a patient develops a readmission-causing condition after discharge, the delay time defines a time window during which a follow-up checkup can prevent readmission. Existing research uses the delay time model to characterize the dynamics of readmission and further derives the optimal follow-up schedule to maximize the probability of detecting the readmission-causing condition. Our research extended these modeling approaches in several aspects. First, we considered the impact of inpatient treatment decisions on baseline readmission risk and optimized treatment decisions and follow-up monitoring strategies simultaneously. Second, we measured the effect of follow-up intervention on the patient’s readmission risk. Both extensions made the model construction and computational complexity more challenging. The main contributions are as follows. We proposed a systematic optimization model of a healthcare warranty policy that allows healthcare providers to determine the optimal combination of treatment decisions and disease-monitoring policies to minimize the total expected healthcare warranty cost over the prespecified period. To the best of our knowledge, there has been a lack of research on the development of healthcare warranty policies in the healthcare operations and management. We used elaborate mathematical formulas to characterize the relationship between the treatment intensity and baseline readmission rates, and we utilized the delay time model to analyze and optimize the disease-monitoring strategy. The effect of a follow-up intervention on the patient’s readmission risk was measured by the accumulative age method. In addition, a healthcare warranty policy optimization model was constructed to determine the optimal combination of the treatment decisions and the timing of follow-up checkups during the warranty period. A case study of pediatric type 1 diabetes mellitus is presented to illustrate the applicability of the proposed model. The proposed model framework and practical implications can provide a basis for the healthcare provider to formulate healthcare warranty policies, further contributing to improving the quality of healthcare and control the costs. Furthermore, the application of the delay time model and accumulative age method provide a reference for disease modeling and management.
2. Problem Definition
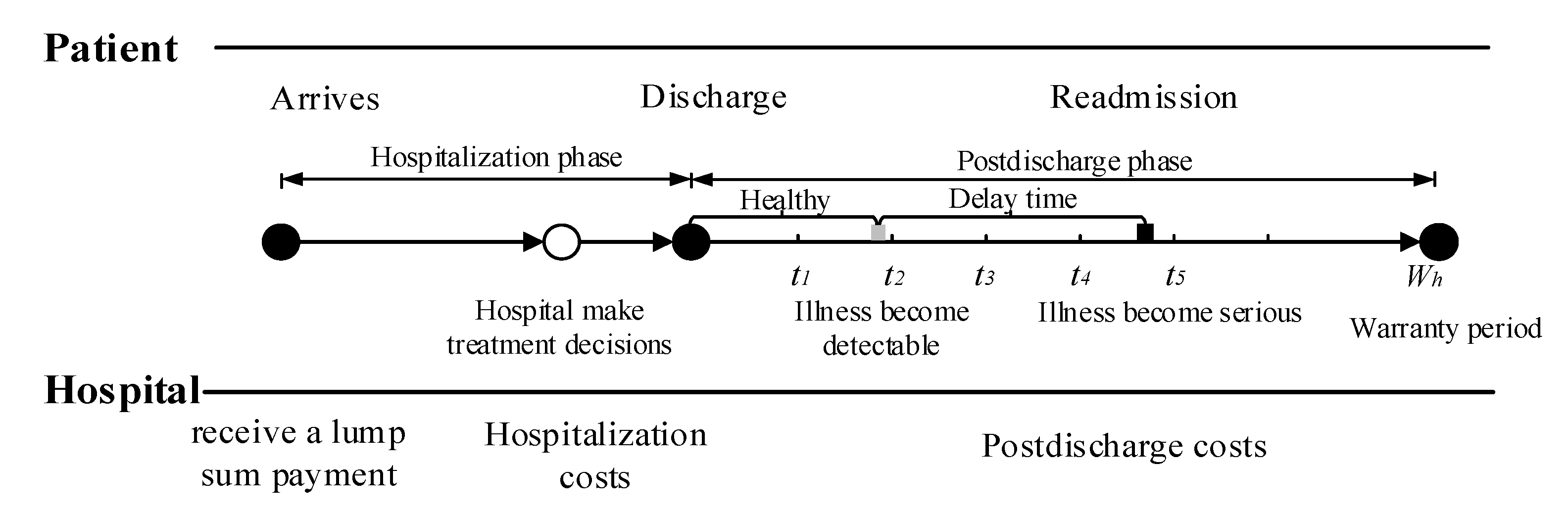
Consider a healthcare delivery system with two parties, namely, a hospital and its cohort of patients. Under the healthcare warranty scheme, the length of care episodes (i.e., warranty period) is prespecified. Once a patient enters the hospital, the hospital receives a lump sum payment to cover all services during the entire care episode. These medical services include treatment options during hospitalization, disease monitoring, and possible readmission treatment after discharge.
Figure 1 illustrates the sequence of events. In medical practice, patients are often considered to be homogeneous under healthcare warranties. This consensus is reasonable, since patients are classified into heterogeneous diagnosis-related groups (DRGs) based on their individual characteristics. Patients in the same group have similar physical and disease conditions; that is, they are homogeneous [
42,
43]. When a patient is entered into a healthcare delivery system, the hospital chooses treatment intensity
to maximize their expected profit [
14]. The variable
refers to the level of treatment services provided by the hospital for patients, such as the professional level of doctors, the professional competence of the nursing staff, the length of stay (LOS), and the precision of the medical devices. The associated costs incurred by hospitals during hospitalization increase with the treatment intensity
. After a patient is discharged, disease-monitoring plans consisting of periodic follow-up activities are necessary to reduce hospital readmission rates and control healthcare costs. During the post-discharge phase, the patient’s condition undergoes several states of progression before readmission. In this study, we used a delay time model to capture the progression of disease. For example, diabetic patients usually have polydipsia and polyuria before being readmitted to the hospital. Under the condition that the patient is monitored after discharge from the hospital, if any readmission-causing conditions are detected by follow-up, intervention measures can be taken immediately to mitigate illness deterioration. The purpose of disease monitoring is to detect developing conditions before they deteriorate, reducing unnecessary readmissions.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}