
The Regional Burden and Disability-Adjusted Life Years of Knee Osteoarthritis in Kazakhstan 2014–2020
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Exposures and Covariates
2.3. Disability-Adjusted Life Years Calculation
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic and Baseline Characteristics
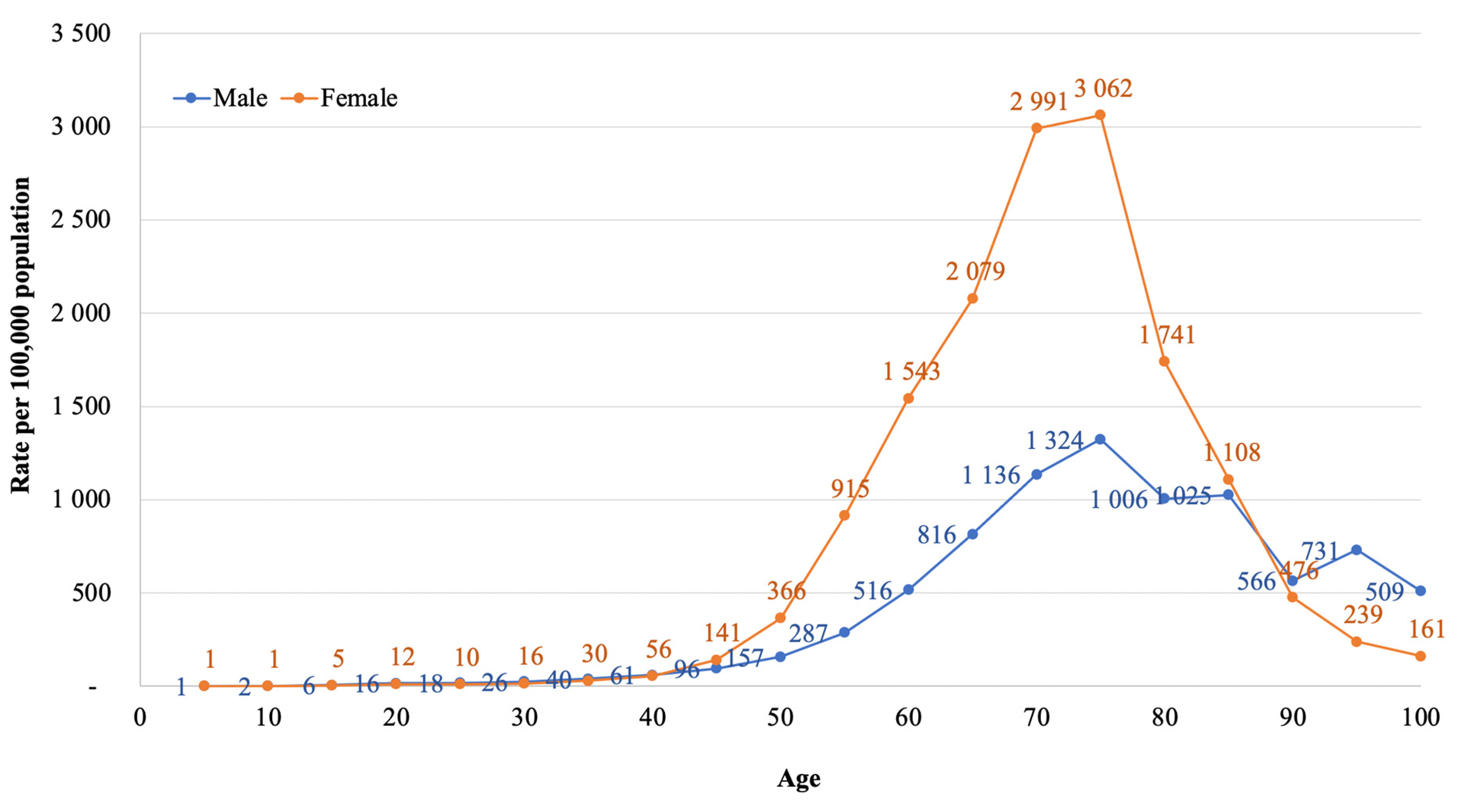
3.2. Incidence Based on Hospital Admission Records
3.3. DALY
4. Discussion
4.1. Socio-Demographic and Baseline Characteristics
4.2. Incidence Based on Hospital Admission and Discharge Records
4.3. DALY
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Torres, L.; Dunlop, D.D.; Peterfy, C.; Guermazi, A.; Prasad, P.; Hayes, K.W.; Song, J.; Cahue, S.; Chang, A.; Marshall, M. The relationship between specific tissue lesions and pain severity in persons with knee osteoarthritis. Osteoarthr. Cartil. 2006, 14, 1033–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oo, W.M.; Liu, X.; Hunter, D.J. Pharmacodynamics, efficacy, safety and administration of intra-articular therapies for knee osteoarthritis. Expert Opin. Drug Metab. Toxicol. 2019, 15, 1021–1032. [Google Scholar] [CrossRef] [PubMed]
- Hanna, F.S.; Teichtahl, A.J.; Wluka, A.E.; Wang, Y.; Urquhart, D.M.; English, D.R.; Giles, G.G.; Cicuttini, F.M. Women have increased rates of cartilage loss and progression of cartilage defects at the knee than men: A gender study of adults without clinical knee osteoarthritis. Menopause 2009, 16, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Heidari, B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Casp. J. Intern. Med. 2011, 2, 205. [Google Scholar]
- Zhang, W.; McWilliams, D.F.; Ingham, S.L.; Doherty, S.A.; Muthuri, S.; Muir, K.R.; Doherty, M. Nottingham knee osteoarthritis risk prediction models. Ann. Rheum. Dis. 2011, 70, 1599–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safiri, S.; Kolahi, A.-A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A. Global, regional and national burden of osteoarthritis 1990-2017: A systematic analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2019; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Gusmanov, A.; Zhakhina, G.; Yerdessov, S.; Sakko, Y.; Mussina, K.; Alimbayev, A.; Syssoyev, D.; Sarria, A.; Gaipov, A. Review of the research databases on population-based registries of Unified electronic Healthcare system of Kazakhstan (UNEHS): Possibilities and limitations for epidemiological research and Real-World Evidence. Int. J. Med. Inform. 2022, 170, 104950. [Google Scholar] [CrossRef] [PubMed]
- Ministry on National economy of the Republic of Kazakhstan Committee on Statistics. Demographic yearbook of Kazakhstan. Available online: https://stat.gov.kz/official/industry/61/publication (accessed on 20 November 2022).
- Yerdessov, S.; Kadyrzhanuly, K.; Sakko, Y.; Gusmanov, A.; Zhakhina, G.; Galiyeva, D.; Bekbossynova, M.; Salustri, A.; Gaipov, A. Epidemiology of Arterial Hypertension in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019. J. Cardiovasc. Dev. Dis. 2022, 9, 52. [Google Scholar] [CrossRef]
- Gaipov, A.; Galiyeva, D.; Gusmanov, A.; Sakko, Y.; Issanov, A.; Atageldiyeva, K.; Kadyrzhanuly, K.; Nurpeissova, A.; Rakhimzhanova, M.; Durmanova, A. Epidemiology of Type 1 and Type 2 Diabetes Mellitus in Kazakhstan: Data from Unified National Electronic Health System 2014-2019. BMC Endocr. Disord. 2022. [Google Scholar] [CrossRef]
- Liu, M.; Jin, F.; Yao, X.; Zhu, Z. Disease burden of osteoarthritis of the knee and hip due to a high body mass index in China and the USA: 1990–2019 findings from the global burden of disease study 2019. BMC Musculoskelet. Disord. 2022, 23, 63. [Google Scholar] [CrossRef]
- Vina, E.R.; Ran, D.; Ashbeck, E.L.; Ratzlaff, C.; Kwoh, C.K. Race, sex, and risk factors in radiographic worsening of knee osteoarthritis. In Seminars in Arthritis and Rheumatism; WB Saunders: Philadelphia, PA, USA, 2018; pp. 464–471. [Google Scholar]
- Mochizuki, T.; Tanifuji, O.; Koga, Y.; Sato, T.; Kobayashi, K.; Nishino, K.; Watanabe, S.; Ariumi, A.; Fujii, T.; Yamagiwa, H. Sex differences in femoral deformity determined using three-dimensional assessment for osteoarthritic knees. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 468–476. [Google Scholar] [CrossRef]
- Bawa, H.S.; Weick, J.W.; Dirschl, D.R. Gender disparities in osteoarthritis-related health care utilization before total knee arthroplasty. J. Arthroplast. 2016, 31, 2115–2118. [Google Scholar] [CrossRef]
- Hawker, G.A. Osteoarthritis is a serious disease. Clin. Exp. Rheumatol. 2019, 37, 3–6. [Google Scholar] [PubMed]
- Stevens-Lapsley, J.E.; Kohrt, W.M. Osteoarthritis in women: Effects of estrogen, obesity and physical activity. Women’s Health 2010, 6, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Roman-Blas, J.A.; Castañeda, S.; Largo, R.; Herrero-Beaumont, G. Osteoarthritis associated with estrogen deficiency. Arthritis Res. Ther. 2009, 11, 241. [Google Scholar] [CrossRef] [Green Version]
- Richette, P.; Corvol, M.; Bardin, T. Estrogens, cartilage, and osteoarthritis. Jt. Bone Spine 2003, 70, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Klerk, B.; Schiphof, D.; Groeneveld, F.; Koes, B.; van Osch, G.; van Meurs, J.; Bierma-Zeinstra, S. No clear association between female hormonal aspects and osteoarthritis of the hand, hip and knee: A systematic review. Rheumatology 2009, 48, 1160–1165. [Google Scholar] [CrossRef] [Green Version]
- Tschon, M.; Contartese, D.; Pagani, S.; Borsari, V.; Fini, M. Gender and sex are key determinants in osteoarthritis not only confounding variables. A systematic review of clinical data. J. Clin. Med. 2021, 10, 3178. [Google Scholar] [CrossRef]
- Redondo-Sendino, Á.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health 2006, 6, 155. [Google Scholar] [CrossRef] [Green Version]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender differences in the utilization of health care services. J. Fam. Pract. 2000, 49, 147. [Google Scholar]
- Rahmati, M.; Nalesso, G.; Mobasheri, A.; Mozafari, M. Aging and osteoarthritis: Central role of the extracellular matrix. Ageing Res. Rev. 2017, 40, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; Bridgett, L.; March, L.; Hoy, D.; Penserga, E.; Brooks, P. The epidemiology of osteoarthritis in Asia. Int. J. Rheum. Dis. 2011, 14, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Kang, X.; Fransen, M.; Zhang, Y.; Li, H.; Ke, Y.; Lu, M.; Su, S.; Song, X.; Guo, Y.; Chen, J. The high prevalence of knee osteoarthritis in a rural Chinese population: The Wuchuan osteoarthritis study. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2009, 61, 641–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schur, C.L.; Franco, S.J. Access to health care. In Rural Health United States; Oxford University Press: New York, NY, USA, 1999; pp. 25–37. [Google Scholar]
- Szilagyi, I.A.; Waarsing, J.H.; Schiphof, D.; van Meurs, J.B.J.; Bierma-Zeinstra, S.M.A. Towards sex-specific osteoarthritis risk models: Evaluation of risk factors for knee osteoarthritis in males and females. Rheumatology 2022, 61, 648–657. [Google Scholar] [CrossRef]
- Bureau of National Statistics of the Agency for Strategic Planning and Reforms of the Republic of Kazakhstan. Employment in Kazakhstan 2016–2020. Available online: https://www.stat.gov.kz/official/industry/25/statistic/6 (accessed on 23 November 2022).
- Rossignol, M.; Leclerc, A.; Allaert, F.A.; Rozenberg, S.; Valat, J.P.; Avouac, B.; Coste, P.; Litvak, E.; Hilliquin, P. Primary osteoarthritis of hip, knee, and hand in relation to occupational exposure. Occup. Environ. Med. 2005, 62, 772–777. [Google Scholar] [CrossRef] [Green Version]
- Funck-Brentano, T.; Nethander, M.; Movérare-Skrtic, S.; Richette, P.; Ohlsson, C. Causal factors for knee, hip, and hand osteoarthritis: A Mendelian randomization study in the UK biobank. Arthritis Rheumatol. 2019, 71, 1634–1641. [Google Scholar] [CrossRef] [Green Version]
- Niu, J.; Clancy, M.; Aliabadi, P.; Vasan, R.; Felson, D.T. Metabolic syndrome, its components, and knee osteoarthritis: The Framingham Osteoarthritis Study. Arthritis Rheumatol. 2017, 69, 1194–1203. [Google Scholar] [CrossRef] [Green Version]
- Alenazi, A.M.; Alshehri, M.M.; Alothman, S.; Alqahtani, B.A.; Rucker, J.; Sharma, N.; Segal, N.A.; Bindawas, S.M.; Kluding, P.M. The association of diabetes with knee pain severity and distribution in people with knee osteoarthritis using data from the osteoarthritis initiative. Sci. Rep. 2020, 10, 3985. [Google Scholar] [CrossRef] [Green Version]
- Alenazi, A.M.; Alshehri, M.M.; Alothman, S.; Alqahtani, B.A.; Rucker, J.; Sharma, N.K.; Bindawas, S.M.; Kluding, P.M. The association of diabetes with knee pain locations, pain while walking, and walking speed: Data from the osteoarthritis initiative. Phys. Ther. 2020, 100, 1977–1986. [Google Scholar] [CrossRef]
- Phillips, M.R.; Chang, Y.; Zura, R.D.; Mehta, S.; Giannoudis, P.V.; Nolte, P.A.; Bhandari, M. Impact of COVID-19 on orthopaedic care: A call for nonoperative management. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20934276. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19: Operational Guidance for Maintaining Essential Health Services during an Outbreak; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- NHS England and Improvement. Clinical Guide for the Management of Trauma and Orthopaedic Patients during the Coronavirus Pandemic; NHS England and Improvement: London, UK, 2020. [Google Scholar]
- Garrido-Cumbrera, M.; Marzo-Ortega, H.; Christen, L.; Plazuelo-Ramos, P.; Webb, D.; Jacklin, C.; Irwin, S.; Grange, L.; Makri, S.; Mateus, E.F. Assessment of impact of the COVID-19 pandemic from the perspective of patients with rheumatic and musculoskeletal diseases in Europe: Results from the REUMAVID study (phase 1). RMD Open 2021, 7, e001546. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Razak, H.R.B.A.; Talaei, M.; Ang, L.-W.; Yuan, J.-M.; Koh, W.-P. Duration of physical activity, sitting, sleep and the risk of total knee replacement among Chinese in Singapore, the Singapore Chinese Health Study. PLoS ONE 2018, 13, e0202554. [Google Scholar] [CrossRef]
- Apold, H.; Meyer, H.E.; Nordsletten, L.; Furnes, O.; Baste, V.; Flugsrud, G.B. Risk factors for knee replacement due to primary osteoarthritis, a population based, prospective cohort study of 315,495 individuals. BMC Musculoskelet. Disord. 2014, 15, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry on National economy of the Republic of Kazakhstan Committee on Statistics. Statistics of labour and employment. 2020. Available online: https://www.stat.gov.kz/official/industry/25/statistic/6 (accessed on 20 November 2022).
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.L.; Lopez, A.D.; World Health, O. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Kendzerska, T.; Jüni, P.; King, L.K.; Croxford, R.; Stanaitis, I.; Hawker, G.A. The longitudinal relationship between hand, hip and knee osteoarthritis and cardiovascular events: A population-based cohort study. Osteoarthr. Cartil. 2017, 25, 1771–1780. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.A.; Croxford, R.; Bierman, A.S.; Harvey, P.J.; Ravi, B.; Stanaitis, I.; Lipscombe, L.L. All-cause mortality and serious cardiovascular events in people with hip and knee osteoarthritis: A population based cohort study. PloS ONE 2014, 9, e91286. [Google Scholar] [CrossRef]
- Ravi, B.; Croxford, R.; Austin, P.C.; Lipscombe, L.; Bierman, A.S.; Harvey, P.J.; Hawker, G.A. The relation between total joint arthroplasty and risk for serious cardiovascular events in patients with moderate-severe osteoarthritis: Propensity score matched landmark analysis. BMJ 2013, 347, f6187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Total (n = 56,895) | Female (n = 43,427; 76%) | Male (n = 13,468; 24%) | p-Value | |
|---|---|---|---|---|
| Socio-Demographics | ||||
| Age category, n (%) | <0.001 | |||
| <17 y.o. | 193 (0.3) | 77 (0.2) | 116 (0.9) | |
| 18–34 y.o. | 1105 (2) | 446 (1) | 659 (5) | |
| 35–50 y.o | 5851 (10) | 3931 (9) | 1920 (14) | |
| 51–69 y.o. | 36,898 (64.7) | 28,968 (66.8) | 7930 (59) | |
| >70 y.o. | 12,848 (23) | 10,005 (23) | 2843 (21.1) | |
| Ethnicity, n (%) | <0.001 | |||
| Kazakh | 37,658 (66) | 27,977 (64) | 9681 (72) | |
| Russian | 11,872 (21) | 9657 (22) | 2215 (16) | |
| Other | 7365 (13) | 5793 (14) | 1572 (12) | |
| Living area, n (%) | <0.001 | |||
| Urban | 34,079 (60) | 26,838 (62) | 7241 (54) | |
| Rural | 22,816 (40) | 16,589 (38) | 6227 (46) | |
| Social status, n (%) | <0.001 | |||
| Employed | 11,761 (21) | 7842 (18) | 3919 (29) | |
| Unemployed | 8607 (15) | 6099 (14) | 2508 (19) | |
| Retiree | 32,550 (57) | 27,051 (62) | 5499 (41) | |
| Disabled | 1584 (3) | 905 (2) | 679 (5) | |
| Other | 2393 (4) | 1530 (4) | 863 (6) | |
| Outcome | <0.001 | |||
| Living | 53,108 (93) | 41,068 (95) | 12,040 (89) | |
| Died | 3787 (7) | 2359 (5) | 1428 (11) | |
| Comorbidities | ||||
| Obesity, n (%) | <0.001 | |||
| Yes | 1090 (2) | 888 (2) | 202 (1) | |
| No | 55,805 (98) | 42,539 (98) | 13,266 (99) | |
| Hypertension, n (%) | <0.001 | |||
| Yes | 27,897 (49) | 22,674 (52) | 5223 (39) | |
| No | 28,998 (51) | 20,753 (48) | 8245 (61) | |
| Diabetes, n (%) | <0.001 | |||
| Yes | 6398 (11) | 5248 (12) | 1150 (9) | |
| No | 50,497 (89) | 38,179 (88) | 12,318 (91) | |
| Age Group | Life Expectancy | Female | Male | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| YLL | YLD | DALY | YLL | YLD | DALY | YLL | YLD | DALY | ||
| 0-19 | 76.2525 | 0.0 | 687.6 | 687.6 | 0.0 | 1022.1 | 1022.1 | 0.0 | 1709.7 | 1709.7 |
| 20-24 | 63.88 | 63.9 | 392.5 | 456.4 | 127.8 | 728.0 | 855.8 | 191.6 | 1120.6 | 1312.2 |
| 25-29 | 58.94 | 117.9 | 656.1 | 774.0 | 235.8 | 1044.8 | 1280.5 | 353.6 | 1700.9 | 2054.6 |
| 30-34 | 54 | 216.0 | 1029.7 | 1245.7 | 324.0 | 1328.7 | 1652.7 | 540.0 | 2358.5 | 2898.5 |
| 35-39 | 49.09 | 392.7 | 1500.0 | 1892.7 | 490.9 | 1571.2 | 2062.1 | 883.6 | 3071.2 | 3954.8 |
| 40-44 | 44.23 | 442.3 | 3238.6 | 3680.9 | 309.6 | 2060.7 | 2370.3 | 751.9 | 5299.3 | 6051.2 |
| 45-49 | 39.43 | 1104.0 | 6974.3 | 8078.3 | 1025.2 | 2691.6 | 3716.7 | 2129.2 | 9665.8 | 11,795.1 |
| 50-54 | 34.72 | 3888.6 | 15,305.0 | 19,193.6 | 2916.5 | 4051.8 | 6968.3 | 6805.1 | 19,356.8 | 26,161.9 |
| 55-59 | 30.1 | 6110.3 | 20,409.4 | 26,519.7 | 4605.3 | 5622.1 | 10,227.4 | 10,715.6 | 26,031.4 | 36,747.0 |
| 60-64 | 25.55 | 6821.9 | 18,161.5 | 24,983.4 | 5340.0 | 5003.2 | 10,343.2 | 12,161.8 | 23,164.7 | 35,326.5 |
| 65-69 | 21.12 | 10,792.3 | 15,391.7 | 26,184.0 | 5617.9 | 3604.0 | 9221.9 | 16,410.2 | 18,995.6 | 35,405.9 |
| 70-74 | 16.78 | 7450.3 | 7451.6 | 14,901.9 | 3557.4 | 1734.7 | 5292.0 | 11,007.7 | 9186.3 | 20,194.0 |
| 75-79 | 12.85 | 6270.8 | 3398.2 | 9669.0 | 3341.0 | 856.7 | 4197.7 | 9611.8 | 4254.9 | 13,866.7 |
| 80-84 | 9.34 | 1802.6 | 755.5 | 2558.1 | 1158.2 | 268.1 | 1426.2 | 2960.8 | 1023.6 | 3984.4 |
| 85+ | 5.05 | 444.4 | 94.5 | 538.9 | 328.3 | 43.6 | 371.8 | 772.7 | 138.1 | 910.7 |
| Total | 45,918.1 | 95,446.3 | 141,364.3 | 29,377.6 | 31,631.1 | 61,008.7 | 75,295.7 | 127,077.3 | 202,373.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhakhina, G.; Gusmanov, A.; Sakko, Y.; Yerdessov, S.; Semenova, Y.; Saginova, D.; Batpen, A.; Gaipov, A. The Regional Burden and Disability-Adjusted Life Years of Knee Osteoarthritis in Kazakhstan 2014–2020. Biomedicines 2023, 11, 216. https://doi.org/10.3390/biomedicines11010216
Zhakhina G, Gusmanov A, Sakko Y, Yerdessov S, Semenova Y, Saginova D, Batpen A, Gaipov A. The Regional Burden and Disability-Adjusted Life Years of Knee Osteoarthritis in Kazakhstan 2014–2020. Biomedicines. 2023; 11(1):216. https://doi.org/10.3390/biomedicines11010216
Chicago/Turabian StyleZhakhina, Gulnur, Arnur Gusmanov, Yesbolat Sakko, Sauran Yerdessov, Yuliya Semenova, Dina Saginova, Arman Batpen, and Abduzhappar Gaipov. 2023. "The Regional Burden and Disability-Adjusted Life Years of Knee Osteoarthritis in Kazakhstan 2014–2020" Biomedicines 11, no. 1: 216. https://doi.org/10.3390/biomedicines11010216