
Infection Spread, Recovery, and Fatality from Coronavirus in Different Provinces of Saudi Arabia

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Collection and Recording of Data:
2.3. Analysis of Data
2.3.1. Pattern of Spread of COVID-19 in Different Provinces
2.3.2. Percentage of Confirmed Cases Detected
2.3.3. Infection Rate in Population of Different Provinces
2.3.4. Rate of Recovery from COVID-19 in Different Provinces
2.3.5. Mortality Rate from COVID-19 in Different Provinces
2.3.6. Case-Fatality Rate (CFR) in Different Provinces
2.3.7. Total Pattern of Spread of COVID-19 in Different Provinces
2.4. Representation of Data
2.5. Statistics
3. Results
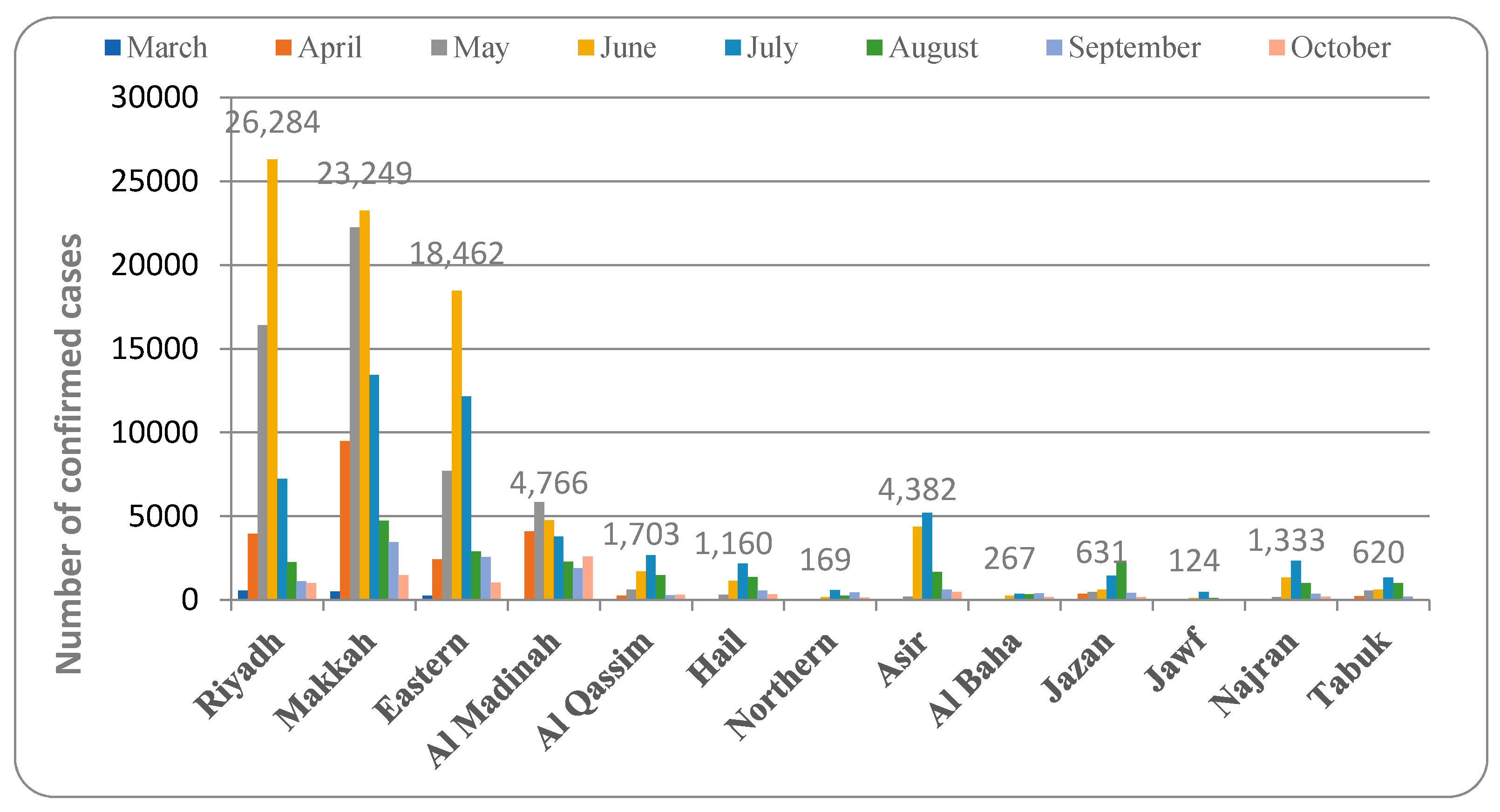
3.1. Pattern of Spread of COVID-19 in Different Provinces of Saudi Arabia
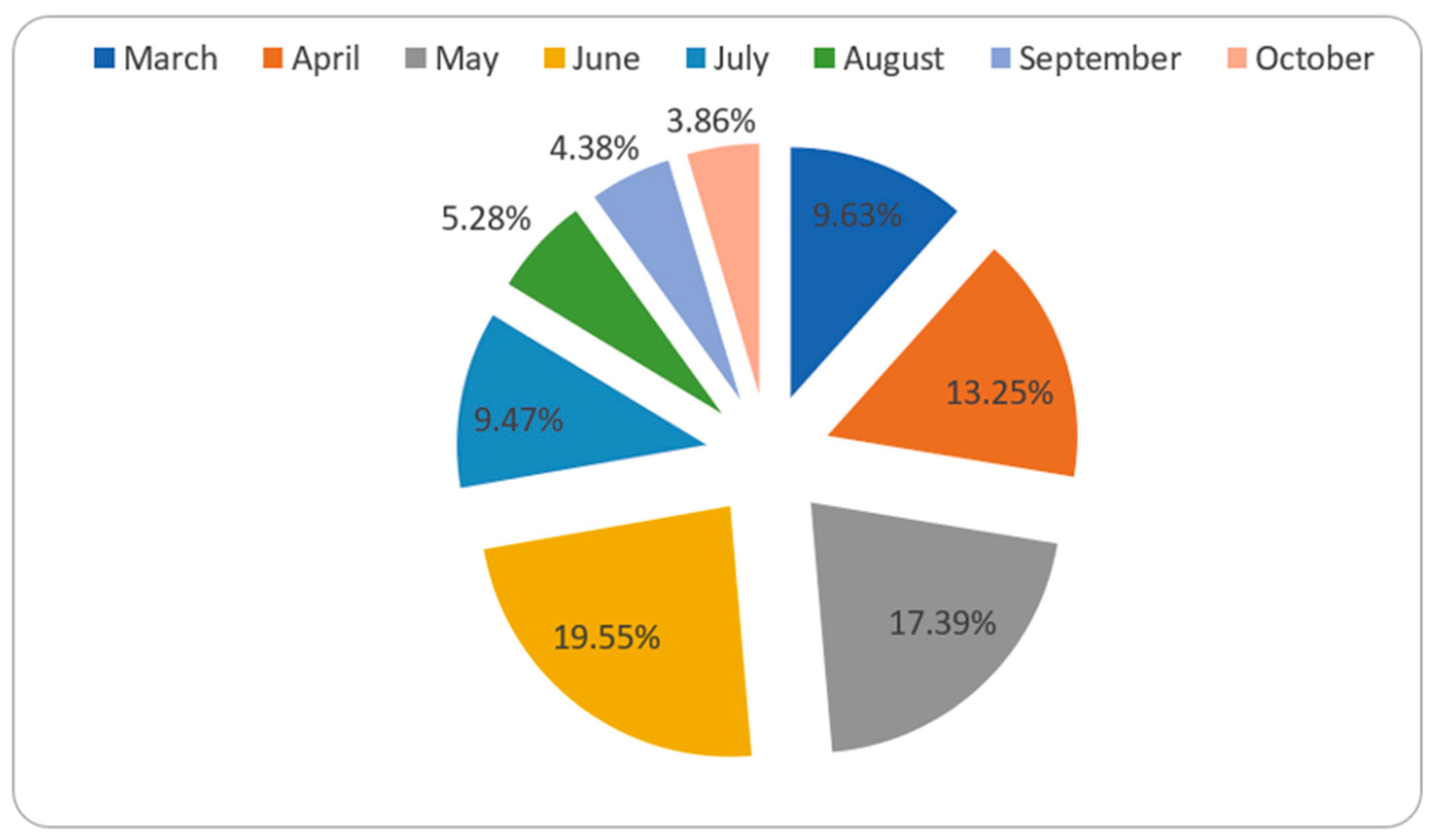
3.2. Percentage of Confirmed COVID-19 Cases Detected
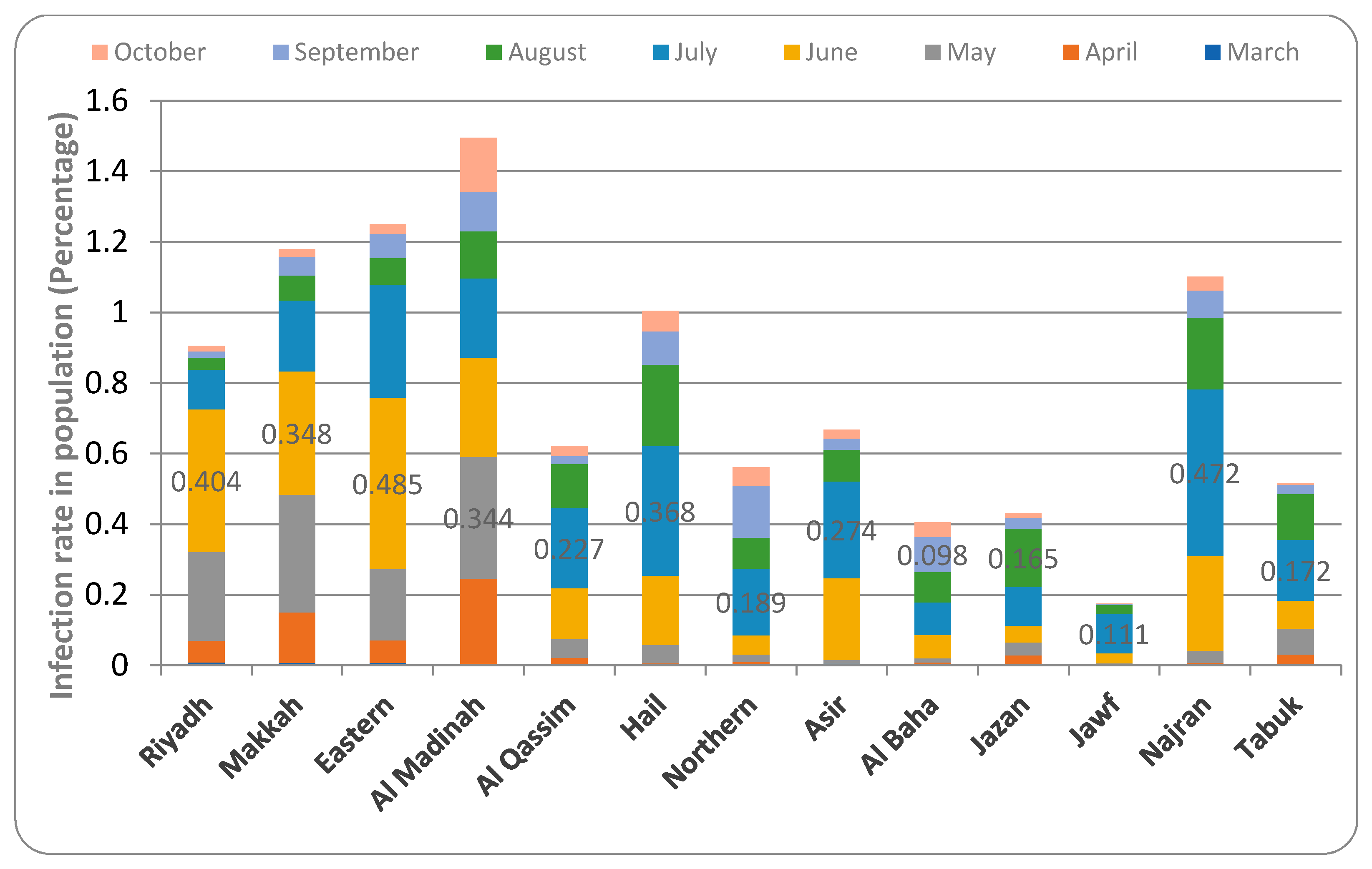
3.3. Infection Rate in Population of Different Provinces of Saudi Arabia
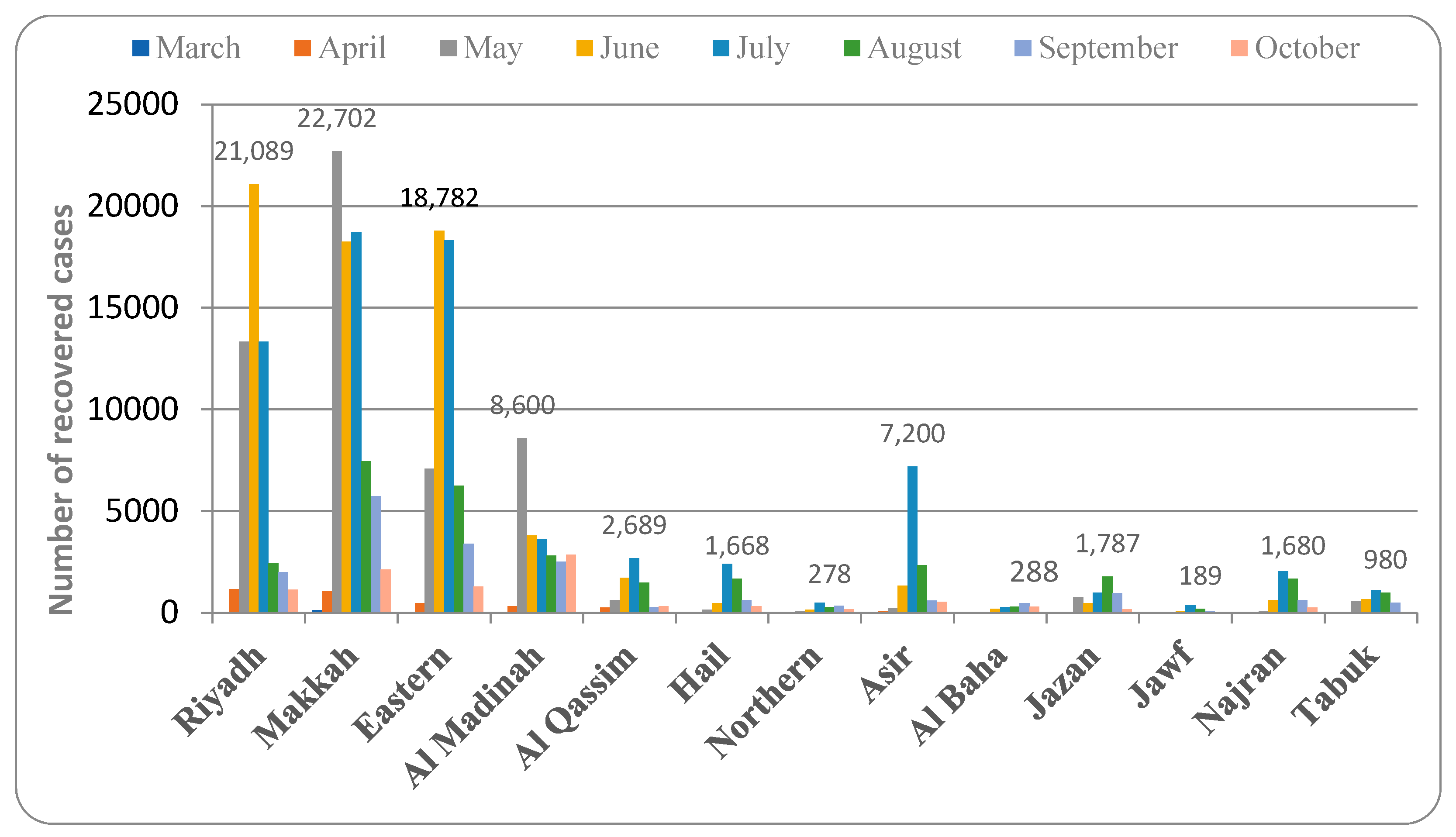
3.4. Rate of Recovery from COVID-19 in Different Provinces of Saudi Arabia
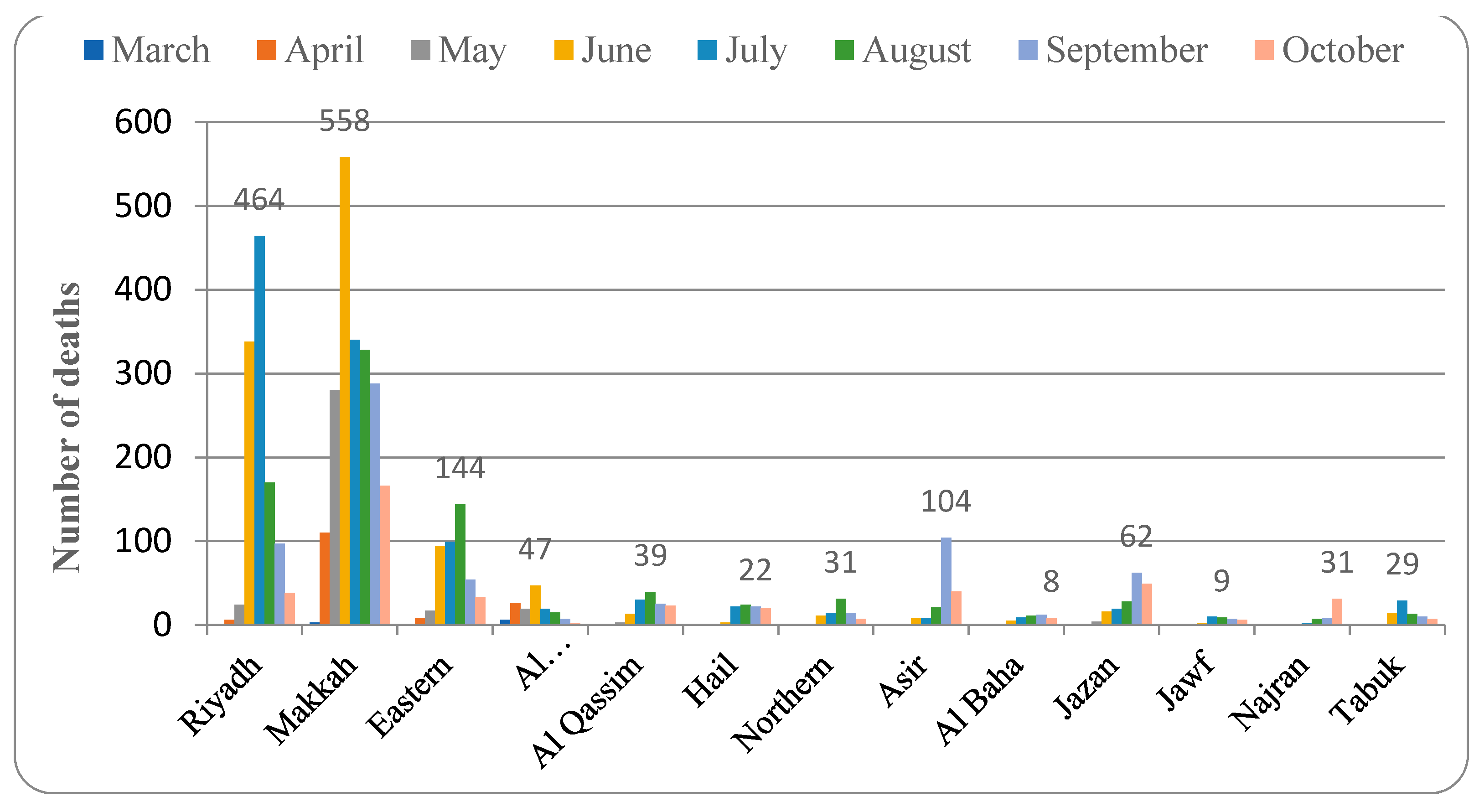
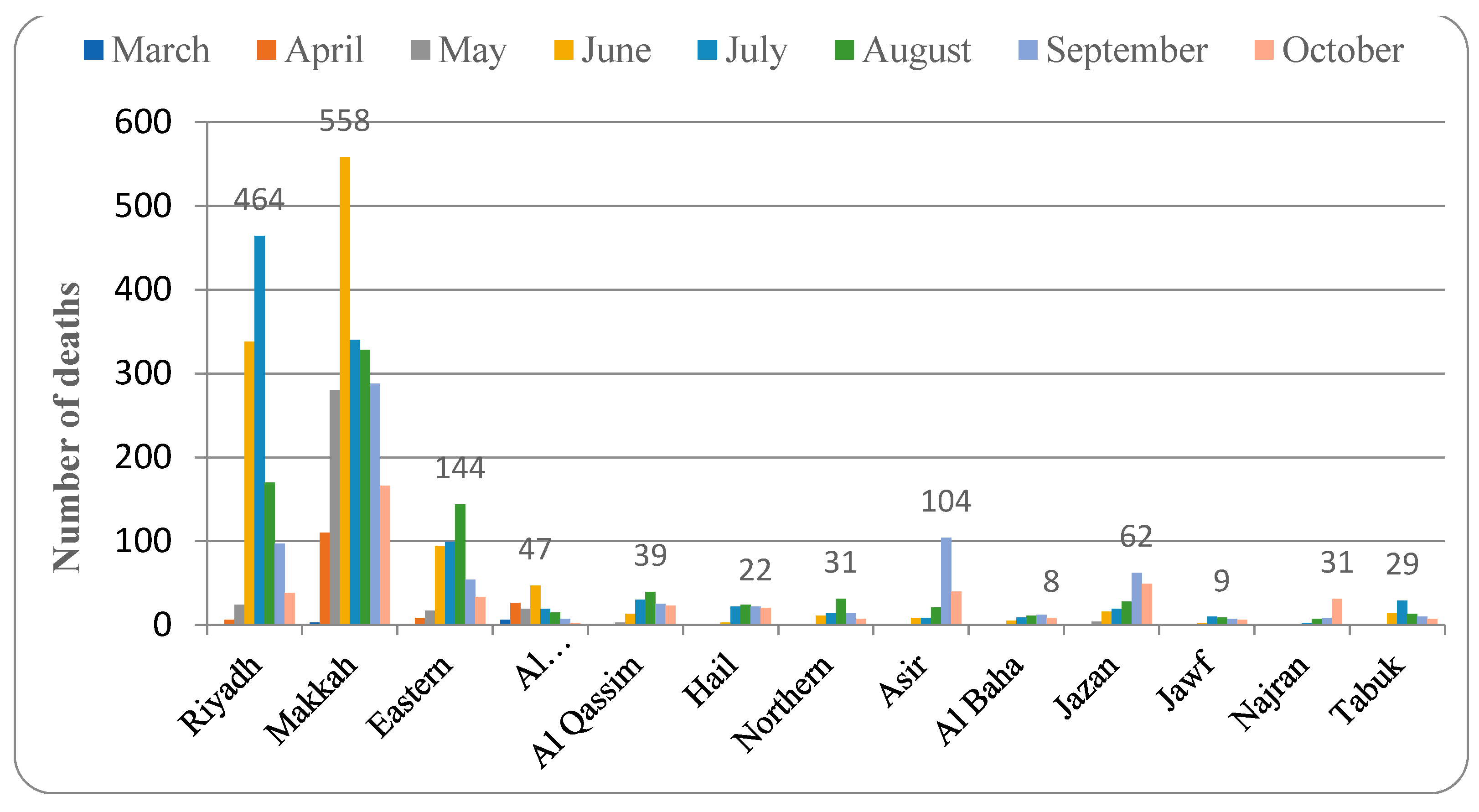
3.5. Mortality Rate from COVID-19 in Different Provinces of Saudi Arabia
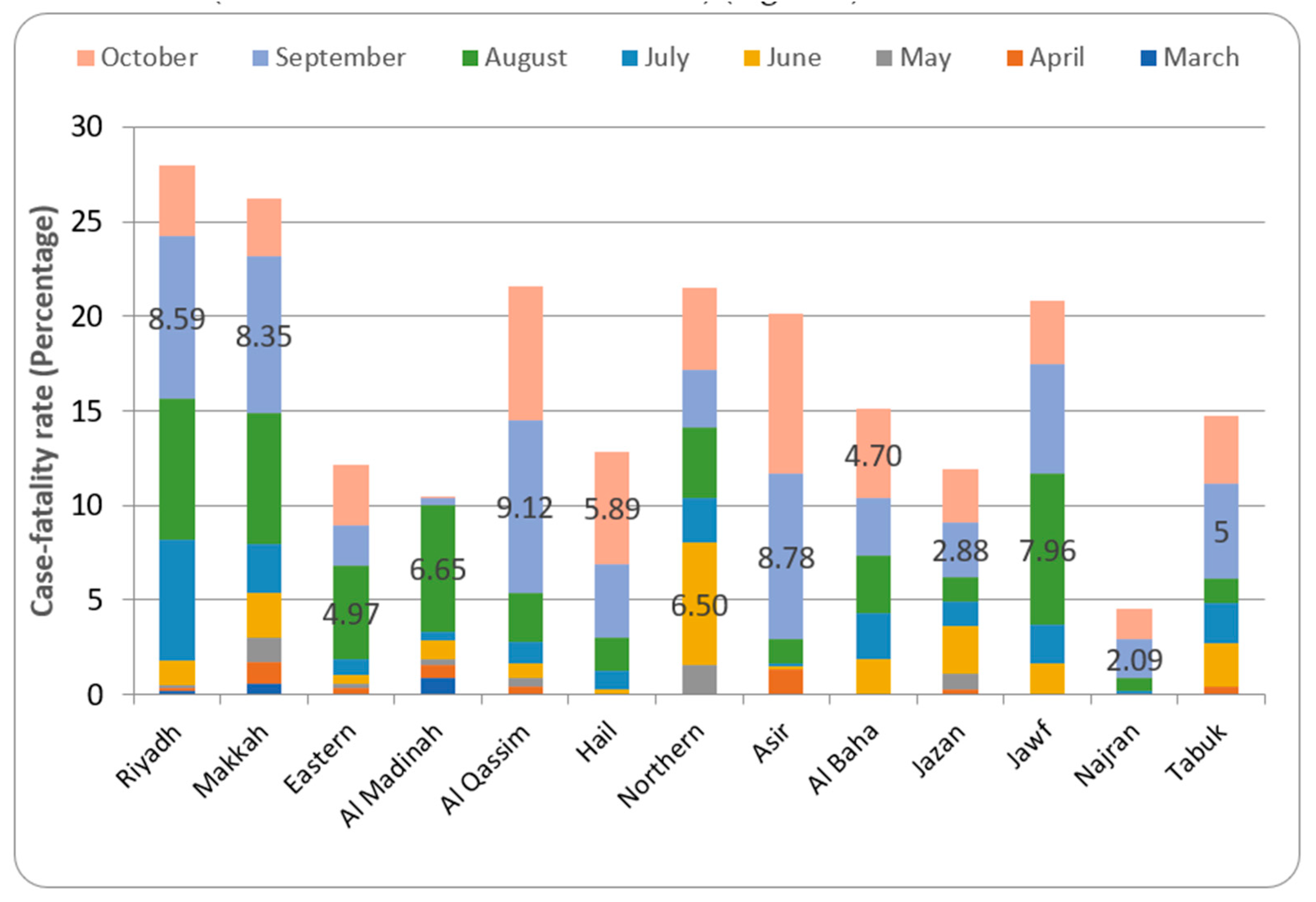
3.6. Case-Fatality Ratio in Different Provinces of Saudi Arabia
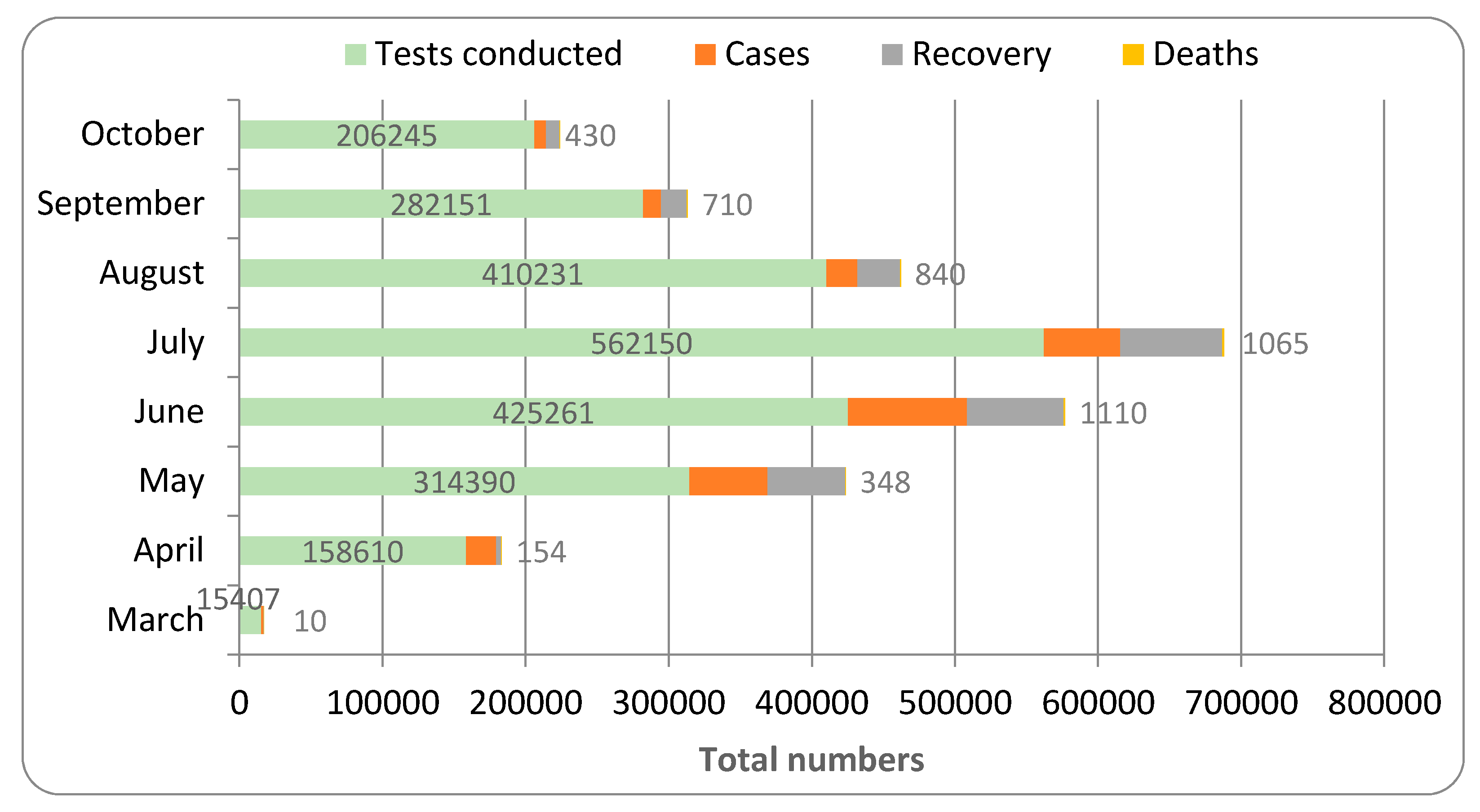
3.7. Total Pattern of Spread in All the Provinces
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rothan, H.; Byrareddy, S. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Hughes, J.M.; Wilson, S.; Luby, E.; Gurley, M. Hossain Transmission of human infection with Nipah virus. Clin. Infect. Dis. 2009, 49, 1743–1748. [Google Scholar]
- Linton, N.; Kobayashi, T.; Yang, Y.; Hayashi, K.; Akhmetzhanov, A.; Jung, S.; Yuam, B.; Kinoshita, R.; Nishiura, H. Incubation Period and Other Epidemiological Characteristics of 2019 Novel Coronavirus Infections with Right Truncation: A Statistical Analysis of Publicly Available Case Data. J. Clin. Med. 2020, 9, 538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, P.; McAuley, D.; Brown, M.; Sanchez, E.; Tattersall, R.; Manson, J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Liu, B.; Forman, M.; Valsamakis, A. Optimization and evaluation of a novel real-time RT-PCR test for detection of parechovirus in cerebrospinal fluid. J. Virol. Methods 2019, 272, 1136–1190. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lew, T. Acute Respiratory Distress Syndrome in Critically Ill Patients With Severe Acute Respiratory Syndrome. JAMA 2003, 290, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, J.; Monogue, M.; Jodlowski, T.; Cutrell, J. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19). JAMA 2020, 18, 1824–1837. [Google Scholar] [CrossRef] [PubMed]
- Alkhowailed, M.; Shariq, A.; Alqossayir, F.; Alzahrani, O.A.; Rasheed, Z.; Al Abdulmonem, W. Impact of meteorological parameters on COVID-19 pandemic: A comprehensive study from Saudi Arabia. Inform. Med. Unlocked 2020, 20, 100418. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Memish, Z.A. COVID-19 in the Eastern Mediterranean Region and Saudi Arabia: Prevention and therapeutic strategies. Int. J. Antimicrob. Agents 2020, 55, 105968. [Google Scholar] [CrossRef] [PubMed]
- Yaro, C.A.; Kogi, E.; Opara, K.N.; Batiha, G.E.; Baty, R.S.; Albrakati, A.; Altalbawy, F.M.A.; Innocent Etuh, U.; Oni, J.P. Infection pattern, case fatality rate and spread of Lassa virus in Nigeria. BMC Infect. Dis. 2021, 21, 149. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z. Clinical course and risk factorsfor mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality ratio and characteristic of patients dying in relation to Covid-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [PubMed]
- Grubaugh, N.; Hanage, W.; Rasmussen, A. Making Sense of Mutation: What D614G Means for the COVID-19 Pandemic Remains Unclear. Cell 2020, 182, 794–795. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, A.A.; Khan, A.A.; Elganainy, A.; Almohammadi, E.L.; Hakawi, M.; Assiri, A.M.; Jokhdar, H.A. Epidemiological and clinical features of COVID-19 patients in Saudi Arabia. J. Infect. Public Health 2021, 14, 437–443. [Google Scholar] [CrossRef]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.H.; Naser, A.Y.; Orabi, M.A.A.; Alwafi, H.; Alyami, H.S. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: An Ecological Study. Front. Public Health 2020, 8, 506. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, A.; Khavarian-Garmsir, A.R. The COVID-19 pandemic: Impacts on cities and major lessons for urban planning, design, and management. Sci. Total Environ. 2020, 749, 142391. [Google Scholar] [CrossRef] [PubMed]
- Rahal, L.; Bouchedoub, Y. Role of nutrition in immune response: Case of COVID-19. Nutr. Santé. 2020, 14, 18–27. [Google Scholar] [CrossRef]
- Song, P.; Karako, T. COVID-19: Real-time dissemination of scientific information to fight a public health emergency of international concern. Biosci. Trends 2020, 14, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, M.; Wang, M.; Zhang, J.; Ye, J.; Xu, Y.; Wang, Z.; Ye, D.; Liu, J.; Wan, J. Advances in the relationship between coronavirus infection and cardiovascular diseases. Biomed. Pharmacother. 2020, 127, 1102–1130. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alharbi, M.M.; Rabbani, S.I.; Asdaq, S.M.B.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; Bamogaddam, R.F.; Alajlan, S.A.; et al. Infection Spread, Recovery, and Fatality from Coronavirus in Different Provinces of Saudi Arabia. Healthcare 2021, 9, 931. https://doi.org/10.3390/healthcare9080931
Alharbi MM, Rabbani SI, Asdaq SMB, Alamri AS, Alsanie WF, Alhomrani M, Mohzari Y, Alrashed A, Bamogaddam RF, Alajlan SA, et al. Infection Spread, Recovery, and Fatality from Coronavirus in Different Provinces of Saudi Arabia. Healthcare. 2021; 9(8):931. https://doi.org/10.3390/healthcare9080931
Chicago/Turabian StyleAlharbi, Mohammed Muberek, Syed Imam Rabbani, Syed Mohammed Basheeruddin Asdaq, Abdulhakeem S. Alamri, Walaa F. Alsanie, Majid Alhomrani, Yahya Mohzari, Ahmed Alrashed, Reem Faisal Bamogaddam, Saleh Ahmad Alajlan, and et al. 2021. "Infection Spread, Recovery, and Fatality from Coronavirus in Different Provinces of Saudi Arabia" Healthcare 9, no. 8: 931. https://doi.org/10.3390/healthcare9080931
APA StyleAlharbi, M. M., Rabbani, S. I., Asdaq, S. M. B., Alamri, A. S., Alsanie, W. F., Alhomrani, M., Mohzari, Y., Alrashed, A., Bamogaddam, R. F., Alajlan, S. A., Alharbi, M. A., Aldhawyan, N. N., & Najmi, S. A. (2021). Infection Spread, Recovery, and Fatality from Coronavirus in Different Provinces of Saudi Arabia. Healthcare, 9(8), 931. https://doi.org/10.3390/healthcare9080931