
Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options


Abstract
:1. Introduction and General Aspects
2. COVID-19 Vaccines
2.1. Vaccine Development and Approval
2.2. mRNA Vaccines
2.3. Recombinant Viral Vector Vaccines
3. Thrombotic Complications after COVID-19 Vaccination
4. The Pathogenesis of Vaccine-Induced Thrombotic Thrombocytopenia
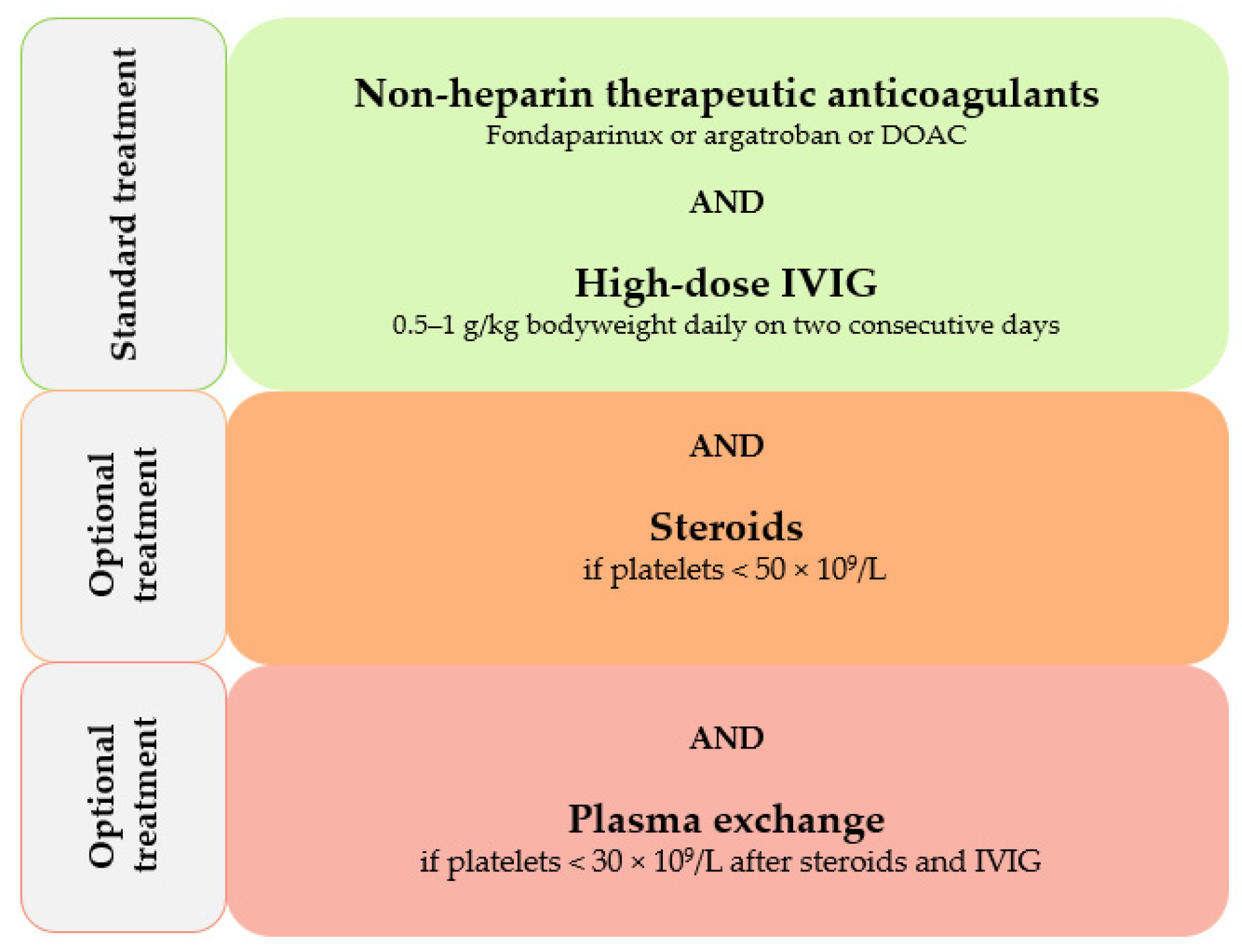
5. Diagnostic and Therapeutic Approaches in Vaccine-Induced Thrombotic Thrombocytopenia
6. Prevention of Thrombotic Complications after COVID-19 Vaccination
7. Recommendations for Vaccination in VITT Patients Post-Recovery
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castells, M.C.; Phillips, E.J. Maintaining Safety with SARS-CoV-2 Vaccines. N. Engl. J. Med. 2021, 384, e37. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.H.; Sorvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattor, T.H.; Tjonnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US Case Reports of Cerebral Venous Sinus Thrombosis With Thrombocytopenia After Ad26.COV2.S Vaccination, March 2 to April 21, 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef] [PubMed]
- Schulz, J.B.; Berlit, P.; Diener, H.C.; Gerloff, C.; Greinacher, A.; Klein, C.; Petzold, G.C.; Piccininni, M.; Poli, S.; Rohrig, R.; et al. COVID-19 Vaccine-Associated Cerebral Venous Thrombosis in Germany. Ann. Neurol. 2021, 90, 627–639. [Google Scholar] [CrossRef]
- Greinacher, A.; Selleng, K.; Warkentin, T.E. Autoimmune heparin-induced thrombocytopenia. J. Thromb. Haemost. 2017, 15, 2099–2114. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guidance for clinical Case Management of Thrombosis with Thrombocytopenia Syndome (TTS) Following Vaccination to Prevent Coronavirus Disease (COVID-19). Available online: https://apps.who.int/iris/bitstream/handle/10665/342999/WHO-2019-nCoV-TTS-2021.1-eng.pdf?sequence=1&isAllowed=y (accessed on 29 April 2022).
- Ropper, A.H.; Klein, J.P. Cerebral Venous Thrombosis. N. Engl. J. Med. 2021, 385, 59–64. [Google Scholar] [CrossRef]
- Stam, J. Thrombosis of the cerebral veins and sinuses. N. Engl. J. Med. 2005, 352, 1791–1798. [Google Scholar] [CrossRef] [Green Version]
- Warkentin, T.E.; Greinacher, A. Thrombosis of the cerebral veins and sinuses. N. Engl. J. Med. 2005, 353, 314–315. [Google Scholar] [CrossRef]
- Otite, F.O.; Patel, S.; Sharma, R.; Khandwala, P.; Desai, D.; Latorre, J.G.; Akano, E.O.; Anikpezie, N.; Izzy, S.; Malik, A.M.; et al. Trends in incidence and epidemiologic characteristics of cerebral venous thrombosis in the United States. Neurology 2020, 95, e2200–e2213. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.T.B.; Bobos, P.; Odutayo, A.; Pai, M. Meta-analysis of risk of vaccine-induced immune thrombocytopenia and thrombosis following ChAdOx1—A recombinant vaccine. MedRxiv 2021. [Google Scholar] [CrossRef]
- Spanish Agency of Medicine and Healthcare Products. Pharmacovigilance Report, Published on 9 April 2021. Available online: https://www.aemps.gob.es/acciones-informativas/boletines-de-la-aemps/boletin-mensual-de-farmacovigilancia (accessed on 29 April 2022).
- Center for Disease Control and Prevention. National Center for Immunization & Respiratory Diseases. Update: Thrombosis with Thrombocytopenia Syndrome (TTS) Following COVID-19 Vaccination. Available online: https://www.cdc.gov/vaccines/ACIP/meetings/downloads/slides-2021-05-12/07-COVID-Shimabukuro-508.pdf (accessed on 29 April 2022).
- European Medicines Agency. 29 March 2021 Update. COVID-19 Vaccine Safety Update VAXZEVRIA AstraZeneca AB. Available online: https://www.ema.europa.eu/en/documents/covid-19-vaccine-safety-update/covid-19-vaccinesafety-update-vaxzevria-previously-covid-19-vaccine-astrazeneca-29-march-2021_en.pdf (accessed on 29 April 2022).
- European Medicines Agency. COVID-19 Vaccine Janssen: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets. 20 April 2021. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 29 April 2022).
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 19 May 2022).
- Dedicated COVID-19 Vaccination Dashboard. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 19 May 2022).
- European Centre for Disease Prevention and Control (ECDC). COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/covid-19/vaccine-tracker.html#distribution-tab (accessed on 19 May 2022).
- Our World In Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 19 May 2022).
- Kandimalla, R.; Chakraborty, P.; Vallamkondu, J.; Chaudhary, A.; Samanta, S.; Reddy, P.H.; De Feo, V.; Dewanjee, S. Counting on COVID-19 Vaccine: Insights into the Current Strategies, Progress and Future Challenges. Biomedicines 2021, 9, 1740. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Coronovirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines?gclid=Cj0KCQjw-JyUBhCuARIsANUqQ_JQix8FzcHYwqzqQWMmGAlmXs2xWFZ4lCPfRRcGiypTeXHVba33d1EaAkbmEALw_wcB&topicsurvey=v8kj13) (accessed on 20 May 2022).
- European Medicines Agency (EMA). COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/covid-19-vaccines (accessed on 20 May 2022).
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Lee, S.S. From COVID-19 to Cancer mRNA Vaccines: Moving From Bench to Clinic in the Vaccine Landscape. Front. Immunol. 2021, 12, 679344. [Google Scholar] [CrossRef]
- World Health Organizsation (WHO). The Pfizer BioNTech (BNT162b2) COVID-19 Vaccine: What You Need To Know. Available online: https://www.who.int/news-room/feature-stories/detail/who-can-take-the-pfizer-biontech-covid-19--vaccine (accessed on 29 April 2022).
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Humphreys, I.R.; Sebastian, S. Novel viral vectors in infectious diseases. Immunology 2018, 153, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Connors, M.; Graham, B.S.; Lane, H.C.; Fauci, A.S. SARS-CoV-2 Vaccines: Much Accomplished, Much to Learn. Ann. Intern. Med. 2021, 174, 687–690. [Google Scholar] [CrossRef]
- Kaur, S.P.; Gupta, V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020, 288, 198114. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The Janssen Ad26.COV2.S COVID-19 Vaccine: What You Need To Know. Available online: https://www.who.int/news-room/feature-stories/detail/the-j-j-covid-19-vaccine-what-you-need-to-know (accessed on 29 April 2022).
- Franchini, M.; Testa, S.; Pezzo, M.; Glingani, C.; Caruso, B.; Terenziani, I.; Pognani, C.; Bellometti, S.A.; Castelli, G. Cerebral venous thrombosis and thrombocytopenia post-COVID-19 vaccination. Thromb. Res. 2021, 202, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Liumbruno, G.M.; Pezzo, M. COVID-19 vaccine-associated immune thrombosis and thrombocytopenia (VITT): Diagnostic and therapeutic recommendations for a new syndrome. Eur. J. Haematol. 2021, 107, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Krzywicka, K.; Heldner, M.R.; Sanchez van Kammen, M.; van Haaps, T.; Hiltunen, S.; Silvis, S.M.; Levi, M.; Kremer Hovinga, J.A.; Jood, K.; Lindgren, E.; et al. Post-SARS-CoV-2-vaccination cerebral venous sinus thrombosis: An analysis of cases notified to the European Medicines Agency. Eur. J. Neurol. 2021, 28, 3656–3662. [Google Scholar] [CrossRef]
- Rosenthal, M.A.; Rischin, D.; McArthur, G.; Ribbons, K.; Chong, B.; Fareed, J.; Toner, G.; Green, M.D.; Basser, R.L. Treatment with the novel anti-angiogenic agent PI-88 is associated with immune-mediated thrombocytopenia. Ann. Oncol. 2002, 13, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Tardy-Poncet, B.; Tardy, B.; Grelac, F.; Reynaud, J.; Mismetti, P.; Bertrand, J.C.; Guyotat, D. Pentosan polysulfate-induced thrombocytopenia and thrombosis. Am. J. Hematol. 1994, 45, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.R.; Wang, Y.; Weil, E.L.; Padmanabhan, A.; Warkentin, T.E.; Pruthi, R.K. Cerebral venous sinus thrombosis associated with spontaneous heparin-induced thrombocytopenia syndrome after total knee arthroplasty. Platelets 2021, 32, 936–940. [Google Scholar] [CrossRef]
- Jay, R.M.; Warkentin, T.E. Fatal heparin-induced thrombocytopenia (HIT) during warfarin thromboprophylaxis following orthopedic surgery: Another example of ‘spontaneous’ HIT? J. Thromb. Haemost. 2008, 6, 1598–1600. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Basciano, P.A.; Knopman, J.; Bernstein, R.A. Spontaneous heparin-induced thrombocytopenia syndrome: 2 new cases and a proposal for defining this disorder. Blood 2014, 123, 3651–3654. [Google Scholar] [CrossRef] [Green Version]
- Warkentin, T.E.; Makris, M.; Jay, R.M.; Kelton, J.G. A spontaneous prothrombotic disorder resembling heparin-induced thrombocytopenia. Am. J. Med. 2008, 121, 632–636. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Greinacher, A. Spontaneous HIT syndrome: Knee replacement, infection, and parallels with vaccine-induced immune thrombotic thrombocytopenia. Thromb. Res. 2021, 204, 40–51. [Google Scholar] [CrossRef]
- Salih, F.; Schonborn, L.; Kohler, S.; Franke, C.; Mockel, M.; Dorner, T.; Bauknecht, H.C.; Pille, C.; Graw, J.A.; Alonso, A.; et al. Vaccine-Induced Thrombocytopenia with Severe Headache. N. Engl. J. Med. 2021, 385, 2103–2105. [Google Scholar] [CrossRef] [PubMed]
- Nazi, I.; Arnold, D.M.; Warkentin, T.E.; Smith, J.W.; Staibano, P.; Kelton, J.G. Distinguishing between anti-platelet factor 4/heparin antibodies that can and cannot cause heparin-induced thrombocytopenia. J. Thromb. Haemost. 2015, 13, 1900–1907. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, A.; Jones, C.G.; Curtis, B.R.; Bougie, D.W.; Sullivan, M.J.; Peswani, N.; McFarland, J.G.; Eastwood, D.; Wang, D.; Aster, R.H. A Novel PF4-Dependent Platelet Activation Assay Identifies Patients Likely to Have Heparin-Induced Thrombocytopenia/Thrombosis. Chest 2016, 150, 506–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, D.; Liu, Y.; Shayakhmetov, D.; Li, Z.Y.; Ni, S.; Lieber, A. Adenovirus-platelet interaction in blood causes virus sequestration to the reticuloendothelial system of the liver. J. Virol. 2007, 81, 4866–4871. [Google Scholar] [CrossRef] [Green Version]
- Othman, M.; Labelle, A.; Mazzetti, I.; Elbatarny, H.S.; Lillicrap, D. Adenovirus-induced thrombocytopenia: The role of von Willebrand factor and P-selectin in mediating accelerated platelet clearance. Blood 2007, 109, 2832–2839. [Google Scholar] [CrossRef]
- Lopez Yomayuza, C.C.; Preissner, K.T.; Lorenz, B.; Stieger, K. Optimizing Measurement of Vascular Endothelial Growth Factor in Small Blood Samples of Premature Infants. Sci. Rep. 2019, 9, 6744. [Google Scholar] [CrossRef]
- Rauova, L.; Zhai, L.; Kowalska, M.A.; Arepally, G.M.; Cines, D.B.; Poncz, M. Role of platelet surface PF4 antigenic complexes in heparin-induced thrombocytopenia pathogenesis: Diagnostic and therapeutic implications. Blood 2006, 107, 2346–2353. [Google Scholar] [CrossRef]
- Greinacher, A.; Selleng, K.; Palankar, R.; Wesche, J.; Handtke, S.; Wolff, M.; Aurich, K.; Lalk, M.; Methling, K.; Volker, U.; et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood 2021, 138, 2256–2268. [Google Scholar] [CrossRef]
- Lubenow, N.; Hinz, P.; Thomaschewski, S.; Lietz, T.; Vogler, M.; Ladwig, A.; Junger, M.; Nauck, M.; Schellong, S.; Wander, K.; et al. The severity of trauma determines the immune response to PF4/heparin and the frequency of heparin-induced thrombocytopenia. Blood 2010, 115, 1797–1803. [Google Scholar] [CrossRef]
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nat. Rev. Immunol. 2020, 20, 95–112. [Google Scholar] [CrossRef]
- Dias, L.; Soares-Dos-Reis, R.; Meira, J.; Ferrao, D.; Soares, P.R.; Pastor, A.; Gama, G.; Fonseca, L.; Fagundes, V.; Carvalho, M. Cerebral Venous Thrombosis after BNT162b2 mRNA SARS-CoV-2 vaccine. J. Stroke Cerebrovasc. Dis. 2021, 30, 105906. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Bourguignon, A.; Arnold, D.M.; Warkentin, T.E.; Smith, J.W.; Pannu, T.; Shrum, J.M.; Al Maqrashi, Z.A.A.; Shroff, A.; Lessard, M.C.; Blais, N.; et al. Adjunct Immune Globulin for Vaccine-Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 385, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Warkentin, T.E. High-dose intravenous immunoglobulin for the treatment and prevention of heparin-induced thrombocytopenia: A review. Expert Rev. Hematol. 2019, 12, 685–698. [Google Scholar] [CrossRef]
- Oldenburg, J.; Klamroth, R.; Langer, F.; Albisetti, M.; von Auer, C.; Ay, C.; Korte, W.; Scharf, R.E.; Potzsch, B.; Greinacher, A. Diagnosis and Management of Vaccine-Related Thrombosis following AstraZeneca COVID-19 Vaccination: Guidance Statement from the GTH. Hamostaseologie 2021, 41, 184–189. [Google Scholar] [CrossRef]
- Mohanty, E.; Nazir, S.; Sheppard, J.I.; Forman, D.A.; Warkentin, T.E. High-dose intravenous immunoglobulin to treat spontaneous heparin-induced thrombocytopenia syndrome. J. Thromb. Haemost. 2019, 17, 841–844. [Google Scholar] [CrossRef]
- Graf, T.; Thiele, T.; Klingebiel, R.; Greinacher, A.; Schabitz, W.R.; Greeve, I. Immediate high-dose intravenous immunoglobulins followed by direct thrombin-inhibitor treatment is crucial for survival in Sars-Covid-19-adenoviral vector vaccine-induced immune thrombotic thrombocytopenia VITT with cerebral sinus venous and portal vein thrombosis. J. Neurol. 2021, 268, 4483–4485. [Google Scholar] [CrossRef]
- Guetl, K.; Gary, T.; Raggam, R.B.; Schmid, J.; Wolfler, A.; Brodmann, M. SARS-CoV-2 vaccine-induced immune thrombotic thrombocytopenia treated with immunoglobulin and argatroban. Lancet 2021, 397, e19. [Google Scholar] [CrossRef]
- Gattringer, T.; Gressenberger, P.; Gary, T.; Wolfler, A.; Kneihsl, M.; Raggam, R.B. Successful management of vaccine-induced immune thrombotic thrombocytopenia-related cerebral sinus venous thrombosis after ChAdOx1 nCov-19 vaccination. Stroke Vasc. Neurol. 2022, 7, 86–88. [Google Scholar] [CrossRef]
- International Society on Thrombosis and Hemostasis (ISTH) Interim Guidance for the Diagnosis and Treatment on Vaccine-Induced Immune Thrombotic Thrombocytopenia. Available online: https://cdn.ymaws.com/www.isth.org/resource/resmgr/ISTH_VITT_Guidance_2.pdf (accessed on 29 April 2022).
- Greinacher, A.; Langer, F.; Makris, M.; Pai, M.; Pavord, S.; Tran, H.; Warkentin, T.E. Vaccine-induced immune thrombotic thrombocytopenia (VITT): Update on diagnosis and management considering different resources: Response to Comment from Yamada. J. Thromb. Haemost. 2022, 20, 542–543. [Google Scholar] [CrossRef]
- Schonborn, L.; Thiele, T.; Kaderali, L.; Greinacher, A. Decline in Pathogenic Antibodies over Time in VITT. N. Engl. J. Med. 2021, 385, 1815–1816. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (First) | Cases (n) | Females n (%) | Age <60 y n (%) | Events (n) | Site of Thrombosis | Thrombo- Cytopenia <150 × 109/L | Anti-PF4 Antibodies Positive | |||
|---|---|---|---|---|---|---|---|---|---|---|
| CVT n (%) | SVT n (%) | VTE n (%) | Others n (%) | |||||||
| Greinacher et al. [2] | 11 | 9 (81.8%) | 9 (81.8%) * | 19 † | 9 (47.4) | 3 (15.8%) | 3 (15.8%) | 4 (21.1%) | 10 (90.9%) † | 9 (81.8%) * |
| Schultz et al. [3] | 5 | 4 (80%) | 5 (100%) | 5 | 4 (80%) | 1 (20%) | 0 /0%) | 0 (0%) | 5 (100%) | 5 (100%) |
| Franchini et al. [34] | 1 | 0 (0%) | 1 (100%) | 1 | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (100%) | 1 (100%) |
| Scully et al. [4] | 23 | 14 (60.8%) | 19 (82.6%) | 29 | 13 (44.8%) | 3 (10.3%) | 7 (24.1%) | 6 (20.7%) | 22 (95.7%) † | 21 (91.3%) † |
| See et al. [5] | 12 | 12 (100%) | 12 (100%) | 25 | 12 (48%) | 2 (8%) | 5 (20%) | 6 (24%) | 12 (100%) | 12 (100%) |
| Total | 52 | 39 (75%) | 46 (88.5%) | 79 | 39 (49.4%) | 9 (11.4%) | 15 (19%) | 16 (20.3%) | 50 (96.2%) | 48 (92.3%) |
| Thrombosis Location | Signs and Symptoms |
|---|---|
| suggestive of cerebral venous thrombosis | severe persistent headache |
| +/− vision change | |
| +/− seizure-like activity | |
| suggestive of splanchnic vein thrombosis | severe persistent abdominal pain |
| suggestive of deep vein thrombosis | leg pain and/or swelling |
| suggestive of pulmonary embolism | chest pain and/or shortness of breath |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guetl, K.; Raggam, R.B.; Gary, T. Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options. Biomedicines 2022, 10, 1246. https://doi.org/10.3390/biomedicines10061246
Guetl K, Raggam RB, Gary T. Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options. Biomedicines. 2022; 10(6):1246. https://doi.org/10.3390/biomedicines10061246
Chicago/Turabian StyleGuetl, Katharina, Reinhard Bernd Raggam, and Thomas Gary. 2022. "Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options" Biomedicines 10, no. 6: 1246. https://doi.org/10.3390/biomedicines10061246
APA StyleGuetl, K., Raggam, R. B., & Gary, T. (2022). Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options. Biomedicines, 10(6), 1246. https://doi.org/10.3390/biomedicines10061246