
Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Patients
2.2. Angiography and Embolization Techniques
2.3. Study Objectives and Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
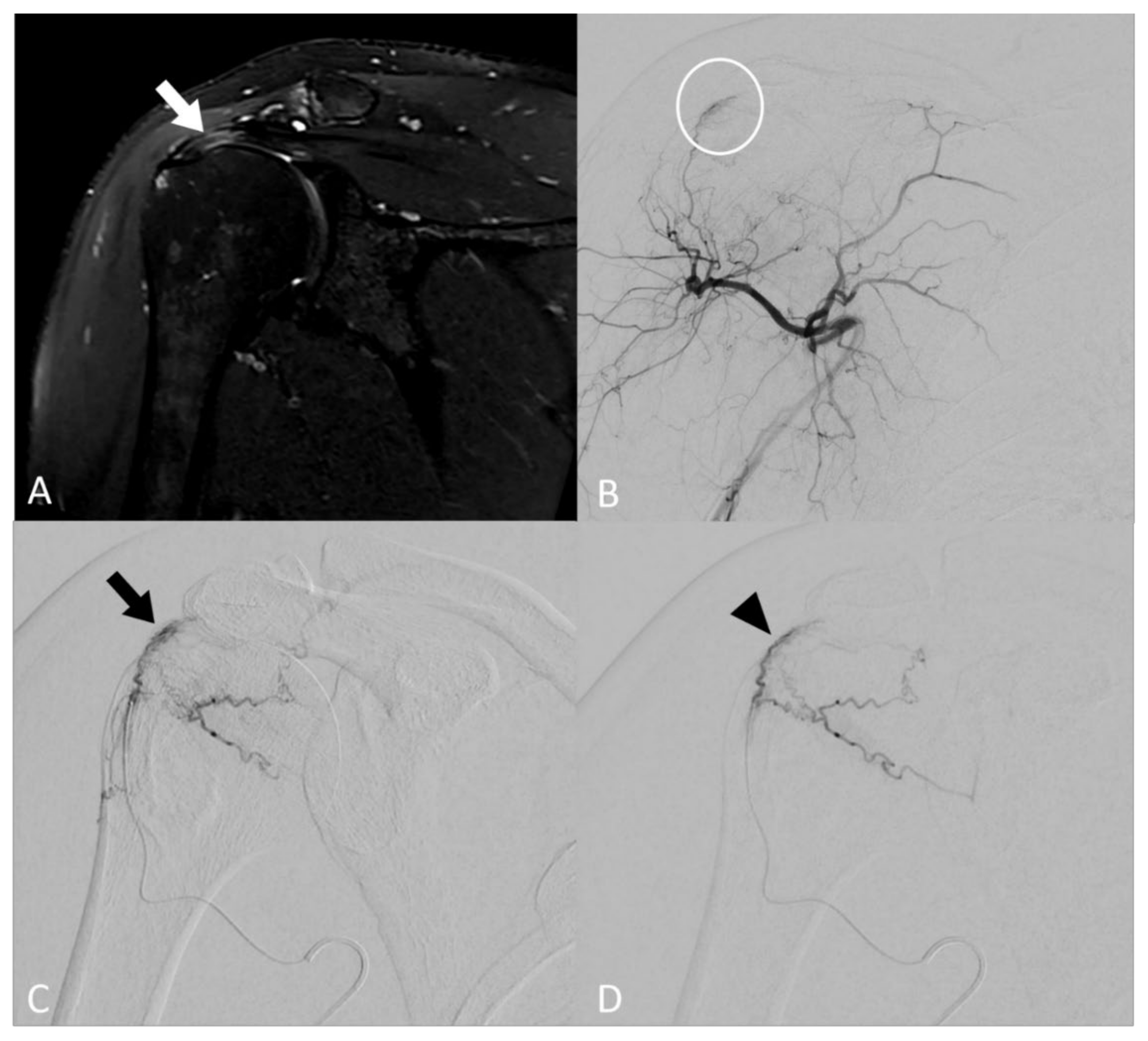
3.2. Angiographic Findings
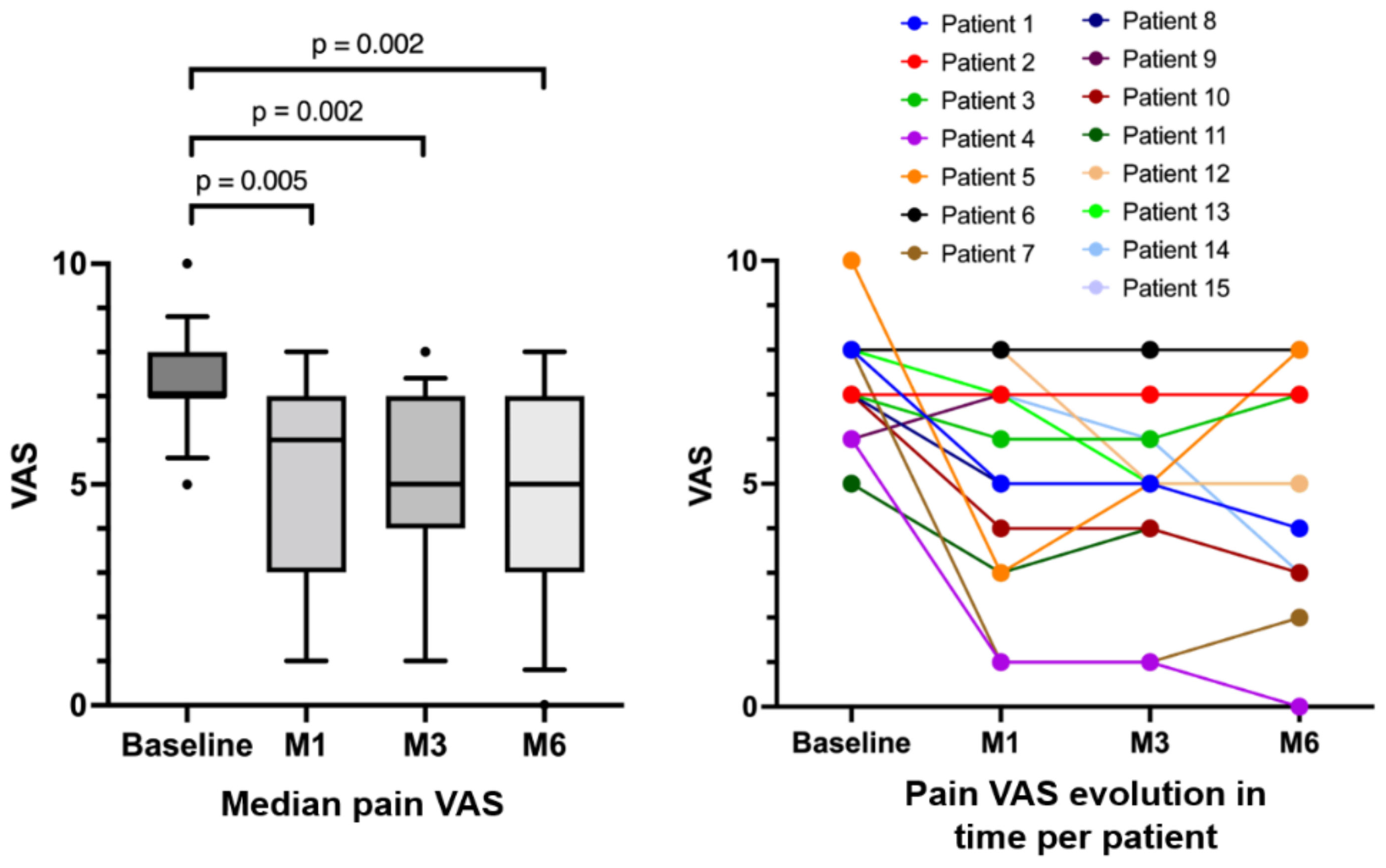
3.3. Efficacy
3.4. Safety
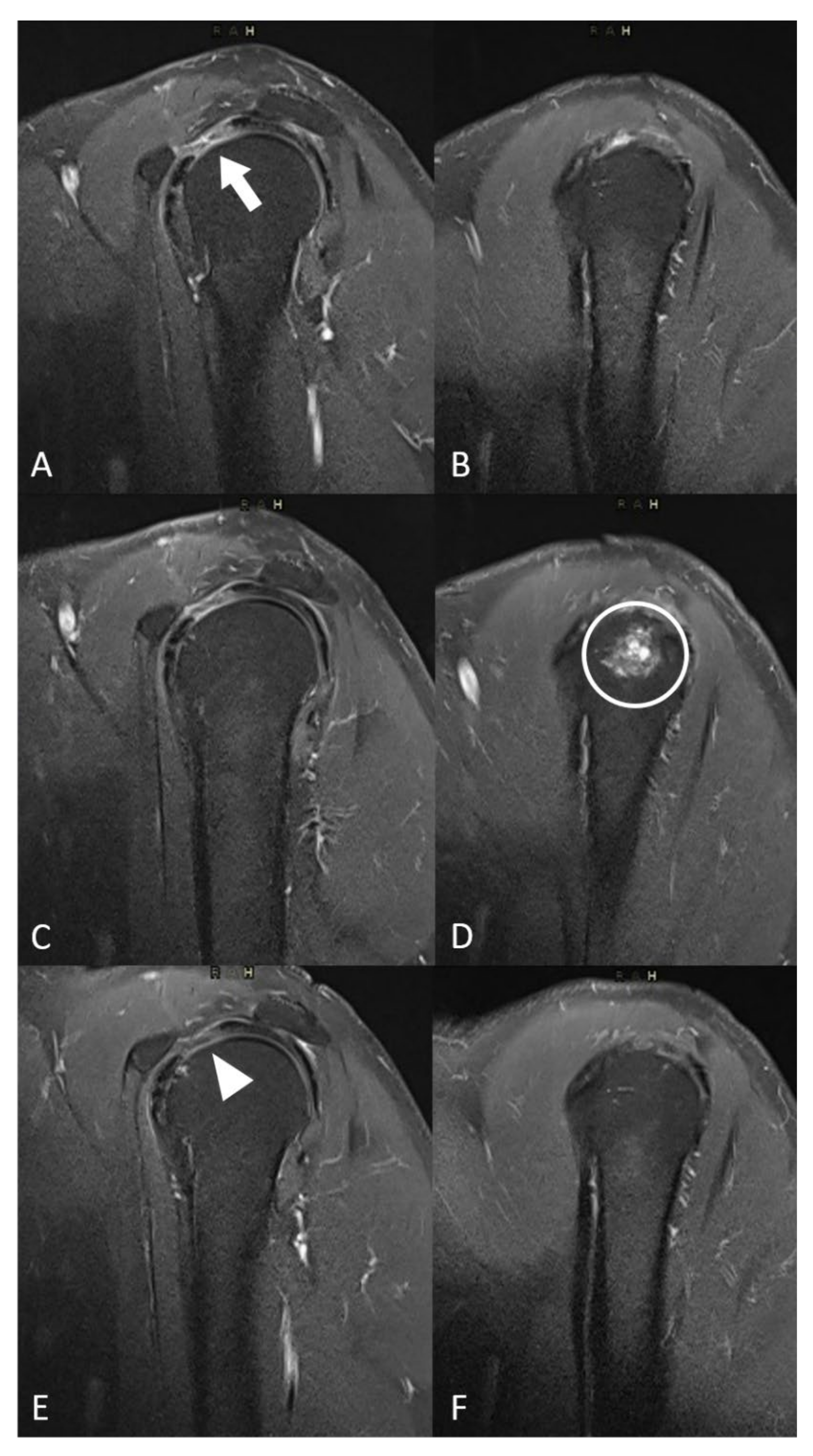
3.5. MRI Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Djade, C.D.; Porgo, T.V.; Zomahoun, H.T.V.; Perrault-Sullivan, G.; Dionne, C.E. Incidence of shoulder pain in 40 years old and over and associated factors: A systematic review. Eur. J. Pain 2020, 24, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Bodin, J.; Garlantézec, R.; Costet, N.; Descatha, A.; Viel, J.-F.; Roquelaure, Y. Risk Factors for Shoulder Pain in a Cohort of French Workers: A Structural Equation Model. Am. J. Epidemiol. 2017, 187, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Cheung, E.V.; Silverio, L.; Sperling, J.W. Strategies in Biologic Augmentation of Rotator Cuff Repair: A Review. Clin. Orthop. Relat. Res. 2010, 468, 1476–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangan, A.; Brealey, S.D.; Keding, A.; Corbacho, B.; Northgraves, M.; Kottam, L.; Goodchild, L.; Srikesavan, C.; Rex, S.; Charalambous, C.P.; et al. Management of adults with primary frozen shoulder in secondary care (UK FROST): A multicentre, pragmatic, three-arm, superiority randomised clinical trial. Lancet 2020, 396, 977–989. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.-H.; Bae, K.-C.; Kim, D.-H. Treatment Strategy for Frozen Shoulder. Clin. Orthop. Surg. 2019, 11, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Garving, C.; Jakob, S.; Bauer, I.; Nadjar, R.; Brunner, U.H. Impingement Syndrome of the Shoulder. Deutsches Ärzteblatt Int. 2017, 114, 765–776. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, B.; Tibone, J.E.; Kerlan, R.K. Frozen Shoulder. A Long-Term Follow-Up. J. Bone Jt. Surg. 1992, 74, 738–746. [Google Scholar]
- Redler, L.H.; Dennis, E.R. Treatment of Adhesive Capsulitis of the Shoulder. J. Am. Acad. Orthop. Surg. 2019, 27, e544–e554. [Google Scholar] [CrossRef]
- Forsgren, S.; Alfredson, H.; Öhberg, L. Is vasculo-neural ingrowth the cause of pain in chronic Achilles tendinosis? An Investigation Using Ultrasonography and Colour Doppler, Immunohistochemistry, and Diagnostic Injections. Knee Surg. Sports Traumatol. Arthrosc. 2003, 11, 334–338. [Google Scholar] [CrossRef]
- Bjur, D.; Alfredson, H.; Forsgren, S. The innervation pattern of the human Achilles tendon: Studies of the normal and tendinosis tendon with markers for general and sensory innervation. Cell Tissue Res. 2005, 320, 201–206. [Google Scholar] [CrossRef]
- Mapp, P.I.; Walsh, D.A. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Koucheki, R.; Dowling, K.I.; Patel, N.R.; Matsuura, N.; Mafeld, S. Characteristics of Imipenem/Cilastatin: Considerations for Musculoskeletal Embolotherapy. J. Vasc. Interv. Radiol. 2021, 32, 1040–1043.e1. [Google Scholar] [CrossRef]
- Alfredson, H.; Lorentzon, R. Sclerosing polidocanol injections of small vessels to treat the chronic painful tendon. Cardiovasc. Hematol. Agents Med. Chem. 2007, 5, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Okuno, Y.; Oguro, S.; Iwamoto, W.; Miyamoto, T.; Ikegami, H.; Matsumura, N. Short-term results of transcatheter arterial embolization for abnormal neovessels in patients with adhesive capsulitis: A pilot study. J. Shoulder Elb. Surg. 2014, 23, e199–e206. [Google Scholar] [CrossRef] [PubMed]
- Okuno, Y.; Matsumura, N.; Oguro, S. Transcatheter Arterial Embolization Using Imipenem/Cilastatin Sodium for Tendinopathy and Enthesopathy Refractory to Nonsurgical Management. J. Vasc. Interv. Radiol. 2013, 24, 787–792. [Google Scholar] [CrossRef]
- Fernández Martínez, A.M.; Baldi, S.; Alonso-Burgos, A.; López, R.; Vallejo-Pascual, M.E.; Cuesta Marcos, M.T.; Alonso, D.R.; Rodríguez Prieto, J.; Mauriz, J.L. Mid-Term Results of Transcatheter Arterial Embolization for Adhesive Capsulitis Resistant to Conservative Treatment. Cardiovasc. Interv. Radiol. 2021, 44, 443–451. [Google Scholar] [CrossRef]
- Inui, S.; Yoshizawa, S.; Shintaku, T.; Kaneko, T.; Ikegami, H.; Okuno, Y. Intra-Arterial Infusion of Imipenem/Cilastatin Sodium through a Needle Inserted into the Radial Artery as a New Treatment for Refractory Trapeziometacarpal Osteoarthritis. J. Vasc. Interv. Radiol. 2021, 32, 1341–1347. [Google Scholar] [CrossRef]
- Taguchi, H.; Tanaka, T.; Nishiofuku, H.; Fukuoka, Y.; Minamiguchi, K.; Taiji, R.; Takayama, K.; Takeda, M.; Hatakeyama, K.; Inoue, T.; et al. A Rat Model of Frozen Shoulder Demonstrating the Effect of Transcatheter Arterial Embolization on Angiography, Histopathology, and Physical Activity. J. Vasc. Interv. Radiol. 2021, 32, 376–383. [Google Scholar] [CrossRef]
- Woodhams, R.; Nishimaki, H.; Ogasawara, G.; Fujii, K.; Yamane, T.; Ishida, K.; Kashimi, F.; Matsunaga, K.; Takigawa, M. Imipenem/cilastatin sodium (IPM/CS) as an embolic agent for transcatheter arterial embolisation: A preliminary clinical study of gastrointestinal bleeding from neoplasms. SpringerPlus 2013, 2, 344. [Google Scholar] [CrossRef] [Green Version]
- Yamada, K.; Jahangiri, Y.; Li, J.; Gabr, A.; Anoushiravani, A.; Kumagai, K.; Uchida, B.; Farsad, K.; Horikawa, M. Embolic Characteristics of Imipenem-Cilastatin Particles in Vitro and in Vivo: Implications for Transarterial Embolization in Joint Arthropathies. J. Vasc. Interv. Radiol. 2021, 32, 1031–1039.e2. [Google Scholar] [CrossRef]
- Okuno, Y.; Korchi, A.M.; Shinjo, T.; Kato, S.; Kaneko, T. Midterm Clinical Outcomes and MR Imaging Changes after Transcatheter Arterial Embolization as a Treatment for Mild to Moderate Radiographic Knee Osteoarthritis Resistant to Conservative Treatment. J. Vasc. Interv. Radiol. 2017, 28, 995–1002. [Google Scholar] [CrossRef]
- Karam, G.; Chastre, J.; Wilcox, M.H.; Vincent, J.-L. Antibiotic strategies in the era of multidrug resistance. Crit. Care 2016, 20, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Shamy, T.; Amer, S.A.K.; Mohamed, A.A.; James, C.; Jayaprakasan, K. The impact of uterine artery embolization on ovarian reserve: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand 2019, 99, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Abt, D.; Mordasini, L.; Hechelhammer, L.; Kessler, T.M.; Schmid, H.-P.; Engeler, D.S. Prostatic artery embolization versus conventional TUR-P in the treatment of benign prostatic hyperplasia: Protocol for a prospective randomized non-inferiority trial. BMC Urol. 2014, 14, 94. [Google Scholar] [CrossRef] [Green Version]
- Kucukay, F.; Topcuoglu, O.M.; Alpar, A.; Altay, C.M.; Küçükay, M.B.; Ozbulbul, N.I. Bronchial Artery Embolization with Large Sized (700–900 µm) Tris-acryl Microspheres (Embosphere) for Massive Hemoptysis: Long-Term Results (Clinical Research). Cardiovasc. Interv. Radiol. 2018, 41, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Little, M.W.; Gibson, M.; Briggs, J.; Speirs, A.; Yoong, P.; Ariyanayagam, T.; Davies, N.; Tayton, E.; Tavares, S.; MacGill, S.; et al. Genicular artEry embolizatioN in patiEnts with oSteoarthrItiS of the Knee (GENESIS) Using Permanent Microspheres: Interim Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 931–940. [Google Scholar] [CrossRef]
- Bagla, S.; Piechowiak, R.; Hartman, T.; Orlando, J.; Del Gaizo, D.; Isaacson, A. Genicular Artery Embolization for the Treatment of Knee Pain Secondary to Osteoarthritis. J. Vasc. Interv. Radiol. 2020, 31, 1096–1102. [Google Scholar] [CrossRef]
- Hwang, J.H.; Park, S.W.; Kim, K.H.; Lee, S.J.; Oh, K.-S.; Chung, S.W.; Moon, S.G. Early Results of Transcatheter Arterial Embolization for Relief of Chronic Shoulder or Elbow Pain Associated with Tendinopathy Refractory to Conservative Treatment. J. Vasc. Interv. Radiol. 2018, 29, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Okuno, Y.; Iwamoto, W.; Matsumura, N.; Oguro, S.; Yasumoto, T.; Kaneko, T.; Ikegami, H. Clinical Outcomes of Transcatheter Arterial Embolization for Adhesive Capsulitis Resistant to Conservative Treatment. J. Vasc. Interv. Radiol. 2017, 28, 161–167.e1. [Google Scholar] [CrossRef]
- Filippiadis, D.K.; Binkert, C.; Pellerin, O.; Hoffmann, R.T.; Krajina, A.; Pereira, P.L. Cirse Quality Assurance Document and Standards for Classification of Complications: The Cirse Classification System. Cardiovasc. Interv. Radiol. 2017, 40, 1141–1146. [Google Scholar] [CrossRef]
- Szwedowski, D.; Łukasz, J.; Szwedowska, W.; Pękala, P.; Gagat, M. Neovascularization in Meniscus and Tendon Pathology as a Potential Mechanism in Regenerative Therapies: Special Reference to Platelet-Rich Plasma Treatment. Appl. Sci. 2021, 11, 8310. [Google Scholar] [CrossRef]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2021, 7, 1–21. [Google Scholar] [CrossRef]
- Casadaban, L.C.; Mandell, J.C.; Epelboym, Y. Genicular Artery Embolization for Osteoarthritis Related Knee Pain: A Systematic Review and Qualitative Analysis of Clinical Outcomes. Cardiovasc. Interv. Radiol. 2021, 44, 1–9. [Google Scholar] [CrossRef]
- Park, K.H.; Kim, D.H.; Jang, S.W.; Ryu, J.H.; Ko, K.Y. Treatment of Recurrent Hemarthrosis Following Total Knee Arthroplasty Using Surgical Interventions. Clin. Orthop. Surg. 2021, 13, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Cornman-Homonoff, J.; Kishore, S.A.; Waddell, B.S.; Kesler, J.; Mandl, L.A.; Westrich, G.H.; Potter, H.G.; Trost, D.W. Genicular Artery Embolization for Refractory Hemarthrosis following Total Knee Arthroplasty: Technique, Safety, Efficacy, and Patient-Reported Outcomes. J. Vasc. Interv. Radiol. 2021, 32, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, H.F.; Taqi, M.; Gillani, S.F.U.H.S.; Masood, F.; Ali, M. Comparison of Functional Outcome Between Intra-Articular Injection of Corticosteroid Versus Platelet-Rich Plasma in Frozen Shoulder: A Randomized Controlled Trial. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Mao, B.; Peng, R.; Zhang, Z.; Zhang, K.; Li, J.; Fu, W. The Effect of Intra-articular Injection of Hyaluronic Acid in Frozen Shoulder: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Orthop. Surg. Res. 2022, 17, 1–10. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hung, C.-Y.; Wu, W.-T.; Han, D.-S.; Yang, R.-S.; Lin, C.-P. Comparison of the Effectiveness of Suprascapular Nerve Block with Physical Therapy, Placebo, and Intra-Articular Injection in Management of Chronic Shoulder Pain: A Meta-Analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2016, 97, 1366–1380. [Google Scholar] [CrossRef]
- Torkian, P.; Golzarian, J.; Chalian, M.; Clayton, A.; Rahimi-Dehgolan, S.; Tabibian, E.; Talaie, R. Osteoarthritis-Related Knee Pain Treated with Genicular Artery Embolization: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211021356. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | N = 15 |
|---|---|
| Age (years), median (IQR) | 50.3 (46.7–54.5) |
| Gender, n (%) | |
| Female | 11 (73) |
| Male | 4 (27) |
| Nighttime pain, n (%) | 13 (87) |
| Limitation of joint amplitude, n (%) | 12 (80) |
| Limitation of daily life gestures, n (%) | 15 (100) |
| Occupational disease, n (%) | 6 (40) |
| Laterality, n (%) | |
| Right | 10 (67) |
| Left | 5 (33) |
| Surgical treatment before embolization, n (%) | 9 (60) |
| Pathology type, n (%) | |
| Adhesive capsulitis | 6 (40) |
| Tendinobursitis | 6 (40) |
| Both | 3 (20) |
| Duration of symptoms (months), median (IQR) | 26.6 (20.6–39.8) |
| Variables | N = 15 |
|---|---|
| Technical success, n (%) | 15 (100) |
| Number of treated arteries (by patient), median (IQR] | 2 (2–3] |
| Targeted arteries, n (%) | |
| Thoracoacromial artery | 8/35 (23) |
| Anterior circumflex humeral artery | 11/35 (31) |
| Posterior circumflex humeral artery | 9/35 (26) |
| Scapular circumflex artery | 7/35 (20) |
| Volume of diluted microspheres injected (mL), median (IQR) | 3.0 (2.4–3.5) |
| Homolateral radial access, n (%) | 14 (93) |
| Procedure duration (min), median (IQR) | 106.0 (91.0–114.5) |
| Scopy duration (min), median (IQR) | 32.1 (26.4–34.1) |
| Dose (Gy.cm2), median (IQR) | 15.6 (11.1–28.4) |
| Variables | N = 15 |
|---|---|
| Post-embolization syndrome, n (%) | 8 (53%) |
| Grade I * complications, n (%) | |
| Transient paraesthesia | 2 (13%) |
| Transient humeral osteo-medullary edema | 1 (7%) |
| Grade II * complications, n (%) | |
| Transient skin necrosis | 2 (13%) |
| Variables | N = 15 |
|---|---|
| Baseline imaging modality, n (%) | |
| Injected MRI | 13 (87%) |
| MRI without injection | 1 (7%) |
| Arthroscanner | 1 (7%) |
| Angiographic blushes correlated with baseline MRI contrast, n (%) | 11 (85%) |
| MRI follow-up, n (%) | 12/13 (92%) |
| MRI inflammatory signal decreased after embolization, n (%) | 9/12 (75%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gremen, E.; Frandon, J.; Lateur, G.; Finas, M.; Rodière, M.; Horteur, C.; Benassayag, M.; Thony, F.; Pailhe, R.; Ghelfi, J. Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients. Biomedicines 2022, 10, 744. https://doi.org/10.3390/biomedicines10040744
Gremen E, Frandon J, Lateur G, Finas M, Rodière M, Horteur C, Benassayag M, Thony F, Pailhe R, Ghelfi J. Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients. Biomedicines. 2022; 10(4):744. https://doi.org/10.3390/biomedicines10040744
Chicago/Turabian StyleGremen, Emeric, Julien Frandon, Gabriel Lateur, Mathieu Finas, Mathieu Rodière, Clément Horteur, Michaël Benassayag, Frédéric Thony, Régis Pailhe, and Julien Ghelfi. 2022. "Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients" Biomedicines 10, no. 4: 744. https://doi.org/10.3390/biomedicines10040744
APA StyleGremen, E., Frandon, J., Lateur, G., Finas, M., Rodière, M., Horteur, C., Benassayag, M., Thony, F., Pailhe, R., & Ghelfi, J. (2022). Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients. Biomedicines, 10(4), 744. https://doi.org/10.3390/biomedicines10040744