
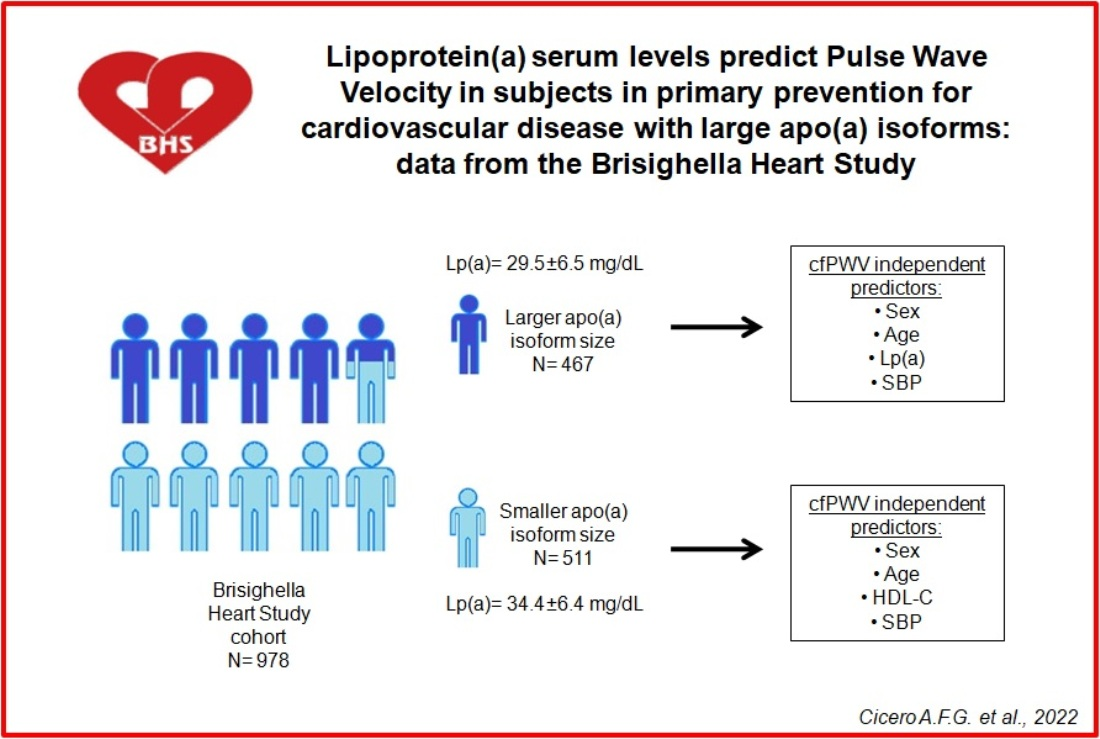
Lipoprotein(a) Serum Levels Predict Pulse Wave Velocity in Subjects in Primary Prevention for Cardiovascular Disease with Large Apo(a) Isoforms: Data from the Brisighella Heart Study

 ,
,  , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Laboratory Analyses
2.3. Arterial Stiffness Evaluation
2.4. Ankle Brachial Index
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Peng, J.; Liu, M.M.; Liu, H.H.; Xu, R.X.; Zhu, C.G.; Guo, Y.L.; Wu, N.Q.; Dong, Q.; Cui, C.J.; Li, J.J. Lipoprotein (a)-mediated vascular calcification: Population-based and in vitro studies. Metabolism 2021, 127, 154960. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Sirtori, C.R.; Corsini, A.; Watts, G.F.; Sahebkar, A. Lipoprotein(a): Knowns, unknowns and uncertainties. Pharmacol. Res. 2021, 173, 105812. [Google Scholar] [CrossRef] [PubMed]
- van der Hoek, Y.Y.; Wittekoek, M.E.; Beisiegel, U.; Kastelein, J.J.; Koschinsky, M.L. The apolipoprotein(a) kringle IV repeats which differ from the major repeat kringle are present in variably-sized isoforms. Hum. Mol. Genet. 1993, 2, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Yang, Y.; Lu, J.; Liang, J.; He, Y.; Yu, Y.; Huang, H.; Li, Q.; Wang, B.; Li, S.; et al. Association of Lipoprotein(a)-Associated Mortality and the Estimated Glomerular Filtration Rate Level in Patients Undergoing Coronary Angiography: A 51,500 Cohort Study. Front. Cardiovasc. Med. 2021, 8, 747120. [Google Scholar] [CrossRef]
- Liu, J.; Liu, L.; Wang, B.; Chen, S.; Liu, B.; Liang, J.; Huang, H.; Li, Q.; Lun, Z.; Ying, M.; et al. Coronary Artery Disease: Optimal Lipoprotein(a) for Survival-Lower Is Better? A Large Cohort with 43,647 Patients. Front. Cardiovasc. Med. 2021, 8, 670859. [Google Scholar] [CrossRef]
- Brosolo, G.; Da Porto, A.; Bulfone, L.; Vacca, A.; Bertin, N.; Colussi, G.; Cavarape, A.; Sechi, L.A.; Catena, C. Plasma Lipoprotein(a) Levels as Determinants of Arterial Stiffening in Hypertension. Biomedicines 2021, 9, 1510. [Google Scholar] [CrossRef]
- Sorokin, A.; Kotani, K. Lipoprotein(a) and Arterial Stiffness Parameters. Pulse 2015, 3, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Cicero, A.F.G.; Gitto, S.; Fogacci, F.; Rosticci, M.; Giovannini, M.; D’Addato, S.; Andreone, P.; Borghi, C.; Brisighella Heart Study Group Medical and Surgical Sciences Dept., University of Bologna. Fatty liver index is associated to pulse wave velocity in healthy subjects: Data from the Brisighella Heart Study. Eur. J. Intern. Med. 2018, 53, 29–33. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Rizzoli, E.; D’Addato, S.; Borghi, C. Long-Term Impact of Different Triple Combination Antihypertensive Medications on Blood Pressure Control, Metabolic Pattern and Incident Events: Data from the Brisighella Heart Study. J. Clin. Med. 2021, 10, 5921. [Google Scholar] [CrossRef]
- Coppola, P.; Cicero, A.F.G.; Fogacci, F.; D’Addato, S.; Bacchelli, S.; Borghi, C.; On Behalf of the Brisighella Heart Study Group. Laboratory and Instrumental Risk Factors Associated with a Sudden Cardiac Death Prone ECG Pattern in the General Population: Data from the Brisighella Heart Study. J. Clin. Med. 2021, 10, 640. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Grandi, E.; D’Addato, S.; Borghi, C.; Brisighella Heart Study Group. Interaction between low-density lipoprotein-cholesterolaemia, serum uric level and incident hypertension: Data from the Brisighella Heart Study. J. Hypertens. 2019, 37, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Rosticci, M.; Bove, M.; Fogacci, F.; Giovannini, M.; Urso, R.; D’Addato, S.; Borghi, C.; Brisighella Heart Study Group. Serum uric acid change and modification of blood pressure and fasting plasma glucose in an overall healthy population sample: Data from the Brisighella heart study. Ann. Med. 2017, 49, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Dati, F.; Tate, J.R.; Marcovina, S.M.; Steinmetz, A. International Federation of Clinical Chemistry and Laboratory Medicine, & IFCC Working Group for Lipoprotein(a) Assay Standardization. First WHO/IFCC International Reference Reagent for Lipoprotein(a) for Immunoassay—Lp(a) SRM 2B. Clin. Chem. Lab. Med. 2004, 42, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Langer, C.; Tambyrayah, B.; Nowak-Göttl, U. Testing for apolipoprotein(a) phenotype using isoelectric focusing and immunoblotting technique. Methods Mol. Biol. 2013, 992, 407–412. [Google Scholar] [CrossRef]
- Gazzaruso, C.; Garzaniti, A.; Buscaglia, P.; Bonetti, G.; Falcone, C.; Fratino, P.; Finardi, G.; Geroldi, D. Apolipoprotein(a) phenotypes and their predictive value for coronary heart disease: Identification of an operative cut-off of apolipoprotein(a) polymorphism. J. Cardiovasc. Risk 1998, 5, 37–42. [Google Scholar] [CrossRef]
- Emanuele, E.; Lusignani, L.S.; Peros, E.; Montagna, G.; D’Angelo, A.; Montagna, L.; Geroldi, D. Lipoprotein(a)-associated atherothrombotic risk in hemodialysis patients. Am. J. Nephrol. 2004, 24, 221–229. [Google Scholar] [CrossRef]
- Parsons, T.J.; Sartini, C.; Ellins, E.A.; Halcox, J.P.J.; Smith, K.E.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Lee, I.M.; Whincup, P.H.; et al. Objectively measured physical activity, sedentary time and subclinical vascular disease: Cross-sectional study in older British men. Prev. Med. 2016, 89, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Müller, J.; Ewert, P.; Hager, A. Increased aortic blood pressure augmentation in patients with congenital heart defects e a cross sectional study in 1125 patients and 322 controls. Int. J. Cardiol. 2015, 184, 225–229. [Google Scholar] [CrossRef]
- Hickson, S.; Butlin, M.; Broad, J.; Avolio, A.P.; Wilkinson, I.B.; McEniery, C.M. Validity and repeatability of the Vicorder apparatus: A comparison with the SphygmoCor device. Hypertens. Res. 2009, 32, 1079–1085. [Google Scholar] [CrossRef]
- McGreevy, C.; Barry, M.; Bennett, K.; Williams, D. Repeatability of the measurement of aortic pulse wave velocity (aPWV) in the clinical assessment of arterial stiffness in community welling older patients using the Vicorder device. Scand. J. Clin. Lab. Investig. 2013, 73, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruscica, M.; Macchi, C.; Fogacci, F.; Ferri, N.; Grandi, E.; Rizzoli, E.; D’Addato, S.; Borghi, C.; Cicero, A.F.; Brisighella Heart Study Group. Angiopoietin-like 3 and subclinical peripheral arterial disease: Evidence from the Brisighella Heart Study. Eur. J. Prev. Cardiol. 2020, 27, 2251–2254. [Google Scholar] [CrossRef] [Green Version]
- Samba, H.; Guerchet, M.; Ndamba-Bandzouzi, B.; Kehoua, G.; Mbelesso, P.; Desormais, I.; Aboyans, V.; Preux, P.M.; Lacroix, P. Ankle Brachial Index (ABI) predicts 2-year mortality risk among older adults in the Republic of Congo: The EPIDEMCA-FU study. Atherosclerosis 2019, 286, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Simera, I.; Moher, D.; Hoey, J.; Schulz, K.F.; Altman, D.G. A catalogue of reporting guidelines for health research. Eur. J. Clin. Investig. 2010, 40, 35–53. [Google Scholar] [CrossRef]
- Sahebkar, A.; Reiner, Ž.; Simental-Mendía, L.E.; Ferretti, G.; Cicero, A.F. Effect of extended-release niacin on plasma lipoprotein(a) levels: A systematic review and meta-analysis of randomized placebo-controlled trials. Metabolism 2016, 65, 1664–1678. [Google Scholar] [CrossRef]
- Fogacci, F.; Ferri, N.; Toth, P.P.; Ruscica, M.; Corsini, A.; Cicero, A.F.G. Efficacy and Safety of Mipomersen: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Drugs 2019, 79, 751–766. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Bove, M.; Borghi, C. Pharmacokinetics, pharmacodynamics and clinical efficacy of non-statin treatments for hypercholesterolemia. Expert Opin. Drug Metab. Toxicol. 2018, 14, 9–15. [Google Scholar] [CrossRef]
- Strilchuk, L.; Fogacci, F.; Cicero, A.F. Safety and tolerability of injectable lipid-lowering drugs: An update of clinical data. Expert Opin. Drug Saf. 2019, 18, 611–621. [Google Scholar] [CrossRef]
- Willeit, P.; Ridker, P.M.; Nestel, P.J.; Simes, J.; Tonkin, A.M.; Pedersen, T.R.; Schwartz, G.G.; Olsson, A.G.; Colhoun, H.M.; Kronenberg, F.; et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: Individual patient-data meta-analysis of statin outcome trials. Lancet 2018, 392, 1311–1320. [Google Scholar] [CrossRef] [Green Version]
- Erqou, S.; Thompson, A.; Di Angelantonio, E.; Saleheen, D.; Kaptoge, S.; Marcovina, S.; Danesh, J. Apolipoprotein(a) isoforms and the risk of vascular disease: Systematic review of 40 studies involving 58,000 participants. J. Am. Coll. Cardiol. 2010, 55, 2160–2167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostner, K.M.; Kostner, G.M. Lipoprotein (a): A historical appraisal. J. Lipid Res. 2017, 58, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Fogacci, F.; Cicero, A.F.; D’Addato, S.; D’Agostini, L.; Rosticci, M.; Giovannini, M.; Bertagnin, E.; Borghi, C.; Brisighella Heart Study Group. Serum lipoprotein(a) level as long-term predictor of cardiovascular mortality in a large sample of subjects in primary cardiovascular prevention: Data from the Brisighella Heart Study. Eur. J. Intern. Med. 2017, 37, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Kuwabara, M.; Johnson, R.; Bove, M.; Fogacci, F.; Rosticci, M.; Giovannini, M.; D’Addato, S.; Borghi, C.; Brisighella Heart Study Group. LDL-oxidation, serum uric acid, kidney function and pulse-wave velocity: Data from the Brisighella Heart Study cohort. Int. J. Cardiol. 2018, 261, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Ferri, N.; Fogacci, F.; Rosticci, M.; Botta, M.; Marchiano, S.; Magni, P.; D’Addato, S.; Giovannini, M.; Borghi, C.; et al. Circulating Levels of Proprotein Convertase Subtilisin/Kexin Type 9 and Arterial Stiffness in a Large Population Sample: Data from the Brisighella Heart Study. J. Am. Heart Assoc. 2017, 6, e005764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Q.; Hu, M.J.; Cui, Y.J.; Liang, L.; Zhou, M.M.; Yang, Y.W.; Huang, F. Carotid-Femoral Pulse Wave Velocity in the Prediction of Cardiovascular Events and Mortality: An Updated Systematic Review and Meta-Analysis. Angiology 2018, 69, 617–629. [Google Scholar] [CrossRef]
- Parish, S.; Hopewell, J.C.; Hill, M.R.; Marcovina, S.; Valdes-Marquez, E.; Haynes, R.; Offer, A.; Pedersen, T.R.; Baigent, C.; Collins, R.; et al. Impact of Apolipoprotein(a) Isoform Size on Lipoprotein(a) Lowering in the HPS2-THRIVE Study. Circ. Genom. Precis. Med. 2018, 11, e001696. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Smaller Apo(a) Isoform Size (N. 511) | Larger Apo(a) Isoform Size (N. 467) | |||||
|---|---|---|---|---|---|---|
| Sex | Men | Women | Men | Women | ||
| 247 (53.5%) | 215 (46.5%) | 264 (51.2%) | 252 (48.8%) | |||
| Smoking habit | No-Smokers | Current smokers | Ex-smokers | No-Smokers | Current smokers | Ex-smokers |
| 278 (54.8%) | 131 (25.8%) | 98 (19.3%) | 269 (57.8%) | 119 (25.6%) | 77 (16.6%) | |
| Family history of early CVD | No | Yes | No | Yes | ||
| 480 (93.9%) | 31 (6.1%) | 432 (93.5%) | 35 (7.5%) | |||
| Parameters | Smaller Apo(a) Isoform Size (N. 511) | Larger Apo(a) Isoform Size (N. 467) | ||
|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | |
| Age (years) | 56.9 | 10.9 | 60.1 | 10.1 |
| Waist circumference (cm) | 91.8 | 14.0 | 92.8 | 12.9 |
| Body mass index (Kg/m2) | 26.6 | 4.5 | 26.9 | 4.6 |
| Systolic blood pressure (mmHg) | 137.4 | 11.3 | 142.8 * | 9.6 |
| Diastolic blood pressure (mmHg) | 73.1 | 5.2 | 73.8 | 4.8 |
| Heart Rate (bpm) | 63.3 | 12.1 | 63.7 | 11.0 |
| Aortic blood pressure (mmHg) | 134.4 | 10.6 | 139.8 * | 9.7 |
| Aortic pulse pressure (mmHg) | 60.20 | 8.7 | 63.7 | 10.2 |
| Augmentation Index | 24.3 | 9.8 | 26.0 | 8.1 |
| Cardiac output (L/min) | 6.6 | 2.3 | 7.2 | 2.3 |
| Stroke volume (mL) | 106.8 | 13.0 | 110.8 | 18.1 |
| Anke brachial index | 1.13 | 0.16 | 1.13 | 0.15 |
| Carotid femoral pulse wave velocity (m/s) | 9.39 | 1.68 | 8.49 * | 2.41 |
| Parameters | Smaller Apo(a) Isoform Size (N. 511) | Larger Apo(a) Isoform Size (N. 467) | ||
|---|---|---|---|---|
| Mean | Standard Deviation | Mean | Standard Deviation | |
| Fasting plasma glucose (mg/dL) | 94.6 | 15.0 | 96.6 | 15.1 |
| Total cholesterol (mg/dL) | 213.5 | 21.8 | 221.1 | 17.4 |
| Triglycerides (mg/dL) | 118.3 | 70.8 | 122.5 | 77.2 |
| HDL-cholesterol (mg/dL) | 52.9 | 5.3 | 52.2 | 5.6 |
| LDL-cholesterol (mg/dL) | 137.5 | 17.1 | 145.1 | 15.6 |
| Apolipoprotein B (mg/dL) | 89.6 | 20.6 | 92.7 | 19.5 |
| Apolipoprotein AI (mg/dL) | 155.5 | 28.4 | 155.7 | 26.9 |
| Lipoprotein (a) (mg/dL) | 34.4 | 6.4 | 29.5 * | 6.5 |
| Serum uric acid (mg/dL) | 5.2 | 1.3 | 5.2 | 1.2 |
| eGFR (mL/min) | 84.2 | 5.2 | 81.9 | 4.9 |
| Variables | Beta | RR | 95% Confidence Intervals | p | ||
|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||
| Entire cohort (N. 978) | ||||||
| Model 1 (R = 0.397) | Age | 0.397 | 0.254 | 0.146 | 0.362 | <0.001 |
| Model 2 (R = 0.423) | Age SBP | 0.312 0.170 | 0.242 0.118 | 0.133 0.111 | 0.352 0.125 | <0.001 <0.001 |
| Model 3 (R = 0.432) | Age SBP HDL-C | 0.338 0.182 −0.92 | 0.246 0.119 −0.114 | 0.137 0.112 −0.205 | 0.355 0.126 −0.024 | <0.001 <0.001 0.004 |
| Model 4 (R = 0.437) | Age SBP HDL-C TG | 0.337 0.178 −0.116 0.070 | 0.246 0.119 −0.118 0.103 | 0.136 0.112 −0.108 0.001 | 0.355 0.126 −0.029 0.005 | <0.001 <0.001 <0.001 0.027 |
| Model 5 (R = 441) | Age SBP HDL-C TG Sex (W versus M) | 0.347 0.180 −0.143 0.073 −0.64 | 0.247 0.119 −0.123 0.103 −0.027 | 0.138 0.112 −0.034 0.001 −0.054 | 0.057 0.026 −0.012 0.005 −0.010 | <0.001 <0.001 <0.001 0.022 0.042 |
| Smaller apo(a) isoform size (N. 511) | ||||||
| Model 1 (R = 0.404) | Age | 0.404 | 0.243 | 0.134 | 0.351 | <0.001 |
| Model 2 (R = 0.423) | Age SBP | 0.336 0.144 | 0.235 0.112 | 0.126 0.014 | 0.345 0.169 | 0.005 0.013 |
| Model 3 (R = 0.434) | Age SBP Sex (W versus M) | 0.342 0.135 −0.098 | 0.236 0.111 −0.331 | 0.127 0.004 −0.602 | 0.346 0.159 −0.060 | 0.004 0.017 <0.001 |
| Model 4 (R = 0.444) | Age SBP Sex (W versus M) HDL-C | 0.377 0.142 −0.135 −0.107 | 0.240 0.112 −0.457 −0.113 | 0.130 0.004 −0.748 −0.202 | 0.350 0.119 −0.167 −0.024 | <0.001 0.011 <0.001 0.002 |
| Larger apo(a) isoform size (N. 467) | ||||||
| Model 1 (R = 0.363) | Age | 0.363 | 0.207 | 0.144 | 0.372 | <0.001 |
| Model 2 (R = 0.397) | Age SBP | 0.271 0.185 | 0.208 0.106 | 0.128 0.011 | 0.359 0.235 | <0.001 <0.001 |
| Model 3 (R = 0.414) | Age SBP Sex (W versus M) | 0.302 0.205 −0.126 | 0.208 0.106 0.109 | 0.132 0.013 −0.241 | 0.364 0.168 −0.017 | <0.001 <0.001 0.004 |
| Model 4 (R = 0.423) | Age SBP Lp(a) Sex (W versus M) | 0.305 0.216 0.189 −0.134 | 0.208 0.106 0.103 0.109 | 0.133 0.015 0.012 −0.242 | 0.365 0.139 0.218 −0.011 | <0.001 <0.001 0.004 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicero, A.F.G.; Fogacci, F.; Derosa, G.; D’Angelo, A.; Ventura, F.; Rizzoli, E.; D’Addato, S.; Borghi, C.; on behalf of the Brisighella Heart Study Group. Lipoprotein(a) Serum Levels Predict Pulse Wave Velocity in Subjects in Primary Prevention for Cardiovascular Disease with Large Apo(a) Isoforms: Data from the Brisighella Heart Study. Biomedicines 2022, 10, 656. https://doi.org/10.3390/biomedicines10030656
Cicero AFG, Fogacci F, Derosa G, D’Angelo A, Ventura F, Rizzoli E, D’Addato S, Borghi C, on behalf of the Brisighella Heart Study Group. Lipoprotein(a) Serum Levels Predict Pulse Wave Velocity in Subjects in Primary Prevention for Cardiovascular Disease with Large Apo(a) Isoforms: Data from the Brisighella Heart Study. Biomedicines. 2022; 10(3):656. https://doi.org/10.3390/biomedicines10030656
Chicago/Turabian StyleCicero, Arrigo F. G., Federica Fogacci, Giuseppe Derosa, Angela D’Angelo, Fulvio Ventura, Elisabetta Rizzoli, Sergio D’Addato, Claudio Borghi, and on behalf of the Brisighella Heart Study Group. 2022. "Lipoprotein(a) Serum Levels Predict Pulse Wave Velocity in Subjects in Primary Prevention for Cardiovascular Disease with Large Apo(a) Isoforms: Data from the Brisighella Heart Study" Biomedicines 10, no. 3: 656. https://doi.org/10.3390/biomedicines10030656