
Platelet-Rich Plasma in Alopecia Areata—A Steroid-Free Treatment Modality: A Systematic Review and Meta-Analysis of Randomized Clinical Trials

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Eligibility Criteria
2.2. Study Selection and Data Collection
2.3. Quality Assessment and Quality of Evidence
2.4. Data Synthesis and Analysis
3. Results
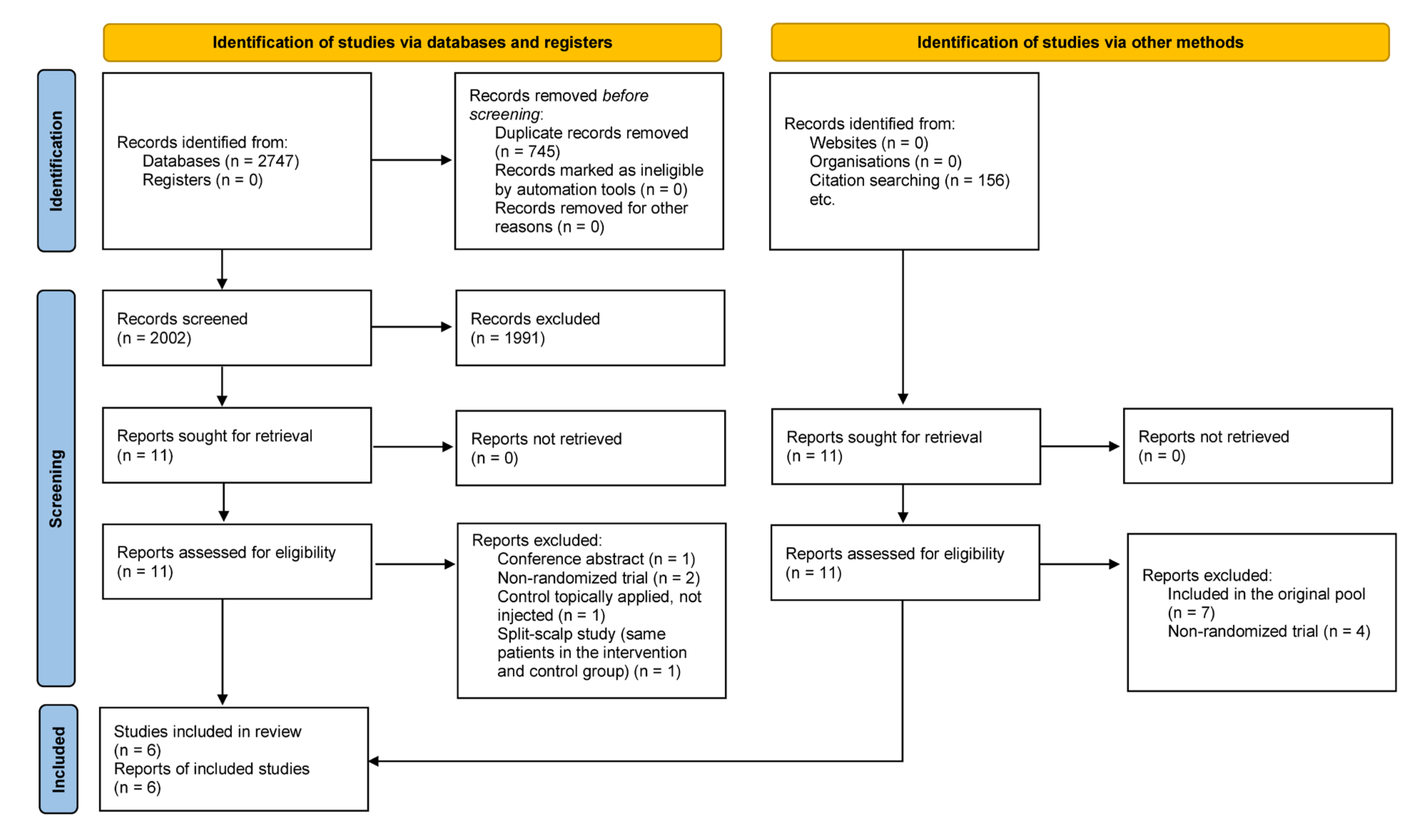
3.1. Search and Selection
3.2. Main Characteristics of the Included Studies
3.3. Primary Outcome (SALT score)
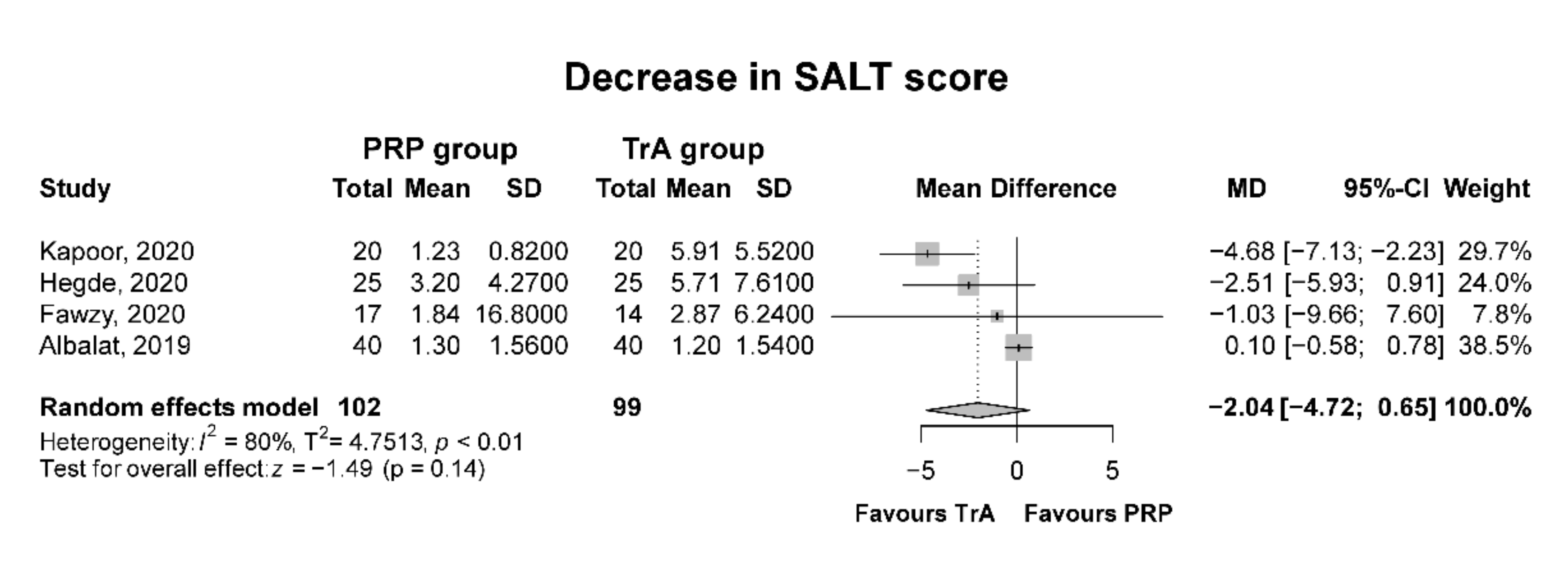
3.3.1. PRP Compared to Triamcinolone Acetonide
3.3.2. PRP Compared to Placebo
3.4. Secondary Outcomes
3.4.1. Patient Safety
Adverse Effects
Administration-Related Pain
Recurrence Rates
3.5. Risk of Bias Assessment
3.6. Quality of Evidence
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Research
4.3. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertolini, M.; McElwee, K.; Gilhar, A.; Bulfone-Paus, S.; Paus, R. Hair follicle immune privilege and its collapse in alopecia areata. Exp. Dermatol. 2020, 29, 703–725. [Google Scholar] [CrossRef] [PubMed]
- Rencz, F.; Gulácsi, L.; Péntek, M.; Wikonkál, N.; Baji, P.; Brodszky, V. Alopecia areata and health-related quality of life: A systematic review and meta-analysis. Br. J. Dermatol. 2016, 175, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Pratt, C.H.; King, L.E., Jr.; Messenger, A.G.; Christiano, A.M.; Sundberg, J.P. Alopecia areata. Nat. Rev. Dis. Primers 2017, 3, 17011. [Google Scholar] [CrossRef] [Green Version]
- Fukumoto, T.; Fukumoto, R.; Magno, E.; Oka, M.; Nishigori, C.; Horita, N. Treatments for alopecia areata: A systematic review and network meta-analysis. Dermatol. Ther. 2021, 34, e14916. [Google Scholar] [CrossRef]
- Messenger, A.G.; McKillop, J.; Farrant, P.; McDonagh, A.J.; Sladden, M. British association of dermatologists’ guidelines for the management of alopecia areata 2012. Br. J. Dermatol. 2012, 166, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Meah, N.; Wall, D.; York, K.; Bhoyrul, B.; Bokhari, L.; Sigall, D.A.; Bergfeld, W.F.; Betz, R.C.; Blume-Peytavi, U.; Callender, V.; et al. The alopecia areata consensus of experts (ace) study: Results of an international expert opinion on treatments for alopecia areata. J. Am. Acad. Dermatol. 2020, 83, 123–130. [Google Scholar] [CrossRef]
- Contento, M.; Cline, A.; Russo, M. Steroid phobia: A review of prevalence, risk factors, and interventions. Am. J. Clin. Dermatol. 2021, 22, 837–851. [Google Scholar] [CrossRef]
- Hesseler, M.J.; Shyam, N. Platelet-rich plasma and its utility in the treatment of acne scars: A systematic review. J. Am. Acad. Dermatol. 2019, 80, 1730–1745. [Google Scholar] [CrossRef] [PubMed]
- Qu, W.; Wang, Z.; Hunt, C.; Morrow, A.S.; Urtecho, M.; Amin, M.; Shah, S.; Hasan, B.; Abd-Rabu, R.; Ashmore, Z.; et al. The effectiveness and safety of platelet-rich plasma for chronic wounds: A systematic review and meta-analysis. Mayo Clin. Proc. 2021, 96, 2407–2417. [Google Scholar] [CrossRef]
- Gupta, A.K.; Cole, J.; Deutsch, D.P.; Everts, P.A.; Niedbalski, R.P.; Panchaprateep, R.; Rinaldi, F.; Rose, P.T.; Sinclair, R.; Vogel, J.E.; et al. Platelet-rich plasma as a treatment for androgenetic alopecia. Dermatol. Surg. 2019, 45, 1262–1273. [Google Scholar] [CrossRef] [Green Version]
- El-Husseiny, R.; Saleh, H.; Moustafa, A.; Salem, S. Comparison between single- versus double-spin prepared platelet-rich plasma injection in treatment of female pattern hair loss: Clinical effect and relation to vascular endothelial growth factor. Arch. Dermatol. Res. 2021, 313, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Salem, S.A.; Elhusseiny, R.M.; Saleh, H.M. A split scalp study of single versus double spin platelet-rich plasma injections in treatment of female pattern hair loss: Clinical effect and relation to vascular endothelial growth factor in prp. QJM Int. J. Med. 2021, 114, 557–566. [Google Scholar] [CrossRef]
- Li, Z.J.; Choi, H.I.; Choi, D.K.; Sohn, K.C.; Im, M.; Seo, Y.J.; Lee, Y.H.; Lee, J.H.; Lee, Y. Autologous platelet-rich plasma: A potential therapeutic tool for promoting hair growth. Dermatol. Surg. 2012, 38, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.A.; Roberts, J.; Sperling, L.; Tosti, A.; Shapiro, J.; McMichael, A.; Bergfeld, W.; Callender, V.; Mirmirani, P.; Washenik, K.; et al. Objective outcome measures: Collecting meaningful data on alopecia areata. J. Am. Acad. Dermatol. 2018, 79, 470–478.e3. [Google Scholar] [CrossRef]
- Albalat, W.; Ebrahim, H.M. Evaluation of platelet-rich plasma vs intralesional steroid in treatment of alopecia areata. J. Cosmet. Dermatol. 2019, 18, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, A.; Joy, B.; Thyvalappil, A.; Mathew, P.; Sreenivasan, A.; Sridharan, R. A comparative study of therapeutic response to intralesional injections of platelet-rich plasma versus triamcinolone acetonide in alopecia areata. Indian Dermatol. Online J. 2020, 11, 920–924. [Google Scholar]
- Fawzy, M.M.; Hay, R.A.; Mohammed, F.N.; Sayed, K.S.; Ghanem, M.E.D.; Ezzat, M. Trichoscopy as an evaluation method for alopecia areata treatment: A comparative study. J. Cosmet. Dermatol. 2021, 20, 1827–1836. [Google Scholar] [CrossRef] [PubMed]
- Hegde, P.; Relhan, V.; Sahoo, B.; Garg, V.K. A randomized, placebo and active controlled, split scalp study to evaluate the efficacy of platelet-rich plasma in patchy alopecia areata of the scalp. Dermatol. Ther. 2020, 33, e14388. [Google Scholar] [CrossRef]
- Kapoor, P.; Kumar, S.; Brar, B.K.; Kukar, N.; Arora, H.; Brar, S.K. Comparative evaluation of therapeutic efficacy of intralesional injection of triamcinolone acetonide versus intralesional autologous platelet-rich plasma injection in alopecia areata. J. Cutan. Aesthet. Surg. 2020, 13, 103–111. [Google Scholar]
- Trink, A.; Sorbellini, E.; Bezzola, P.; Rodella, L.; Rezzani, R.; Ramot, Y.; Rinaldi, F. A randomized, double-blind, placebo- and active-controlled, half-head study to evaluate the effects of platelet-rich plasma on alopecia areata. Br. J. Dermatol. 2013, 169, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.; Hopewell, S. Cochrane methods—Twenty years experience in developing systematic review methods. Syst. Rev. 2013, 2, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. Rob 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schünemann, H.J.; Vist, G.E.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H. Chapter 14: Completing ‘summary of findings’ tables and grading the certainty of the evidence. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3 (Updated February 2022); Higgins, J.P.T., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Oxford, UK, 2022; Available online: http://www.training.cochrane.org/handbook (accessed on 1 March 2022).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing meta-Analysis with R: A Hands-On Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Chu, T.W.; AlJasser, M.; Alharbi, A.; Abahussein, O.; McElwee, K.; Shapiro, J. Benefit of different concentrations of intralesional triamcinolone acetonide in alopecia areata: An intrasubject pilot study. J. Am. Acad. Dermatol. 2015, 73, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Rajan, M.B.; Bhardwaj, A.; Singh, S.; Budania, A.; Bains, A.; Thirunavukkarasu, P.; Kumar, M.P. Identification of novel step-up regimen of intralesional triamcinolone acetonide in scalp alopecia areata based on a double-blind randomized controlled trial. Dermatol. Ther. 2021, 34, e14555. [Google Scholar] [CrossRef] [PubMed]
- Ragab, S.E.M.; Nassar, S.O.; Morad, H.A.; Hegab, D.S. Platelet-rich plasma in alopecia areata: Intradermal injection versus topical application with transepidermal delivery via either fractional carbon dioxide laser or microneedling. Acta Dermatovenerol. Alp. Pannonica Adriat. 2020, 29, 169–173. [Google Scholar] [CrossRef]
- Maisel-Campbell, A.L.; Ismail, A.; Reynolds, K.A.; Poon, E.; Serrano, L.; Grushchak, S.; Farid, C.; West, D.P.; Alam, M. A systematic review of the safety and effectiveness of platelet-rich plasma (prp) for skin aging. Arch. Dermatol. Res. 2020, 312, 301–315. [Google Scholar] [CrossRef]
- Pototschnig, H.; Madl, M.T. Successful treatment of alopecia areata barbae with platelet-rich plasma. Cureus 2020, 12, e7495. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| First Author, Year of Publication | Country | Study Design | Number of Patients | Intervention | Control | Administration | Timepoints of Evaluation (weeks) a |
| Studies included in meta-analysis | |||||||
| Albalat, 2019 [15] | Egypt | RCT | 80 | PRP injection (double-spin method) | TrA injection (5 mg/mL) | 3–5 sessions, 2-week intervals | 12 |
| Fawzy, 2020 [17] | Egypt | RCT | 31 | PRP injection (single-spin method) | TrA injection (5 mg/mL) | 3 sessions, 4-week intervals | 12 |
| Hegde, 2020 [18] | India | RCT | 50 | PRP injection (double-spin method) | TrA injection (10 mg/mL), placebo | 3 sessions, 4-week intervals | 16 |
| Kapoor, 2020 [19] | India | RCT | 40 | PRP injection (single-spin method) | TrA injection (10 mg/mL) | 4 sessions, 3-week intervals | 3, 6, 9, 12 b, 24 |
| Studies included only in systematic review | |||||||
| Balakrishnan, 2020 [16] | India | RCT | 32 | PRP injection (double-spin method) | TrA injection (10 mg/mL) | 3 sessions, 4-week intervals | 0, 4, 8, 12 |
| Trink, 2013 [20] | Italy | RCT | 30 | PRP injection (single-spin method) | TrA injection (2,5 mg/mL), placebo | 3 sessions, 4-week intervals | 8, 24, 48 |
| Intervention (PRP) Group | Control (TrA) Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| First Author, Year of Publication | Number of Patients | Age, Mean (SD) | Sex (Female % of Total) | Baseline SALT Score, Mean (SD) | Post-Treatment SALT Score, Mean (SD) | Numberof Patients | Age, Mean (SD) | Sex (Female % of Total) | Baseline SALT Score, Mean (SD) | Post-Treatment SALT Score, Mean (SD) |
| Albalat, 2019 [15] | 40 | 30.8 (7.5) | 15.0 | 1.7 (0.9) | 0.4 (0.7) | 40 | 36.3 (11.3) | 15.0 | 1.7 (0.8) | 0.5 (0.8) |
| Fawzy, 2020 [17] | 17 | 31.4 (10.6) | 23.5 | 5.6 (8.4) | 3.8 (8.4) | 14 | 34.2 (12.3) | 28.6 | 4.2 (4.4) | 1.4 (1.8) |
| Hegde, 2020 [18] | 25 | N/A | N/A | 7.2 (3.8) | 4.0 (5.3) | 25 | N/A | N/A | 8.8 (5.8) | 3.1 (5.1) |
| Kapoor, 2020 [19] | 20 | 25.4 (4.9) | 45.0 | 4.4 (2.5) | 3.2 (2.0) | 20 | 28.8 (8.6) | 65.0 | 9.0 (1.4) | 3.1 (0.8) |
| Quantitative Data Synthesis | Heterogeneity | ||||||
|---|---|---|---|---|---|---|---|
| Study | PRP Group (n) | TrA Group (n) | Effect Size | 95% CI | p Value | I2 | T2 |
| Overall Effect | 102 | 99 | −2.04 | [−4.72; 0.65] | 0.14 | 80.4% | 2.24 |
| Leave-one-out sensitivity analysis | |||||||
| Albalat, 2019 [15] | 62 | 59 | −3.79 | [−5.75; −1.83] | 0.001 | 0.0% | 0.04 |
| Fawzy, 2020 [17] | 85 | 85 | −2.15 | [−5.14; 0.83] | 0.15 | 87.0% | 5.57 |
| Hegde, 2020 [18] | 77 | 74 | −1.94 | [−5.62; 1.73] | 0.30 | 85.0% | 7.32 |
| Kapoor, 2020 [19] | 82 | 79 | −0.57 | [−2.54; 1.41] | 0.57 | 9.0% | 1.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meznerics, F.A.; Illés, K.; Dembrovszky, F.; Fehérvári, P.; Kemény, L.V.; Kovács, K.D.; Wikonkál, N.M.; Csupor, D.; Hegyi, P.; Bánvölgyi, A. Platelet-Rich Plasma in Alopecia Areata—A Steroid-Free Treatment Modality: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomedicines 2022, 10, 1829. https://doi.org/10.3390/biomedicines10081829
Meznerics FA, Illés K, Dembrovszky F, Fehérvári P, Kemény LV, Kovács KD, Wikonkál NM, Csupor D, Hegyi P, Bánvölgyi A. Platelet-Rich Plasma in Alopecia Areata—A Steroid-Free Treatment Modality: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomedicines. 2022; 10(8):1829. https://doi.org/10.3390/biomedicines10081829
Chicago/Turabian StyleMeznerics, Fanni Adél, Kata Illés, Fanni Dembrovszky, Péter Fehérvári, Lajos Vince Kemény, Kata Dorottya Kovács, Norbert Miklós Wikonkál, Dezső Csupor, Péter Hegyi, and András Bánvölgyi. 2022. "Platelet-Rich Plasma in Alopecia Areata—A Steroid-Free Treatment Modality: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" Biomedicines 10, no. 8: 1829. https://doi.org/10.3390/biomedicines10081829