
A Nationwide Mystery Caller Evaluation of Oral Emergency Contraception Practices from German Community Pharmacies: An Observational Study Protocol

 ,
,
Abstract
:1. Introduction
- -
- Primary objective: to investigate information gathering based on the BAK checklist, a possible recommendation as well as availability and pricing for oral EC.
- -
- Secondary objective: to determine to what extent the study results differ with regard to possible influencing factors.
2. Materials and Methods
2.1. Study Design
- -
- by a person (mystery caller (MC)),
- -
- who contacts a CP,
- -
- with the help of a call,
- -
- to simulate a lifelike conversation situation based on a predefined scenario.
- -
- the data collection according to predefined criteria using an assessment form and
- -
- the data management and analysis.
- -
- the CP contacted is given performance feedback, if applicable.
2.2. Mystery Caller
2.3. Setting and Participation
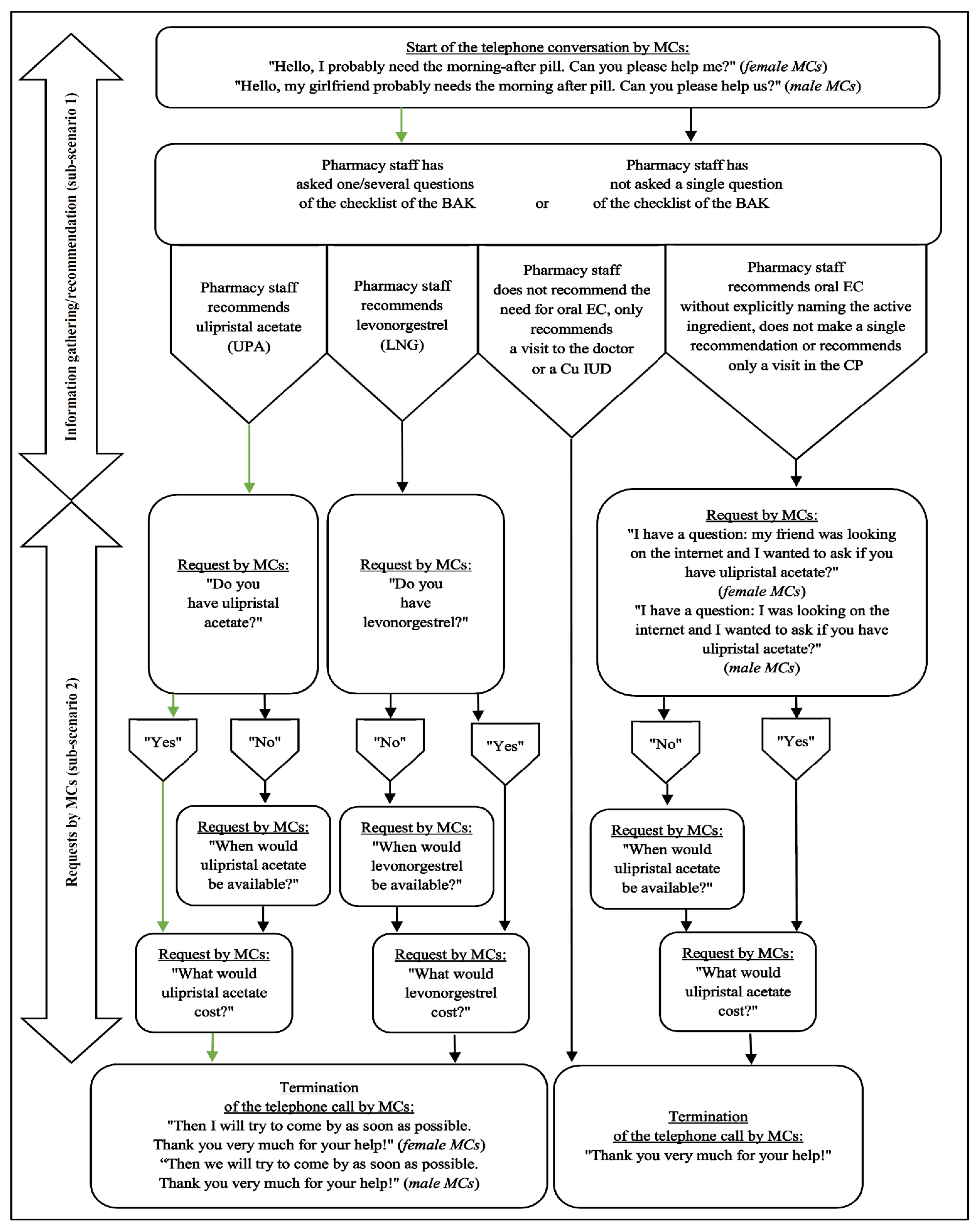
2.4. Scenario
2.5. Assessment
- -
- the MC number (item 22) [81],
- -
- the gender of the MC (item 23) [82],
- -
- the gender of the pharmacy staff (item 24) [83], which is usually identifiable by the voice during the call,
- -
- a possible quality certificate of the CP (item 25) [84], which should be determined by the MC on the same day of the call on the internet—if documented there—and which—if not yet determined—should be asked for on the basis of a further call after all calls have been completed
- -
- as well as the length of the telephone call (item 26) [85] by using a clock accurate to the second.
2.6. Data Collection
2.7. Data Management and Analysis
2.8. Performance Feedback
2.9. Ethics and Dissemination
3. Discussion
Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO—World Health Organization. Emergency Contraception. Available online: https://www.who.int/news-room/fact-sheets/detail/emergency-contraception (accessed on 22 February 2021).
- Rabe, T.; Goeckenjan, M.; Ahrendt, H.-J.; Ludwig, M.; Merkle, E.; König, K.; Merki Feld, G.; Albring, C. Postkoitale Kontrazeption. Gemeinsame Stellungnahme der Deutschen Gesellschaft für Gynäkologische Endokrinologie und Fortpflanzungsmedizin (DGGEF) e.V. und des Berufsverbands der Frauenärzte (BVF) e.V. J. Reproduktionsmed. Endokrinol. 2011, 8, 390–414. [Google Scholar]
- Rabe, T.; Albring, C.; Ahrendt, H.-J.; Mueck, A.O.; Merkle, E.; König, K.; Merki, G. Notfallkontrazeption—ein Update. Gynäkologische Endokrinol. 2013, 11, 197–202. [Google Scholar] [CrossRef]
- Goeckenjan, M.; Rabe, T.; Strowitzki, T. Postkoitale Kontrazeption. Gynäkologische Endokrinol. 2012, 10, 45–56. [Google Scholar] [CrossRef]
- ICEC—International Consortium on Emergency Contraception. Status & Availability Database. Available online: https://www.cecinfo.org/country-by-country-information/status-availability-database/ (accessed on 3 June 2021).
- Bundesrat; Beschluss des Bundesrates. Vierzehnte Verordnung zur Änderung der Arzneimittelverschreibungsverordnung. Drucksache 28/15. 06.03.2015. Available online: https://www.bundesrat.de/SharedDocs/drucksachen/2015/0001-0100/28-15(B).pdf?__blob=publicationFile&v=4 (accessed on 22 February 2021).
- AMVV. Arzneimittelverschreibungsverordnung vom 21. Dezember 2005 (BGBl. I S. 3632), die zuletzt durch Artikel 1 der Verordnung vom 21. Oktober 2020 (BGBl. I S. 2260) geändert worden ist. Available online: https://www.gesetze-im-internet.de/amvv/AMVV.pdf (accessed on 22 February 2021).
- ECEC—European Consortium for Emergency Contraception. Emergency Contraception in Europe. Poland. Available online: https://www.ec-ec.org/emergency-contraception-in-europe/country-by-country-information-2/poland/ (accessed on 3 June 2021).
- Amnesty International. Poland: Emergency Contraception Restrictions Catastrophic for Women and Girls. Available online: https://www.amnesty.org/en/latest/news/2017/06/poland-emergency-contraception-restrictions-catastrophic-for-women-and-girls/ (accessed on 3 June 2021).
- ApoG. Apothekengesetz in der Fassung der Bekanntmachung vom 15. Oktober 1980 (BGBl. I S. 1993), das zuletzt durch Artikel 2 des Gesetzes vom 9. Dezember 2020 (BGBl. I S. 2870) Geändert Worden ist. Available online: https://www.gesetze-im-internet.de/apog/ApoG.pdf (accessed on 22 February 2021).
- Chau, V.M.; Stamm, C.A.; Borgelt, L.; Gaffaney, M.; Moore, A.; Blumhagen, R.Z.; Rupp, L.; Topp, D.; Gilroy, C. Barriers to Single-Dose Levonorgestrel-Only Emergency Contraception Access in Retail Pharmacies. Women’s Health Issues 2017, 27, 518–522. [Google Scholar] [CrossRef] [Green Version]
- Chin, J.; Salcedo, J.; Raidoo, S. Over-The-Counter Availability of Levonorgestrel Emergency Contraception in Pharmacies on Oahu. Pharmacy 2020, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Deutscher Bundestag. Achtzehntes Hauptgutachten der Monopolkommission 2008/2009. Drucksache 17/2600. Available online: http://www.monopolkommission.de/images/PDF/HG/HG18/1702600.pdf (accessed on 22 February 2021).
- Arora, S.; Sood, N.; Terp, S.; Joyce, G. The price may not be right: The value of comparison shopping for prescription drugs. Am. J. Manag. Care 2017, 23, 410–415. [Google Scholar]
- Langer, B.; Kunow, C. Medication dispensing, additional therapeutic recommendations, and pricing practices for acute diarrhoea by community pharmacies in Germany: A simulated patient study. Pharm. Pract. 2019, 17, 1579. [Google Scholar] [CrossRef] [Green Version]
- ABDA—Federal Union of German Associations of Pharmacists. German Pharmacies. Figures, Data, Facts. Available online: https://www.abda.de/fileadmin/user_upload/assets/ZDF/ZDF_2020/ABDA_ZDF_2020_Brosch_english.pdf (accessed on 22 February 2021).
- BAK—Federal Chamber of Pharmacists. Information und Beratung des Patienten bei der Abgabe von Arzneimitteln—Selbstmedikation. Available online: https://www.abda.de/fuer-apotheker/qualitaetssicherung/leitlinien/leitlinien-und-arbeitshilfen/ (accessed on 3 June 2021).
- ApBetrO. Apothekenbetriebsordnung in der Fassung der Bekanntmachung vom 26. September 1995 (BGBl. I S. 1195), die zuletzt durch Artikel 3 des Gesetzes vom 9. Dezember 2020 (BGBl. I S. 2870) geändert worden ist. Available online: https://www.gesetze-im-internet.de/apobetro_1987/ApBetrO.pdf (accessed on 22 February 2021).
- Schulz, M.; Goebel, R.; Schumann, C.; Zagermann-Muncke, P. Non-prescription dispensing of emergency oral contraceptives: Recommendations from the German Federal Chamber of Pharmacists [Bundesapothekerkammer]. Pharm. Pract. 2016, 14, 828. [Google Scholar] [CrossRef]
- BAK—Federal Chamber of Pharmacists. Handlungsempfehlung: Rezeptfreie Abgabe von Notfallkontrazeptiva (“Pille danach“). Available online: https://www.abda.de/aktuelles-und-presse/newsroom/detail/pille-danach/ (accessed on 22 February 2021).
- Arzbach, V. Pille Danach: Ein Jahr Rezeptfrei. PTA-Forum. Available online: https://ptaforum.pharmazeutische-zeitung.de/ausgabe-062016/ein-jahr-rezeptfrei/ (accessed on 22 February 2021).
- Heßling, A.; Bode, H. Sexual- und Verhütungsverhalten Jugendlicher im Wandel Sexual and contraceptive behaviour of young people throughout the decades. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2017, 60, 937–947. [Google Scholar] [CrossRef]
- Von Rosen, F.T.; Von Rosen, A.J.; Muller-Riemenschneider, F.; Tinnemann, P. Awareness and knowledge regarding emergency contraception in Berlin adolescents. Eur. J. Contracept. Reprod. Health Care 2017, 22, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Burgo, C.L.-D.; Mikolajczyk, R.T.; Osorio, A.; Carlos, S.; Errasti, T.; De Irala, J. Knowledge and beliefs about mechanism of action of birth control methods among European women. Contraception 2012, 85, 69–77. [Google Scholar] [CrossRef]
- Nappi, R.E.; Abascal, P.L.; Mansour, D.; Rabe, T.; Shojai, R.; for the Emergency Contraception Study Group. Use of and attitudes towards emergency contraception: A survey of women in five European countries. Eur. J. Contracept. Reprod. Health Care 2014, 19, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Arzbach, V. Pille Danach: Wissenslücken und Abgabehindernisse. PTA-Forum. Available online: https://ptaforum.pharmazeutische-zeitung.de/ausgabe-222018/wissensluecken-und-abgabehindernisse/ (accessed on 22 February 2021).
- Freye, R. Immer noch viel Unwissenheit über die Pille danach. Gynäkologie + Geburtshilfe 2018, 23, 68. [Google Scholar] [CrossRef]
- Bode, H.; Heßling, A. Jugendsexualität 2015. Die Perspektive der 14- bis 25-Jährigen. Ergebnisse einer aktuellen Repräsentativen Wiederholungsbefragung. Bundeszentrale für gesundheitliche Aufklärung, Köln. Available online: https://www.forschung.sexualaufklaerung.de/fileadmin/fileadmin-forschung/pdf/Jugendendbericht%2001022016%20.pdf (accessed on 22 February 2021).
- Renner, I. Informationsstand zur Pille danach—Ergebnisse einer bundesweiten repräsentativen Befragung erwachsener Frauen. In Rezeptfreie Pille danach—Abgabepraxis und Information; pro familia Bundesverband: Berlin, Germany, 2015; pp. 11–13. Available online: https://www.profamilia.de/fileadmin/publikationen/Fachpublikationen/doku_pille__danach-2016_web.pdf (accessed on 22 February 2021).
- Wilkinson, T.A.; Fahey, N.; Shields, C.; Suther, E.; Cabral, H.J.; Silverstein, M. Pharmacy Communication to Adolescents and Their Physicians Regarding Access to Emergency Contraception. Pediatrics 2012, 129, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, T.A.; Fahey, N.; Suther, E.; Cabral, H.J.; Silverstein, M. Access to Emergency Contraception for Adolescents. JAMA 2012, 307, 362–363. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, T.A.; Vargas, G.; Fahey, N.; Suther, E.; Silverstein, M. “I’ll See What I Can Do”: What Adolescents Experience When Requesting Emergency Contraception. J. Adolesc. Heal. 2014, 54, 14–19. [Google Scholar] [CrossRef]
- Wilkinson, T.A.; Clark, P.; Rafie, S.; Carroll, A.E.; Miller, E. Access to Emergency Contraception After Removal of Age Restrictions. Pediatrics 2017, 140, e20164262. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, T.A.; Rafie, S.; Clark, P.D.; Carroll, A.E.; Miller, E. Evaluating Community Pharmacy Responses about Levonorgestrel Emergency Contraception by Mystery Caller Characteristics. J. Adolesc. Heal. 2018, 63, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Ritter, A.H.; Isaacs, C.R.; Lee, S.M.; Lee, A.J. Single-Dose Levonorgestrel Emergency Contraception and Silent Barriers to Its Access: Is It Really Just One Step? J. Women’s Health 2018, 27, 646–650. [Google Scholar] [CrossRef]
- French, V.A.; Rangel, A.V.; Mattingly, T.L. Access to emergency contraception in Kansas City clinics. Contraception 2018, 98, 482–485. [Google Scholar] [CrossRef] [PubMed]
- French, V.A.; Mattingly, T.L.; Rangel, A.V.; Shelton, A.U. Availability of ulipristal acetate: A secret shopper survey of pharmacies in a metropolitan area on emergency contraception. J. Am. Pharm. Assoc. 2019, 59, 832–835. [Google Scholar] [CrossRef]
- Ditmars, L.; Rafie, S.; Kashou, G.; Cleland, K.; Bayer, L.; Wilkinson, T.A. Emergency Contraception Counseling in California Community Pharmacies: A Mystery Caller Study. Pharmacy 2019, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Brant, A.; White, K.; Marie, P.S. Pharmacy availability of ulipristal acetate emergency contraception: An audit study. Contraception 2014, 90, 338–339. [Google Scholar] [CrossRef]
- Peters, J.; Desai, K.; Ricci, D.; Chen, D.; Singh, M.; Chewning, B. The power of the patient question: A secret shopper study. Patient Educ. Couns. 2016, 99, 1526–1533. [Google Scholar] [CrossRef]
- Bullock, H.; Steele, S.; Kurata, N.; Tschann, M.; Elia, J.; Kaneshiro, B.; Salcedo, J. Pharmacy access to ulipristal acetate in Hawaii: Is a prescription enough? Contraception 2016, 93, 452–454. [Google Scholar] [CrossRef] [Green Version]
- Bullock, H.; Tschann, M.; Elia, J.; Kaneshiro, B.; Salcedo, J. From Kaua‘i to Hawai‘i Island: Interisland Differences in Emergency Contraceptive Pill Availability. Hawaii J. Med. Public Health 2017, 76, 178–182. [Google Scholar]
- Gaffaney, M.; Stamm, C.; Borgelt, L.; Chau, V.M.; Rupp, L.; Blumhagen, R.; Gilroy, C. 67. Barriers to Emergency Contraception Access in the State of Wyoming. J. Adolesc. Health 2015, 56, S36. [Google Scholar] [CrossRef]
- Orr, K.K.; Lemay, V.A.; Wojtusik, A.P.; Opydo-Rossoni, M.; Cohen, L.B. Availability and Accuracy of Information Regarding Nonprescription Emergency Contraception. J. Pharm. Pract. 2016, 29, 454–460. [Google Scholar] [CrossRef]
- Shigesato, M.; Elia, J.; Tschann, M.; Bullock, H.; Hurwitz, E.; Wu, Y.Y.; Salcedo, J. Pharmacy access to Ulipristal acetate in major cities throughout the United States. Contraception 2018, 97, 264–269. [Google Scholar] [CrossRef]
- Uysal, J.; Tavrow, P.; Hsu, R.; Alterman, A. Availability and Accessibility of Emergency Contraception to Adolescent Callers in Pharmacies in Four Southwestern States. J. Adolesc. Health 2019, 64, 219–225. [Google Scholar] [CrossRef]
- Bell, D.L.; Camacho, E.J.; Velasquez, A.B. Male access to emergency contraception in pharmacies: A mystery shopper survey. Contraception 2014, 90, 413–415. [Google Scholar] [CrossRef]
- Bruhns, C. Ergebnisse einer bundesweiten Befragung zur aktuellen Abgabepraxis der Pille danach. In Rezeptfreie Pille danach—Abgabepraxis und Information; pro familia Bundesverband: Berlin, Germany, 2015; pp. 14–20. Available online: https://www.profamilia.de/fileadmin/publikationen/Fachpublikationen/doku_pille__danach-2016_web.pdf (accessed on 22 February 2021).
- Dierolf, V.; Freytag, S. Zugang zur Pille danach in den Apotheken nach der Rezeptfreigabe. Pro Fam. Magazin. 2017, 45, 9–12. [Google Scholar]
- Pro familia Bundesverband. Pille danach rezeptfrei: Zugang ohne Hürden? Nutzerrinnenbefragung zur Vergabepraxis in Apotheken. Available online: https://www.profamilia.de/fileadmin/publikationen/Fachpublikationen/Verhuetung/Pille_danach-Zugang-ohne_huerden.pdf (accessed on 22 February 2021).
- Said, A.; Ganso, M.; Freudewald, L.; Schulz, M. Trends in dispensing oral emergency contraceptives and safety issues: A survey of German community pharmacists. Int. J. Clin. Pharm. 2019, 41, 1499–1506. [Google Scholar] [CrossRef] [Green Version]
- Callegaro, M. Social Desirability. In Encyclopedia of Survey Research; SAGE Publications: Los Angeles, CA, USA, 2008; pp. 825–826. [Google Scholar] [CrossRef]
- Saxena, P.; Mishra, A.; Nigam, A. Evaluation of pharmacists’ services for dispensing emergency contraceptive pills in Delhi, India: A mystery shopper study. Indian J. Community Med. 2016, 41, 198–202. [Google Scholar] [CrossRef]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [Green Version]
- Caamaño, F.; Ruano, A.; Figueiras, A.; Gestal-Otero, J. Data collection methods for analyzing the quality of the dispensing in pharmacies. Pharm. World Sci. 2002, 24, 217–223. [Google Scholar] [CrossRef]
- Puspitasari, H.P.; Aslani, P.; Krass, I. A review of counseling practices on prescription medicines in community pharmacies. Res. Soc. Adm. Pharm. 2009, 5, 197–210. [Google Scholar] [CrossRef]
- Converse, L.; Barrett, K.; Rich, E.; Reschovsky, J. Methods of Observing Variations in Physicians’ Decisions: The Opportunities of Clinical Vignettes. J. Gen. Intern. Med. 2015, 30, 586–594. [Google Scholar] [CrossRef] [Green Version]
- Bardage, C.; Westerlund, T.; Barzi, S.; Bernsten, C. Non-prescription medicines for pain and fever—A comparison of recommendations and counseling from staff in pharmacy and general sales stores. Heal. Policy 2013, 110, 76–83. [Google Scholar] [CrossRef]
- Xu, T.; Neto, A.C.D.A.; Moles, R.J. A systematic review of simulated-patient methods used in community pharmacy to assess the provision of non-prescription medicines. Int. J. Pharm. Pract. 2012, 20, 307–319. [Google Scholar] [CrossRef]
- Langer, B.; Grimm, S.; Lungfiel, G.; Mandlmeier, F.; Wenig, V. The Quality of Counselling for Oral Emergency Contraceptive Pills—A Simulated Patient Study in German Community Pharmacies. Int. J. Environ. Res. Public Health 2020, 17, 6720. [Google Scholar] [CrossRef]
- Hussainy, S.Y.; Ghosh, A.; Taft, A.; Mazza, D.; Black, K.I.; Clifford, R.; Gudka, S.; Mc Namara, K.; Ryan, K.; Jackson, J.K. Protocol for ACCESS: A qualitative study exploring barriers and facilitators to accessing the emergency contraceptive pill from community pharmacies in Australia. BMJ Open 2015, 5, e010009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- STROBE Statement—Checklist of Items That Should Be Included in Reports of Cross-Sectional Studies. Available online: https://www.strobe-statement.org/fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_cross-sectional.pdf (accessed on 22 February 2021).
- Langer, B.; Kunow, C. Do north-eastern German pharmacies recommend a necessary medical consultation for acute diarrhoea? Magnitude and determinants using a simulated patient approach [version 2; peer review: 3 approved]. F1000Research 2020, 8, 1841. [Google Scholar] [CrossRef] [PubMed]
- Kunow, C.; Langer, B. Using the simulated patient methodology to assess the quality of counselling in german community pharmacies: A systematic review from 2005 to 2018. Int. J. Pharm. Pharm. Sci. 2021, 13, 10–19. [Google Scholar] [CrossRef]
- Watson, M.C.; Norris, P.; Granas, A.G. A systematic review of the use of simulated patients and pharmacy practice research. Int. J. Pharm. Pract. 2010, 14, 83–93. [Google Scholar] [CrossRef]
- Björnsdottir, I.; Granas, A.G.; Bradley, A.; Norris, P. A systematic review of the use of simulated patient methodology in pharmacy practice research from 2006 to 2016. Int. J. Pharm. Pract. 2020, 28, 13–25. [Google Scholar] [CrossRef] [Green Version]
- da Costa, F.A. Covert and overt observations in pharmacy practice. In Pharmacy Practice Research Methods; Babar, Z.U.D., Ed.; Springer: Singapore, 2020; pp. 93–114. [Google Scholar] [CrossRef]
- PSA—Pharmaceutical Society of Australia. Guidance for Provision of a Pharmacist Only Medicine. Levonorgestrel. Approved Indication: Emergency Contraception. Available online: https://www.familyplanningallianceaustralia.org.au/wp-content/uploads/2015/08/PSA-Guidelines-on-EC.pdf (accessed on 3 June 2021).
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M. Does abortion reduce the mental health risks of unwanted or unintended pregnancy? A re-appraisal of the evidence. Aust. N. Z. J. Psychiatry 2013, 47, 819–827. [Google Scholar] [CrossRef]
- Steinberg, J.; Rubin, L.R. Psychological Aspects of Contraception, Unintended Pregnancy, and Abortion. Policy Insights Behav. Brain Sci. 2014, 1, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Abajobir, A.A.; Maravilla, J.C.; Alati, R.; Najman, J. A systematic review and meta-analysis of the association between unintended pregnancy and perinatal depression. J. Affect. Disord. 2016, 192, 56–63. [Google Scholar] [CrossRef]
- BZgA. Contraceptive Behaviour of Adults 2011. Results of a Representative Survey. Available online: https://publikationen.sexualaufklaerung.de/fileadmin/redakteur/publikationen/dokumente/13317270.pdf (accessed on 22 February 2021).
- David, M.; Radke, A.-M.; Pietzner, K. The Prescription of the Morning-After Pill in a Berlin Emergency Department Over a Four-Year Period—User Profiles and Reasons for Use. Geburtshilfe Frauenheilkd. 2012, 72, 392–396. [Google Scholar] [CrossRef] [Green Version]
- Apotheken Umschau. Apotheken in Deutschland nach Postleitzahlbereichen suchen und finden. Available online: https://www.apotheken-umschau.de/apotheken/Deutschland (accessed on 22 February 2021).
- Israel, G.D. Determining Sample Size. University of Florida. Available online: http://www.psycholosphere.com/Determining%20sample%20size%20by%20Glen%20Israel.pdf (accessed on 22 February 2021).
- ICEC/FIGO—International Consortium for Emergency Contraception/International Federation of Gynecology and Obstetrics. Emergency Contraceptive Pills. Medical and Service Delivery Guidance. Available online: https://www.cecinfo.org/wp-content/uploads/2018/12/ICEC-guides_FINAL.pdf (accessed on 3 June 2021).
- Creinin, M.D.; Schlaff, W.; Archer, D.F.; Wan, L.; Frezieres, R.; Thomas, M.; Rosenberg, M.; Higgins, J. Progesterone Receptor Modulator for Emergency Contraception. Obstet. Gynecol. 2006, 108, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Glasier, A.F.; Cameron, S.T.; Fine, P.M.; Logan, S.J.; Casale, W.; Van Horn, J.; Sogor, L.; Blithe, D.L.; Scherrer, B.; Mathe, H.; et al. Ulipristal acetate versus levonorgestrel for emergency contraception: A randomised non-inferiority trial and meta-analysis. Lancet 2010, 375, 555–562. [Google Scholar] [CrossRef]
- Shen, J.; Che, Y.; Showell, E.; Chen, K.; Cheng, L. Interventions for emergency contraception. Cochrane Database Syst. Rev. 2019, 2019, CD001324. [Google Scholar] [CrossRef]
- Lauer Taxe. LTO4.0. Available online: https://www.cgm.com/deu_de/produkte/apotheke/lauer-taxe.html (accessed on 24 April 2021).
- Zapata-Cachafeiro, M.; Piñeiro-Lamas, M.; Guinovart, M.C.; López-Vázquez, P.M.; Vazquez-Lago, J.; Figueiras, A. Magnitude and determinants of antibiotic dispensing without prescription in Spain: A simulated patient study. J. Antimicrob. Chemother. 2019, 74, 511–514. [Google Scholar] [CrossRef]
- Paravattil, B.; Kheir, N.; Yousif, A. Utilization of simulated patients to assess diabetes and asthma counseling practices among community pharmacists in Qatar. Int. J. Clin. Pharm. 2017, 28, 179–768. [Google Scholar] [CrossRef]
- Saba, M.; Diep, J.; Bittoun, R.; Saini, B. Provision of smoking cessation services in Australian community pharmacies: A simulated patient study. Int. J. Clin. Pharm. 2014, 36, 604–614. [Google Scholar] [CrossRef]
- Kippist, C.; Wong, K.K.H.; Bartlett, D.; Saini, B. How do pharmacists respond to complaints of acute insomnia? A simulated patient study. Int. J. Clin. Pharm. 2011, 33, 237–245. [Google Scholar] [CrossRef]
- Al Qarni, H.; Alrahbini, T.; AlQarni, A.M.; Alqarni, A. Community pharmacist counselling practices in the Bisha health directorate, Saudi Arabia –simulated patient visits. BMC Health Serv. Res. 2020, 20, 745. [Google Scholar] [CrossRef]
- StGB—Strafgesetzbuch in der Fassung der Bekanntmachung vom 13. November 1998 (BGBl. I S. 3322), das zuletzt durch Artikel 1 des Gesetzes vom 3. März 2020 (BGBl. I S. 431) geändert worden ist. Available online: https://www.gesetze-im-internet.de/stgb/StGB.pdf (accessed on 8 March 2021).
- Rhodes, K.V.; Miller, F.G. Simulated Patient Studies: An Ethical Analysis. Milbank Q. 2012, 90, 706–724. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, A.; Tumlinson, K. Strategies for Optimal Implementation of Simulated Clients for Measuring Quality of Care in Low- and Middle-Income Countries. Glob. Health Sci. Pract. 2017, 5, 108–114. [Google Scholar] [CrossRef] [Green Version]
- BKK—Bundesamt für Bevölkerungsschutz und Katastrophenhilfe. COVID-19: Übersicht Kritischer Dienstleistungen. Sektorspezifische Hinweise und Informationen mit KRITIS-Relevanz. Available online: https://www.bbk.bund.de/SharedDocs/Downloads/BBK/DE/Sonstiges/Covid_19_Uebersicht_Kritischer_Dienstleistungen.pdf?__blob=publicationFile (accessed on 17 March 2021).
- Habibzadeh, F. Common statistical mistakes in manuscripts submitted to biomedical journals. Eur. Sci. Ed. 2013, 39, 92–94. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Berger, K.; Eickhoff, C.; Schulz, M. Counselling quality in community pharmacies: Implementation of the pseudo customer methodology in Germany. J. Clin. Pharm. Ther. 2005, 30, 45–57. [Google Scholar] [CrossRef]
- BVM. Berufsverband Deutscher Markt-und Sozialforscher e.V. Richtlinie für den Einsatz von Mystery Research in der Markt- und Sozialforschung. Available online: https://www.bvm.org/fileadmin/user_upload/Verbandsdokumente/Standesregeln/RL_2006_Mystery.pdf (accessed on 22 February 2021).
- Kashyap, K.C.; Nissen, L.; Smith, S.; Kyle, G. Management of over-the-counter insomnia complaints in Australian community pharmacies: A standardized patient study. Int. J. Pharm. Pract. 2014, 22, 125–134. [Google Scholar] [CrossRef]
- da Rocha, C.E.; Bispo, M.L.; dos Santos, A.C.O.; Mesquita, A.; Brito, G.C.; de Lyra, D.P. Assessment of Community Pharmacists’ Counseling Practices With Simulated Patients Who Have Minor Illness. Simul. Heal. J. Soc. Simul. Heal. 2015, 10, 227–238. [Google Scholar] [CrossRef]
- Mobark, D.M.; Al-Tabakha, M.M.; Hasan, S. Assessing hormonal contraceptive dispensing and counseling provided by community pharmacists in the United Arab Emirates: A simulated patient study. Pharm. Pract. 2019, 17, 1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, J.H.; Mbadu, M.F.; Garcia, M.; Glover, A. The provision of emergency contraception in Kinshasa’s private sector pharmacies: Experiences of mystery clients. Contraception 2018, 97, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavares, M.P.; Foster, A.M. Emergency contraception in a public health emergency: Exploring pharmacy availability in Brazil. Contraception 2016, 94, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.C.; Schneider, C.R.; Naughtin, C.L.; Wilson, F.; Neto, A.C.D.A.; Moles, R.J. Mystery shopping and coaching as a form of audit and feedback to improve community pharmacy management of non-prescription medicine requests: An intervention study. BMJ Open 2017, 7, e019462. [Google Scholar] [CrossRef] [Green Version]
- Hussainy, S.Y.; Stewart, K.; Pham, M.-P. A mystery caller evaluation of emergency contraception supply practices in community pharmacies in Victoria, Australia. Aust. J. Prim. Heal. 2015, 21, 310–316. [Google Scholar] [CrossRef]
- Langer, B.; Bull, E.; Burgsthaler, T.; Glawe, J.; Schwobeda, M.; Simon, K. Assessment of counselling for acute diarrhoea in German pharmacies: A simulated patient study. Int. J. Pharm. Pract. 2018, 26, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Sharif, S.I. Peer Review Report For: Do north-eastern German pharmacies recommend a necessary medical consultation for acute diarrhoea? Magnitude and determinants using a simulated patient approach [version 1; peer review: 1 approved, 2 approved with reservations]. F1000Research 2019, 8, 1841. [Google Scholar] [CrossRef]

{kind=link}
| Possible Questions by the Pharmacy Staff Based on the Questions of the BAK Checklist [20] | Response Specifications for MCs |
|---|---|
| “I am 24.” (female MCs) “She’s 24.” (male MCs) |
| “We had a condom failure.” |
| “4 days ago.” |
| “11 days ago.” |
| 5th to 8th: “No.” (female MCs) 5th to 8th: “I don’t know.” (male MCs) |
| “No.” (female MCs) |
| “Is your friend aware of any acute health problems or chronic illnesses?” | “No.” (male MCs) |
| “No.” (female MCs) “No.” (male MCs) |
| “No.” (female MCs) “No.” (male MCs) |
| “No.” (female MCs) “No.” (male MCs) |
| Information Gathering Including a Possible Recommendation of Oral EC by Pharmacy Staff (Based on Sub-Scenario 1) | ||
|---|---|---|
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
Did the pharmacy staff enquire whether…
| Yes ☐ Yes ☐ Yes ☐ Yes ☐ | No ☐ No ☐ No ☐ No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ | No ☐ |
| Yes ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ | No ☐ No ☐ No ☐ No ☐ No ☐ |
| Visit to the doctor ☐ Visit in CP ☐ | |
| Requests by MCs (Based on Sub-Scenario 2) | ||
| Yes ☐ (UPA) Yes ☐ (LNG) Yes ☐ (UPA) Yes ☐ (LNG) | No ☐ (UPA) No ☐ (LNG) No ☐ (UPA) No ☐ (LNG) |
| on the same day ☐ the next day ☐ later than the next day ☐ unknown ☐ on the same day ☐ the next day ☐ later than the next day ☐ unknown ☐ | |
| Price (UPA): … Price (LNG): … | |
| Possible Influencing Factors | ||
| … | |
| female ☐ | male ☐ |
| female ☐ | male ☐ |
| Yes ☐ No ☐ unknown ☐ | |
| …, … min. | |
| Yes ☐ | No ☐ |
| …………………………………… | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunow, C.; Bello, M.A.; Diedrich, L.; Eutin, L.; Sonnenberg, Y.; Wachtel, N.; Langer, B. A Nationwide Mystery Caller Evaluation of Oral Emergency Contraception Practices from German Community Pharmacies: An Observational Study Protocol. Healthcare 2021, 9, 945. https://doi.org/10.3390/healthcare9080945
Kunow C, Bello MA, Diedrich L, Eutin L, Sonnenberg Y, Wachtel N, Langer B. A Nationwide Mystery Caller Evaluation of Oral Emergency Contraception Practices from German Community Pharmacies: An Observational Study Protocol. Healthcare. 2021; 9(8):945. https://doi.org/10.3390/healthcare9080945
Chicago/Turabian StyleKunow, Christian, Moulika Aline Bello, Laura Diedrich, Laura Eutin, Yanneck Sonnenberg, Nele Wachtel, and Bernhard Langer. 2021. "A Nationwide Mystery Caller Evaluation of Oral Emergency Contraception Practices from German Community Pharmacies: An Observational Study Protocol" Healthcare 9, no. 8: 945. https://doi.org/10.3390/healthcare9080945
APA StyleKunow, C., Bello, M. A., Diedrich, L., Eutin, L., Sonnenberg, Y., Wachtel, N., & Langer, B. (2021). A Nationwide Mystery Caller Evaluation of Oral Emergency Contraception Practices from German Community Pharmacies: An Observational Study Protocol. Healthcare, 9(8), 945. https://doi.org/10.3390/healthcare9080945